 Rina Hariniaina Razafimahefa
Rina Hariniaina Razafimahefa Jerico Franciscus Pardosi
Jerico Franciscus Pardosi Adem Sav1
Adem Sav1- 1School of Public Health and Social Work, Faculty of Health, Queensland University of Technology, Brisbane, QLD, Australia
- 2Centre for Accident Research and Road Safety, Queensland University of Technology, Kelvin Grove, QLD, Australia
- 3School of Psychology and Counselling, Faculty of Health, Queensland University of Technology, Brisbane, QLD, Australia
Objectives: Globally, female workers workforce in Oil, Gas, and Mining (OGM) industry have increased significantly. The complexities of the OGM operations and the extensive exposure to workplace hazards potentially affect the health status of workers, including sexual and reproductive health (SRH) outcomes of female workers. Yet, the current state of knowledge on SRH issues in OGM contexts seems to be limited and fragmented. This scoping review aims to identify the occupational factors that influence women’s SRH outcomes in OGM industry.
Methods: This scoping review followed the Joanna Briggs Institute’s guidelines (PRISMA) and was conducted in five databases, including the citation chaining via Google Scholar and manual search through relevant organisations and Government websites. Sixteen articles met the inclusion criteria and were analysed.
Results: Despite the scarcity of evidence, chemical and physical are found to be the predominant factors greatly influencing women workers’ SRH outcomes in OGM. Most studies showed menstrual and cycle disorders, and risky pregnancy as key SRH issues. However, menstruation disorder was considerably linked with psychological and organisational factors.
Conclusion: This review suggests further empirical research on the relationship between OGM occupational hazards and women workers’ SRH. This will contribute to improvements in workplace safety legislations, measures, policies, and management systems taking into account women’s needs.
Introduction
The oil, gas, and mining (OGM) industry is one of most hazardous for workers. This is due to the complexity of the processes, workers’ exposure to dangerous substances, and work-related accidents [1, 2]. Despite its high-risk nature and heavy focus of males, there has been a worldwide significant increase in female workers in OGM industry [3]. For example, women represented 38% of newly hired professionals in the Exxon Mobile, and American multinational oil and gas corporations, and 31% in Shell (a British-Dutch multinational oil and gas company) in 2007 [4]. In Australia’s OGM industries, women participation has increased from 13.3% to 14.3% between 2009 and 2016, from 13.5% to 14.7% between 2011 and 2017 in European Union [3, 5]. The most significant increase has been in South Africa, from 3% to 20% between 2002 and 2019 [6].
Many women choose to work in OGM industry because of the employment opportunities, potential career advancement, higher incomes, and family health insurance [7,8]. In return, women’s participation in OGM industry has been acknowledged as a powerful contributor of companies’ economic growth and sustainable development [7, 9–13]. Research suggests because of female workers’ leadership skills and higher organisational performance in OGM industries, there has been an increase in family-friendly practices, workers’ productivity, and a reduction in both turnover and workplace risks [13–15].
Oil, Gas, and Mining Main Operations and Occupational Hazards
In OGM industry, operations are mostly undertaken under the fly-in/fly-out/drive-in/drive-out (FIFO/DIDO) system [16–18]. This practice requires long distance travel by plane or vehicle to work in remote areas during fixed period, without families. Workers are provided accommodation, food, and return travel during a limited number of days [19]. Employees work under pressure, with an inflexible work schedule, uncomfortable postures, and in noisy, hot, or cold environments, requiring strenuous physical and mental resilience [20–22]. These conditions indicate the potential exposure of OGM workers to chemical, physical, ergonomic, biological, and psychological hazards [16–18, 23–25]. As a result of exposure to such hazards, workers in OGM industry are at risk of experiencing diseases, injuries, disabilities, or fatalities. Women workers in particular are also at risk of sexual and reproductive impairment [16–18, 21, 23].
Women’s Sexual and Reproductive Health Status
Sexual and reproductive health is defined as “the state of physical, emotional, mental, and social wellbeing concerning all aspects of sexuality and reproduction, as well as concerning disease, dysfunction and infirmity” [26]. It contributes to the individual quality of life and community’s sustainable development [27]. Women’s reproductive system is complex, with specific gene function exhibiting hormonal cyclic changes to ensure fertilisation and pregnancy [28–30]. Maternal deaths, poor pregnancy outcomes, and sexual health problems, such as HIV/AIDS, still remain as global SRH key challenges, especially among women in low- and middle-income countries (LMICs) [31]. It is estimated that there are approximately 810 daily maternal deaths in 2017, 2 million stillbirth cases and 295,000 newborn deaths within 28 days of birth every year [32–34]. Stillbirth and neonatal deaths might occur due to sexually transmitted diseases (STDs) during gestational phase, such as congenital syphilis, human papillomavirus infection (HIV), chlamydia, gonorrhoea and trichomoniasis [26, 34–36]. Finally, women can also experience other forms of diseases during pregnancy and postnatal stages, including diabetes, hypertension, toxoplasmosis, rubella, urinary tract infections, obesity, and mental disorder [26, 37].
Physical Affects of Maternal Exposure to Oil, Gas, and Mining Hazards
Several studies indicate that maternal exposure to OGM hazards affects women’s physical and/or mental health, pre-conception germ cells and hormones, and foetal development [38–41]. In fact, there have been limited but concerning reports that women employed in OGM industry may experience abnormal menstruation, congenital malformation, pregnancy complications, miscarriage, stillbirth, preterm labour, low birth weight, birth defects and other gynaecological inflammation and hyperplasia [23, 41–46]. For example, research in Nigeria, Kenya, Louisiana, Ecuador, Colorado, China, Iraq, indicate the manifestation of maternal hypertensive disorders, depression, gestational diabetes mellitus, congenital anomalies associated with oil pollution and gas flaring [47–49]. Also, HIV and STD infections were identified among female miners, health care workers and communities in Latina America and the Caribbean [50]. This was mainly because of the oversupply of alcohol and drugs and sex services due to mineworkers’ high income, migration, accommodation system, family distance and communities’ poverty [50]. Female miners can be infected by having an unprotected sex with infected partner or any person working in the OGM industries or from the community.
Although numerous studies have drawn attention to the relationship between women’s work in OGM industry and their sexual and reproductive health, the current state of knowledge seems to be limited and fragmented [40–43, 51, 52]. For example, most of the literature has appeared to focus on the chemical hazards. Although chemical hazards indeed pose an important risk to women’s sexual health and reproduction, little information is available on the other categories of hazards, such as physical, biological, etc. Furthermore, focusing on chemical hazards only may limit the application of current interventions to women’s sexual health and reproduction issues due to the wide variety in OGM workplaces in terms of technology, work processes and organisations [26, 40, 41, 43, 51–53]. Hence, the crucial first stage in understanding the how the OGM industry affect women’s sexual and reproductive health is to scope the body of literature. This will assist health professionals and policy makers with developing the most efficient workplace health and safety strategies to reduce the risk of sexual and reproductive health issues among working women in such a high-risk industry.
Finally, a review of female workers’ sexual and reproductive health issues in OGM industries is timely given that 70% of female workers in OGM industry are 20–54 years old globally [54–56]. This suggests that most women working in OGM industry are within childbearing age period. Nevertheless, considering the decline of women’s fertility after the age of 32, their pregnancy plans and reproductive health status could be threatened [57–59]. Women’s participation in the workforce Employment and their decisions to delay pregnancy are argued to be among the causes of this SRH issue [27, 60–64].
The aim of this study is to review the current evidence to understand the occupational factors affecting sexual and reproductive health status among female workers in OGM industry. Although we use a systematic process to search for literature, our aim is not to assess the quality of this body of literature, which is conducted in a systematic review. Instead, we map the literature, and identify the gaps, and incite future research for a scientific-based knowledge about this field and a gendered-based health and safety management system, policies, and practices.
Methods
This scoping review, which was guided by the principles established by Arksey and O’Malley, was conducted from July to August 2020 [65]. We followed Joanna Briggs Institute’s Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA_ScR checklist) as shown in Supplementary Appendix S1 [66, 67]. The searches of articles from 2000 to 2019 were undertaken in five relevant databases, including CINAHL, Embase, PubMed, Scopus, Web of Science as shown in Supplementary Appendix S2. The search terms focused on Population, Exposure and Outcomes elements as presented in Table 1.

TABLE 1. Search terms used for the searches (Queensland, Australia. 2020).
Additional citation chaining in Google Scholar, hand searching and browsing organisations and government websites were performed [1, 3, 33, 34, 68, 69]. This is mainly to generate more relevant articles and avoid missing significant evidence that would provide more comprehensive findings to the review. During the literature search, the authors also received assistance from a librarian.
All studies were exported into Endnote X9 citation management software [70] and screened for eligibility based on the following inclusion criteria: articles investigating female workers, sexual and reproductive issues, occupational hazards, large-scale OGM industry considering other associated operations, such as manufacturing and transport, primary data. Primary data included qualitative, quantitative, mixed method, textual papers, reviews, and grey literature, published and unpublished studies. Studies: published prior to year 2000, without full-text, in non-English languages, based on animal experiments, involving solely male workers or female community populations, focussed on non-occupational factors or non SRH diseases, safety hazards and risks, policies, interventions or treatment investigations, in industries other than OGM, small-scale mining, and OGM marketing activity were excluded. Female community was excluded due to the study focus on workers and their low exposure to the mining activities. Additionally, as the review was operational in focus, studies that concentrated on commercial and marketing activities in OGM were excluded.
Included studies were extracted by the first author using the inclusion criteria. The extracted studies were sorted in a charting table (Table 1), which included information on the author(s), year of publication, countries, objectives, study design, sample size, OGM types, occupational factors, sexual and reproductive status outcomes, and summary of the key findings. The results were thematically analysed and collated within six key themes of occupational factors.
Results
The scoping review initially identified 1,038 studies (Figure 1) and sixteen were included in the final analysis (see Table 2).
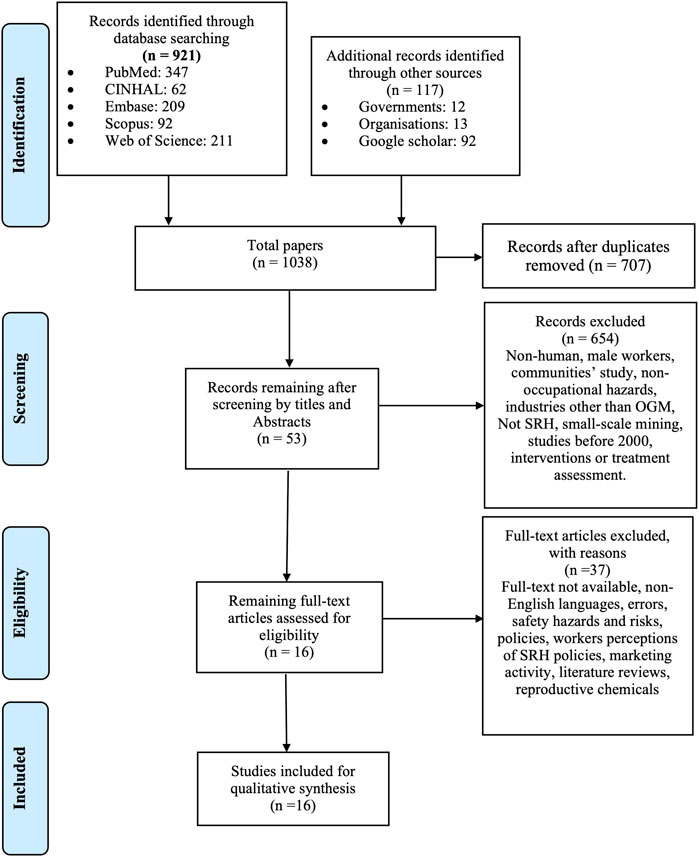
FIGURE 1. PRISMA flow diagram (Queensland, Australia. 2020).
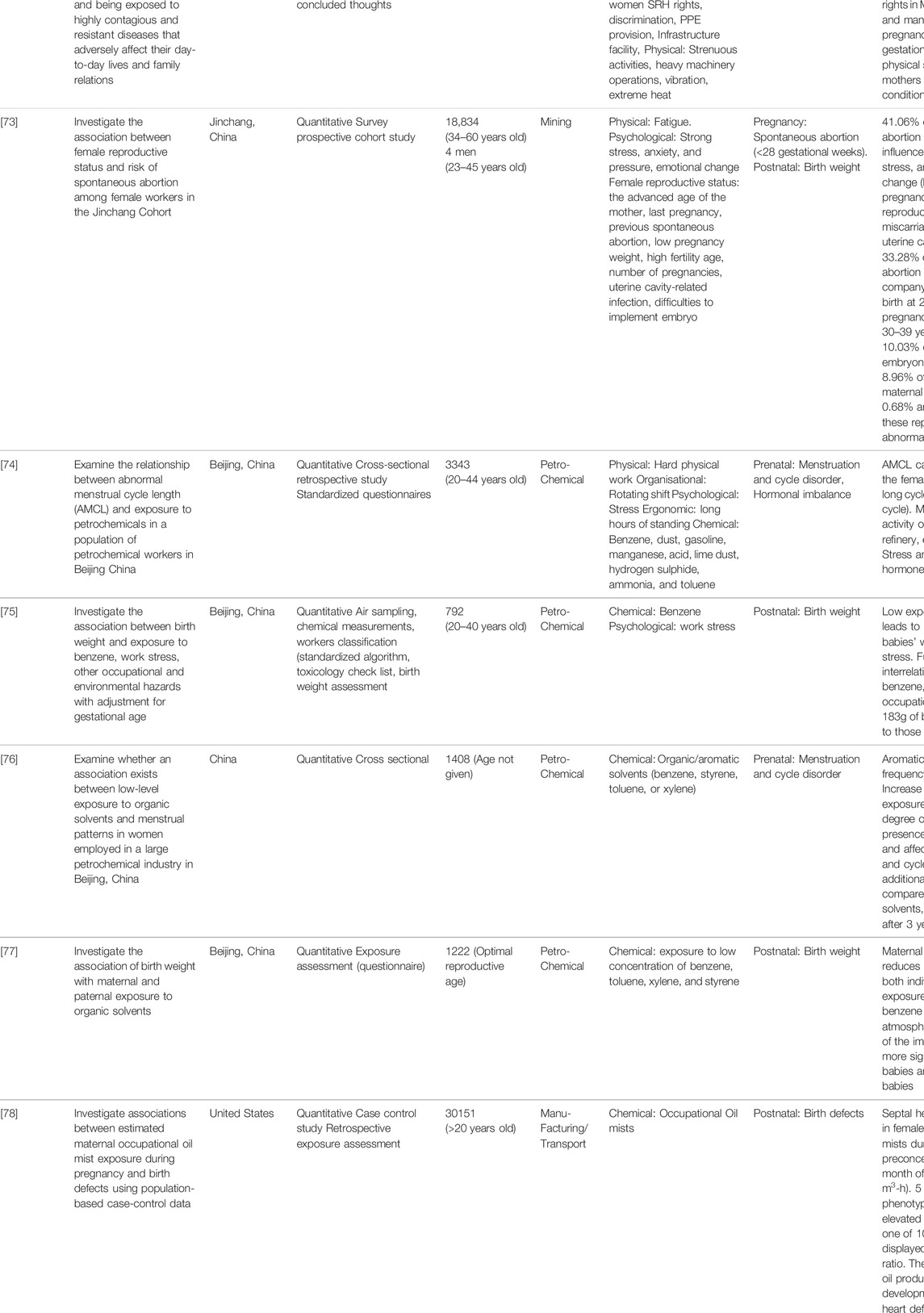
TABLE 2. Data extraction of included studies (Queensland, Australia. 2020).
Study Characteristics
This review has utilised 15 published articles and one unpublished source. Eight of the 16 studies used a quantitative research method with sample sizes ranging from 792 to 3,343 for the petrochemical operations, and 1,035 to 44,000 for the mining [71–78]. Three studies applied qualitative research methods, often combined with a literature review and empirical investigation, with all participants coming from mining [79–81]. Two other studies in mining applied a mixed methods with 156–686 respondents [72, 81–83]. Two other studies were transaction and conference papers which examine the OHS in the mining industry in South Africa [84, 85]. Transaction paper refers to a paper that meets the requirements of a conference paper. These two articles are constituted of general information without clear description of the methods. However, both met the inclusion criteria of this scoping review and fostered a balanced picture of available evidence relating to the scope of the review. Studies were conducted in both developed and developing countries, such as South Africa [71, 79–82, 84–86]; Australia [80, 83]; China [74–77] Indonesia [72] and the United States [78]. Those in South Africa, Australia, and Indonesia focused on mining, whereas those in China were based on the petrochemical industry. The studies in South Africa were related to mining activities [71, 79, 81, 82, 84–86]. The one study in the United States investigated the risks of female SRH by exposure to hydrocarbon oil mists in manufacturing and transport activities [78].
Eleven studies focused on the mining industry, which generally involved work underground and constituted of exploration, quantification, extraction, and processing of different minerals [71–73, 79–86]. These included, iron, ore, coal, gold, copper, aluminium, nickel, zinc, platinum, gold, hard rock, phosphate [71–73, 79–86]. Four studies on petrochemical focused on plants operating, processing and refinery [74–77]. One study investigated exposure to occupational oil mists from manufacturing and transport in the United States [78].
Occupational Factors of Sexual and Reproductive Health in Oil, Gas, and Mining Industry
The thematic analysis identified six occupational factors, which potentially affected sexual and reproductive health status among female workers in OGM industry. These factors were: biological, chemical, ergonomic, physical, psychological, and organisational (Figure 2). Within women’s reproductive lifecycle period, precisely for pre to postnatal, chemical hazards posed the most significant threat to sexual and reproductive health, particularly during the intrapartum phase (Figure 2). However, ergonomic, physical, and psychological hazards were also harmful during the intrapartum and prenatal stages.
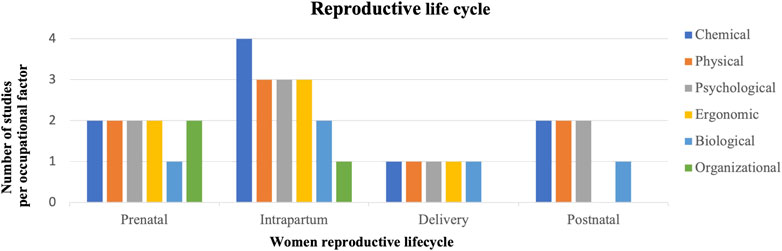
FIGURE 2. Predominant occupational factors in women’s reproductive life cycle (Queensland, Australia. 2020).
Sexual and Reproductive Disorders in Oil, Gas, and Mining Industry
Based on the 16 included studies, Table 3 shows the sexual and reproductive health characteristics experienced by women workers in OGM industry, ranging from infertility to sexual violence.
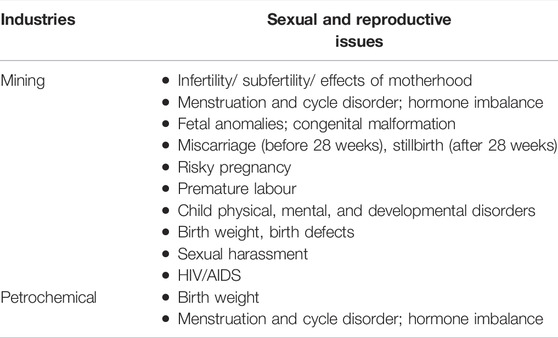
TABLE 3. Sexual and Reproductive Health Characteristics in Oil, Gas and Mining industry (Queensland, Australia. 2020).
Female workers in OGM industry experienced poor sexual and reproductive health outcomes during either prenatal or intrapartum stages [68, 70-73, 76, 78-79, 81] compared with delivery and postnatal periods [71, 76, 80, 87] (Supplementary Appendix S3). Chemical and physical hazards were the most dangerous occupational factors affecting sexual and reproductive health outcomes among female workers in OGM industry (Supplementary Appendix S3) [71, 74–79, 84, 85]. The geographic analysis of the 16 studies revealed a concentration of research in South Africa for the mining industry and in China for the petrochemical industry. Two studies discussed sexually motivated physical and psychological harassment or intimidation, generally linked to organisational factors, which promoted gender discrimination and male dominance [79, 85]. Four studies into African and Indonesian mining reported HIV/AIDS cases among female workers [72, 84–86]. The seroprevalence survey performed in South Africa, Botswana, Zambia disclosed a significant rate of HIV/AIDS among women of different age groups, especially the unskilled and semi-skilled workers (14.6% between 20 and 29 years old, 14.9% between 30 and 39 years and 4.5% between 40 and 49-years [86].
Key Themes on Occupational Factors and Women’s Sexual and Reproductive Health
Biological
Biological factors were the least discussed in the included studies. In fact, only one conference report of South African Institute of Mining and Metallurgy Hard Road Safety in 2009 discussed exposure of female workers in hard rock mining to various biological hazards, such as cytomegalovirus, hepatitis, HIV, rubella, varicella, Toxoplasma gondii [85]. This report highlighted that exposure to these microorganisms was associated with menstruation and cycle disorder, teratogenesis, gene mutation, pregnancy complications, miscarriage, stillbirth, preterm birth, and other development-related abnormalities in foetal and children [85].
Organizational
Five studies identified organisational factors as influencing female workers sexual and reproductive health in mining [79, 80, 82, 83]. Most were qualitative and found risky pregnancy and menstruation and cycle disorders as the main sexual and reproductive health concerns [71–73,75, 86]. Some of the organisational factors affecting sexual and reproductive health were FIFO/DIDO system-related schedule and gender discrimination in Australia, racist and discriminative management and policies, and violence in South Africa. For instance, women in South Africa Mining preferred to hide their pregnancy to secure their job [81]. Female black South African miners felt disadvantaged as they were not re-allocation to light duties during pregnancy compared to their white counterparts [79]. In Australia, women of childbearing age complained about their difficulties to have a proper work-life balance due to FIFO/DIDO system and its long, inflexible work hours [83].
Chemical
Nine studies showed chemical factors affected female workers’ sexual and reproductive health status [71, 74–79, 84, 85]. Some of the chemical hazards reported included organic and inorganic solvents in the five petrochemical quantitative studies in China and United States [75–78] and heavy metals, toxic gases and dust, pesticide, alcohol, and tobacco smoke in the four studies on South Africa mining studies [71, 79, 84, 85]. For example, Badenhorst and Platinum (2009) report that the exposure to lead can affect women miners’ pregnancy at early stages (8–10 weeks) by crossing the placenta and damaging the foetus [85].
Physical
Physical factors associated with sexual and reproductive health among female workers in OGM industry was also identified in eight of the papers [71, 73, 74, 79, 81, 82, 84, 85]. Menstruation and cycle disorders and risky pregnancy were recognised to be triggered by physical factors. For example, a study by Calitz (2004) found South African female miners suffer from painful menstrual periods due to their exposure to the underground mining hot or cold environments [79]. Six studies in South Africa pointed out the different physical hazards involving radiation, heat, noise and vibration, mechanical shocks, physical strain, male-designed tools and equipment [71, 79, 82, 84, 85]. While the physical factors influencing menstruation disorders and miscarriage in the petrochemical industry were physical exertion and fatigue, caused by strenuous activities, prolonged standing, long working shift, heavy equipment vibration and underground heat stress [74, 75].
Ergonomic
Ergonomic factors adversely impacted women’s sexual and reproductive health in five studies, particularly risky pregnancy [74, 79, 82, 85]. Three qualitative research and reports related to South Africa mining suggested that women have difficulties to use the existing equipment, including the working environment, which might affect their sexual and reproductive health status [71, 80, 86]. For example, Zungu (2011) highlights that the constant use of oversized and heavy tools and equipment, manual handling and lifting activities, and other ranges of motions cause stress and fatigue affecting hormone levels, fluid balance, and reducing fertility [71].
Psychological
Psychological factors influenced sexual and reproductive health in six studies [71, 73–75, 79, 85]. Menstrual disorders and risky pregnancy were the main consequences of workplace stress, anxiety, and depression. Studies from South Africa detailed male harassment, gender discrimination, and work-life imbalance, which led to stress, frustration, and pressure among female workers [71, 73, 79, 85]. In contrast, the quantitative studies in China’s petrochemical operation found workplace stress as the outcomes of strenuous physical activities, long hours of standing, and an inflexible work schedule [74, 75].
Discussion
This scoping review demonstrates the scarcity of global research on the influence of occupational factors on female workers’ sexual and reproductive health outcomes in OGM industry. Nevertheless, the geographic analysis suggests a concentration of the research mainly in low-and middle-income countries. This could be aligned with the amendment of policies and legislation promoting women’s employment and gender equality in South Africa mining [87] and the significant economic profits generated by the petrochemical industry in China [88, 89]. Despite being limited, the findings show that chemical and physical hazards could be considered as potential risk factors for sexual and reproductive health disorders among women workers in OGM industry. The included studies suggest menstrual and cycle disorders due to chemical hazards, such as heavy metals, toxic gases, and dust. Similar findings were also reported in other industries, such as plastic, agriculture, health care, waste management and construction where chemical hazards are detrimental factors to women’s sexual and reproduction system [90–94]. Hence, this study adds to the growing body of evidence of the detrimental impact of chemic hazards on women’s sexual and reproduction system.
Menstruation and cycle disorders were also negatively affected by physical factors, such as heat, noise, dust, and physically demanding work activities also placed pregnancy at risk [71, 74, 79, 82, 85]. This is in line with literature, which suggests that strenuous exercise during pregnancy can have negative physiological outcomes, such as hormonal imbalance, vasoconstriction, myometrial contraction, reduced plasma volume, and diversion of blood flow away from the placental bed causing foetal hypoxia [95]. In addition, there is evidence to suggest that poor work organisation can adversely affect menstruation and pregnancy in OGM industry [74, 79, 81, 82, 85]. For example, an occupational health-related study indicates that shift work and irregular work schedules in different industries can change women’s circadian rhythm causing menstrual irregularities and pregnancy complications, such as gestational hypertension, preterm delivery, small for gestational age baby and preeclampsia [95]. This has been observed in a few women working in petrochemical engineering, medical industry, and metallurgy with a high proportion of abnormal periods, reproductive system infection and infertility [96].
Psychological factors are also reported to be associated with menstruation and cycle disorders, including stress, anxiety, constant feeling of fear and pressure due to the strenuous physical work and male counterparts’ harassment [71, 73–75, 79, 85]. This is concerning as OGM activities are recognised as stressful in both developed and developing countries; however, no studies clearly investigate its association with female sexual and reproductive health status [97–99]. Existing studies in the mining industry were based on reports or qualitative self-reported methods that rely on the participants’ experience and their perceptions on the psychological factors relating to sexual and reproductive health issues [71–73, 79–86]. In contrast, those in the petrochemical industry applied quantitative measures and analysis [74–77]. This disregards women workers’ opinions and experience of their working conditions and the health and safety outcomes in the petrochemical industry. Besides, it excludes other types of occupational hazards that can affect their SRH.
Existing studies on organisational factors of sexual and reproductive health disorders in OGM industry mostly used qualitative methods or reports in which female workers’ perceptions and experiences in underground mining are explored [74, 79–83, 85]. However, research suggests that employers’ leadership and duties towards employees’ health and wellbeing are the fundamental keys that need to be investigated through legislation, policies, organisation culture and management systems [100]. Laws, regulations, and organisational health and safety management systems are powerful tools to influence safety leadership, preventive culture, and workers’ positive behaviour and commitment that mitigate the risks of exposure to workplace hazards [101–105].
Concerning the physical factors, this scoping review found that body stress, heavy tools, illumination, heat, heights, noise, vibration, electromagnetic radiation, ventilation pressure potentially harm female workers sexual and reproductive health in the mining industry [71, 74, 79, 82, 85]. These physical hazards are perceived as less harmful than chemical hazards in oil and gas industry and have been underrated because of their chronic effects on individual health [106]. Hence, workers are largely unaware of these hazards and the severity of the risks [106]. Different investigations confirmed that physical hazards can cause chronic diseases and mortality, involving sexual and reproductive health issues [106–110]. This is due to fatigue, stress, pain, body mechanism disorders and damage of the internal organs and tissues [106–110].
The findings of this scoping review suggest a hostile working environment for women, including organisational structure, management systems, practices, and facilities in OGM industry [71,74,79,85]. For example, the male-designed ablution facilities, change houses and bathrooms without privacy, ill-fitting personal protective clothing, machinery and equipment, heavy tools, social environment of male hostility, violence, and sexual assaults [71, 74, 75, 79, 85]. These circumstances subsequently affect women’s psychological state due to the lack of comfortability and the stress, anxiety, or frustration they experience. The selected studies reveal the development of stress and anxiety as a result of organisational and physical factors involving strenuous work, gender discrimination, work-life balance, and harassment [71, 73–75, 79, 80]. Other studies also highlight different issues affecting women’s psychology in OGM industry, including professional and social isolation, loneliness, women’s identity on masculinity, and uncompromising supervisors [111–113]. Hence, further research is needed to investigate industries’ management and organisational system, including policies, programs, and implementation, to address such circumstances and recommend implementable strategies that promote women’s health and wellbeing.
Finally, a few cases of HIV/AIDS among female workers in OGM industry have been reported in several included studies [84–86]. Men were claimed to be the source of transmission [85]. However, this claim requires further investigation and empirical evidence as this statement is obtained from a report with limited scientific study. Studies also raise the issues of underreported HIV/AIDS cases at the workplace to prevent stigma [114–116].
Implications for Future Research
The findings of this scoping review have several implications for future research. Firstly, future research should consider quantitative research methods to obtain high quality evidence of the relationship between occupational hazards and female workers’ sexual and reproductive health. Longitudinal research designs to better establish the causal relationship between exposure to occupational hazards and female workers’ sexual and reproductive health would be valuable. Additionally, new studies should consider the analysis of legislation, policies and programs related to gender diversity and women’s health in developed and developing countries, and across OGM industry to help understand its effects on the organisational culture and management of female sexual and reproductive health status. Also, future studies should identify all potential biological, chemical, and environmental health hazards, particularly air and water pollutants, which are often found in OGM industry. Environmental health hazards including heavy metals, carbon monoxide, nitrogen oxide, sulfur dioxide and particulate matter can be detrimental to women’s reproductive system [105, 117–122]. Yet, this scoping review has shown that there is very little research and knowledge on these hazards. The consideration of women’s differences in biological, physiological characteristics, and physical capacities in research and workplace risk assessment is also needed and justified by other researchers [123,124]. This is crucial for a specific and effective control of health and safety concerns of women in OGM industry. The combination of the epidemiologic studies, ergonomic assessment checklist tools and medical examination is needed to ensure the accuracy of the investigation [19]. From the psychological factor perspectives, future studies should consider occupational mental health and wellbeing, particularly in the developing countries where mental health issues are still perceived as Western luxury or religious-based punishment [125]. Finally, future research should include HIV/AIDS and sexual health in OGM industry to investigate the source and magnitude of the risks and develop preventive and reactive strategies and programs.
The findings also have managerial, policy and practical implications. In addition to the potential of exposure to multiple hazards in OGM industry, there are specific health issues that manifest exclusively in women requiring thorough investigation and control measures. Moreover, women in OGM industry are reported to endure various forms of gender inequality, including discriminatory policies and practices, violence, sexual harassment due to the persistent traditional male norms. These unfair situations still occur in the workplace because women’s employment concerns remain overlooked in the industry’s investigations [126]. Considering the economic benefits of increasing women’s workforce participation in the industries, promoting a female friendly workplace appears to be crucial [127]. It consists of developing organisational and managerial policies and practices that respond to women’s special needs. Studies should therefore be conducted to investigate the current policy making, organisational structures, management systems and practices in OGM industry and identify their suitability to women’s health, safety, and wellbeing. Some of the specific strategies to support women may include policies, hazards identification, risk assessments control strategies and interventions which pose a risk to their health and wellbeing. Human resources management systems, including recruitment processes, resources provision, development opportunities, and organisation’s policies and practices that support work-life balance for female employees could also be implemented [127–131]. However, future research is needed to more coherently identify which of these strategies women may find most beneficial to their career advancement.
Limitations
This scoping review has few limitations. Firstly, it did not cover gynaecological and breast cancers, which are also part of women’s sexual and reproductive health issues Secondly, since there was no evaluation of the quality of the included studies in this scoping review, the accuracy and validity of the findings remain controversial and require thorough scientific research. Nevertheless, all expected occupational factors relating to women’s SRH were identified in the relevant studies. Additionally, because our review was restricted to English language articles, we may have missed key articles in non-English. This scoping review also exhibited heterogenous SRH characteristics among female workers in OGM industry.
Conclusion and Future Research
Research on occupational factors influencing sexual and reproductive health status among women workers in OGM industry is scarce and limited. Nevertheless, the included studies display various sexual and reproductive health issues throughout women reproductive lifecycle periods (prenatal, intrapartum, delivery, and postnatal) as the results of the exposure of OGM occupational hazards. Chemical and physical hazards were found to have substantial effects on women workers SRH in OGM industry, while menstrual and cycle disorders and risky pregnancy are the major SRH health concerns. Recognising the lack of quality assessment of the included studies, the accuracy and the validity of the findings and interpretation are constrained. However, this review is a preliminary step to inform about the key characteristics and occupational factors of SRH in OGM industry, as mapped in the literature. Empirical studies are recommended for an evidence-based decision making, initiatives, policies, and practices promoting a gender-based human resources and health and safety management systems in OGM industry.
Author Contributions
All authors participated in designing the study and the interpretation of the findings from the included studies. RR developed the review protocol, carried out the search activities, and drafted the manuscript. JP reviewed studies as part of the screening and eligibility stages, reviewed, and edited the manuscript. AS reviewed and edited the manuscript. All authors read and approved the final manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.ssph-journal.org/articles/10.3389/phrs.2022.1604653/full#supplementary-material
References
1. Abrahamsson, L, Segerstedt, E, Nygren, M, Johansson, J, Johansson, B, Edman, I, et al. Gender, Diversity and Work Conditions in Mining, Mining and Sustainable Development. Lulea University of Technology (2014). p. 8–17.
2. Fernandez-Stark, K. Background Paper for WBG-WTO Global Report on Trade and Gender: How Can 21st century Trade Help to Close the Gender gap? (2019). Available from: http://documents1.worldbank.org/curated/ar/824061568089601224/pdf/Background-Paper-for-WBG-WTO-Global-Report-on-Trade-and-Gender-How-can-Twenty-First-Century-Trade-Help-to-Close-the-Gender-Gap-Industry-4-0-in-Developing-Countries-The-Mine-of-the-Future-and-the-Role-of-Women.pdf (Accessed August 20, 2020).
3.The advocates for human rights. Promoting Gender Diversity and Inclusion in the Oil, Gas and Mining Extractive Industries. A Women’s Human Rights Report (2019). Available from: https://www.unece.org/fileadmin/DAM/energy/images/CMM/CMM_CE/AHR_gender_diversity_report_FINAL.pdf (Accessed August 20, 2020).
4. Feltus, A. Women in Energy: Closing the Gender gap. WPC (2017). Available from: https://www.world-petroleum.org/docs/docs/wpc_women.pdf (Accessed September 30, 2020).
5.Catalyst. Women in Energy – Gas, Mining, and Oil: Quick Take (2019). Available from: https://www.catalyst.org/research/women-in-energy-gas-mining-oil/ (Accessed July 23, 2020).
6. Minerals council South Africa, . Making Mining Matter. Facts and Figures Pocketbook 2019 (2019). Available from: https://www.mineralscouncil.org.za/industry-news/publications/facts-and-figures (Accessed August 15, 2020).
7. Pimpa, N. How Mining Companies Promote Gender equality through Sustainable Development? Cogent Business Management (2019) 6(1):1647590. doi:10.1080/23311975.2019.1647590
8. McKee, LE. Women in American Energy: De-feminizing Poverty in the Oil and Gas Industries. J Int Women's Stud (2014) 15(1):167–78.
9.Worldbank group. Women’s Employment in the Extractive Industry (2015). Available from: https://olc.worldbank.org/system/files/WB_Nairobi_Notes_2_RD3.pdf (Accessed August 7, 2020).
10.UNDP. Mapping the Oil and Gas Industry to the Sustainable Development Goals: An Atlas. Sustainable Development Goals (2017).
11. Minerals council of Australia, . Workplace Gender equality agency, Case Study: Attracting Women to a Male-Dominated Industry. Australian Government (2018). Available from: https://minerals.org.au/sites/default/files/st%20barbara%20case%20study%20web.pdf (Accessed July 23, 2020).
12.APEC. Women's Participation in the Mining Industry: APEC Policy Partnership on Women and the Economy. [cited 2019 Dec 1] (2019). Available from: file:///Users/rinarazafimahefa/Downloads/219_PPWE_APEC%20Womens%20Participation%20in%20the%20Mining%20Industry%20(2).pdf (Accessed August 11, 2020).
13. Doku, L. Why the Mining Industry Needs More Women (2019). Available from: https://www.forbes.com/sites/woodmackenzie/2019/05/24/why-the-mining-industry-needs-more-women/?sh=38576f45585c (Accessed September 30, 2020).
14. Turner, J. How Do We Decrease the Gender gap in the Oil and Gas Industry? (2018). Available from: https://www.nsenergybusiness.com/news/women-in-oil-and-gas/ (Accessed August 27, 2020).
15.Quora Contributor. Why Are Fewer Women Employed in the Oil and Gas Industry than Men? (2019). Available from: https://www.forbes.com/sites/quora/2019/03/08/why-are-fewer-women-employed-in-the-oil-and-gas-industry-than-men/?sh=296b8d3c6033 (Accessed August 15, 2020).
16. Niven, K, and McLeod, R. Offshore Industry: Management of Health Hazards in the Upstream Petroleum Industry. Occup Med (2009) 59(5):304–9. doi:10.1093/occmed/kqp076
17. Daley, J. Game-changers: Economic Reform Priorities for Australia (2012). Available from: https://grattan.edu.au/wp-content/uploads/2014/04/Game_Changers_Web.pdf (Accessed August 9, 2020).
18. Bowers, J, Lo, J, Miller, P, Mawren, D, and Jones, B. Psychological Distress in Remote Mining and Construction Workers in Australia. Med J Aust (2018) 208(9):391–7. doi:10.5694/mja17.00950
20. Devold, H. Oil and Gas Production Handbook: An Introduction to Oil and Gas Production. Lulu. Com (2013) (Accessed August 19, 2020).
21.Doctors for the Environment Australia. The Implications for Human Health and Wellbeing of Expanding Gas Mining in Australia: Onshore Oil and Gas Policy Background Paper (2018). Available from: https://www.dea.org.au/wp-content/uploads/2018/12/DEA-Oil-and-Gas-final-28-11-18.pdf (Accessed August 19, 2020).
22. Elsevier, BV. Mineral Extraction. Science Direct (2019). https://www.sciencedirect.com/topics/earth-and-planetary-sciences/mineral-extraction (Accessed August 20, 2020).
23.CCSG Associates Canada. Overburdened: Understanding the Impacts of mineral Extraction on Women’s Health in Mining Communities (2004). https://miningwatch.ca/sites/default/files/Overburdened_0.pdf? (Accessed August 20, 2020).
24. Donoghue, AM. Occupational Health Hazards in Mining: an Overview. Occup Med (2004) 54(5):283–9. doi:10.1093/occmed/kqh072
25. Dorman, SC, and Boudreau-Lariviere, C. Guide to Healthy Pregnancies in the Mining Workplace. A Laurentian University & Workplace Safety North Initiative (2012). http://crosh.ca/wp-content/uploads/2017/06/HealthyPregMiningWorkplace_Feb2012.pdf (Accessed August 15, 2020).
26. Starrs, AM, Ezeh, AC, Barker, G, Basu, A, Bertrand, JT, Blum, R, et al. Accelerate Progress-Sexual and Reproductive Health and Rights for All: Report of the Guttmacher- Lancet Commission. The Lancet (2018) 391(10140):2642–92. doi:10.1016/s0140-6736(18)30293-9
27. Gutiérrez-Domènech, M. Employment after Motherhood: a European Comparison. Labour Econ (2005) 12(1):99–123. doi:10.1016/j.labeco.2004.04.004
28.ML Pardue, and TM Wizemann, editors. Exploring the Biological Contributions to Human Health: Does Sex Matter? Washington (DC): National Academies Press (2001).
29. Wu, BN, and O'Sullivan, AJ. Sex Differences in Energy Metabolism Need to Be Considered with Lifestyle Modifications in Humans. J Nutr Metab (2011) 2011:391809. doi:10.1155/2011/391809
30. Thiyagarajan, DK, Basit, H, and Jeanmonod, R. Physiology, Menstrual Cycle. StatPearls [Internet] (2019). Available from: https://www.ncbi.nlm.nih.gov/books/NBK500020/ (Accessed April 15, 2021).
31.World Health Organisation. Sexual Health and its Linkages to Reproductive Health: An Operational Approach (2017). Available from: https://www.who.int/reproductivehealth/publications/sexual_health/sh-linkages-rh/en/ (Accessed April 15, 2021).
32.United Nations Children’s Fund (UNICEF). A Neglected Tragedy: The Global burden of Stillbirths Report of the UN Inter-agency Group for Child Mortality Estimation (2020). Available from: https://thedocs.worldbank.org/en/doc/845141602114822604-0090022020/original/AneglectedtragedystillbirthsIGMEreportEnglish2020.pdf (Accessed February 12, 2021).
33.World Health Organisation. Congenital Anomalies (2020). Available from: https://www.who.int/news-room/fact-sheets/detail/congenital-anomalies (Accessed October 14, 2020).
34.World Health Organisation. Maternal Mortality (2019). Available from: https://www.who.int/news-room/fact-sheets/detail/maternal-mortality (Accessed February 12, 2021).
35. de Sanjosé, S, Diaz, M, Castellsagué, X, Clifford, G, Bruni, L, Muñoz, N, et al. Worldwide Prevalence and Genotype Distribution of Cervical Human Papillomavirus DNA in Women with normal Cytology: a Meta-Analysis. Lancet Infect Dis (2007) 7(7):453–9. doi:10.1016/s1473-3099(07)70158-5
36. Korenromp, EL, Rowley, J, Alonso, M, Mello, MB, Wijesooriya, NS, Mahiané, SG, et al. Global burden of Maternal and Congenital Syphilis and Associated Adverse Birth Outcomes-Estimates for 2016 and Progress since 2012. PLoS One (2019) 14(2):e0211720. doi:10.1371/journal.pone.0211720
37.Centers of Disease Control and Prevention (CDC). Pregnancy Complications (2020). Available from: https://www.cdc.gov/reproductivehealth/maternalinfanthealth/pregnancy-complications.html (Accessed October 14, 2020).
38. Lindbohm, M-L, and Taskinen, H. Reproductive Hazards in the Workplace. Women’s Health (2000). p. 463–73. doi:10.1016/b978-012288145-9/50043-7
39. Valsamakis, G, Chrousos, G, and Mastorakos, G. Stress, Female Reproduction and Pregnancy. Psychoneuroendocrinology (2019) 100:48–57. doi:10.1016/j.psyneuen.2018.09.031
40. Brzoza, R, and Swiadro, J. Incidence of Congenital Spinal Anomalies and Their Effect on Morbidity in Miners. Pol Tyg Lek (1960) 28(18):642–6.
41. Bolden, AL, Schultz, K, Pelch, KE, and Kwiatkowski, CF. Exploring the Endocrine Activity of Air Pollutants Associated with Unconventional Oil and Gas Extraction. Environ Health (2018) 17(1):26–7. doi:10.1186/s12940-018-0368-z
42. Figà-Talamanca, I. Occupational Risk Factors and Reproductive Health of Women. Occup Med (2006) 56(8):521–31. doi:10.1093/occmed/kql114
43. Xu, X, Cho, SI, Sammel, M, You, L, Cui, S, Huang, Y, et al. Association of Petrochemical Exposure with Spontaneous Abortion. Occup Environ Med (1998) 55(1):31–6. doi:10.1136/oem.55.1.31
44. Gold, EB, and Tomich, E. Occupational Hazards to Fertility and Pregnancy Outcome. Occup Med (1994) 9(3):435–69.
45. Mactaggart, F, McDermott, L, Tynan, A, and Whittaker, M. Exploring the Broader Health and Well-Being Outcomes of Mining Communities in Low- and Middle-Income Countries: A Systematic Review. Glob Public Health (2018) 13(7):899–913. doi:10.1080/17441692.2016.1240821
46. Deziel, NC, Brokovich, E, Grotto, I, Clark, CJ, Barnett-Itzhaki, Z, Broday, D, et al. Unconventional Oil and Gas Development and Health Outcomes: A Scoping Review of the Epidemiological Research. Environ Res (2020) 182:109124. doi:10.1016/j.envres.2020.109124
47. Duydu, Y, Başaran, N, Üstündağ, A, Aydın, S, Yalçın, CÖ, Anlar, HG, et al. Birth Weights of Newborns and Pregnancy Outcomes of Environmentally boron-exposed Females in Turkey. Arch Toxicol (2018) 92(8):2475–85. doi:10.1007/s00204-018-2238-4
48. Kou, ZX, Wang, SL, Chen, ZL, He, YH, Yu, WL, Mei, LY, et al. Influencing Factors for Reproductive Health of Female Workers in Petrochemical Industry. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi (2018) 36(2):139–43. doi:10.3760/cma.j.issn.1001-9391.2018.02.016
49. Oghenetega, OB, Ana, GR, Okunlola, MA, and Ojengbede, OA. Oil Spills, Gas Flaring and Adverse Pregnancy Outcomes: A Systematic Review. OJOG (2019) 10(1):187–99.
50. Wilches-Gutierrez, J, and Documet, P. What Is Known about Sexual and Reproductive Health in Latin American and Caribbean Mining Contexts? A Systematic Scoping Review. Public Health Rev (2018) 39(1):1–3. doi:10.1186/s40985-017-0078-z
51. Simeonova, M, Georgieva, V, and Alexiev, C. Cytogenetic Investigations of Human Subjects Occupationally Exposed to Chemicals from the Petroleum-Processing Industry. Environ Res (1989) 48(2):145–53. doi:10.1016/s0013-9351(89)80030-1
52. Balise, VD, Meng, C-X, Cornelius-Green, JN, Kassotis, CD, Kennedy, R, and Nagel, SC. Systematic Review of the Association between Oil and Natural Gas Extraction Processes and Human Reproduction. Fertil Sterility (2016) 106(4):795–819. doi:10.1016/j.fertnstert.2016.07.1099
53. Cameron, PD, and Stanley, MC. Oil, Gas, and Mining: A Sourcebook for Understanding the Extractive Industries. International Bank for Reconstruction and Development/ The World Bank (2017). Available from: https://openknowledge.worldbank.org/bitstream/handle/10986/26130/9780821396582.pdf?sequence=2&isAllowed=y (Accessed August 08, 2020).
54.Australia Government-Department of Employment. Labour Market Research and Analysis Branch. Industry Outlook – Mining (2014). Available from: https://cica.org.au/wp-content/uploads/2014-Mining-Industry-Employment-Outlook.pdf (Accessed July 15, 2020).
55.Oil and gas UK. WORKFORCE REPORT (2018). Available from: https://oilandgasuk.co.uk/wp-content/uploads/2019/03/OGUK-Workforce-Report-2018.pdf (Accessed July 15, 2020).
56.U.S Bureau of Statistics. Labor Force Statistics from the Current Population Survey. Household Data Averages (2020). Available from: https://www.bls.gov/cps/cpsaat18b.htm (Accessed August 05, 2020).
57. Blatstone, T, Berry, E, Cole, D, Crowe, K, Deller, N, Howson, T, et al. Workplace Reproductive Health Research & strategiesOntario’s Maternal Newborn and Early Child Development Resource Centre (2001). p. 1–74. Available from: https://www.beststart.org/resources/wrkplc_health/pdf/WorkplaceDocum.pdf (Accessed August 09, 2020).
58. Spandorfer, S, Bendikson, K, Dragisic, K, Schattman, G, Davis, O, and Rosenwaks, Z. Outcome of In Vitro Fertilization in Women 45 Years and Older Who Use Autologous Oocytes. Fertil Sterility (2007) 87(1):74–6. doi:10.1016/j.fertnstert.2006.05.081
59. Nyboe Andersen, A, Goossens, V, Bhattacharya, S, Ferraretti, AP, Kupka, MS, De Mouzon, J, et al. Assisted Reproductive Technology and Intrauterine Inseminations in Europe, 2005: Results Generated from European Registers by ESHRE: ESHRE. The European IVF Monitoring Programme (EIM), for the European Society of Human Reproduction and Embryology (ESHRE). Hum Reprod (2009) 24(6):1267–87. doi:10.1093/humrep/dep035
60. Chandra, A, Copen, CE, and Stephen, EH. Infertility and Impaired Fecundity in the United States, 1982-2010: Data from the National Survey of Family Growth. Natl Health Stat Rep (2013) 2013:1–18.
61. Meng, Q, Ren, A, Zhang, L, Liu, J, Li, Z, Yang, Y, et al. Incidence of Infertility and Risk Factors of Impaired Fecundity Among Newly Married Couples in a Chinese Population. Reprod BioMedicine Online (2015) 30(1):92–100. doi:10.1016/j.rbmo.2014.10.002
62. Mascarenhas, MN, Flaxman, SR, Boerma, T, Vanderpoel, S, and Stevens, GA. National, Regional, and Global Trends in Infertility Prevalence since 1990: a Systematic Analysis of 277 Health Surveys. Plos Med (2012) 9(12):e1001356. doi:10.1371/journal.pmed.1001356
64.Office of Population Affairs. Female Infertility (2019). Available from: https://www.hhs.gov/opa/reproductive-health/fact-sheets/female-infertility/index.html (Accessed June 2, 2021).
65. Arksey, H, and O'Malley, L. Scoping Studies: towards a Methodological Framework. Int J Soc Res Methodol (2005) 8:19–32. doi:10.1080/1364557032000119616
66.Joanna Briggs Institute. JBI Manual for Evidence Synthesis. Chapter 11: Scoping reviews (2020). Available from: https://wiki.jbi.global/display/MANUAL/Chapter+11%3A+Scoping+reviews (Accessed September 8, 2020).
67.World Health Organization. Congenital Anomalies (2016). Available from: https://www.who.int/news-room/fact-sheets/detail/congenital-anomalies (Accessed August 8, 2020).
68. Ngabiirwe, W. An in - Depth Research on Oil & Gas Extraction Industry in East Africa: An African Feminist Perspective (2014). Available from: http://awdflibrary.org/bitstream/handle/123456789/267/Feminist%20Analysis%20on%20%20Oil%20and%20Gas%20Report.pdf?sequence=2&isAllowed=y (Accessed September 08, 2020).
69. Australian Women’s Health Network, . Women and Sexual and Reproductive Health. [updated 2019 April]. 2nd ed. (2012). Available from: https://awhn.org.au/wp-content/uploads/2019/04/AWHN_WomenSRHP_2019_02.pdf (Accessed August 08, 2020).
70.Clarivate Web of Science. EndNote: EndNote X9 (2021). Available from: https://clarivate.libguides.com/endnote_training/users/enx9 (Accessed July 03, 2021).
71. Zungu, LI. Women in the South African Mining Industry: An Occupational Health and Safety Perspective (2011). p. 1–31. Available from: https://uir.unisa.ac.za/bitstream/handle/10500/5005/Inaugurallecture_Women%20in%20the%20SAMI_LIZungu_20October2011.pdf (Accessed August 19, 2020).
72. Rodriguez-Fernandez, R, Ng, N, Susilo, D, Prawira, J, Bangs, MJ, and Amiya, RM. The Double burden of Disease Among Mining Workers in Papua, Indonesia: at the Crossroads between Old and New Health Paradigms. BMC Public Health (2016) 16(1):951–7. doi:10.1186/s12889-016-3630-8
73. Hu, X, Miao, M, Bai, Y, Cheng, N, and Ren, X. Reproductive Factors and Risk of Spontaneous Abortion in the Jinchang Cohort. Int. J. Environ. Res. Public Health (2018) 15(11):2444. doi:10.3390/ijerph15112444
74. Thurston, SW, Ryan, L, Christiani, DC, Snow, R, Carlson, J, You, L, et al. Petrochemical Exposure and Menstrual Disturbances. Am J Ind Med (2000) 38(5):555–64. doi:10.1002/1097-0274(200011)38:5<555:aid-ajim8>3.0.co;2-e
75. Chen, D, Cho, SI, Chen, C, Wang, X, Damokosh, AI, Ryan, L, et al. Exposure to Benzene, Occupational Stress, and Reduced Birth Weight. Occup Environ Med (2000) 57(10):661–7. doi:10.1136/oem.57.10.661
76. Cho, S-I, Damokosh, AI, Ryan, LM, Chen, D, Hu, YA, Smith, TJ, et al. Effects of Exposure to Organic Solvents on Menstrual Cycle Length. J Occup Environ Med (2001) 43(6):567–75. doi:10.1097/00043764-200106000-00012
77. Ha, E, Cho, S-I, Chen, D, Chen, C, Ryan, L, Smith, TJ, et al. Parental Exposure to Organic Solvents and Reduced Birth Weight. Arch Environ Health Int J (2002) 57(3):207–14. doi:10.1080/00039890209602938
78. Siegel, M, Rocheleau, CM, Johnson, CY, Waters, MA, Lawson, CC, Riehle-Colarusso, T, et al. Maternal Occupational Oil Mist Exposure and Birth Defects, National Birth Defects Prevention Study, 1997–2011. Int J Environ Res Public Health (2019) 16(9):1560. doi:10.3390/ijerph16091560
79. Calitz, PL. Experiences of Women in the Platinum Mining Industry. [doctoral dissertation]. Potchefstroom, South Africa: South Africa North-West University (2004). p. 1–48.
80. Bailey-Kruger, A. The Psychological Wellbeing of Women Operating Mining Machinery in a Fly-In Fly-Out Capacity (2012). Available from: https://ro.ecu.edu.au/cgi/viewcontent.cgi?referer=https://scholar .google.com/&httpsredir=1&article=2683&context=theses (Accessed September 12, 2020).
81. Mutendi, M. The Invisible story: Underground Health Narratives of Women in Mining. Master's thesis. Cape Town, South Africa: University of Cape (2017).
82. Botha, D, and Cronjé, F. Occupational Health and Safety Considerations for Women Employed in Core Mining Positions. SA J Hum Resour.Manag (2015) 13(1):1–12. doi:10.4102/sajhrm.v13i1.652
83. Terrill, J. Women in the Australian Mining Industry: Careers and Families. PhD dissertation. Brisbane, Australia: The University of Queensland (2016). p. 1–269. doi:10.14264/uql.2016.830
84. Hermanus, MA. Occupational Health and Safety in Mining-Status, New Developments, and Concerns. J South Afr Inst Min Metall (2007) 107(8):531–8.
85. Badenhorst, CJ, and Platinum, A. Occupational Health and Safety Considerations for the Employment of Female Workers in Hard Rock Mines. In: Southern African Institute of Mining and Metallurgy, Hard Rock Safety Conference; 28-30 September, 2009; Sun City, South Africa (2009). p. 55–74.
86. Evian, C, Fox, M, MacLeod, W, Slotow, SJ, and Rosen, S. Prevalence of HIV in Workforces in Southern Africa, 2000-2001. S Afr Med J (2004) 94(2):125–30.
87. Botha, C, Fourie, JD, Botha, D, and Bischoff, C. Progress in Implementing the Mineral and Petroleum Resources Development Act 28 of 2002 (MPRDA) Provisions for the Employment of Women in Mining. J South Afr Inst Min Metall (2012) 112(5):395–404.
88. Todeva, E, and Lu, L. The Petrochemical Industry in China-Government Regulation and Development Policies. In: In the proceedings of APROS 2000, Asia-Pacific Research in Organisation Studies Annual; 14-16 December 2000; Sidney, Australia (2000). p. 22.
89. Webb, E, Bushkin-Bedient, S, Cheng, A, Kassotis, CD, Balise, V, and Nagel, SC. Developmental and Reproductive Effects of Chemicals Associated with Unconventional Oil and Natural Gas Operations. Rev Environ Health (2014) 29(4):307–18. doi:10.1515/reveh-2014-0057
90. DeMatteo, R, Keith, MM, Brophy, JT, Wordsworth, A, Watterson, AE, Beck, M, et al. Chemical Exposures of Women Workers in the Plastics Industry with Particular Reference to Breast Cancer and Reproductive Hazards. New Solut (2013) 22(4):427–48. doi:10.2190/ns.22.4.d
91. Mrema, EJ, Ngowi, AV, Kishinhi, SS, and Mamuya, SH. Pesticide Exposure and Health Problems Among Female Horticulture Workers in Tanzania. Environ Health Insights (2017) 17:1178630217715237. doi:10.1177/1178630217715237
92. Assadi, SN. Is Being a Health-Care Worker a Risk Factor for Women's Reproductive System? Int J Prev Med (2013) 4(7):852–7.
93. Nicolopoulou-Stamati, P, Maipas, S, Kotampasi, C, Stamatis, P, and Hens, L. Chemical Pesticides and Human Health: the Urgent Need for a New Concept in Agriculture. Front Public Health (2016) 4(4):148. doi:10.3389/fpubh.2016.00148
94. Fucic, A, Galea, K, Duca, R, El Yamani, M, Frery, N, Godderis, L, et al. Potential Health Risk of Endocrine Disruptors in Construction Sector and Plastics Industry: a New Paradigm in Occupational Health. Int. J. Environ. Res. Public Health (2018) 15(6):1229. doi:10.3390/ijerph15061229
95. Banerjee, B. Physical Hazards in Employment and Pregnancy Outcome. Indian J Community Med (2009) 34(2):89. doi:10.4103/0970-0218.51224
96. Yu, CY, Yu, WL, Xu, M, and Xing, ZL. Investigation and Analysis on Shift Work Female Workers' and the Impact on Reproductive Health. Chinese J Indust Hyg Occupat Dis (2018) 36(2):126–9. doi:10.3760/cma.j.issn.1001-9391.2018.02.012
97. Taiwo, AS. The Influence of Work Environment on Workers Productivity: A Case of Selected Oil and Gas Industry in Lagos, Nigeria. Afr J Bus Manag (2010) 4(3):299–307.
98.GM Stave, and PH Wald eds. Physical and Biological Hazards of the Workplace. Hoboken, New Jersey, US: John Wiley & Sons (2016).
99. Carlisle, KN, and Parker, AW. Psychological Distress and Pain Reporting in Australian Coal Miners. Saf Health Work (2014) 5(4):203–9. doi:10.1016/j.shaw.2014.07.005
100. Kumar, RM, Karthick, RB, Bhuvaneswari, V, and Nandhini, N. Study on Occupational Health and Diseases in Oil Industry. Int Res J Eng Technol (2017) 4(12):954–8.
101. Kim, Y, Park, J, and Park, M. Creating a Culture of Prevention in Occupational Safety and Health Practice. Saf Health Work (2016) 7(2):89–96. doi:10.1016/j.shaw.2016.02.002
102. Nielsen, KJ. Improving Safety Culture through the Health and Safety Organization: A Case Study. J Saf Res (2014) 48:7–17. doi:10.1016/j.jsr.2013.10.003
103. Kelloway, EK, and Barling, J. Leadership Development as an Intervention in Occupational Health Psychology. Work & Stress (2010) 24(3):260–79. doi:10.1080/02678373.2010.518441
104. Arocena, P, and Núñez, I. An Empirical Analysis of the Effectiveness of Occupational Health and Safety Management Systems in SMEs. Int Small Business J (2010) 28(4):398–419. doi:10.1177/0266242610363521
105. Niven, K, Sprigg, CA, and Armitage, CJ. Does Emotion Regulation Protect Employees from the Negative Effects of Workplace Aggression? Eur J Work Organizational Psychol (2013) 22(1):88–106. doi:10.1080/1359432x.2011.626200
106. Eyayo, F. Evaluation of Occupational Health Hazards Among Oil Industry Workers: A Case Study of Refinery Workers. IOSR J Environ Sci (2014) 8:2319–99. doi:10.9790/2402-081212253
107. Eriksson, HP, Söderberg, M, Neitzel, RL, Torén, K, and Andersson, E. Cardiovascular Mortality in a Swedish Cohort of Female Industrial Workers Exposed to Noise and Shift Work. Int Arch Occup Environ Health (2021) 94(2):285–93. doi:10.1007/s00420-020-01574-x
108. Kumar, S. Occupational Exposure Associated with Reproductive Dysfunction. Jrnl Occup Health (2004) 46(1):1–19. doi:10.1539/joh.46.1
109. Wong, EY, Ray, R, Gao, DL, Wernli, KJ, Li, W, Fitzgibbons, ED, Camp, JE, Heagerty, PJ, De Roos, AJ, Holt, VL, Thomas, DB, and Checkoway, H. Physical Activity, Physical Exertion, and Miscarriage Risk in Women Textile Workers in Shanghai, China. Am J Ind Med (2010) 53(5):497–505. doi:10.1002/ajim.20812
110. Rahman, J, Fakhruddin, SH, Rahman, AK, and Halim, MA. Environmental Heat Stress Among Young Working Women: a Pilot Study. Ann Glob Health (2016) 82(5):760–7. doi:10.1016/j.aogh.2016.07.007
111. Li, DK, Chen, H, Ferber, JR, Odouli, R, and Quesenberry, C. Exposure to Magnetic Field Non-ionizing Radiation and the Risk of Miscarriage: A Prospective Cohort Study. Sci Rep (2017) 7(1):17541–7. doi:10.1038/s41598-017-16623-8
112. Pirotta, J. An Exploration of the Experiences of Women Who FIFO. Aust Community Psychol (2009) 21(2):37–51.
113. Lovell, J, and Critchley, J. Women Living in a Remote Australian Mining Community: Exploring Their Psychological Well-Being. AJRH (2010) 18(3):125–30. doi:10.1111/j.1440-1584.2010.01143.x
114. Khoza, N. Womans Career Advancement in the South African Mining Industry: Exploring the Experiences of Women in Management Positions at Lonmin Platinum Mine [doctoral dissertation] (2015). Available from: https://ukzn-dspace.ukzn.ac.za/bitstream/handle/10413/13777/Khoza_Nompumulelo_2015.pdf?sequence=1&isAllowed=y (Accessed August 08, 2020).
115. Baggaley, R, Godfrey-Faussett, P, Msiska, R, Chilangwa, D, Chitu, E, Porter, J, et al. How Have Zambian Businesses Reacted to the HIV Epidemic? Occup Environ Med (1995) 52(9):565–9. doi:10.1136/oem.52.9.565
116. Barbey, A. AIDS in the Workplace: The Experience of an Oilfield Service companyInSPE Health, Safety and Environment in Oil and Gas Exploration and Production Conference. Society of Petroleum Engineers (1996).
117. Wu, J, Laurent, O, Li, L, Hu, J, and Kleeman, M. Adverse Reproductive Health Outcomes and Exposure to Gaseous and Particulate-Matter Air Pollution in Pregnant womenResearch Reports. Massachusetts, US: Health Effects Institute (2016).
118. Vigeh, M, Yunesian, M, Shariat, M, Niroomanesh, S, and Ramezanzadeh, F. Environmental Carbon Monoxide Related to Pregnancy Hypertension. Women & Health (2011) 51(8):724–38. doi:10.1080/03630242.2011.633599
119. Vigeh, M, Yokoyama, K, Kitamura, F, Afshinrokh, M, Beygi, A, and Niroomanesh, S. Early Pregnancy Blood lead and Spontaneous Abortion. Women & Health (2010) 50(8):756–66. doi:10.1080/03630242.2010.532760
120. Quinn, AK, Ae-Ngibise, KA, Jack, DW, Boamah, EA, Enuameh, Y, Mujtaba, MN, et al. Association of Carbon Monoxide Exposure with Blood Pressure Among Pregnant Women in Rural Ghana: Evidence from GRAPHS. Int J Hyg Environ Health (2016) 219(2):176–83. doi:10.1016/j.ijheh.2015.10.004
121. Gonzalez, C. Occupational Reproductive Health and Pregnancy Hazards Confronting Health Care Workers. Aaohn J (2011) 59(9):373–6. doi:10.3928/08910162-20110825-04
122. Sargsyan, A. Heavy Metals and Reproductive Health-Reproductive Health Problems Among Women of Childbearing Age in Alaverdi (Lori Marz) and Artik (Shirak Marz) Cities: A Cross-Sectional Survey. [doctoral dissertation]. Yerevan, Armenia: College of Health Sciences American University of Armenia (2015).
123. Middlesworth, M. Rapid Upper Limb Assessment (RULA) (2020). Available from: https://ergo-plus.com/wp-content/uploads/RULA-A-Step-by-Step-Guide1.pdf (Accessed October 02, 2020).
124. Yong, X, Li, F, Ge, H, Sun, X, Ma, X, and Liu, J. A Cross-Sectional Epidemiological Survey of Work-Related Musculoskeletal Disorders and Analysis of its Influencing Factors Among Coal Mine Workers in Xinjiang. Biomed Res Int (2020) 2020:3164056. doi:10.1155/2020/3164056
128. Ali, M. Impact of Gender-Focused Human Resource Management on Performance: The Mediating Effects of Gender Diversity. Aust J Management (2016) 41(2):376–97. doi:10.1177/0312896214565119
129. Brown, LM. The Relationship between Motherhood and Professional Advancement: Perceptions versus Reality. Empl Relat (2010) 32:470–94. doi:10.1108/01425451011061649
130. Yoon, SJ, Lin, HK, Chen, G, Yi, S, Choi, J, and Rui, Z. Effect of Occupational Health and Safety Management System on Work-Related Accident Rate and Differences of Occupational Health and Safety Management System Awareness between Managers in South Korea's Construction Industry. Saf Health work (2013) 4(4):201–9. doi:10.1016/j.shaw.2013.10.002
Keywords: women, women health, sexual and reproductive health, work and occupation, oil and natural gas, mining industry
Citation: Razafimahefa RH, Pardosi JF and Sav A (2022) Occupational Factors Affecting Women Workers’ Sexual and Reproductive Health Outcomes in Oil, Gas, and Mining Industry: A Scoping Review. Public Health Rev 43:1604653. doi: 10.3389/phrs.2022.1604653
Received: 30 November 2021; Accepted: 31 March 2022;
Published: 28 April 2022.
Edited by:
Milena Maule, Università di Torino, ItalyReviewed by:
Vivi Schlunssen, Aarhus University, DenmarkCopyright © 2022 Razafimahefa, Pardosi and Sav. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms. PHR is edited by the Swiss School of Public Health (SSPH+) in a partnership with the Association of Schools of Public Health of the European Region (ASPHER)+
*Correspondence: Rina Hariniaina Razafimahefa, cmluYWhhcmluaWFpbmFAeWFob28uZnI=