 Lena Jäggi1,2*
Lena Jäggi1,2* Stella M. Hartinger1,2,3
Stella M. Hartinger1,2,3 Günther Fink1,2Dana C. McCoy4Milagros Alvarado Llatance1,2
Günther Fink1,2Dana C. McCoy4Milagros Alvarado Llatance1,2 Kristen Hinckley1,2,3Lucero Ramirez-Varela4Leonel Aguilar5Andreana Castellanos6Daniel Mäusezahl1,2,3
Kristen Hinckley1,2,3Lucero Ramirez-Varela4Leonel Aguilar5Andreana Castellanos6Daniel Mäusezahl1,2,3- 1University of Basel, Basel, Switzerland
- 2Department of Epidemiology and Public Health, Swiss Tropical and Public Health Institute, Allschwil, Switzerland
- 3School of Public Health and Administration, Universidad Peruana Cayetano Heredia, Lima, Peru
- 4Harvard Graduate School of Education, Cambridge, MA, United States
- 5Department of Computer Science, ETH Zurich, Zurich, Switzerland
- 6Afinidata, Guatemala City, Guatemala
Objectives: This scoping review examines the evidence and knowledge gaps regarding the effectiveness of digital early childhood parenting interventions in Low- and Middle-Income Countries (LMICs).
Methods: Using PRISMA-ScR and PICOS frameworks, we systematically reviewed studies published since 2010 from four databases, focusing on the impact of digital parenting interventions on Early Childhood Development and parent-level outcomes.
Results: Of 1,399 studies identified, 13 met inclusion criteria, evaluating digital interventions for parents of children aged 0–5 years. These interventions included digital-only and hybrid approaches, leveraging technologies for tasks such as sharing health and ECD information, reminders, group chats, or screening. Among ECD studies, three of four with parent-reported outcomes found positive effects, but none of three using direct assessments did. Parent-level outcomes, such as mental health and parenting behaviors, showed consistent positive impacts.
Conclusion: Digital parenting interventions are feasible in LMICs but face challenges in implementation and reaching vulnerable families. Most studies are small-scale with variable designs and outcomes. Rigorous, high-quality studies are needed to establish effectiveness and optimize implementation strategies before these programs are deployed at scale.
Introduction
Skills acquired during early childhood, including language, cognition, and social-emotional abilities before age 5, are essential for later educational, emotional, and economic achievements [1]. Consequently, delays in these foundational Early Childhood Development (ECD) skills can significantly impact a child’s life trajectory. This emphasizes the importance of prioritizing strategies to support ECD, especially in Low- and Middle-Income Countries (LMIC), where it is estimated that almost 45% of children under 5 fail to reach their full developmental potential [2, 3]. Parenting interventions are gaining prominence as crucial strategies for enhancing ECD outcomes spanning diverse socioeconomic contexts, as documented in the Lancet series on ECD [4, 5]. Notably, parenting interventions in LMICs are especially impactful and exhibit over three times the effect on children’s cognitive, language, and motor development compared to those implemented in High-Income Countries (HICs) [6].
An expanding body of evidence underscores the increasing popularity of digital interventions to improve maternal and child health outcomes worldwide over the last decades [7, 8]. This trend can be attributed to the rapid global expansion of cell phone coverage and internet access, providing continual opportunities for health and educational systems to engage with families remotely [9–11], including vulnerable and hard-to-reach families in LMIC [7, 8]. Traditional ECD interventions are typically dependent on home visitations, face-to-face interactions, or community groups [6, 12]. However, they are expensive and can encounter disruptions due to unforeseen budget constraints, extreme events, or global occurrences such as COVID-19. This underscores the need for innovative solutions that allow remote delivery. Digital parenting interventions use technologies such as computers, apps, or (smart-) phones to enhance parenting skills and practices that promote ECD, including stimulation, early learning, and responsive parent-child interactions [13, 14]. In response, digital ECD interventions targeting parents of young children are increasingly implemented globally as potential tools to effectively bridge educational and service delivery gaps [11, 13, 14].
While some digital ECD parenting interventions show promise, the scarce data that exists on the effectiveness of such programs largely stems from high-income settings [13, 14]. Recent reviews highlight the potential of scalable and cost-effective digital interventions for maternal and child health in LMICs [1, 14] but little is known about the feasibility of using and adapting, and the compliance of digital ECD parenting interventions in LMICs.
Even more importantly, the impact of such digital ECD programs on child development and parental outcomes in these contexts remains unclear.
This scoping review aims to systematically assess and consolidate the current literature on digital interventions designed to enhance ECD in LMICs, focusing on those that are exclusively digital or include a significant digital component.
Methods
Search Strategy
We used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR; Supplementary Appendix S1) and the Population, Intervention, Comparator, Outcome, and Study types (PICOS) framework to structure our review (Table 1). No separate protocol was published.
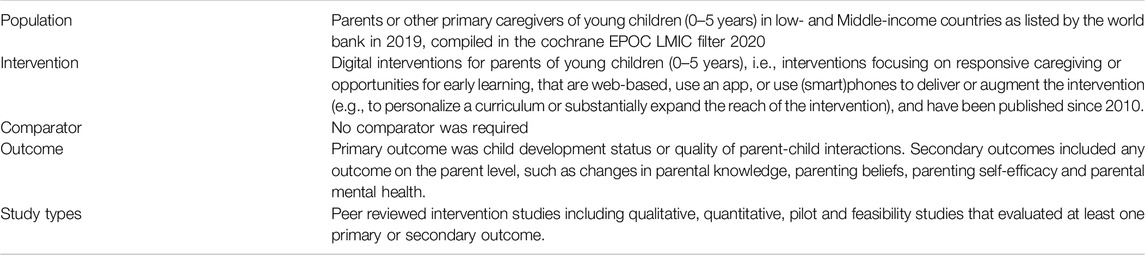
Table 1. Population, Intervention, Comparator, Outcome, and Study types (PICOS) framework (Allschwil, Switzerland. 2024).
After a preliminary literature review we consulted with a librarian to group a combination of MeSH terms, subject headings and text words in title and abstract to group the Boolean search into three thematic blocks: 1) young child terms (population) AND parenting/parent terms (population, content of intervention) AND child development terms (primary outcomes), AND 2) digital terms (type of intervention), AND 3) LMIC terms (Cochrane EPOC LMIC Filter 2020; location of population). We searched peer-reviewed articles in 4 databases (Pubmed/Medline, APA PsycInfo, Scopus, and Web of Science) on 08 June 2022, updated on 12 July 2023. The full search string for PubMed on Ovid and the final number of records returned are included in Supplementary Appendix S2. We used the Systematic Review Accelerator web app [15, 16] to conduct searches in different databases and deduplicate records and screened articles in the Rayyan web app [17].
Selection Criteria
We considered all original, peer-reviewed studies of digital parenting interventions (i.e., computer or app-supported, or using (smart-) phones) published from the invention of smartphones in 2010 to July 2023. Interventions had to target primary caregivers (henceforth “parents”) of children 0–5 years of age. While interventions could start during pregnancy, we required that they continued beyond birth. Interventions needed to focus on supporting parenting competencies and practices that promote ECD, such as opportunities for increasing stimulation, early learning, or responsiveness in parent-child interactions. We included interventions for special populations, such as for parents of children with a disability or for parents with mental health issues. Interventions needed to report an ECD outcome (primary outcome) or at least one secondary outcome on the parent level, such as parental knowledge, parenting beliefs, parenting self-efficacy, parental mental health or quality of parent-child interactions. The primary ECD outcome could be assessed by any means (e.g., direct assessment, parent report, observation).
Included interventions could be entirely digital or include a significant complementary digital component. The latter had to be a separate component that augmented the primary intervention, such as meaningfully expanding or personalizing a curriculum or expanding the reach of the intervention. For example, we excluded studies if digital tools were used exclusively to enhance in-person delivery, such as using videos or other digital teaching materials in live teaching sessions.
Finally, the study had to take place in a LMIC country, as defined by the World Bank list of countries 2019 compiled in the Cochrane EPOC LMIC filter 2020.
Exclusion Criteria
We excluded grey literature. Relevant reviews, meta-analyses, or study protocols were also excluded, but their reference lists were screened to identify potentially eligible studies. We further excluded school- or center-based interventions but included interventions in samples recruited from daycare centers that targeted parents and parenting behaviors at home. We also excluded digital interventions without a specific objective to promote ECD, such as reminders to get vaccinations, medical checkups or after-delivery care, interventions encouraging breastfeeding, or interventions targeting perinatal maternal depression without an explicit parenting or ECD component.
Screening and Data Extraction
After deduplication, articles were screened for relevance and the full text was evaluated. At least two of four reviewers (LJ, MA, KH, and LV) independently evaluated articles at each stage. Discrepancies in coding were resolved by consensus. Figure 1 shows a flowchart of the screening results. Extracted key data of the included studies are included in Table 2. A list of studies excluded during full-text screening and the reason for exclusion are included in Supplementary Appendix S3.
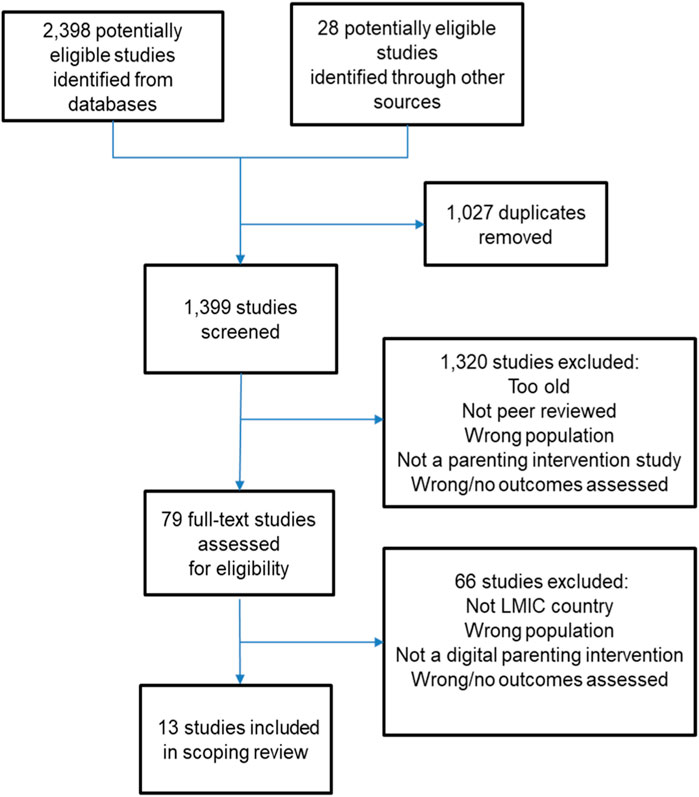
Figure 1. Screening flowchart (Allschwil, Switzerland. 2024).
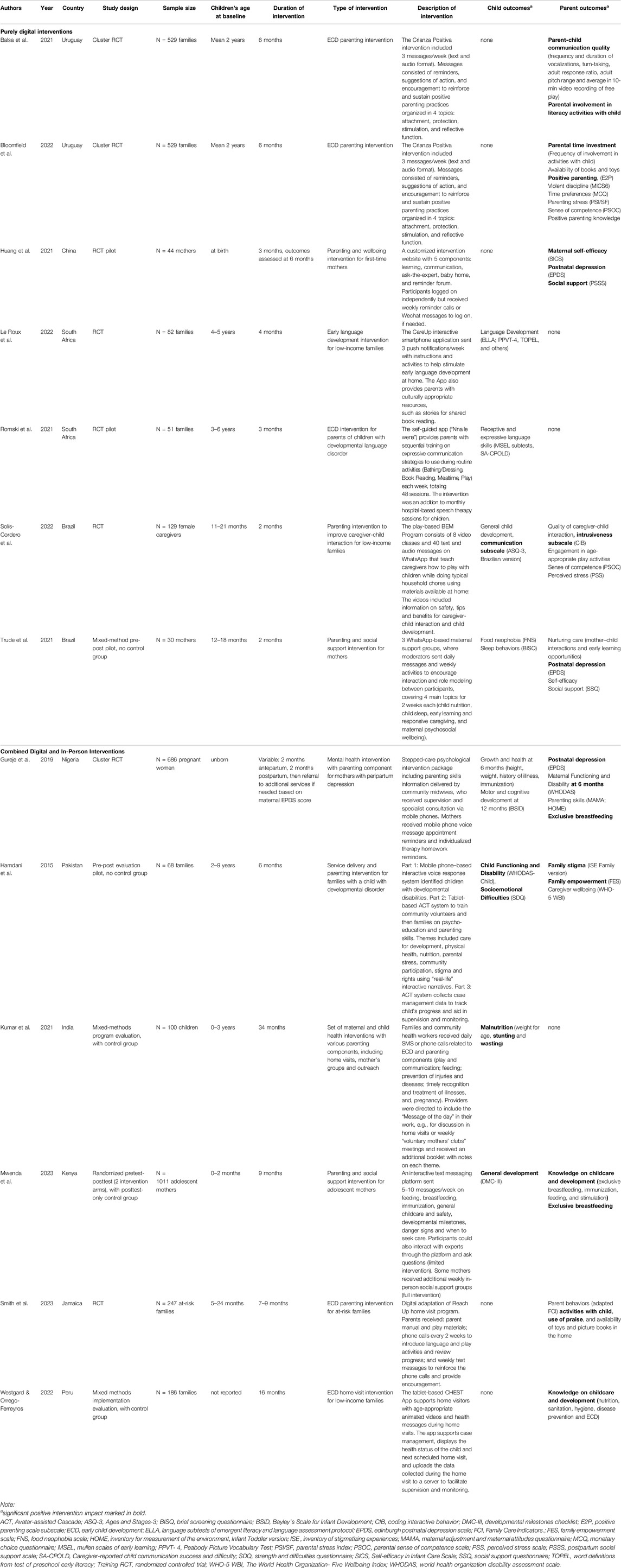
Table 2. Overview of included studies by type of intervention (Allschwil, Switzerland. 2024).
The data extraction table was developed based on the research questions and the PICOS framework and included basic demographic information about the sample (i.e., sample size, age), study design (e.g., pilot study, randomized controlled trial), country, general information on the intervention, information on the digital component of the intervention, and child development and parenting outcomes assessed. We conducted a descriptive analysis and summarized the strengths and weaknesses of research about digital ECD parenting interventions in LMICs.
Results
In total, 1,399 potentially relevant studies were identified (Figure 1). The abstract and full-text screening resulted in 13 included articles covering 5 interventions from Central and South America [Jamaica, Uruguay (2 studies from 1 intervention), Brazil and Peru], 4 from Africa [Kenya, Nigeria and South Africa (2 studies)], and 3 from Asia (Pakistan, China, and India). See Table 2 for details.
Study Characteristics
Among the 13 studies, 3 were cluster-randomized controlled trials (cRCT), 5 RCTs, 1 randomized study with posttest-only control, 2 studies without control groups, and 2 studies included control groups but did not provide information on randomization. The studies included 5 pilot or feasibility studies and 3 studies included qualitative components. The sample sizes included in the studies ranged from 30 to over 1′000, but 5 studies had fewer than 100 participants.
Most studies compared either a digital [18–23] or mixed intervention [24, 25] to no-intervention or usual-care control. In two studies [18, 19], all eligible families had completed an 8-week parenting workshop in-person before they were randomized to receive the purely digital intervention versus not. No studies directly compared a digital versus an in-person parenting intervention on ECD or parenting outcomes.
Intervention Characteristics
As shown in Table 2, 6 of the interventions (7 studies) were only digital, while 6 interventions combined digital and in-person components. Interventions targeted different age brackets of children, ranging from starting before birth [26], at birth [20, 27], to spanning 2–9 years [28]. However, 9 of the studies targeted infants through children up to 3 years and only 3 studies included children who were older than 3 years. Purely digital interventions were comparatively shorter than mixed interventions and lasted between 2 and 6 months. In terms of the target population, the purely digital interventions consisted predominantly (5/6) of general parenting programs for healthy parents of typically developing children, though some targeted low-income families or first-time mothers. One exception was a parenting app that promoted language development at home for parents of children with a developmental language disorder who were already receiving the local usual care treatment of hospital-based speech therapy [22]. Among the mixed-delivery interventions, there were 4 general parenting interventions: one digitally supported home-visit intervention [29] a remote adaptation of a home visit intervention [25], a digital parenting and social support intervention for adolescent mothers [27] and a comprehensive set of general maternal and child health interventions [24]. The other 2 mixed interventions targeted special groups, namely, mothers suffering from peri-partum depression [26] and families of children with a developmental disability [28].
Most purely digital interventions delivered content via pre-programmed scheduled Whatsapp [18, 19, 23, 30], SMS [18, 19] or in-App push-notification [21] messages to parents. Similarly the limited intervention arm in Mwenda et al.’s study received scheduled messages on an unnamed interactive messaging platform [27]. Only one study used moderators in the Whatsapp groups to encourage and facilitate spontaneous exchange between participants, though these exchanges were organized around pre-defined bi-weekly topics [30]. Moving beyond using a digital way to deliver fixed content at specific time points, one intervention used a self-guided, manualized parent training program in an App [22] and one intervention used a self-guided web-based content program [20]. However, both self-guided interventions were in fact accompanied and used strategies to increase compliance of the participants: Huang and colleagues’ monitored log-on data and sent individual WeChat reminders to log into the website to participants who fell under a weekly minimum [20]. Parents in the intervention by Romski and colleagues [22] received the tablet on which the app was installed. They were instructed on how to use the app, and how to integrate the communication strategies described in the app into everyday activities with their children. Moreover, participants were asked to fill out weekly in-app questionnaires and brought the tablet in for study staff to download monthly usage data.
Mixed digital and in-person interventions varied in the importance of the digital component concerning the overall intervention. For example, in the Kenyan program for adolescent mothers, the digital component was the main part of the intervention, which was compared to an enhanced version with an additional supportive in-person element [27]. One study replaced in-person home visits with remote delivery of content via phone calls and smartphone messages due to the restrictions brought by the COVID pandemic and was thus not intentionally designed as a mixed intervention [25]. The other 4 mixed interventions were predominantly delivered in-person, with some enhancing digital components to support community health workers providing the intervention [29] or both the intervention providers and the participating families [24, 26, 28], making them more digitally-enhanced rather than true mixed-delivery interventions. The support for providers consisted mainly of facilitating scheduling, monitoring participation, providing access to supervision, tracking of ECD, or providing them with digital or interactive content to support their in-person training of families. On the other hand, families received text reminders of therapy homework or appointments [26], informational messages on maternal and child health and ECD [24], or computer-assisted disability screening via phone to connect them to a comprehensive set of interventions and services if needed [28].
The level of detail in the description of intervention content varied greatly, but most digital general parenting interventions delivered content that was intended to give parents concrete ideas for activities or parenting strategies centered around positive parenting and nurturing care, and/or early learning and language development, sometimes combined with general informational content on ECD. Three studies did not describe details of the parenting or ECD content [20, 24, 26]. Three interventions explicitly mentioned being based on the multi-lateral Nurturing Care Framework [23, 27, 30], 2 studies referenced the Crianza Positiva positive parenting program [18, 19] and one intervention was a new locally developed home visit curriculum [29]. Three interventions were digital adaptations of existing interventions: one study was an adaptation of the validated Wordworks early literacy program [21], Smith and colleagues [25] described the remote delivery of the Reach Up home visit curriculum, and Romski and colleagues [22] adapted a protocol for young children with developmental disorders. Finally, Hamdani and colleagues [28] developed their intervention based on the mental health gap intervention guide from the WHO.
Intervention Compliance
In general, one important determinant of intervention success is participant compliance and participation. For the present sample of programs, all purely digital intervention studies and two mixed-delivery studies [24, 29] tracked program engagement with the digital component.
One study presented detailed results on program engagement and noted significant declines in participant contributions throughout their Whatsapp-based intervention [30]. Another study concluded they did not find significant impacts on child outcomes in their self-directed app intervention because most parents used the smartphone app very little; only 28.6% of parents in the experimental group used the application for more than half of the intervention period [21]. However, follow-up analyses did not find associations between app-use and child outcomes in their small sample size of 42 experimental families. Similarly, the only other study that looked at the influence of program engagement found no moderating effect of adherence on any of the child or parent outcomes [23]. In another intervention study in South Africa using a self-guided app, participation rates were much higher, and over half of the parents (13/20) completed almost all of the sessions [22]. However, this intervention was delivered via a tablet that was given to the parents at the beginning of the study, and was connected to monthly therapy visits to the hospital for the children, where parents met with research staff during their waiting time and could address any questions, clarifications, or comments about the intervention, including technical support.
Several other studies also used specific strategies to increase engagement with the digital intervention: One study [20] monitored logins and sent weekly reminders to mothers who did not use the program website at least twice weekly or who stayed logged on for less than an hour per week. Another intervention [18, 19] re-contacted intervention families and the childcare centers to get updated phone information and maximize the number of families who would receive the content on their phones. Finally, one study used research assistant participants to keep conversations flowing in some of their moderated Whatsapp groups, though this did not seem to make a difference in the overall contribution rates of the groups [30].
Child Outcome Findings
Nine of the studies measured at least one child outcome: only 3 studies used a validated direct assessment of ECD [21, 22, 26], and 4 studies used validated parent-reported child development or child disability questionnaires [22, 23, 27, 28]. Two studies assessed sleep behaviors or malnutrition.
None of the 3 studies using direct assessments found effects on ECD, while 3/4 studies assessing ECD with validated parent-reported instruments found positive child effects. One study [27] found improved general ECD, while another study [23] found positive effects on language but not on socio-emotional, cognitive or motor development. Hamdani and colleagues [28] found decreases in the children’s general disability and socioemotional difficulties over time. Kumar and colleagues [24] found positive effects on malnutrition outcomes. One pre-post study found negative effects on child’s food neophobia over time [30]. No change in communication difficulty was found in another small study [22].
Parent Outcome Findings
In 2 studies, direct measurements of parent-child interactions were conducted using video recordings [18, 23]. In both studies, the digital intervention group showed improved outcomes, with less intrusiveness in the caregiver-child interaction [23] and better communication quality and responsiveness [18].
Ten studies assessed self-reported parenting outcomes, such as parenting behaviors, skills or knowledge centered on positive parenting, nurturing care, and healthy child development; often using multiple measures. Most studies observed positive effects on self-reported parenting behaviors or parenting knowledge, such as increased involvement in games or literacy activities [18, 19, 25], increased use of positive parenting practices [25], increased exclusive breastfeeding [26, 27], increases in parenting self-efficacy [20], or more knowledge on child development [27, 29]. However, several studies found no change in some parenting outcomes, such as sense of parenting competence [23], parental knowledge [19], nurturing care behaviors [30], self-efficacy [19, 30], or parenting skills [26]. One study assessed stimulation, immunization and feeding parenting practices, but no results were reported [27]. In summary, all studies who assessed parent outcomes, found improvement on some parenting measure in their intervention groups, though not on all measures.
Six studies also assessed parent outcomes which were not directly parenting related, such as parental stress [19, 23], wellbeing [28], social support [20, 30], or depression [20, 26, 30]. All 3 interventions targeting maternal depression found lower rates of maternal depression [20, 26, 30], and one of the studies also found increases in social support [20]. However, the other 3 studies found no differences in parental wellbeing [28] or stress levels [19, 23].
Discussion
This scoping review aimed to evaluate existing evidence on digital parenting interventions in LMICs. Among the 12 interventions covered in 13 studies meeting inclusion criteria, 6 were purely digital, while the remaining 6 combined digital and in-person components.
The great diversity of intervention content, delivery, targeted participants, duration, study design, and outcome assessments makes a comparison and summary of trends challenging. Furthermore, even though parenting interventions ultimately seek to improve ECD, only 6/13 studies included assessments of ECD. Finally, 5 studies had fewer than 100 participants and only 3 had sample sizes of over 500 participants, highlighting the early stage of the current state of the literature.
Leveraging the Digital Component
Broadly, current programs can be divided into purely digital, digitally supported, and true mixed digital and in-person interventions. Concerning the second type, supporting known in-person interventions with a digital component showed promising results [24, 28, 29], both to make content more attractive for parents and to assist in efficient case management and quality control. For example, digital supports including innovative screening approaches, cascade training, and monitoring using a supervision system between trained agents have been used successfully to increase the reach and quality of interventions in the included studies.
In many studies of purely digital interventions [18, 19, 21–29], the digital component primarily consisted of changing the delivery method from in-person to remote or digital. Specifically, most of these programs mirrored manual in-person interventions, relying on one-way messaging to deliver curriculum content at regular intervals. Even in self-directed app environments, the self-directed component translated largely into re-visiting previous sessions or a content library at parents’ discretion [22]. The most interactive parts of such programs were help or ask-an-expert functions, where parents could reach out (to a real person) for specific advice [20, 27]. While these interventions could be valuable, it remains questionable whether a passive, largely informational approach is enough to lead to meaningful behavioral change. Additionally, this approach does not fully capitalize on the true potential of more current digital solutions such as artificial intelligence, e.g., personalized content selection [31], content personalization [32], real-time monitoring and feedback, adaptive learning [33], intelligent engagement, virtual assistance, developmental risks, and opportunities detection. For example, using artificial intelligence could help personalize content delivery based on user preferences and behavior, enhancing engagement and relevance. Similarly, intelligent engagement could tailor notifications, reminders, and other forms of communication to the specific caregiver needs to keep them engaged. Incorporating more automated features, such as personalized messaging systems, can facilitate real-time interaction, foster social exchanges, and cultivate online communities.
Only in one study were mothers asked to freely choose content without a curriculum on an internet-based support program [20]. Unfortunately, the program was not well described, and while the authors found program impacts on maternal mental health and wellbeing, they did not assess parenting behaviors or ECD. Further, mothers who did not spend a minimum amount of weekly time logged on received reminders, which might have different effects outside of a research context.
Keeping users engaged is a challenging but crucial issue for all self-guided digital interventions [9, 11]. In digital parenting interventions in HIC completion rates from 7% [34] to 15% [35] have been reported. Strategies employed to bolster compliance, such as weekly reminders and re-contacting families for updated contact information [18–20], underscore the importance of proactive measures to maximize participant involvement. However, evidence of the effectiveness of these strategies remains mixed [30]. This variability prompts critical questions about the factors influencing compliance levels, including the user-friendliness of digital platforms, relevance of intervention content, and cultural adaptation. Understanding these dynamics is essential for optimizing the design and impact of digital interventions.
Importantly, while the use of such strategies might be a crucial component to ensure participants receive an adequate dosage of the digital intervention, it raises questions about the feasibility of achieving comparable results in a real-world setting where such supporting measures might not always be appropriate or available. Furthermore, infrastructure and resource barriers play a significant role in shaping engagement with digital interventions. Factors like unstable internet access, lack of devices, or limited technical support can disproportionately hinder compliance in under-resourced settings. Without addressing these underlying inequities, the potential impact of digital interventions may remain unevenly distributed, further perpetuating health disparities.
The Impact of Digital Parenting Interventions
There is an established evidence base showing that in-person parenting interventions following an established curriculum improve ECD if well-executed [6]. Nine of the included studies implemented digitized versions of such interventions but only 3 of them assessed ECD outcomes [21, 23, 27]. While 2 studies found some parent-reported ECD impact [23, 27], the one study using a direct child assessment had major intervention compliance issues and did not find ECD effects [21]. Notably, the other 2 studies using direct child assessments were not general parenting interventions [6]: One intervention with a comparatively minor parenting component compared high-to low-intensity mental health treatment groups among mothers screened positive for depression [26]. The study found positive effects for maternal mental health and exclusive breastfeeding, but no gains in parenting skills. This suggests that the parenting component was not emphasized enough, and that improvements in maternal depression might need more time to translate into ECD impact. The other intervention was a parent-training addition to hospital-based speech therapy for children [22]. Even with high compliance, a 4-month parent training might not be enough to show effects on children above sessions with a speech therapist. Finally, no studies directly compared a digital versus an in-person parenting intervention on ECD or parenting outcomes.
Digital parenting interventions generally showed positive effects on parenting behaviors and knowledge, such as increased activity involvement and better communication. These interventions also tended to improve parental wellbeing, particularly by reducing depression. Although many studies reported various parent outcomes, with some non-significant findings, the successes suggest potential benefits for child outcomes as well, which may be revealed in long-term observational studies.
Successful Digital Interventions
Most studies that found intervention effects either included an important in-person component in the intervention (mixed-delivery interventions) or were able to attach the digital intervention to in-person interactions. This included a follow-up to a previous in-person intervention [18, 19], embedding it in monthly visits to the hospital [22], or creating a community on Whatsapp [30]. Even the individualized logon reminders used in one study could be argued to create a social pressure similar to in-person interactions that would increase compliance [20]. One possible explanation for this is that digital interventions alone might not (yet) provide sufficient levels of community, support and personalized exchange to keep parents engaged compared to in-person interactions.
However, in our review, we have only found 1 intervention testing the added value of an in-person component versus a purely digital intervention [27]. The study showed child and mother impacts compared to control in both intervention arms. Interestingly, the added in-person component only marginally improved knowledge scores of the adolescent mothers in Kenya and generated no additional impact on the parent-reported child development outcome compared to the purely digital intervention group.
Several distinguishing intervention features could potentially explain the success of this Kenyan intervention: i.) The frequency of messages was high with 5–10 weekly messages and the 9 months intervention period was longer than other purely digital interventions, ii.) there was an interactive component, where participants could directly use the messaging platform to ask questions to experts, iii.) participants were adolescent mothers, who might be more open to receive support compared to older mothers and iv.) the intervention might have integrated easily with existing social media habits [27].
Limitations
This study has limitations. In accordance with accepted standards for scoping reviews, we did not examine the methodological quality and risk of bias of the studies. Due to the limited availability of data, we also were not able to conduct a formal meta-analysis.
Recommendations for Future Research
Concretely, based on these findings we recommend 5 main directions for future research:
1. Assessing the efficacy, cost-effectiveness, and best practices for digital parenting interventions, including measurements of child impact.
2. Exploring and comparing the potential of digital versus in-person parenting interventions is a highly important avenue of investigation that is to date completely absent from the literature.
3. Examining how different delivery methods affect intervention outcomes and the potential benefits of offering participants a choice in the digital versus in-person elements. Similarly, examining how different strategies improve compliance and take-up of interventions.
4. Addressing the current one-way digital information delivery by incorporating personalized, AI-integrated curricula that can automate engagement and utilize interactive features to foster online communities.
5. Exploring strategies for translating the application and adherence of these interventions from research settings to real-world practice, a notably under-discussed area in existing literature.
Conclusion
In summary, results show that to date there is a severe lack of data on ECD outcomes (direct assessments or parent-reported) in the context of digital parenting interventions. There is some indication that updating existing in-person interventions into a digitally-supported or digitally-enhanced version holds promise to make such interventions more effective. However, interventions that integrate more current digital solutions, such as artificial intelligence, for personalization, online community-building or real-time exchanges, are still missing. Finally, current studies often fail to address crucial factors such as acceptance, adoption, and sustained use of the interventions, which are integral to understanding their impact on ECD. Overall, it is evident that despite their promise for large-scale dissemination, the effectiveness of digital parenting interventions remains uncertain due to a scarcity of data from rigorous, larger studies that include ECD outcomes.
Future work in the domain of digital interventions should thus prioritize tailored approaches that actively monitor and enhance engagement for optimal outcomes. Addressing these issues will be essential for realizing the full potential of digital interventions in achieving meaningful and lasting outcomes for families.
Author Contributions
LJ: conceptualisation, investigation, formal analysis, writing–original draft; SH: conceptualisation, methodology, supervision, writing–original draft; GF: supervision, writing–review and editing, funding acquisition; DMc: supervision, writing–review and editing; MA: investigation, data curation, writing–review and editing; KH: investigation, data curation, writing–review and editing; LR-V: investigation, data curation, writing–review and editing; LA: writing–review and editing; AC: writing–review and editing; DMä: conceptualisation, methodology, supervision, writing–review and editing, funding acquisition.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This research was supported by the Basel Research Center on Child Health through the Multiple Investigator Program.
Conflict of Interest
The authors declare that they do not have any conflicts of interest.
Acknowledgments
Dr. Christian Appenzeller-Herzog, Medical Information Specialist, University Library Basel, Switzerland. Monika Wechsler, Head of Medicine, University Library Basel, Switzerland.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.ssph-journal.org/articles/10.3389/phrs.2024.1607651/full#supplementary-material
Footnotes
1http://epoc.cochrane.org/lmic-filters
2http://epoc.cochrane.org/lmic-filters
References
1. Shah, R, Camarena, A, Park, C, Martin, A, Clark, M, Atkins, M, et al. Healthcare-Based Interventions to Improve Parenting Outcomes in LMICs: A Systematic Review and Meta-Analysis. Matern Child Health J (2022) 26(6):1217–30. doi:10.1007/s10995-022-03445-y
2. Li, C, Black, MM, and Richter, L. Risk of Poor Development in Young Children in Low-Income and Middle-Income Countries: An Estimation and Analysis at the Global, Regional, and Country Level. The Lancet (2016) 4:e916–22. doi:10.1016/S2214-109X(16)30266-2
3. McCoy, DC, Peet, ED, Ezzati, M, Danaei, G, Black, MM, Sudfeld, CR, et al. Early Childhood Developmental Status in Low- and Middle-Income Countries: National, Regional, and Global Prevalence Estimates Using Predictive Modeling. Plos Med (2016) 13(6):e1002034. doi:10.1371/journal.pmed.1002034
4. Black, MM, Walker, SP, Fernald, LCH, Andersen, CT, DiGirolamo, AM, Lu, C, et al. Early Childhood Development Coming of Age: Science through the Life Course. Lancet (2017) 389(10064):77–90. doi:10.1016/s0140-6736(16)31389-7
5. Britto, PR, Lye, SJ, Proulx, K, Yousafzai, AK, Matthews, SG, Vaivada, T, et al. Nurturing Care: Promoting Early Childhood Development. The Lancet (2017) 389(10064):91–102. doi:10.1016/S0140-6736(16)31390-3
6. Jeong, J, Franchett, EE, Ramos de Oliveira, CV, Rehmani, K, and Yousafzai, AK. Parenting Interventions to Promote Early Child Development in the First Three Years of Life: A Global Systematic Review and Meta-Analysis. Plos Med (2021) 18(5):e1003602. doi:10.1371/journal.pmed.1003602
7. Lee, SH, Nurmatov, UB, Nwaru, BI, Mukherjee, M, Grant, L, and Pagliari, C. Effectiveness of mHealth Interventions for Maternal, Newborn and Child Health in Low– and Middle–Income Countries: Systematic Review and Meta–Analysis. J Glob Health (2016) 6(1):010401. doi:10.7189/jogh.06.010401
8. Till, S, Mkhize, M, Farao, J, Shandu, LD, Muthelo, L, Coleman, TL, et al. Digital Health Technologies for Maternal and Child Health in Africa and Other Low- and Middle-Income Countries: Cross-Disciplinary Scoping Review with Stakeholder Consultation. J Med INTERNET Res (2023) 25(4):e42161. doi:10.2196/42161
9. MacDonell, KW, and Prinz, RJ. A Review of Technology-Based Youth and Family-Focused Interventions. Clin Child Fam Psychol Rev (2017) 20(2):185–200. doi:10.1007/s10567-016-0218-x
10. Feroz, A, Perveen, S, and Aftab, W. Role of mHealth Applications for Improving Antenatal and Postnatal Care in Low and Middle Income Countries: A Systematic Review. BMC Health Serv Res (2017) 17(1):704. doi:10.1186/s12913-017-2664-7
11. Hall, CM, and Bierman, KL. Technology-assisted Interventions for Parents of Young Children: Emerging Practices, Current Research, and Future Directions. Early Child Res Q (2015) 33:21–32. doi:10.1016/j.ecresq.2015.05.003
12. Aboud, FE, and Yousafzai, AK. Global Health and Development in Early Childhood. Annu Rev Psychol (2015) 66:433–57. doi:10.1146/annurev-psych-010814-015128
13. Corralejo, SM, and Domenech Rodríguez, MM. Technology in Parenting Programs: A Systematic Review of Existing Interventions. J Child Fam Stud (2018) 27(9):2717–31. doi:10.1007/s10826-018-1117-1
14. Solís-Cordero, K, Duarte, LS, and Fujimori, E. Effectiveness of Remotely Delivered Parenting Programs on Caregiver-Child Interaction and Child Development: A Systematic Review. J Child Fam Stud (2022) 31(11):3026–36. doi:10.1007/s10826-022-02328-8
15. Clark, J, Glasziou, P, Del Mar, C, Bannach-Brown, A, Stehlik, P, and Scott, AM. A Full Systematic Review Was Completed in 2 Weeks Using Automation Tools: A Case Study. J Clin Epidemiol (2020) 121:81–90. doi:10.1016/j.jclinepi.2020.01.008
16. Clark, J, Sanders, S, Carter, M, Honeyman, D, Cleo, G, Auld, Y, et al. Improving the Translation of Search Strategies Using the Polyglot Search Translator: A Randomized Controlled Trial. J Med Libr Assoc JMLA (2020) 108(2):195–207. doi:10.5195/jmla.2020.834
17. Ouzzani, M, Hammady, H, Fedorowicz, Z, and Elmagarmid, A. Rayyan—a Web and Mobile App for Systematic Reviews. Syst Rev (2016) 5(1):210–0. doi:10.1186/s13643-016-0384-4
18. Balsa, A, Boo, FL, Bloomfield, J, Cristia, A, Cid, A, Ferro, M, et al. Effect of Crianza Positiva E-Messaging Program on Adult–Child Language Interactions. Behav Public Policy (2023) 7(3):607–43. doi:10.1017/bpp.2021.25
19. Bloomfield, J, Balsa, A, and Cid, A. Using Behavioral Insights in Early Childhood Interventions: The Effects of Crianza Positiva E-Messaging Program on Parental Investment. Rev Econ Househ (2023) 21(1):95–130. doi:10.1007/s11150-021-09593-4
20. Huang, L, Shen, Q, Fang, Q, and Zheng, X. Effects of Internet-Based Support Program on Parenting Outcomes for Primiparous Women: A Pilot Study. Int J Environ Res Public Health (2021) 18(9):4402. doi:10.3390/ijerph18094402
21. Le Roux, E, Eccles, R, Abdoola, S, Graham, M, and van der Linde, J. The Effect of a Parental mHealth Resource on Language Outcomes in 4- to 5-Year-Old Children. SOUTH Afr J Child Educ (2022) 12(1). doi:10.4102/sajce.v12i1.1026
22. Romski, MA, Sevcik, RA, King, M, DeLeo, G, Branum-Martin, L, and Bornman, J. Using a Self-Guided App to Provide Communication Strategies for Caregivers of Young Children with Developmental Disorders: A Pilot Investigation. J Policy Pract Intellect Disabil (2023) 20(1):73–88. doi:10.1111/jppi.12436
23. Solís-Cordero, K, Marinho, P, Camargo, P, Takey, S, Lerner, R, Ponczek, VP, et al. Effects of an Online Play-Based Parenting Program on Child Development and the Quality of Caregiver-Child Interaction: A Randomized Controlled Trial. Child Youth Care Forum (2022) 52:935–53. doi:10.1007/s10566-022-09717-6
24. Kumar, V, Mohanty, P, and Sharma, M. Promotion of Early Childhood Development Using mHealth: Learnings from an Implementation Experience in Haryana. Indian Pediatr (2021) 58(Suppl. 1):S37–S41. doi:10.1007/s13312-021-2354-8
25. Smith, JA, Chang, SM, Brentani, A, Fink, G, Lopez-Boo, F, Torino, BM, et al. A Remote Parenting Program and Parent and Staff Perspectives: A Randomized Trial. Pediatrics (2023) 151:e2023060221F. doi:10.1542/peds.2023-060221F
26. Gureje, O, Oladeji, BD, Montgomery, AA, Araya, R, Bello, T, Chisholm, D, et al. High-versus Low-Intensity Interventions for Perinatal Depression Delivered by Non-specialist Primary Maternal Care Providers in Nigeria: Cluster Randomised Controlled Trial (The EXPONATE Trial). Br J Psychiatry (2019) 215(3):528–35. doi:10.1192/bjp.2019.4
27. Mwenda, V, Makena, I, Ogweno, V, Obonyo, J, and Were, V. The Effectiveness of Interactive Text Messaging and Structured Psychosocial Support Groups on Developmental Milestones of Children from Adolescent Pregnancies in Kenya: Quasi-Experimental Study. JMIR Pediatr Parent (2023) 6(101727244):e37359. doi:10.2196/37359
28. Hamdani, SU, Minhas, FA, Iqbal, Z, and Rahman, A. Model for Service Delivery for Developmental Disorders in Low-Income Countries. Pediatrics (2015) 136(6):1166–72. doi:10.1542/peds.2015-0861
29. Westgard, CM, and Orrego-Ferreyros, LA. An mHealth Tool for Community Health Workers to Improve Caregiver Knowledge of Child Health in the Amazon: An Effectiveness-Implementation Hybrid Evaluation. PLOS Glob Public Health (2022) 2(9):e0001118. doi:10.1371/journal.pgph.0001118
30. Trude, ACB, Martins, RC, Martins-Silva, T, Blumenberg, C, Carpena, MX, Del-Ponte, B, et al. A WhatsApp-Based Intervention to Improve Maternal Social Support and Maternal-Child Health in Southern Brazil: The Text-Message Intervention to Enhance Social Support (TIES) Feasibility Study. Inq J Health Care Organ Provis Financ (2021) 58. doi:10.1177/00469580211048701
31. Lü, L, Medo, M, Yeung, CH, Zhang, YC, Zhang, ZK, and Zhou, T. Recommender Systems. Recomm Syst (2012) 519(1):1–49. doi:10.1016/j.physrep.2012.02.006
32. Hermann, E. Artificial Intelligence and Mass Personalization of Communication Content—An Ethical and Literacy Perspective. New Media Soc (2022) 24(5):1258–77. doi:10.1177/14614448211022702
33. Kabudi, T, Pappas, I, and Olsen, DH. AI-Enabled Adaptive Learning Systems: A Systematic Mapping of the Literature. Comput Educ Artif Intell (2021) 2:100017. doi:10.1016/j.caeai.2021.100017
34. Dadds, MR, Sicouri, G, Piotrowska, PJ, Collins, DAJ, Hawes, DJ, Moul, C, et al. Keeping Parents Involved: Predicting Attrition in a Self-Directed, Online Program for Childhood Conduct Problems. J Clin Child Adolesc Psychol (2019) 48(6):881–93. doi:10.1080/15374416.2018.1485109
Keywords: early child development, digital intervention, parenting, stimulation, app
Citation: Jäggi L, Hartinger SM, Fink G, McCoy DC, Alvarado Llatance M, Hinckley K, Ramirez-Varela L, Aguilar L, Castellanos A and Mäusezahl D (2025) Parenting in the Digital Age: A Scoping Review of Digital Early Childhood Parenting Interventions in Low- and Middle-Income Countries (LMIC). Public Health Rev 45:1607651. doi: 10.3389/phrs.2024.1607651
Received: 14 June 2024; Accepted: 30 December 2024;
Published: 21 January 2025.
Edited by:
Raquel Lucas, University Porto, PortugalReviewed by:
3 reviewers who chose to remain anonymousCopyright © 2025 Jäggi, Hartinger, Fink, McCoy, Alvarado Llatance, Hinckley, Ramirez-Varela, Aguilar, Castellanos and Mäusezahl. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
PHR is edited by the Swiss School of Public Health (SSPH+) in a partnership with the Association of Schools of Public Health of the European Region (ASPHER)+
*Correspondence: Lena Jäggi, bGVuYS5qYWVnZ2lAdW5pYmFzLmNo