 Mercedes Gomez del Pulgar1,2
Mercedes Gomez del Pulgar1,2 Miguel Angel Cuevas-Budhart3*Sonsoles Hernández-Iglesias4Maria Kappes5Veronica Andrea Riquelme Contreras6Esther Rodriguez-Lopez1Alina Maria De Almeida Souza7Maximo A. Gonzalez Jurado1Almudena Crespo Cañizares8
Miguel Angel Cuevas-Budhart3*Sonsoles Hernández-Iglesias4Maria Kappes5Veronica Andrea Riquelme Contreras6Esther Rodriguez-Lopez1Alina Maria De Almeida Souza7Maximo A. Gonzalez Jurado1Almudena Crespo Cañizares8- 1Centro de Educación Superior Hygiea, Madrid, Spain
- 2Coordination of the Center for Advanced Clinical Simulation of the Nursing Degree, Universidad Francisco de Vitoria, Posuelo de Alarcon, Madrid, España
- 3Unidad de Investigación Médica en Enfermedades Nefrológicas, Instituto Mexicano del Seguro Social (IMSS), Mexico City, México
- 4Institutional Relations and Health Practices of Health Sciences, Faculty of the Nursing Degree, Universidad Francisco de Vitoria, Pozuelo de Alarcon, Madrid, España
- 5College of Health Care Sciences, Nursing School, Universidad San Sebastián, Puerto Montt, Chile
- 6San Sebastián University, Santiago, Chile
- 7Spanish Nursing Research Institute, Consejo General de Enfermería, Madrid, Spain
- 8Clinical Practices of the Degree in Nursing, Universidad Francisco de Vitoria, Pozuelo de Alarcón, Spain
Objectives: To explore nursing health education interventions for non-communicable disease patients.
Methods: The design was a systematic review of research work published between 2008 and 2018. The data sources included the Web of Science, PubMed, Scopus, COCHRANE, and LILACS. The studies that met the inclusion were assessed, and the analysis for methodological quality through the recommended tools CASPe, and JADAD.
Results: Fifteen original studies from eight counties were included in the review; Findings revealed 13 studies with randomized samples and six used power analysis. Nurses’ interventions included house calls, home care, and individual and group health education.
Conclusion: Nursing interventions showed 76.4% the effectiveness of results in patient outcomes to promote and improve healthier lifestyles and quality of life of non-communicable disease patients. This review discloses the significant impact of nursing health education interventions. Nursing leadership and political decision-makers should consider providing programs to enhance health education knowledge and abilities. All of this can favor the sustainability of the global economy by changing the life style of thousands of people worldwide.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/, identifier CRD42020208809.
Introduction
The current increase in the prevalence and incidence of non-communicable diseases (NCDs), part of the chronic diseases realm, has become a priority for all health systems worldwide. The World Health Organization (WHO) has defined these conditions as being of long duration and generally slow progression and causing early death [1]. Cardiovascular diseases affecting the heart, several kinds of cancer, chronic respiratory conditions, diabetes, and rheumatic and neurological disorders are among the most frequent NCDs affecting all adult population [2, 3].
The NCDs have a significant impact on the population’s quality of life. It affects patients, families, and their environment with consequences for society, economic, psychological, and social levels [4]. Health systems in most counties need to undergo structural changes to provide healthcare services focusing on continuous surveillance and efficiency. It also should include investment in a specialized workforce and resources to guarantee the quality of care and an association with a network of auxiliary services.
These concerns require more research to provide new evidence and therapeutic advances, enhance institutional integration, and community health services, and close personalized and specialized family continuous surveillance. Improvements should favor distress among professionals [5, 6].
Within this framework, primary health care (PHC) has been considered an essential service associated with better health outcomes for individuals who live with NCDs [7]. In the PHC settings, nurses specialize in public health, and community nursing and nurse practitioners perform control and prevention of NCDs [8], as mentioned by Toney-Butler and Thayer 2019 [9]; Semachew 2018 [10]; Hanlon et al. 2018 [11]; Costa et al. 2016 [12]: Nursing services in PHC integrated into the different levels of the health system, with close interaction with hospitals and other agencies, should be an essential instrument in advancing NCD care.
Public health, community, or family specialized nurses should have the knowledge and abilities to identify problems and plan, implement, and evaluate quality nursing care. Their contribution to the control of NCDs could add to attaining goals to improve the quality of life of NDCs patients [13, 14], Gathering research evidence on the knowledge underlying nursing care should improve and reinforce their contribution to nursing science and practice [13, 14], while answering the population’s need for wellbeing and health [15, 16]. The tested relevance of nursing interventions and the outcome for the patients is indeed an imposition facing 21st century nursing [17].
Nursing interventions and teamwork cooperation with other healthcare professionals help to establish holistic, integrative healthcare. In this respect, nursing has shown extensive knowledge, skills, and attitudes, underlining their teamwork competencies as highly valued for necessary and systematic coordination within the multidisciplinary health team. In summary, nursing services should rely on specialized nurses at all levels of the health system [18].
In this order of ideas, studies conducted on nursing interventions within NCD show improvement in glycemic control [19], enhancement of quality of life [20], decrease in hospitalizations to complications, and effective reduction in mortality, as mentioned by Zegers et al. 2016 [21] and Lloyd et al. 2012 [22]. Evidence suggests that nursing services could be a vital instrument to help control healthcare costs, as mentioned by Laurant et al. 2018 [23]; Coleman et al. 2009 [24] and Cramm et al. 2013 [25].
Research has also provided control through restructured guidelines to improve the nursing practice and create a patient self-care culture effectively and efficiently. In addition, health administrators and managers in charge of developing policies have taken nurse-led NCD management programs as strategies to decrease the economic and healthcare burden of NCD. A review conducted in 2016 for Khanassov et al [26], shows that interventions organized and led by nurses improve the accessibility, availability, and affordability of primary healthcare services, improving health outcomes for the population. However, understanding and classifying these interventions at the international level can help the national health system learn from others and achieve the expected population health outcomes.
Nursing organizations’ leadership throughout the world since 2013, when the WHO Global Action Plan for the Prevention and Control of NCDs 2013–2020 was created, has pursued calling attention to the important role their professionals should assume in contribution to targets related to the reduction of premature mortality and improvement of life quality from NCDs [6]. In addition, in the realm of the UN Sustainable Development, nursing research centered on interventions of education and promotion of health to NDC patients and their families will certainly generate critical new knowledge to enhance the actions toward the attainment of these goals, good health and well-being, as stated in goal number 3: “Ensuring healthy lives and promoting well-being to CDC patients and their families [27–29].” Thus, the implementation of research about nursing-specific care is among the activities that provide evidence in this respect.
Nursing literature is somewhat limited; however, it has provided evidence of actions oriented toward guidance for self-care and information on community resources as a target in support of actions needed attaining the Sustainable Development Goals. Therefore, this study’s primary purpose was to conduct a systematic literature review to explore nursing health education interventions to promote improvement of the health and quality of life of NCD patients.
Methods
Study Design
The steps guiding this review included formulation of the main question, criteria of inclusion, literature search, and data assessment using a systematic process for identification, evaluation, and synthesis of the existing scientific evidence analysis and conclusions [30–33]. Firstly, the guiding principles based on PICO components were used to develop the questions for this systematic review: 1) Are nurses implementing actions to improve self-care and increasing knowledge about aid support in the community? 2) What method of health education is provided to NCDs patients, families, and home care personnel, if involved? 3) What kinds of information or guidelines are available? 4) What was the population of the study? 5) Do the studies include patient outcomes? As an independent variable, NCD patient-focused nursing interventions are used.
Search Strategy
As a first approach, the search included five health science databases: Web of Science, PubMed, Scopus, COCHRANE, and LILACS, to find publication data between 2008 and 2018 and accomplished in December 2018. A secondary search aiming to retrieve all available information on clinical studies from grey literature, Ph.D. dissertations in the Spanish Dissertations database (TESEO), and The National Library of Medicine Gateway, was completed in January 2019. Healthcare science (DeCS) and Medical Subject Headings (MeSH) used descriptors. The keywords were: nurse, non-communicable diseases, intervention nursing, house calls, community health nursing. The Boolean operators used were intersection (AND) to establish the logical operations between concepts and (OR) to retrieve papers where at least one of the arguments specified appears.
Inclusion and Exclusion Criteria
The study used the following criteria to select the studies: 1) randomized and non-randomized clinical studies; 2) participants older than 18 years; 3) NCD diagnosis; 4) complete description of educational level, interventions related to prevention including health education process, therapeutic procedures after diagnose, rehabilitation, as applied according to NCD, promotion 5) covering field of primary health nursing care, including home care; 6) published between 2008 and 2018; and 7) written in Spanish or English. Exclusion included papers with interventions led by non-nursing healthcare professionals or op-eds and discussion papers.
Selection Process and Quality Assessment
Figure 1 shows a PRISMA diagram summarizing the selection process. The results from the initial database search yielded 1,454 studies and the results from other sources (dissertations and grey literature) identified 807 papers, adding to a total of 2,261 papers; the screening process removed duplicates and studies not fulfilling the inclusion criteria (1607). A total of 74 abstracts remained for full-text screening, after the elimination of 580 articles that were independently reviewed by researchers where the intervention led by health professionals were not nurses or were opinion and discussion articles. In the process, 31 full‐text reports were assessed for eligibility and 16 papers were excluded due to low‐quality research methodology, and the remaining 15 papers were included in this literature review. The assessment of methodological quality used the CASPe [34] and JADAD tools [35].
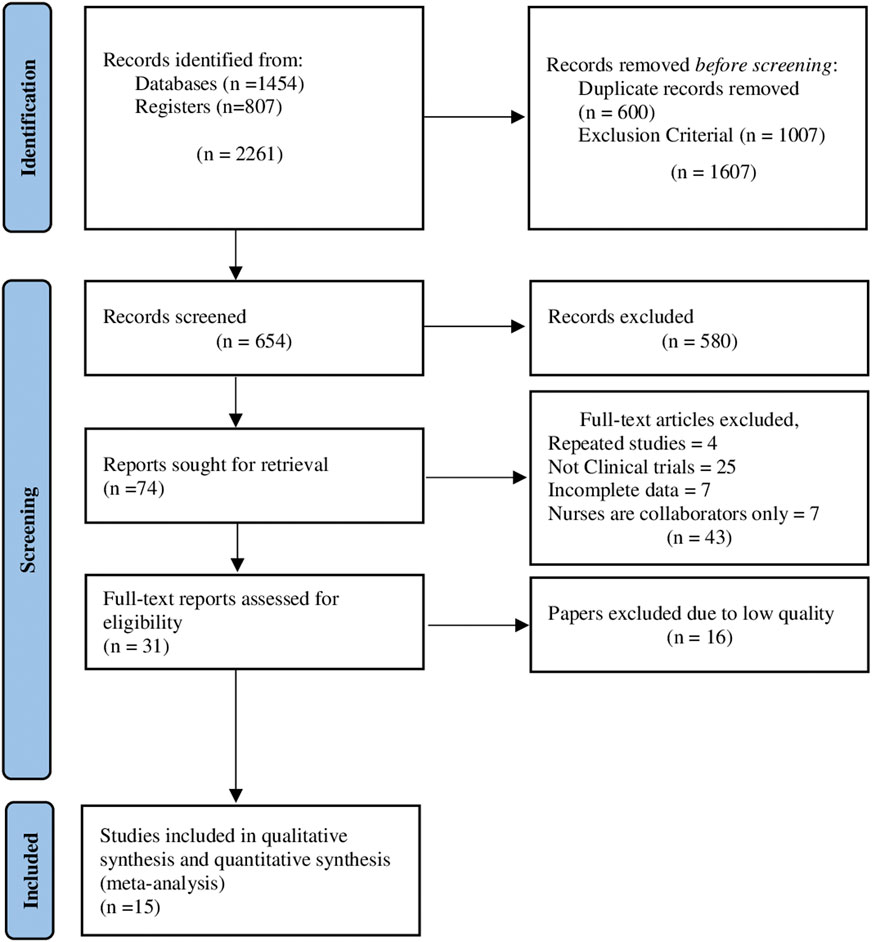
FIGURE 1. Flow diagram for systematic reviews (Page MJ, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. 2021). [Sweden, The Netherlands, the UK, Colombia, Spain, Australia, Hong Kong, China, and Austria. (2009-2017)].
The selected fifteen studies were independently peer-assessed and submitted to a test methodological minimum quality level [36]. Methodological quality was assessed through the CASPe [34] tool, which includes the validity, nature, and applicability of the results, and the JADAD scale [35] to evaluate the methodology of the studies and establish the extent of the possibility of bias in the design, conduct, and analysis.
The first author elaborated the abstraction and synthesis of the included studies that can be seen in Table 1, including aims and design, settings and sample, nursing CDs interventions, main findings, and quality evidence.
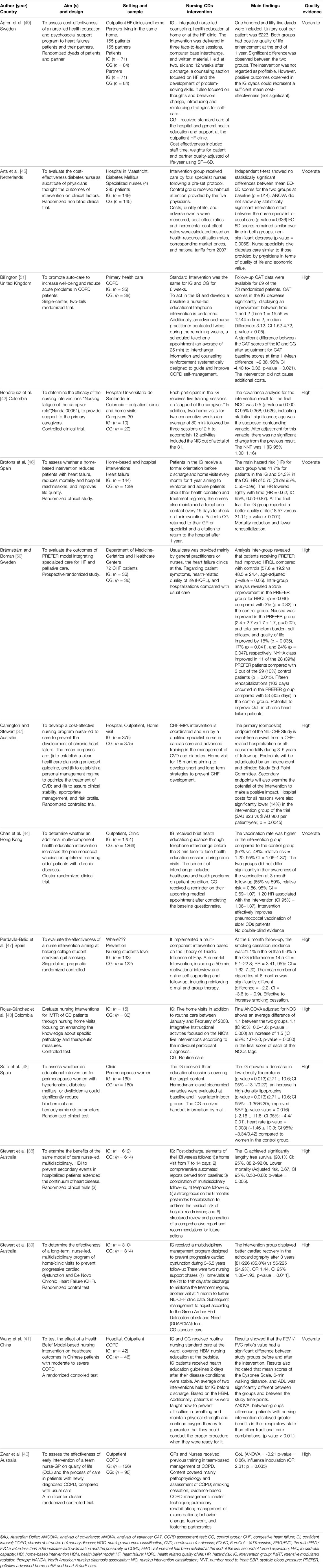
TABLE 1. Summary of Studies on Nursing Interventions for non-communicable diseases [Sweden, The Netherlands, the UK, Colombia, Spain, Australia, Hong Kong, China, and Austria. (2009-2017)].
Results
Characteristics of Selected Studies
The fifteen studies were from eight countries [Australia [4] Carrington and Stewart 2009 [37], Stewart et al. 2016 [38], Stewart et al. 2015 [39]; Zwar et al. 2011 [40]; China [1] Wang et al. 2013 [41]; Colombia [2] Bohórquez et al. 2011 [42], Rojas-Sánchez et al. 2009 [43]; Hong Kong [1] Chan et al. 2015 [44]; Netherland [1] Arts et al. 2011 [45]; Spain [3] Brotons et al. 2009 [46], Pardavila-Belio el al. 2015 [47], Soto et al. 2017 [48]; Sweden [2] Ågren et al. 2013 [49], Brännström & Boman 2014(50); United Kingdom [1] Billington et al. 2015 [51]]. In thirteen studies, participants were reported as randomized and divided into two groups - intervention and control. Two studies were controlled clinical trials (Bohórquez et al. 2011 [42] & Rojas-Sánchez et al. 2009 [43]).
The sample size ranged between 30 and 2,517 (median:121). The median calculated was 58.8 ± 325.4 (range 20–1251) patients and 56.05 ± 328.9 (range 10–1266) for the intervention and control groups, respectively. Most studies reported their abandonment rates.
Six clinical studies used power analysis (Arts et al. 2012(45); Chan et al. 2015 [44]; Zwar et al. 2016 [40]; Billington et al. 2015 [51]; Stewart et al. 2015; Stewart et al. 2016 [40]). Nurses were the principal researcher (n = 8) (Pardavila-Belio et al. 2015 [47]; Zwar et al. 2016 [40]; Rojas-Sánchez et al. 2009 [43]; Bohórquez et al. 2011 [42]; Chan et al. 2015 [44]; Ågren et al. 2013 [49]; Brännström 2014(50); Arts et al. 2012(45)), five do not specify who did the recruitment (Brotons, et al [46], Carrington & Stewart [37], Stewart et al [39], Stewart et al [38], Wang et al [41]) and in two clinical studies subjects were recruited by another professional within the research group, as mentioned for Soto Rodríguez et al [48]. and Billington et al [51].
The studies covered several topics related to the interventions led by nurses in the care of patients with chronic diseases. Interventions most cited were: house call and home care, n = 8 (53.3%) (Bohórquez et al [42], Brotons et al [46], Rojas-Sánchez et al [43], Ågren et al [49]. Wang et al [41]. Billington et al [51]. Stewart et al [38]. Brännström and Boman [50]), health education activities (individual and group), n = 3 (20%) (Chan et al [44]. Soto-Rodríguez et al [48]. Zwar et al [39] = , and additional nursing intervention focusing on general nursing care was also observed n = 3 (20%) [18, 37, 45]. One study performed 3 linked trials testing nurse-led, multidisciplinary, and home-based intervention, using three different clinical managements n = 1 (6.7%) [38].
It is important to note that even with repeated interventions with the same topic, the methodologies and experimental designs used were different. For this reason, outcomes were heterogeneous and not comparable.
Most interventions included a framework for preventing complications caused by NCDs, such as decreasing the risk of developing heart failure, in Carrington and Stewart [37], Stewart et al [38], and Zwar, et al [40], Wang, et al [41]. However, some studies were more specific, improving quality of life [37, 39–42, 44, 45, 51], reducing symptoms caused by the disease, reducing biochemical and hemodynamic parameters, smoking cessation, preventing hospitalization, and effectively managing the therapy system. Just one study assessed the cost-effectiveness of replacing doctors with primary care nurses. Regarding the description of NCDs targeted by interventions, most were chronic obstructive pulmonary disease (COPD) 4 (27%) and heart failure (HF) 4 (27%).
Metrics Outcome
Most studies yielded positive outcomes in one or more metrics. The interventions were conducted to increase knowledge or improve clinical data in the experimental group, including increasing patients’ quality of life (Arts et al [45], Bilington et al [51], Bohorquez, et al [42]; Carrington and Stewart [37], Chan, et al [44]; Stewart et al [39]. Wang, et al [41]; and Zwar, et al. 2011 [40]). Nursing interventions were effective and 76.4% of the research presented positive effectiveness results.
Due to the challenging situation of NCDs in the world, nursing interventions in house calls can positively affect the evolution and management of the disease, preventing various complications. Most studies extensively and carefully described the criteria for selecting subjects, as well as the effectiveness of the interventions (Agren et al. 2013; Arts et al. 2011; Bilington et al. 2015; Brotons, et al. 2009; Brännström and Boman. 2014; Chan, et al. 2015; Pardavila Belio, et al. 2015; Rojas-Sanchez, et al. 2009; Soto, et al. 2017; and Stewart et al. 2016), and even in those results that were not statistically significant, the intervention uptake was low and had no additional beneficial effect over usual care or participants’ health-related QoL [39, 40].
The study by Ågren et al [49], analyzed the intervention costs in institutions and organizations, specifically for NCD patients. It demonstrated success stories, where treatments were compared between doctors and nurses, which proved similar care from both professionals, providing similar economic value and quality of life. This similarity gives rise to an opportunity to save on healthcare costs, given that nurse labor cost is remarkably lower than physicians [23] (Coleman et al [24], Cramm et al [25]). However, interventions are not regarded as profitable for the patient alone, as they are an economic burden. However, it showed positive effects on the quality of life of patients undergoing the intervention [45].
Discussion
This literature review was an attempt to answer two central questions–the kind of nursing interventions and main NCDs in which nurses intervene–to ensure best results as a path to identify scientific evidence of the effectiveness of these interventions, a significant challenge that discloses the gap between nursing theory and practice, as mentioned by Stetler [16] and DiCenso [15].
All studies used several types of clinical studies, including randomized controlled studies, controlled clinical studies, control groups, cost-benefit analysis, and a variety of mixed nursing interventions led by nurses, from formal health education, counselling, information interchange, briefings to psychological support, all related to the Nursing Interventions Classification (NIC), code 5,510 definition and activities listed as health education.
Health education is an essential competence for professional nurses working all health levels and settings, and indeed requires that health professions, especially nurses, know the learning process and teaching skills. Almost all the reviewed studies did not assess or mention the kind of education methodology used. Only three studies referred to a specific component of the educational intervention [1]; Pardavila-Belio et al [47]., who refer to interventions focusing on the Triadic Theory Influence, a theory that considers health behaviors in preventive interventions (Flay & Petraitis 1994(47) mentioned in Frank J. Snyder 2012) [2], Rojas-Sánchez et al [43]., focused on five interventions proposed by the NIC according to the individual participant diagnoses, and [3] Stewart et al. (2015) used the tool surveillance the Green Amber Red Delineation of Risk And Need (GUARDIAN) as a management tool to assess risk and need control frequency and intensity of future interventions [37, 41]; in addition, they used “The Health Belief Model,” an internationally validated model not thoroughly explored in Chinese patients with COPD.
Of the fifteen selected studies, 60% incorporated interventions that could include nursing care plans, for either the prevention, recovery, rehabilitation, or promotion of health. These interventions consisted of standardized care or the enforcement of protocol plans. These protocol plans are studies using multi-disciplinary interventions, motivational interviews, and other strategies. Forty percent of the remaining studies were part of the educational interventions group, including educational plans, follow-up telephonic interventions, and educational sessions. For this purpose, specialist professionals were chosen, accompanied by psychosocial programs or regular care. All studies observed that the intervention group (IG) and control group (CG) received routine health education care in the clinical setting.
The content of all interventions covered issues related to specific patient conditions [1] heart failure—6 (Agren et al.; Brännström and Boman; Brotons et al.; Carrington and Stewart; Stewart et al.; Stewart et al) [2]; COPD patients—3 (Billington et al.; Wang et al.; Zwar et al.) [3]; diabetes mellitus and other related disorders - 2 (Soto et al. and Arts et al.); The remaining studies did not focus on a specific pathology, but a condition related to the prevention of respiratory CDs 2 (Chan et al.; Pardavila-Belio el al.); IMRT to improve the adherence of CDs patients to treatment 1 (Carolina et al.) and, “fatigue” of primary care of patients with CDs—1 (Rojas-Sánchez et al.).
Despite differences in the procedures to measure the nursing interventions, the majority of the studies reviewed point out a significant change in patient lifestyle and their health condition control. This signifies the effectiveness of the educational interventions in the context of CDs specific conditions to improve the quality of life, support primary caregiver, acceptance of immunization program to prevent respiratory diseases, adherence to therapeutic treatment and smoking cessation program, decrease of risk factors, improved cardiac conditions in chronic heart failure, decrease mortality and rehospitalization, improvement of patients with moderate and severe COPD [38–41, 43, 44, 46, 47, 52, 53].
Three studies can be classified as a cost-effectiveness study. Two are of inferior quality due to the specific statement declaration as single-blind studies. In one of them, there is no evidence of the analysis of the results contemplating the group losses.
The three studies measured interventions guided by nurses about conventional care. Nonetheless, the results contemplate different units of analysis. These are total hospital cost for the intervened patients versus the control group, cost of intervention per patient and reduction of expenses in the direct cost of patient care. These results cannot be compared. In two of the three studies, the interventions were considered more cost-effective as compared to the control group. These interventions were displacing doctors for specialist nurses for the checking of patients with non-communicable diseases [45] and a program of care guided by a nurse for patients with chronic heart failure [37]. Another intervention was not regarded as profitable [49]. The third showed that the intervention was significant to improve health conditions of COPD patients and did not cause additional cost [51].
The present review also displays some evidence related to specialized and advanced practice nurses or nurses intervening in the educational process, or training sessions for nurses before the intervention. It is well known that the relevance nursing training programs at the university level emphasize the educational role of nursing in health education, and this has been supported and enforced by governments, nursing, and international organizations. The WHO and the ICN also emphasize the importance of nursing in the control of NCDs, mainly in the primary health care setting with a critical surveillance program, including coordinate and multi-professional care [6, 54]. NCDs are a real threat to human health. Over 50% of all causes of death in the world are chronic diseases, including the population in all counties, high and low income, young and elderly [55].
The study also mentions the role of nurses in support of non-professional care, these need information, training, as well as warmth and attention to their physical and psychological care [52], and strategies for home care, as mention by Brotons et al [46]. This illustrates the importance of home care, showing that it reduces mortality rates, and re-hospitalizations due to complications, and improves quality of life in patients with heart failure.
It is important to note that the search was carried out at the end of 2018, the year in which the Nursing Now movement began. However, a posteriori information search was added, which, is supported by more evidence that home monitoring of older patients with NCDs decreases hospital admission and demonstrably prevents falls and autonomy capacity deficits, according to the results found by Lui M, et al [56]., in 2021.
In addition, Sorensen A, et al [57]., argue through a clinical trial that the home visit favors medication control, and decreases the number of admissions or readmissions in health institutions, a fact that can aggravate the mental state of patients. For its part, the COVID-19 pandemic came to demonstrate how the monitoring carried out by nursing reduced infections and improved sanitary isolation in some cases, greatly increasing the health status of the population.
Taking into consideration the diversity of methodology, and necessary procedures to measure the proposed nursing intervention in all clinical studies in this literature review, it was impossible to perform a meta-analysis.
Relevance for the Fulfillment of the Sustainable Development Goals
This review discloses the significant impact of nursing educational interventions for patients with different NCD conditions. It shows the actual trend of an above-average increase in the incidence and prevalence of NCDs worldwide. Nursing is called on to play a leadership role to create and promote innovative solutions to improve the quality and efficacy of the health system. Furthermore, this guarantees a healthy life and promotes well-being at all ages, especially in the population with NCDs. Therefore, nursing leadership should mainly promote and emphasize the training of nurses to assume a key and active role in primary care settings, emphasizing the development of competencies and skills to care for patients with NCDs [54]. All this can favor the sustainability of the global economy by changing thousands of people in the world; such is the example of the presence of the current epidemiological state.
This key role should include competencies and skills for cooperative work with healthcare professionals and stakeholders in society. It certainly involves rigorous and robust teaching of educational strategies focused on the importance of behavioral changes because of many interventions that deal with patients with NCDs. To do this, the nursing professional helps to achieve significant advances in life expectancy and reduce the risk of infection or complications in patients who most deserve care.
Nursing organizations need to provide standardization of interventions for NCD problems at the local level, and procedures and guidelines that fit the population in their context. Patients with NCDs need to acquire the confidence to deal with their process and seek help before the aggravation of their health status.
Another significant nursing contribution to NCD surveillance and nursing care in the health system is interventions focusing on health promotion and disease prevention. Unhealthy lifestyles, such as smoking, passive attitude, inadequate nutrition, and life stress, aggravate NCDs. Environmental and genetic conditions also play a role in the onset of NCDs that require interventions to promote lifestyle changes [58]. Indeed, nursing can contribute to the battle against these factors, and policies are required in the health system to support and improve the commitment of the nursing profession to the care of NCDs, as well as a social and comprehensive commitment to improve outcomes and the lifestyle of the population it serves. Thus, empowering nurses to play a vital role in NCD control would positively contribute to achieving this goal.
Conclusion
The results of this review show how nursing has published results of research on several topics in the last ten years, with a comprehensive view of research studies, conducting clinical studies, where the independent variable was education and integral intervention focusing on patients with NCDs and generating a culture of active and effective involvement.
The growing international evidence suggests that interventions carried out by community nurses contribute to the favorable modification of risk factors, lifestyles, and control of NCDs.
The outcomes of the review are consistent, despite including various types of nursing interventions based on education and the subjects’ active involvement. They are useful in terms of preventing complications caused by diseases, decreasing the risk of developing heart failure, improving quality of life, reducing the symptoms caused by disease, improving biochemical and hemodynamic parameters, smoke cessation, preventing hospitalization, and effectively managing the therapeutic regime, as well as decreasing healthcare costs in the care of patients with non-communicable diseases.
Nursing interventions were effective in the analysis. 76.4% of the research had positive outcomes regarding the effects of the studies, which is a strong argument to support nurses’ work.
Author Contributions
Study design: MGP and MCB. SHI: collaborated in the evaluation of the methodological quality of the studies, with which we place it in this epigraph, but what it did was carry out a fine evaluation with the instruments to evaluate the quality and risk of bias of documents. Data collection: AC, and ERL. Data analysis: MCB, MK, and VR. Study supervision: MGP and MGJ. Manuscript writing: MGP, MCB, MK, and ADA. Critical revisions for important intellectual content: MGP, ADA, and MGJ.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. World Health Organization, (2016). Global Report on Diabetes [Internet]Available from: http://apps.who.int/iris/bitstream/handle/10665/254649/9789243565255-spa.pdf;jsessionid=D4B78291487E69704A22EBE3F97B1FA9?sequence=1 (Accessed August 15, 2021).
2. Heneghan, C, Blacklock, C, Perera, R, Davis, R, Benerjee, A, Gill, P, et al. Evidence for Non-communicable Diseases: Analysis of Cochrane Reviews and Randomised Trials by World Bank Classification. BMJ Open (2013) 3(7):e003298. doi:10.1136/bmjopen-2013-003298
3.WHO. OMS | Enfermedades Crónicas (2017). Available from: https://www.who.int/topics/chronic_diseases/es/ (Accessed August 15, 2021).
4. Vos, T, Allen, C, Arora, M, Barber, RM, Bhutta, ZA, Brown, A, et al. Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 310 Diseases and Injuries, 1990-2015: a Systematic Analysis for the Global Burden of Disease Study 2015. Lancet (2016) 388:1545–602. doi:10.1016/S0140-6736(16)31678-6
5. Khanal, S, Veerman, L, Nissen, L, and Hollingworth, S. Use of Healthcare Services by Patients with Non-communicable Diseases in Nepal: A Qualitative Study with Healthcare Providers. J Clin Diagn Res (2017) 11:LC01–LC05. doi:10.7860/JCDR/2017/25021.9970
6. Who, . 2013-2020 Action Plan for the Prevention and Control of Non-communicable Diseases (2013). Available from: www.who.int (Accessed August 15, 2021).
7. Hansen, J, Groenewegen, PP, Boerma, WGW, and Kringos, DS. Living in a Country with a strong Primary Care System Is Beneficial to People with Chronic Conditions. Health Aff (2015) 34(9):1531–7. doi:10.1377/hlthaff.2015.0582
8. Beaglehole, R, Epping-Jordan, J, Patel, V, Chopra, M, Ebrahim, S, Kidd, M, et al. Improving the Prevention and Management of Chronic Disease in Low-Income and Middle-Income Countries: a Priority for Primary Health Care. Lancet (2008) 372:940–9. doi:10.1016/S0140-6736(08)61404-X
10. Semachew, A. Implementation of Nursing Process in Clinical Settings: the Case of Three Governmental Hospitals in Ethiopia, 2017. BMC Res Notes (2018) 11:173. doi:10.1186/s13104-018-3275-z
11. Hanlon, P, Yeoman, L, Gibson, L, Esiovwa, R, Williamson, AE, Mair, FS, et al. A Systematic Review of Interventions by Healthcare Professionals to Improve Management of Non-communicable Diseases and Communicable Diseases Requiring Long-Term Care in Adults Who Are Homeless. BMJ Open (2018) 8:20161. doi:10.1136/bmjopen-2017-020161
12. Bonomi, AE, Wagner, EH, Glasgow, RE, and Vonkorff, M. Assessment of Chronic Illness Care (ACIC): A Practical Tool to Measure Quality Improvement. Health Serv Res (2002) 37(3):791–820. doi:10.1111/1475-6773.00049
13. Fawaz, MA, Hamdan-Mansour, AM, and Tassi, A. Challenges Facing Nursing Education in the Advanced Healthcare Environment. Int J Africa Nurs Sci (2018) 9:105–10. doi:10.1016/j.ijans.2018.10.005
14. Melnyk, BM, Fineout-Overholt, E, Stillwell, SB, and Williamson, KM. Evidence-Based Practice: Step by Step: The Seven Steps of Evidence-Based Practice. Am J Nurs (2010) 110:51–3. doi:10.1097/01.NAJ.0000366056.06605.d2
15. DiCenso, A, Guyatt, G, and Ciliska, D. Evidence-Based Nursing: A Guide to Clinical Practice. 1st ed. St. Louis: Elsevier Mosby (2005).
16. Stetler, CB. Updating the Stetler Model of Research Utilization to Facilitate Evidence-Based Practice. Nurs Outlook (2001) 49(6):272–9. doi:10.1067/mno.2001.120517
17. Green, BN, and Johnson, CD. Interprofessional Collaboration in Research, Education, and Clinical Practice: Working Together for a Better Future. J Chiropr Educ (2015) 29:1–10. doi:10.7899/JCE-14-36
18. Peltokoski, J, Vehviläinen-Julkunen, K, and Miettinen, M. Nurses’ Hospital Orientation and Future Research Challenges: An Integrative Review. Int Nurs Rev (2016) 63(1):92–103. doi:10.1111/inr.12226
19. Simon, J, Gray, A, Clarke, P, Wade, A, Neil, A, Farmer, A, et al. Cost Effectiveness of Self Monitoring of Blood Glucose in Patients with Non-insulin Treated Type 2 Diabetes: Economic Evaluation of Data from the DiGEM Trial. BMJ (2008) 336:1177–80. doi:10.1136/bmj.39526.674873.BE
20. Health Quality Ontario, HQ. Continuity of Care to Optimize Chronic Disease Management in the Community Setting: an Evidence-Based Analysis. Ont Health Technol Assess Ser (2013) 13:1–41.
21. Zegers, M, Hesselink, G, Geense, W, Vincent, C, and Wollersheim, H. Evidence-based Interventions to Reduce Adverse Events in Hospitals: a Systematic Review of Systematic Reviews. BMJ Open (2016) 6:e012555. doi:10.1136/bmjopen-2016-012555
22. Lloyd, CE, Roy, T, Nouwen, A, and Chauhan, AM. Epidemiology of Depression in Diabetes: International and Cross-Cultural Issues. J Affect Disord (2012) 142:S22–9. doi:10.1016/S0165-0327(12)70005-8
23. Laurant, M, van der Biezen, M, Wijers, N, Watananirun, K, Kontopantelis, E, and van Vught, AJ. Nurses as Substitutes for Doctors in Primary Care. Cochrane Database Syst Rev (2018) 7:CD001271. doi:10.1002/14651858.CD001271.pub3
24. Coleman, K, Austin, BT, Brach, C, and Wagner, EH. Evidence on the Chronic Care Model in the New Millennium. Health Aff (2009) 28:75–85. doi:10.1377/hlthaff.28.1.75
25. Cramm, JM, Nieboer, AP, Wagner, E, Austin, B, Davis, C, Jacobs, R, et al. High-quality Chronic Care Delivery Improves Experiences of Chronically Ill Patients Receiving Care. Int J Qual Health Care (2013) 25(6):689–95. doi:10.1093/intqhc/mzt065
26. Khanassov, V, Pluye, P, Descoteaux, S, Haggerty, JL, Russell, G, Gunn, J, et al. Organizational Interventions Improving Access to Community-Based Primary Health Care for Vulnerable Populations: a Scoping Review. Int J Equity Health (2016) 15(1):168–34. doi:10.1186/s12939-016-0459-9
27. Osingada, CP, and Porta, CM. Nursing and Sustainable Development Goals (SDGs) in a COVID-19 World: The State of the Science and a Call for Nursing to lead. Public Health Nurs (2020) 37(5):799–805. doi:10.1111/phn.12776
28. Rosa, WE, Fitzgerald, M, Davis, S, Farley, JE, Khanyola, J, Kwong, J, et al. Leveraging Nurse Practitioner Capacities to Achieve Global Health for All: COVID-19 and beyond. Int Nurs Rev (2020) 67:554–9. doi:10.1111/inr.12632
29.Health – United Nations Sustainable Development. Goal 3: Ensure Healthy Lives and Promote Well-Being for All at All Ages (2021). Available from: https://www.un.org/sustainabledevelopment/health/ (Accessed August 15, 2021).
30. Moher, D, Liberati, A, Tetzlaff, J, Altman, DG, and Group, TP. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Plos Med (2009) 6:e1000097. doi:10.1371/journal.pmed.1000097
31. Johnson, BT, Low, RE, and LaCroix, JM. Systematic Reviews to Support Evidence-Based Medicine (2nd Edition) by Khalid Khan, Regina Kunz, Jos Kleijnen and Gerd Antes: A Review. Res Synth Methods (2013) 4:102–8. doi:10.1002/jrsm.1071
32.Institute of Medicine. Finding what Works in Health Care Standards for Systematic Reviews. Washington, DC: National Academies Press (2011).
33. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 Statement: an Updated Guideline for Reporting Systematic Reviews. BMJ (2021) 372:n71. doi:10.1136/bmj.n71
34. Bautista, CJ. Lectura Crítica de la evidencia clínica (2005). Available from: http://www.redcaspe.org/system/tdf/materiales/cohortes11.pdf?file=1&type=node&id=157&force= (Accessed August 15, 2021).
35. Olivo, SA, Macedo, LG, Gadotti, C, Fuentes, J, Stanton, T, and Magee, DJ. Scales to Assess the Quality of Randomized Controlled Trials: A Systematic Review. Phys Ther (2008) 88:156–75. doi:10.2522/ptj.20070147
36. Lockwood, C, and Oh, EG. Systematic Reviews: Guidelines, Tools and Checklists for Authors. Nurs Health Sci (2017) 19:273–7. doi:10.1111/nhs.12353
37. Carrington, MJ, and Stewart, S. Bridging the gap in Heart Failure Prevention: Rationale and Design of the Nurse-Led Intervention for Less Chronic Heart Failure (NIL-CHF) Study. Eur J Heart Fail (2010) 12(1):82–8. doi:10.1093/eurjhf/hfp161
38. Stewart, S, Wiley, JF, Ball, J, Chan, YK, Ahamed, Y, Thompson, DR, et al. Impact of Nurse-Led, Multidisciplinary Home-Based Intervention on Event-free Survival across the Spectrum of Chronic Heart Disease: Composite Analysis of Health Outcomes in 1226 Patients from 3 Randomized Trials. Circulation (2016) 133(19):1867–77. doi:10.1161/CIRCULATIONAHA.116.020730
39. Stewart, S, Chan, YK, Wong, C, Jennings, G, Scuffham, P, Esterman, A, et al. Impact of a Nurse-Led home and Clinic-Based Secondary Prevention Programme to Prevent Progressive Cardiac Dysfunction in High-Risk Individuals: The Nurse-Led Intervention for Less Chronic Heart Failure (NIL-CHF) Randomized Controlled Study. Eur J Heart Fail (2015) 17(6):620–30. doi:10.1002/ejhf.272
40. Zwar, NA, Bunker, JM, Reddel, HK, Dennis, SM, Middleton, S, van Schayck, OCP, et al. Early Intervention for Chronic Obstructive Pulmonary Disease by Practice Nurse and GP Teams: A Cluster Randomized Trial. Fam Pract (2016) 33(6):663–70. doi:10.1093/fampra/cmw077
41. Wang, Y, Zang, X-Y, Bai, J, Liu, S-Y, Zhao, Y, and Zhang, Q. Effect of a Health Belief Model-Based Nursing Intervention on Chinese Patients with Moderate to Severe Chronic Obstructive Pulmonary Disease: A Randomised Controlled Trial. J Clin Nurs (2014) 23:1342–53. doi:10.1111/jocn.12394
42. Cáceres, F, Bohórquez, F, Puerto, H, and Smith Hernández, D. Eficacia de las intervenciones de enfermería para disminuir el temor en personas que inician tratamiento para el cáncer. Un ensayo clínico controlado. MedUNAB (2010) 7(21):161–5.
43. Rojas-Sánchez, OA, Rueda-Díaz, LJ, Vesga-Gualdrón, LM, Orozco-Vargas, LC, Forero-Bulla, CM, and Camargo-Figuera, FA. [Effectiveness of the Nursing Interventions for the Diagnosis "ineffective Management of Therapeutic Regimen"]. Enferm Clin (2009) 19(6):299–305. doi:10.1016/j.enfcli.2009.05.005
44. Chan, SSC, Leung, DYP, Leung, AYM, Lam, C, Hung, I, Chu, D, et al. A Nurse-Delivered Brief Health Education Intervention to Improve Pneumococcal Vaccination Rate Among Older Patients with Chronic Diseases: A Cluster Randomized Controlled Trial. Int J Nurs Stud (2015) 52(1):317–24. doi:10.1016/j.ijnurstu.2014.06.008
45. Arts, EEA, Landewe-Cleuren, SANT, Schaper, NC, and Vrijhoef, HJM. The Cost-Effectiveness of Substituting Physicians with Diabetes Nurse Specialists: A Randomized Controlled Trial with 2-year Follow-Up. J Adv Nurs (2012) 68(6):1224–34. doi:10.1111/j.1365-2648.2011.05797.x
46. Brotons, C, Falces, C, Alegre, J, Ballarín, E, Casanovas, J, Catà, T, et al. Randomized Clinical Trial of the Effectiveness of a Home-Based Intervention in Patients with Heart Failure: The IC-DOM Study. Rev Esp Cardiol (2009) 62(4):400–8. doi:10.1016/s1885-5857(09)71667-6
47. Pardavila-Belio, MI, Garcia-Vivar, C, Pimenta, AM, Canga-Armayor, A, Pueyo-Garrigues, S, and Canga-Armayor, N. Intervention Study for Smoking Cessation in Spanish College Students: Pragmatic Randomized Controlled Trial. Addiction (2015) 110(10):1676–83. doi:10.1111/add.13009
48. Soto Rodríguez, A, García Soidán, JL, de Toro Santos, M, Lagoa Labrador, F, Failde Garrido, JM, and Pérez Fernández, MR. [Benefits of an Educational Intervention on Diet and Anthropometric Profile of Women with One Cardiovascular Risk Factor]. Med Clin (Barc) (2016) 146(10):436–9. doi:10.1016/j.medcli.2015.12.013
49. Ågren, S, Evangelista, LS, Davidson, T, and Strömberg, A. Cost-effectiveness of a Nurse-Led Education and Psychosocial Programme for Patients with Chronic Heart Failure and Their Partners. J Clin Nurs (2013) 22(15–16):2347–53. doi:10.1111/j.1365-2702.2012.04246.x
50. Brännström, M, and Boman, K. Effects of Person-Centred and Integrated Chronic Heart Failure and Palliative home Care. PREFER: A Randomized Controlled Study. Eur J Heart Fail (2014) 16(10):1142–51. doi:10.1002/ejhf.151
51. Billington, J, Coster, S, Murrells, T, and Norman, I. Evaluation of a Nurse-Led Educational Telephone Intervention to Support Self-Management of Patients with Chronic Obstructive Pulmonary Disease: A Randomized Feasibility Study. COPD (2015) 12(4):395–403. doi:10.3109/15412555.2014.974735
52. Carolina, V, Bueno, B, Andrea, B, Pérez, C, Leidy, J, Trigos, S, et al. Eficacia de la intervención enfermera para cuidadores con cansancio del rol del cuidador. Rev Cubana Enferm (2011) 2727(33):210–9.
53. Soto-Rodríguez, A, García-Soidán, JL, de Toro-Santos, M, Rodríguez-González, M, Arias-Gómez, MJ, and Pérez-Fernández, MR. Ensayo clínico con intervención educativa en mujeres perimenopáusicas con un factor de riesgo cardiovascular. Gac Sanit (2016) 31:48–52. doi:10.1016/j.gaceta.2016.07.022
54. Kennedy, A. Nurses: a Voice to lead in the Battle against Non-communicable Disease. Int Nurs Rev (2018) 65:150–1. doi:10.1111/inr.12461
55. Bloom, DE, Chatterji, S, Kowal, P, Lloyd-Sherlock, P, McKee, M, Rechel, B, et al. Macroeconomic Implications of Population Ageing and Selected Policy Responses. Lancet (2015) 385(9968):649–57. doi:10.1016/S0140-6736(14)61464-1
56. Liu, M, Xue, QL, Gitlin, LN, Wolff, JL, Guralnik, J, Leff, B, et al. Disability Prevention Program Improves Life-Space and Falls Efficacy: A Randomized Controlled Trial. J Am Geriatr Soc (2021) 69(1):85–90. doi:10.1111/jgs.16808
57. Sorensen, A, Grotts, JF, Tseng, CH, Moreno, G, Maranon, R, Whitmire, N, et al. A Collaboration Among Primary Care-Based Clinical Pharmacists and Community-Based Health Coaches. J Am Geriatr Soc (2021) 69:68–76. doi:10.1111/jgs.16839
Keywords: non-communicable diseases, nursing, community health nursing, home nursing, house call, nursing interventions
Citation: Gomez del Pulgar M, Cuevas-Budhart MA, Hernández-Iglesias S, Kappes M, Riquelme Contreras VA, Rodriguez-Lopez E, De Almeida Souza AM, Gonzalez Jurado MA and Crespo Cañizares A (2022) Best Nursing Intervention Practices to Prevent Non-Communicable Disease: A Systematic Review. Public Health Rev 43:1604429. doi: 10.3389/phrs.2022.1604429
Received: 23 August 2021; Accepted: 19 August 2022;
Published: 14 September 2022.
Edited by:
Kaspar Wyss, Swiss Tropical and Public Health Institute (Swiss TPH), SwitzerlandCopyright © 2022 Gomez del Pulgar, Cuevas-Budhart, Hernández-Iglesias, Kappes, Riquelme Contreras, Rodriguez-Lopez, De Almeida Souza, Gonzalez Jurado and Crespo Cañizares. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
PHR is edited by the Swiss School of Public Health (SSPH+) in a partnership with the Association of Schools of Public Health of the European Region (ASPHER)+
*Correspondence: Miguel Angel Cuevas-Budhart, YW5nZWwuYnVkaGFydEBnbWFpbC5jb20=, YW5nZWxfYnVkaGFydEBob3RtYWlsLmNvbQ==, bWlndWVsLmN1ZXZhc0BpbXNzLmdvYi5teA==
This Systematic Review is part of the PHR Special Issue “Health in all Sustainable Development Goals”