 Pedro Henrique Alcântara da Silva1Kezauyn Miranda Aiquoc1Aryelly Dayane da Silva Nunes1Wilton Rodrigues Medeiros1
Pedro Henrique Alcântara da Silva1Kezauyn Miranda Aiquoc1Aryelly Dayane da Silva Nunes1Wilton Rodrigues Medeiros1 Talita Araujo de Souza1*Javier Jerez-Roig2Isabelle Ribeiro Barbosa1
Talita Araujo de Souza1*Javier Jerez-Roig2Isabelle Ribeiro Barbosa1- 1Postgraduate Program in Public Health, Federal University of Rio Grande do Norte, Natal, Brazil
- 2Faculty of Health Sciences and Welfare, University of Vic–Central University of Catalonia, Barcelona, Spain
Objective: To analyze the prevalence of access to prenatal care in the first trimester of pregnancy among black women compared to other races/ethnicities through a systematic review and meta-analysis.
Methods: Searches were carried out at PUBMED, LILACS, Web of Science, Scopus, CINAHL, and in the grey literature. The quality of the studies and the risk of bias were analyzed using the Joanna Briggs Critical Appraisal Checklist for Analytical Cross-Sectional Studies instrument. The extracted data were tabulatesd and analyzed qualitatively and quantitatively through meta-analysis.
Results: Black women had the lowest prevalence of access to prenatal services in the first trimester, with prevalence ranging from 8.1% to 74.81%, while among white women it varied from 44.9 to 94.0%; 60.7% of black women started prenatal care in the first trimester, while 72.9% of white women did so.
Conclusion: Black women compared to other racial groups had lower prevalence of access to prenatal care, with less chance of access in the first trimester, and it can be inferred that the issue of race/skin color is an important determinant in obtaining obstetric care.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020159968_, PROSPERO CRD42020159968.
Introduction
Access to prenatal care is considered one of the main prognostic indicators for a healthy birth, contributing to a delivery with less impact on maternal health. The beginning of prenatal care should occur in the first trimester, as it stratifies pregnancy risk, achieving the appropriate number of consultations, and the performance of the recommended procedures and adequacy definers, avoiding unfavorable obstetric and neonatal outcomes, which may contribute to the reduction of maternal morbidity and mortality [1].
Prenatal care is the period before birth and it is composed of clinical and educational procedures with the goal of monitoring the evolution of the pregnancy. The Brazilian Ministry of Health recommends that prenatal care should start in the first trimester of pregnancy, as it makes it possible to reach the appropriate number of consultations, at least 6 overall, as well as to carry out the recommended procedures that define its suitability such as blood screening tests and fetal monitoring.
People of African descent, in addition to having limited access to health services, quality, and safe housing, also suffer from various discrimination, especially regarding class, race, and gender [1]. These aspects are evident in people of black race/skin color from all over the world. Which has repercussions on the life and death of these individuals [2]. When comparing women of white race/skin color, the black women, the interaction between biological, social, and environmental factors makes them more vulnerable to some diseases such as gestational hypertension and gestational diabetes mellitus [3].
Maternal mortality or pregnancy-related mortality provides one of the most striking examples of disparities in women’s health. Currently, the global maternal mortality ratio is around 210 deaths per 100,000 live births. According to Martins (2006), the Center for Disease Control and Prevention reports a decrease in the coefficients of maternal death in the United States from 319.8 to 5.7/100,000 live births among women white and from 781.7 to 18.6/100 thousand live births among black women, in the period 1940 to 1990. This 2 to 4 times greater ratio for black women is explained by the large number of pregnancy with morbidity, difficulty in accessing and using health services, in addition to the quality of care provided, or care received.
Pachecho (2018), conducted a study in the United Kingdom, identifying that 76,158 pregnant women found the risk of fetal death two times higher in black pregnant women compared to white pregnant women, in addition to significantly higher in all adverse outcomes (low birth weight, preeclampsia, preterm, pregnancy-specific hypertension and gestational diabetes mellitus), except elective cesarean section. There are persistent racial disparities in perinatal outcomes, with neonatal mortality rates in black women twice that of white women and maternal mortality rates in black women three to four times that of white women [4].
Thus, identifying whether the issue of race/skin color directly influences access to maternal health service with studies with greater scientific evidence is necessary, as it can elucidate a racial inequity with fatal consequences [5]. This debate may allow the development of public policies of racial equity in maternal health services with greater technical and scientific support, aiming at improving the quality of care in obstetrics and perineonatology.
Thus, this study aims to analyze the prevalence of access to prenatal care in the first trimester of pregnancy among black women compared to other races/ethnicities in a systematic review and meta-analysis and to identify the magnitude of the association.
Methods
For the writing of this systematic review, we used the guidelines of the PRISMA Checklist (Main Items for Reporting Systematic Reviews and Meta-analyzes) [6]. The initial protocol for this review was registered on the PROSPERO platform under the number CRD42020159968.
In this study, the focused research question was: “What is the prevalence of access to prenatal care in the first trimester of pregnancy in black women compared to other races/ethnicities?” The inclusion and exclusion criteria of the articles obtained during searches in the databases were developed based on the PICO strategy [7] Participants–pregnant women, including adolescents, without nationality restriction at any gestational age; Exposure–black pregnant women; Controls–pregnant women from other ethnic or racial groups; Outcome–access to prenatal care in the first trimester; Type of studies–Cross-sectional studies. Cohort, case-control studies and literature reviews (integrative, narrative, or systematic with or without meta-analysis), case series, case reports, and qualitative studies were not considered.
On 10 October 2019, with a subsequent update on 19 February 2021, the following databases were accessed electronically: LILACS, PubMed, Scopus, Web of Science, and CINAHL, in addition to Google Scholar and the Opengrey.org portal to identify files stored in the grey literature (the gray literature includes dissertations, theses, official government reports), without restriction as to the language of the articles or date of publication. The search strategy combined the Mesh terms for “pregnancy”, “prenatal care” and “Health Services Accessibility”, in addition to related free terms (Table 1). Terms related to race, ethnicity, or skin color were not included, since the combination of these terms did not result in findings relevant to the objectives of this study.
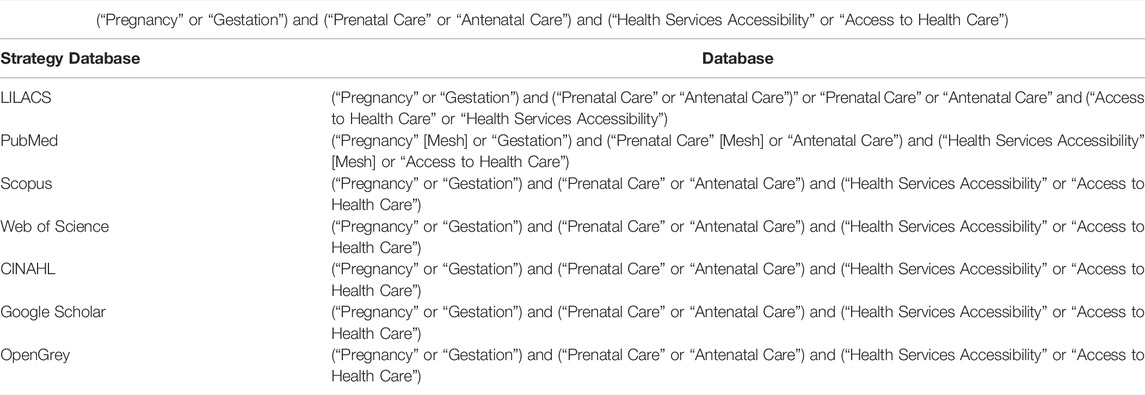
TABLE 1. Search strategy (Brazil, 2021).
Initially, the results obtained in the databases were inserted in the reference manager Mendeley Desktop® version 1.19.4 for the elimination of duplicate studies. Then, the resulting articles were exported to Rayyan QCRI® software to be screened by reading the title and abstract, applying the eligibility criteria. Even using the same software, after the initial screening, the studies selected in the previous step were submitted to full-textual reading to observe the completeness of the articles in the inclusion criteria. From this analysis, studies were obtained to be included in this systematic review and whose data were extracted.
In all stages of study selection, two reviewers trained to select studies, to use analysis software, and to extract data worked independently. To ensure the quality of the process, the divergences were solved by consensus. In cases where the disagreements persisted, a third reviewer was asked to solve the conflicts. The bibliographic references listed in the included studies were also analyzed to identify articles that met the inclusion criteria.
Two reviewers independently extracted study data and discrepancies at this stage were resolved by discussion and consensus. The following information from the observational studies was extracted and presented in a table: 1) Reference of the article (authors, place, year of publication); 2) Sample size; 3) Sociodemographic characteristics (race/ethnicity; the mean age of participants); 4) Prevalence of prenatal consultations in the first trimester of pregnancy; 5) Association measures used.
After reading the full article, the evaluation of the methodological quality of the included studies was carried out with the aid of the critical evaluation tool of cross-sectional studies for use in a systematic review by the Joanna Briggs Institute [8]. This tool consists of eight questions that assess the methodological quality of the study and determine the possibility of bias in its design, conduction, and analysis. Associated with this instrument, the score described by Taylor was used as a strategy to stratify the risk of bias [9]. In it, the studies are classified as “low risk of bias,” if a “yes” score ≥ of 70% is obtained; “Moderate risk of bias,” if the “yes” score is between 50% and 69%; and “high risk of bias,” if the “yes” score is less than 50% [10]. This assessment was carried out independently by the two reviewers and the disagreements were resolved by consensus.
The Review Manager software (RevMan; version 5.3.5–available at: (http://community.cochrane.org/tools/review-production-tools/revman-5/revman-5-download): was used for statistical analysis of results and construction of the meta-analysis graphs, using the random-effects model and Odds Ratio (OR) as a measure of association for dichotomous data, with a 95% confidence interval (CI).
We quantify the inconsistencies between the results of the studies using the I2 statistic, which illustrates the percentage of variability in the effect estimates that surpasses the effect of chance: I2 = [(Q–df)/Q] x 100%, where Q is the statistic Chi [2] and df the degree of freedom. We evaluated the heterogeneity between the studies with a visual examination of the meta-analysis graphs to verify overlapping of the confidence intervals, using the Chi [2] test for homogeneity with a significance level of 5% and considering the I2 statistic [8]. An I2 value of less than 50% corresponded to low heterogeneity; 50% or greater, significant heterogeneity and 75% or greater, substantial heterogeneity [8].
This study received support from the Coordination for the Improvement of Higher Education Personnel (CAPES) through payment of a master’s scholarship [001] and Federal University of Rio Grande do Norte.
Results
We identified 2,840 articles for screening by title and abstract. This evaluation resulted in 264 articles for full reading and 19 studies were then selected to compose this systematic review, being subjected to evaluation of the methodological quality and data extraction (Figure 1).
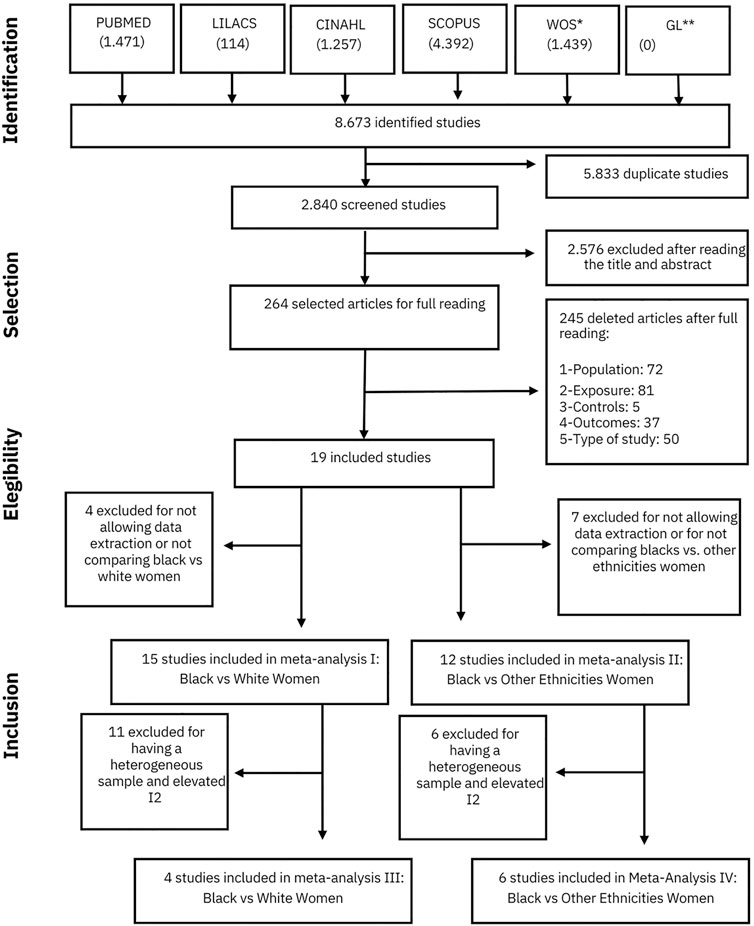
FIGURE 1. Flowchart for Article Selection Caption: * Web of Science; **Grey Literature Source: Designed by the authors (Brazil, 2021).
From the data obtained (Table 2), we found that the studies used the same gestational age (<12 weeks) to define the beginning of prenatal care. The population studied was described by ethnic groups (white, Asian, Hispanic, Latino), and also grouped into age group. For this characteristic, there is a great variety of presentations through age groups, and only one study [11] diverged, analyzing only pregnant adolescents.
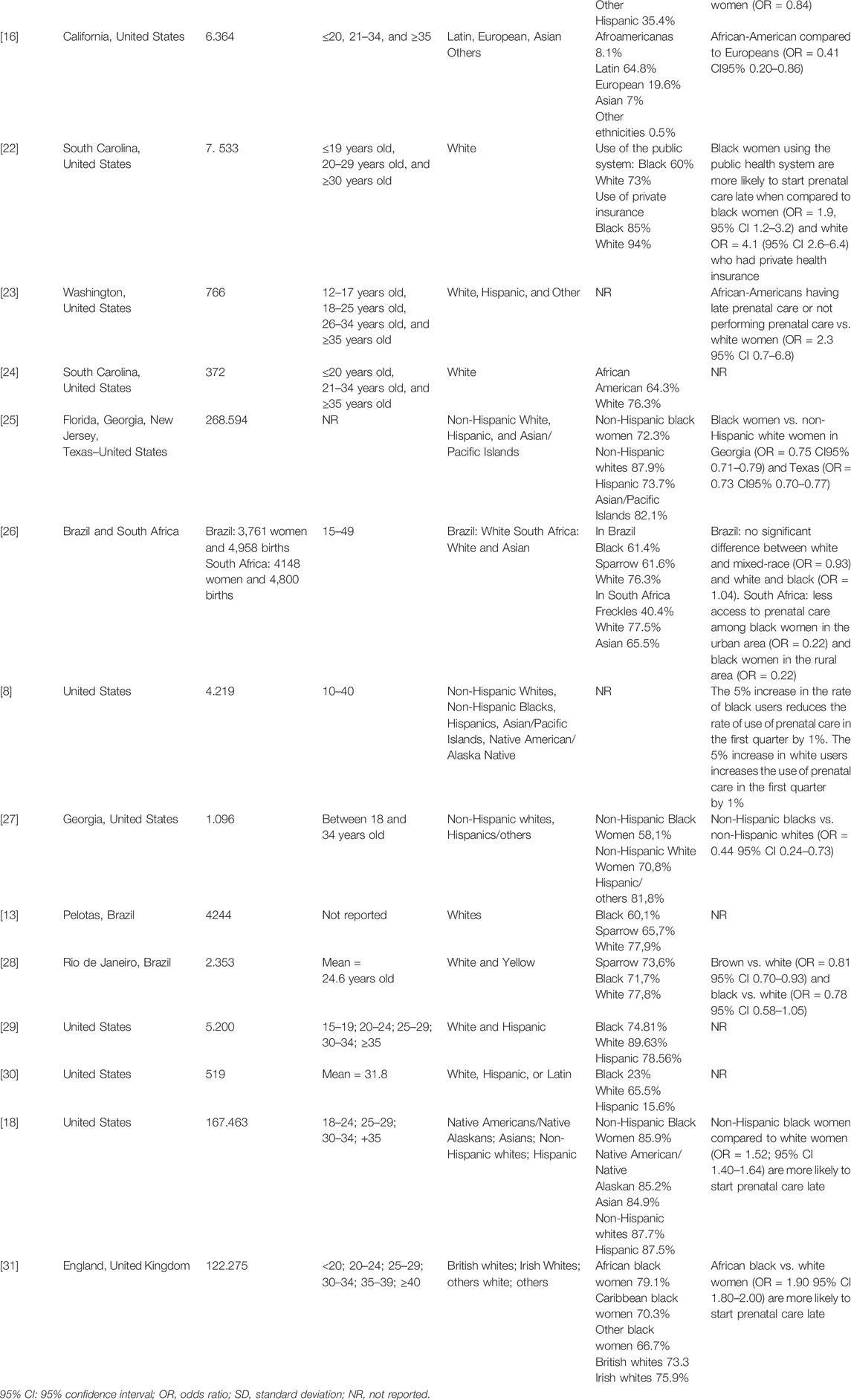
TABLE 2. Characteristics of the included studies (n = 19) (Brazil, 2021).
Most of the studies articles are from the United States of America; only two were Brazilian [12, 13].
In general, there is a significant difference between the racial groups studied in the included articles. Black women, when compared to other ethnicities, have a lower prevalence of early prenatal care in the first trimester, with prevalence ranging from 8.1% to 74.81%, while compared to white women, it varied from 44.9 to 94.0%.
After applying the analysis instrument for the risk of bias (Table 3), we observed that only four studies (21%) [14–18] have a moderate risk of bias, with the others considered low risk. Then, the selected articles have good methodological quality, adequately answer their research questions, allowing their results to be generalized.
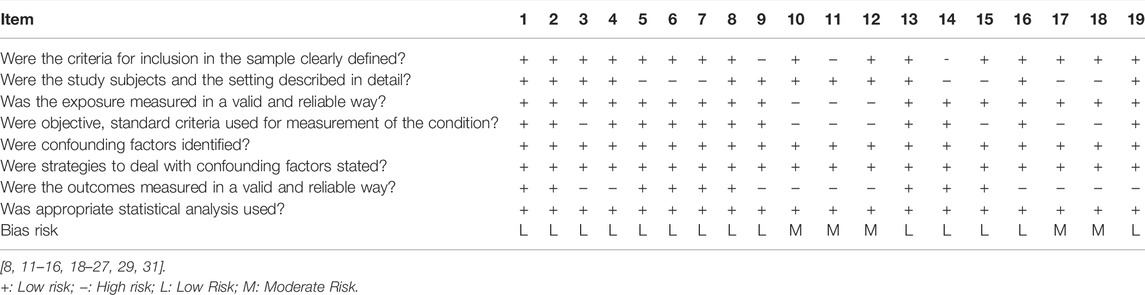
TABLE 3. Methodological quality and bias risk analysis according to Joanna Briggs critical appraisal checklist for analytical cross-sectional studies (Brazil, 2021).
Only 15 (78.9%) of the 19 studies included in the systematic review were included in meta-analysis I (black women versus white women); and 11 (57.9%) entered the meta-analysis II (black women compared to women of other ethnicities, except white). This is because from the data presented, it was not possible to extract the number of black women or other ethnicities belonging to the sample, or they did not make a comparison between whites and blacks or between blacks and other ethnicities.
In meta-analysis I (Figure 2), we included 199,889 black women and 407,930 white women. We observed that 60.7% (95% CI = 60.5–60.9) of black women started prenatal care in the first trimester, while 72.9% (95% CI = 72.8–73.0) of white women did so. Black women are less likely to start their obstetric care early, with an OR of 0.56 (95% CI 0.43–0.74) compared to white women.
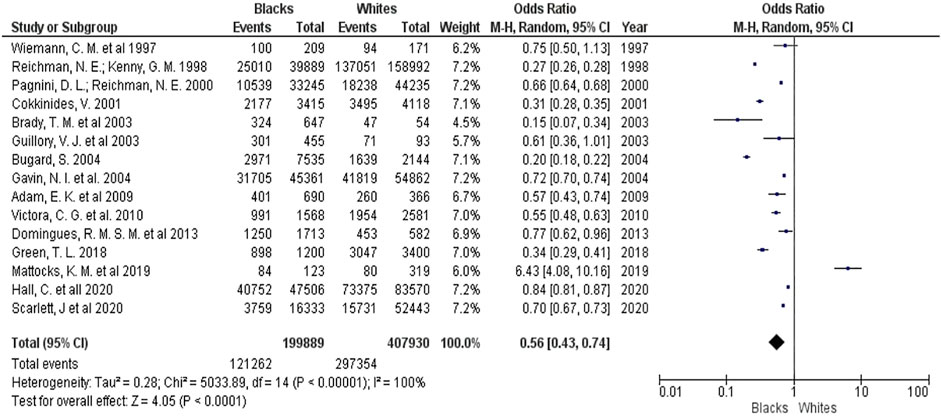
FIGURE 2. Forest Plot for the Early Start of Prenatal Care: Black women compared to white women (Brazil, 2021).
However, the included studies are quite heterogeneous with I2 = 100% and the funnel plot (Figure 3) presents studies with varying data accuracy and outside the area covered by the plot, suggesting the presence of potential publication bias.
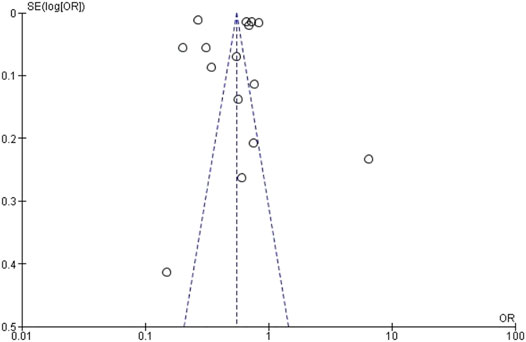
FIGURE 3. Funnel Plot for early prenatal care: black women compared to white women (Brazil, 2021).
When comparing black women with women of other ethnicities (except white)–meta-analysis 2, we included 153,593 black women and 111,002 women of other ethnicities (Supplementary File S1), showing that the chances of black women starting prenatal care at the age of the first trimester are the same as women from other ethnic minorities (OR = 1.0; 95% CI 0.90–1.10) (Supplementary File S1).
Even so, we found a high heterogeneity (I2 = 91%) with the Funnel plot presenting studies with varying data accuracy and suggesting potential publication bias. (Supplementary File S2).
In an attempt to solve the high heterogeneity in the first two meta-analyses, two other meta-analyses were carried out grouping studies with methodologies and samples with similar characteristics (Supplementary File S3).
In this analysis, we studied 2,922 black women and 3,211 white women. We observed that 61.3% of black women start prenatal care in the first trimester, while for white women the prevalence was 74%. The result of the meta-analysis showed that the summary measure was OR = 0.57 (95% CI 0.51–0.64), which means that black women are 43% less likely to start prenatal care in the first trimester (Supplementary File S4), obtaining an I2 = 0% (Supplementary File S4).
In the following analysis, we compared 26,047 black women with 22,953 non-black women belonging to other ethnicities (excluding white ones), noting that black women have 16% less chance of gaining access to these services (OR = 0.84; 95% CI 0.71–0.99), with an I2 = 50% (Supplementary Files S5, S6).
Discussion
This study aimed to analyze the prevalence of access to prenatal care during the first trimester of pregnancy by black pregnant women compared to white women and other ethnicities. As the results show, the prevalence of access to this service was lower among black women, varying from 8.1% to 74.81%, with fewer chances of accessing prenatal care than white women (OR = 0.57, 95% CI 0.51–0.64) and women of other ethnicities (OR = 0.84, 95% CI 0.71–0.99).
Another study showed that race and ethnicity are significant predictors for access to antenatal care [32]. White and Asian women, when compared to black or African American women, had significantly greater chances of punctuality in prenatal care (OR 1.59 and 1.87, respectively) and frequency of prenatal care (OR 1.89 and 2.44, respectively) [32] which shows inequality in access not only in comparison to white women but also to other minorities.
From the qualitative assessment of the studies included in this review, we observed that 16 studies are from the US, 2 from Brazil, and 1 from England. The US and Brazil are two multiracial nations, with a colonialist and slavery background, which allows us to reflect on the importance of this context on how racial discrimination was shaped.
In a study in the US, authors identified that preterm and very premature births, as well as delayed prenatal care, in addition to being reported more frequently by black women compared to white women, were also associated with geographical factors and sociodemographic. It was more frequent in black women living in the southern US and counties with a high rate of racial segregation [33]. This may explain the findings of this review, in which most of the studies were conducted in the states of Texas [11], California [16, 20], Carolina do South [22, 24, 27], and the study by Gavin et al [25] that analyzed data from both Florida, Georgia and Texas and New Jersey. It is noteworthy that the results presented may not be globally representative, but specific to the countries of the inserted studies.
The race/skin color item has been widely used in clinical and public health studies as a variable, especially in the US to assess social inequities in health outcomes and treatments [34]. In that country, a vast literature defines race as an important health predictor and demonstrates that blacks are at a disadvantage when compared to whites [26].
However, in Brazil, there are still few studies that associate race as a variable that defines social inequities, especially about women’s health [2], because the connotation that this condition has acquired throughout history differs from that adopted by North Americans. For a long time, it was related to the skin color phenotype and the characteristics of the individuals and not the ancestry, added to its absence as a question of filling in censuses and health notification/information systems [35].
Another review identified that in Brazilian scientific production, only 19 studies addressed institutional racism and the health of black women [36]. The scarcity of studies on the health of black women may be a consequence of epistemic racism [2, 36, 37]. Besides making difficult to advance and consolidate the debate regarding racial inequalities associated with socioeconomic factors in health outcomes, this facto also contributes to the perpetuation of institutional racism in Brazil.
Despite these differences, the associated analysis of studies from both countries is possible due to the presence of similarities between them. In addition, both nations have reported high levels of race-related discrimination in interpersonal settings and education and health institutions [26].
Most of the American articles included are with subjects belonging to States where the African-American population is higher such as Georgia, Florida, New Jersey, New York, California, and Texas. These studies are similar as they analyzed women who used the services of MEDICAID, Federal and State health insurance for the health of pregnant women, children, the older people over 65, people with physical and intellectual disabilities, and low-income adults. Brazilian studies, when compared to American studies, have a similar methodological design, as they approached women users of the Brazilian Unified Health System (SUS), comparing them in terms of race, income, education, parity, marital status, and age group.
In this context, one of the limitations observed in the studies included in this work is the way in which race was measured. In biomedical literature, there is a consensus that racial/ethnic categories are inaccurate and changeable, and that their measurement in census and health data varies over time [26].
All included studies were submitted to methodological quality assessment and 14 studies had a low risk of bias, which shows the good methodological quality of the included studies. The main limitations found in most studies were related to failures in filling the item race or skin color in health records in some countries, which can generate information bias. In studies carried out in US, data on skin color came from databases of vital statistics and questionnaires sent electronically to participants, in which the fields referring to color/race were self-reported. In addition, the population classified as Latin was not stratified as white Latinos or black Latinos. In Brazilian studies, this variable was measured both by the participants’ self-declaration and by the interviewer’s judgment.
Also, the findings found here are the results of an analysis of observational studies of cross-sectional design, constituting one of the limitations of this review. The inclusion of only articles of this nature can lead to generalized conclusions since the confounding factors are not always adjusted properly, as they are analyzed at the same time. The lack of identification of confounding factors and the strategies to deal with these factors, mainly in studies carried out in the 1990s and early 2000s, were seen from the assessment of the risk of bias.
The high heterogeneity found in the first two meta-analyses carried out with all eligible studies and comparing black and white women; and black women and other ethnicities (except white), can be explained by an overestimated measure of association, based on studies with varying sample sizes, studies that included women with access to private services, who analyzed drug users and that focused only on teenagers.
Considering this and as a strategy to try to minimize the high heterogeneity obtained, we carried out two other meta-analyses, combining studies with participants with similar sociodemographic characteristics. Therefore, results were obtained with low heterogeneity and low publication bias, in addition to high data accuracy. Given these findings, we can assume that the difficulty in accessing black women to prenatal care is not, in fact, only related to socioeconomic status, and maybe the consequence of a much broader and more complex process such as racism.
Even when evaluated together with white women or other ethnicities with similar sociodemographic characteristics and being users of public health services, black women still have little or no participation in prenatal services [38, 39].
Black women are not carefully monitored like white women and, when they have symptoms, most of the time, they are not followed up with due attention [40]. Differences like these occur well before the patient arrives at the place of care and extend through direct care or gaps in communication between health professionals. Among other factors, the explanation for this phenomenon lies in the stereotype formed about people of black color and in racism, affecting the way they are treated in health services [40].
Racism consists of a system of oppression that gives value to people, based on race or ethnicity. There are categories of racism that can contribute to the increase in racial health disparities: 1) institutional racism; 2) personal racism; and 3) internalized racism. Everyone plays an important role in the negative experiences lived by black women during their sexual and reproductive trajectory [41].
Institutional racism is characterized by practices imposed by health organizations that negatively affect user access to the most diverse levels of care, resulting in differences in the quality of service offered to minority racial groups. This category of discrimination promotes attitudes, practices, beliefs, and policies that give advantages to whites and disadvantages to other ethnic groups [41].
Although government policies are created in an attempt to generate social changes that lead to equity of access [42], institutional racism is considered the source of social disparities in health, affecting treatment, the quality of care provided, extending to opportunities for housing, education, and employment [40].
Within these institutions with a discriminatory context, service users can also experience personal racism when the preconceived judgment of health professionals about certain racial groups, resulting in care below the standard provided for ethnic/racial majorities [43].
This type of behavior is seen in the stereotyped attitudes of doctors during their treatment recommendations for black patients, who are seen as promiscuous, receiving inferior and deficient treatments and delays in the screening inherent to prenatal care as rapid tests for the detection of syphilis and HIV in pregnancy, Pap smear exam, Pap smear, performed to track HPV-related pathologies [44, 45].
Finally, considered as a consequence of the previous two levels of discrimination, internalized racism refers to the acceptance and personification of society’s stigmatizing messages and attitudes by the oppressed racial groups. The internalization of these concepts has a major impact on the sexual and reproductive health of these women, causing psychological stress, use of illicit substances, and multimorbidities (gestational diabetes mellitus, gestational hypertension, premature birth, low birth weight), in addition to delaying the search for care, due to the fear, even if unconscious, of experiencing institutional and personal racism [41].
Given the above, studies that make associations between racism and the health of the black population are fundamental as thematic fields of research to observe their repercussions, impact, and ways of coping. Understanding the impact of racism on the sexual and reproductive health of women of African descent provides the context for analyzing the results obtained. The historical and contemporary health experiences of black women provide a perspective that can be considered by health professionals and others who offer services and implement programs, aiming at greater equity for these women.
Conclusion
Black women have a lower prevalence of participation in prenatal care in the first trimester, ranging from 8.1% to 74.81%, with lower chances of accessing prenatal care when compared to white women and women of other ethnicities. The contribution of this study is to raise the discussion about the impact that racial inequity has on the health of individuals, encourage new studies that include the question of race or skin color in their analyzes, in addition to highlighting the need for adjustments between different ethnic-racial classifications.
The study results reveal a current and emerging theme to be worked on globally. Structural racism is present within health services, this practice contributes to the worst health indicators of the black population, as evidenced in this review. It is necessary to turn the attention of public health care policies to this population, in order to recover the long historical process of existing racism, so that all women are treated equally, in addition to working on changes in professional practice, encouraging behavioral changes that reflect on maternal health care.
Author Contributions
PS, KA, AS, and IB conceived of the study and compiled the data used in analyses. PS and KA conducted analyses and drafted the manuscript. PS, KA, AS, WM, TS, JJ-R, and IB assisted with interpretation of the data and provided feedback for this manuscript. All authors read and approved the final manuscript.
Funding
Dean of postgraduate studies at the Federal University of Rio Grande do Norte.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.ssph-journal.org/articles/10.3389/phrs.2022.1604400/full#supplementary-material
Supplementary File S1 | Forest Plot Early prenatal care: black women compared to women of other 517 ethnicities (except white) (Brazil, 2021).
Supplementary File S2 | Funnel Plot for Early onset of prenatal care: black women compared to 520 women of other ethnicities (except white) (Brazil, 2021).
Supplementary File S3 | Forest Plot Early onset of prenatal care: black women compared to white 523 women (Brazil, 2021).
Supplementary File S4 | Funnel Plot Early onset of prenatal care: black women compared to white 526 women (Brazil, 2021).
Supplementary File S5 | Forest Plot Early Start of Prenatal Care: Blacks compared to Other 529 Ethnicities (Brazil, 2021).
Supplementary File S6 | Funnel Plot Early onset of prenatal care: black women compared to other 532 ethnicities (Brazil, 2021).
References
1. Rodrigues, Q. Desigualdades raciais no acesso de mulheres ao cuidado pré-natal e no parto. 2009. 98f. Doctoral dissertation, Dissertação (Mestrado em Enfermagem). Salvador, Brazil: Escola de Enfermagem, Universidade Federal da Bahia (2009).
2. Werneck, J. Racismo institucional e saúde da população negra. Saude Soc (2016). 25:535–49. doi:10.1590/s0104-129020162610
3. Perpétuo, IHO. Raça e acesso às ações prioritárias na agenda da saúde reprodutiva. Anais (2016). 2016:1–14.
4. Berg, C, Atrash, H, Koonin, L, and Tucker, M. Pregnancy-related Mortality in the united states, 1987-1990. Obstet Gynecol (1996). 88(2):161–7. doi:10.1016/0029-7844(96)00135-4
5. Grobman, WA, Bailit, JL, Rice, MM, Wapner, RJ, Reddy, UM, Varner, MW, et al. Racial and Ethnic Disparities in Maternal Morbidity and Obstetric Care. Obstet Gynecol (2015). 125(6):1460–7. doi:10.1097/aog.0000000000000735
6. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. Updating Guidance for Reporting Systematic Reviews: Development of the PRISMA 2020 Statement. J Clin Epidemiol (2021). 134:103–12. doi:10.1016/j.jclinepi.2021.02.003
7. Moola, S, Munn, Z, Tufanaru, C, Aromataris, E, Sears, K, Sfetcu, R, et al. Checklist for Analytical Cross Sectional Studies. In: Joanna Briggs Institute Reviewer’s Manual [Internet]. Adelaide, Australia: The Joanna Briggs Institute (2017).
8. Shi, L, Stevens, GD, Wulu, JT, Politzer, RM, and Xu, J. America's Health Centers: Reducing Racial and Ethnic Disparities in Perinatal Care and Birth Outcomes. Health Serv Res (2004). 39(6p1):1881–902. doi:10.1111/j.1475-6773.2004.00323.x
9. Bryant, AS, Worjoloh, A, Caughey, AB, and Washington, AE. Racial/ethnic Disparities in Obstetric Outcomes and Care: Prevalence and Determinants. Am J Obstet Gynecol (2010). 202(4):335–43. doi:10.1016/j.ajog.2009.10.864
10. Polmann, H, Domingos, FL, Melo, G, Stuginski‐Barbosa, J, Guerra, ENDS, Porporatti, AL, et al. Association between Sleep Bruxism and Anxiety Symptoms in Adults: A Systematic Review. J Oral Rehabil (2019). 46(5):482–91. doi:10.1111/joor.12785
11. Wiemann, CM, Berenson, AB, Pino, LG-d., and McCombs, SL. Factors Associated with Adolescents' Risk for Late Entry into Prenatal Care. Fam Plann Perspect (1997). 29:273–6. doi:10.2307/2953416
12. Domingues, RMSM, Leal, MDC, Hartz, ZMDA, Dias, MAB, and Vettore, MV. Access to and utilization of prenatal care services in the Unified Health System of the city of Rio de Janeiro, Brazil. Rev Bras Epidemiol (2013). 16(4):953–65. doi:10.1590/s1415-790x2013000400015
13. Victora, C, Matijasevich, A, Silveira, M, Santos, I, Barros, A, and Barros, F. Socio-economic and Ethnic Group Inequities in Antenatal Care Quality in the Public and Private Sector in Brazil. Health Pol Plann (2010). 25(4):253–61. doi:10.1093/heapol/czp065
14. Kalmuss, D, and Fennelly, K. Barriers to Prenatal Care Among Low-Income Women in New York City. Fam Plann Perspect (1990). 22:215–31. doi:10.2307/2135495
15. Mattocks, KM, Baldor, R, Bean-Mayberry, B, Cucciare, M, Gerber, MR, Goldstein, KM, ..., , Hammer, KD, Hill, EE, Kroll-Desrosiers, A, Prochazka, AV, Sadler, AG, and Bastian, L. Factors Impacting Perceived Access to Early Prenatal Care Among Pregnant Veterans Enrolled in the Department of Veterans Affairs. Women's Health Issues (2019). 29(1):56–63. doi:10.1016/j.whi.2018.10.001
16. Nothnagle, M, Marchi, K, Egerter, S, and Braveman, P. Risk Factors for Late or No Prenatal Care Following Medicaid Expansions in California. Matern Child Health J (2000). 4(4):251–9. doi:10.1023/a:1026647722295
17. Psicossocial, A. O quesito raça/cor nos estudos de caracterização de usuários de Centro de. Saúde Soc (2017). 26(1):100–14. doi:10.1590/s0104-12902017164968
18. Hall, C, Bukowinski, AT, McGill, AL, You, WB, Gumbs, GR, Wells, NY, et al. Racial Disparities in Prenatal Care Utilization and Infant Small for Gestational Age Among Active Duty US Military Women. Matern Child Health J (2020). 24(7):885–93. doi:10.1007/s10995-020-02941-3
19. Reichman, NE, and Kenney, GM. Prenatal Care, Birth Outcomes and Newborn Hospitalization Costs: Patterns Among Hispanics in New Jersey. Fam Plann Perspect (1998). 30:182–200. doi:10.2307/2991681
20. Braveman, P, Marchi, K, Egerter, S, Pearl, M, and Neuhaus, J. Barriers to Timely Prenatal Care Among Women with Insurance: the Importance of Prepregnancy Factors*1. Obstet Gynecol (2000). 95(6):874–80. doi:10.1016/s0029-7844(00)00780-8
21. Pagnini, DL, and Reichman, NE. Psychosocial Factors and the Timing of Prenatal Care Among Women in New Jersey's HealthStart Program. Fam Plann Perspect (2000). 32:56–64. doi:10.2307/2648213
22. Cokkinides, V. Health Insurance Coverage-Enrollment and Adequacy of Prenatal Care Utilization. J Health Care Poor Underserved (2001). 12(4):461–73. doi:10.1353/hpu.2010.0815
23. Brady, TM, Visscher, W, Feder, M, and Burns, AM. Maternal Drug Use and the Timing of Prenatal Care. J Health Care Poor Underserved (2003). 14(4):588–607. doi:10.1353/hpu.2010.0700
24. Guillory, VJ, Samuels, ME, Probst, JC, and Sharp, G. Prenatal Care and Infant Birth Outcomes Among Medicaid Recipients. J Health Care Poor Underserved (2003). 14(2):272–89. doi:10.1353/hpu.2010.0734
25. Gavin, NI, Adams, EK, Hartmann, KE, Benedict, MB, and Chireau, M. Racial and Ethnic Disparities in the Use of Pregnancy-Related Health Care Among Medicaid Pregnant Women. Matern Child Health J (2004). 8(3):113–26. doi:10.1023/b:maci.0000037645.63379.62
26. Burgard, S. Race and Pregnancy-Related Care in Brazil and South Africa. Soc Sci Med (2004). 59(6):1127–46. doi:10.1016/j.socscimed.2004.01.006
27. Adams, EK, Gavin, NI, Raskind-Hood, C, and Tao, G. Explaining Racial Differences in Prenatal Care Initiation and Syphilis Screening Among Medicaid-Covered Pregnant Women. J Health Care Poor Underserved (2009). 20(1):177–93. doi:10.1353/hpu.0.0099
28. Taylor, CR, Alexander, GR, and Hepworth, JT. Clustering of U.S. Women Receiving No Prenatal Care: Differences in Pregnancy Outcomes and Implications for Targeting Interventions. Matern Child Health J (2005). 9(2):125–33. doi:10.1007/s10995-005-4869-3
29. Green, TL. Unpacking Racial/ethnic Disparities in Prenatal Care Use: the Role of Individual-, Household-, and Area-Level Characteristics. J Women's Health (2018). 27(9):1124–34. doi:10.1089/jwh.2017.6807
30. Thiel de Bocanegra, H, Braughton, M, Bradsberry, M, Howell, M, Logan, J, and Schwarz, EB. Racial and Ethnic Disparities in Postpartum Care And contraception in California's Medicaid Program. Am J Obstet Gynecol (2017). 217(1):47–e7. doi:10.1016/j.ajog.2017.02.040
31. McDonald, H, Moren, C, and Scarlett, J. Health Inequalities in Timely Antenatal Care: Audit of Pre- and post-referral Delays in Antenatal Bookings in London 2015-16. J Public Health (2020). 42(4):801–15. doi:10.1093/pubmed/fdz184
32. Parekh, N, Jarlenski, M, and Kelley, D. Prenatal and Postpartum Care Disparities in a Large Medicaid Program. Matern Child Health J (2018). 22(3):429–37. doi:10.1007/s10995-017-2410-0
33. Thoma, ME, Drew, LB, Hirai, AH, Kim, TY, Fenelon, A, and Shenassa, ED. Black-White Disparities in Preterm Birth: Geographic, Social, and Health Determinants. Am J Prev Med (2019). 57(5):675–86. doi:10.1016/j.amepre.2019.07.007
34. Petruccelli, JL. Raça, etnicidade e origem nos censos de EUA, França, Canadá e Grã-Bretanha. Estud Afro-asiát (2002). 24(3):533–62. doi:10.1590/s0101-546x2002000300005
35. da Silva Nunes, AD, Amador, AE, Dantas, APDQM, de Azevedo, UN, and Barbosa, IR. Acesso à assistência pré-natal no Brasil: análise dos dados da Pesquisa Nacional de Saúde. Revista Brasileira em Promoção da Saúde (2017). 30(3):6158. doi:10.5020/18061230.2017.6158
36. Oliveira, BMC, and Kubiak, F. Racismo institucional e a saúde da mulher negra: uma análise da produção científica brasileira. Saúde debate (2019). 43:939–48. doi:10.1590/0103-1104201912222
37. Cruz, ICFD. A sexualidade, a saúde reprodutiva e a violência contra a mulher negra: aspectos de interesse para assistência de enfermagem. Rev Esc Enferm USP (2004). 38(4):448–57. doi:10.1590/s0080-62342004000400011
38. Silveira, MMP. Influência do tempo de remoção da paciente para a maternidade de alta complexidade e desfecho desfavorável [dissertação]. Salvador: Escola Bahiana de Medicina e Saúde Pública (2015).
39. Howell, EA, Egorova, N, Balbierz, A, Zeitlin, J, and Hebert, PL. Black-white Differences in Severe Maternal Morbidity and Site of Care. Am J Obstet Gynecol (2016). 214(1):122–7. doi:10.1016/j.ajog.2015.08.019
40. Prather, C, Fuller, TR, Marshall, KJ, and Jeffries, WL. The Impact of Racism on the Sexual and Reproductive Health of African American Women. J Women's Health (2016). 25(7):664–71. doi:10.1089/jwh.2015.5637
41. Jones, CP. Levels of Racism: a Theoretic Framework and a Gardener's Tale. Am J Public Health (2000). 90(8):1212–5. doi:10.2105/ajph.90.8.1212
42. Elias, A, and Paradies, Y. The Costs of Institutional Racism and its Ethical Implications for Healthcare. Bioethical Inq (2021). 18(1):45–58. doi:10.1007/s11673-020-10073-0
43. Quadros, Ad., Lemes, TS, Fernandes, MTC, and Paungartner, LM. Racismo Institucional: Uma Revisão Integrativa Sobre a Saúde Da População Negra/Institutional Racism: an Integrative Review on the Health of the Black Population. Bjd (2020). 6(10):81483–92. doi:10.34117/bjdv6n10-538
44. Van Ryn, M, Burgess, DJ, Dovidio, JF, Phelan, SM, Saha, S, Malat, J, ..., , Griffin, JM, Fu, SS, and Perry, S. The Impact of Racism on Clinician Cognition, Behavior, and Clinical Decision Making. Du Bois Rev (2011). 8(1):199–218. doi:10.1017/s1742058x11000191
45. Randolph, SD, Golin, C, Welgus, H, Lightfoot, AF, Harding, CJ, and Riggins, LF. How Perceived Structural Racism and Discrimination and Medical Mistrust in the Health System Influences Participation in HIV Health Services for Black Women Living in the United States South: A Qualitative, Descriptive Study. J Assoc Nurses AIDS Care (2020). 31(5):598–605. doi:10.1097/jnc.0000000000000189
Keywords: systematic review, prenatal care, access to health services, racial factors, black women
Citation: Silva PHAd, Aiquoc KM, Silva Nunes ADd, Medeiros WR, Souza TAd, Jerez-Roig J and Barbosa IR (2022) Prevalence of Access to Prenatal Care in the First Trimester of Pregnancy Among Black Women Compared to Other Races/Ethnicities: A Systematic Review and Meta-Analysis. Public Health Rev 43:1604400. doi: 10.3389/phrs.2022.1604400
Received: 11 August 2021; Accepted: 23 May 2022;
Published: 04 July 2022.
Edited by:
Kasia Czabanowska, Maastricht University, NetherlandsCopyright © 2022 Silva, Aiquoc, Silva Nunes, Medeiros, Souza, Jerez-Roig and Barbosa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
PHR is edited by the Swiss School of Public Health (SSPH+) in a partnership with the Association of Schools of Public Health of the European Region (ASPHER)+
*Correspondence: Talita Araujo de Souza, dGFsaXRhYXJhdWpvMjNAaG90bWFpbC5jb20=