 Esteban Ortiz-Prado1*
Esteban Ortiz-Prado1* Isaac Alexander Suárez Sangucho1
Isaac Alexander Suárez Sangucho1 W. Ricardo Cañizares Fuentes2Jorge Vasconez-Gonzalez1Juan S. Izquierdo-Condoy1
W. Ricardo Cañizares Fuentes2Jorge Vasconez-Gonzalez1Juan S. Izquierdo-Condoy1- 1One Health Research Group, Universidad de Las Américas, Quito, Ecuador
- 2Universidad Católica de Santiago de Guayaquil UCSG y Universidad de Guayaquil UG, Guayaquil, Ecuador
Commentary Letter
In the past three decades, Ecuador’s health system has faced frequent ministerial turnover, often appointing leaders with limited training in public health policy and management. Although many ministers have strong clinical backgrounds, their lack of public health expertise has hindered a cohesive vision, raising concerns about the leadership’s capacity to tackle the nation’s complex health challenges effectively. The Ministry of Health is responsible for upholding the right to health, promoting health, preventing diseases, overseeing surveillance, and providing integrated care. It also develops clinical protocols and management guidelines, delivers health services, and conducts studies comparing national and international health management best practices [1, 2]. To adequately fulfill these responsibilities, a master’s degree in public health should be the minimum requirement for those considered for the position of Minister of Health. While ministers are indeed supported by technical personnel, they must have enough training to understand technical matters and not be overly reliant on staff or influenced by conflicts of interest [3]. Advanced public health training equips leaders with essential knowledge about financing, management, cost-effectiveness, and health communication, enabling them to evaluate and implement comprehensive health policies [4, 5].
A health minister requires both managerial skills to oversee health services and advocacy skills to ensure that potential effects on population health are integrated into the work of other government departments and ministries [6]. Helath Ministers require strong knowledge of epidemiology and public health preparedness, highlighted by challenges from global health crises like COVID-19. However, the Ministry faces internal issues impacting ministerial effectiveness, including overlapping responsibilities in regulations, unclear accountability, fragmented technical programs, and departments prioritizing specific professions over broader functions [7]. Furthermore, governance within the health sector is heavily influenced by institutional power dynamics. This lack of governance can severely hinder the performance of the Ministry of Health, contributing to systemic failures [8, 9].
Over the past 30 years in Ecuador, most health ministers have lacked advanced degrees or experience in key areas such as public health, epidemiology, or health systems management (see Table 1). This absence of qualifications hinders effective public health leadership, which demands an integrated, evidence-based approach to address social, environmental, and behavioral health determinants [10–13].
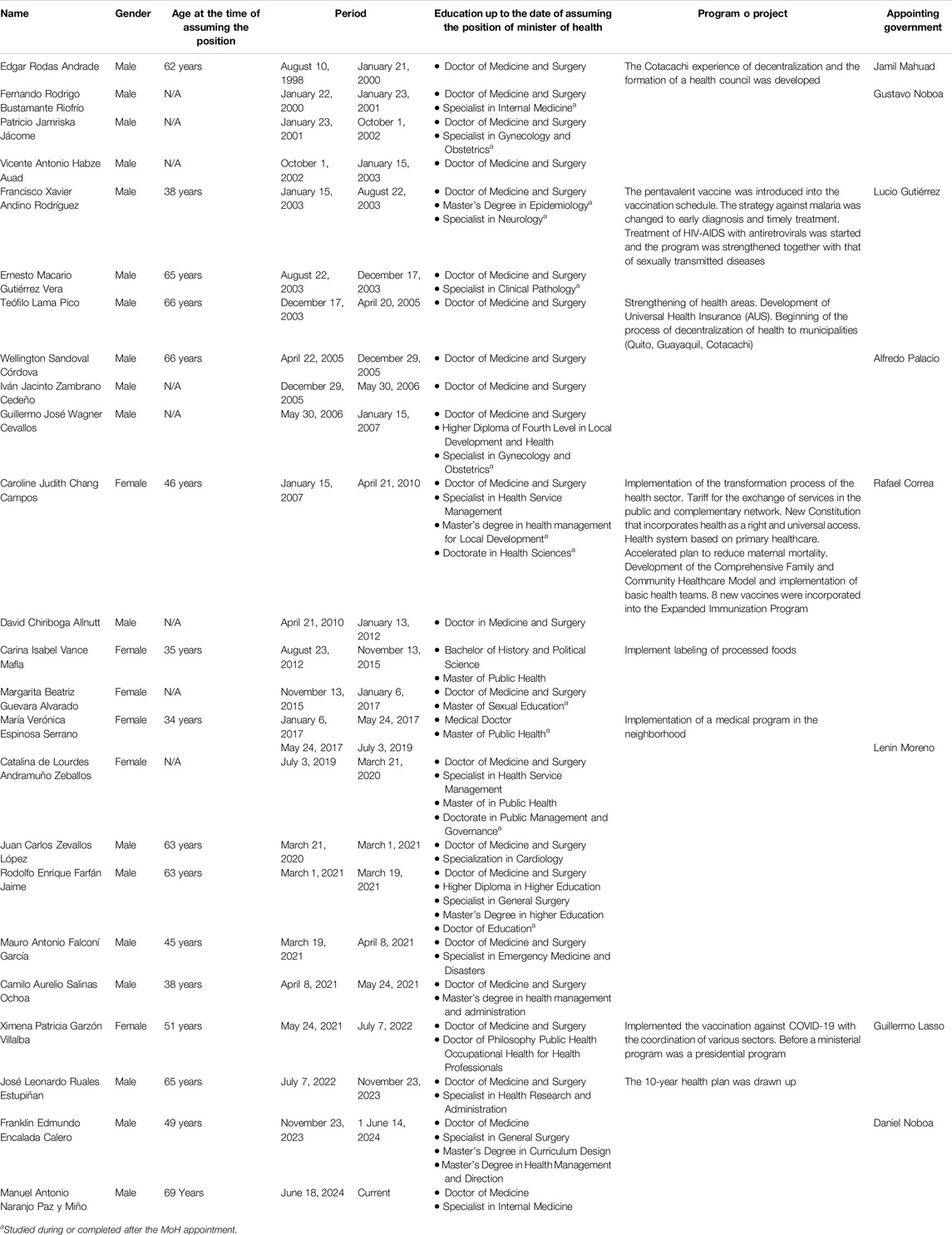
Table 1. Description of ministers of the Ministry of Public Health of Ecuador during the 21st century.
Although the primary role of a health minister is to manage and oversee the national health system, their responsibility also extends to proposing public policies that can be evaluated through tangible improvements in health indicators, such as infant mortality. We believe that this is a significant issue for health governance. Therefore, we conducted an analysis based on the significant reductions in infant mortality during specific periods, identifying the ministers in charge and the outcomes associated with their tenure, highlighting changes that could reflect the impact of effective leadership and policy implementation (Figure 1).
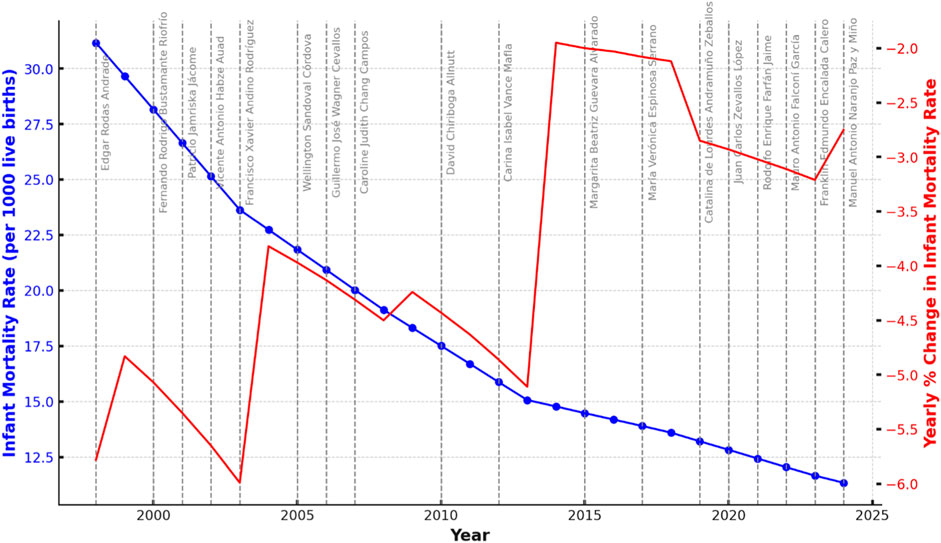
Figure 1. Trends in Infant Mortality Rate in Ecuador (1998–2024) with Ministerial Terms Highlighted. The blue line represents the infant mortality rate per 1,000 live births, while the red line shows the yearly percentage change in the rate. Gray vertical lines indicate changes in ministerial leadership, with ministers labeled.
Although not much can be inferred from non-causal ecological data, the graph illustrates Ecuador’s infant mortality rate (IMR) from 1998 to 2024, with percentage changes between consecutive years in red. It shows some notable changes. Ministerial changes are marked by vertical dashed lines, with ministers identified by name. There has been a consistent decline in IMR from 31.17 deaths per 1,000 live births in 1998 to 11.345 in 2024, although the rate of decline has slowed in recent years. The most significant decreases occurred between 2000–2005 and 2009–2012. Although the reduction in infant mortality is influenced by many circumstances and determinants typical of a country transitioning from low to middle income, a noticeable slowdown in the decline of the infant mortality rate (IMR) occurred between 2010 and 2020. More recently, (2021–2023) oversaw modest declines in the IMR, despite the challenges posed by the COVID-19 pandemic (Table 2).
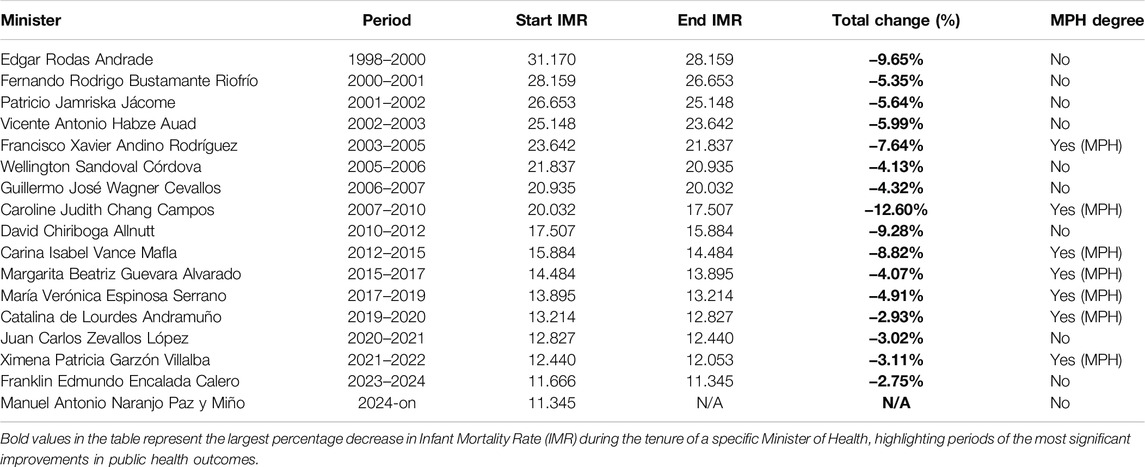
Table 2. Ecuadorian ministers of health (1998–2024), infant mortality rates (IMR), and total percentage change in IMR by ministerial tenure.
In Ecuador, significant milestones in public health were achieved, particularly before the year 2000. Key figures during their tenure led important vaccination campaigns and successfully managed the 1991 cholera outbreak, reducing infant mortality and advancing the Comprehensive Family and Community Health Program [14]. Between 1990 and 2006, the country saw critical reforms, such as the decentralization of health management to municipalities, the formation of Cantonal Health Councils, and the proposal of Universal Health Insurance in 2005–2006 [15]. However, in 2009, these decentralization efforts were reversed with the re-centralization of the health management system [16], undoing much of the progress that had been made.
During 2014, the introduction of new food labeling regulations, which made nutritional information more accessible and positioned Ecuador as a global reference in non-communicable disease prevention was an important contrbution. However, this period was also marked by controversial decisions, including the closure of the National Institute of Hygiene and Tropical Medicine, the elimination of the National Service for the Eradication of Malaria (SNEM), and the shutdown of vaccine production in Ecuador [17]. Despite these public health initiatives, the reduction in infant mortality rates (IMR) during this period was less pronounced compared to other periods. While some improvements were made, the IMR did not decrease as significantly as might have been expected, highlighting a period where public health outcomes did not fully align with the scale of reforms introduced.
The COVID-19 pandemic highlighted Ecuador’s severe shortage of public health expertise, resulting in one of the world’s highest excess death rates. Health ministers, often lacking local experience, communication skills, and disease management knowledge, struggled to provide clear public health messaging. This was worsened by significant mismanagement and corruption, including inflated prices for essential medications and supplies, which deepened the crisis [18, 19].
Corruption has long plagued the health sector, with some ministers facing serious allegations. For example, several scandals have involved the procurement of ambulances and other essential supplies at inflated prices, breaching public procurement laws [20–22].
Ecuador’s health leadership has historically been marked by high ministerial turnover, driven by political interests. This instability, coupled with instances of corruption and controversial policies, has hindered effective public health initiatives and created fragmented health policies. While some achievements exist, persistent leadership issues have led to high malnutrition rates and ineffective campaigns on issues like traffic accidents and drug abuse, contrasting sharply with the successes of neighboring countries like Peru.
Appointing leaders focused solely on clinical medicine without a robust public health background poses several risks:
• Fragmented Policies: Lacking public health foundations can lead to ineffective, fragmented policies [13, 23, 24].
• Curative Bias: Overreliance on treatment instead of prevention perpetuates unsustainable healthcare costs [25].
• Insufficient Emergency Preparedness: COVID-19 underscored the need for leaders skilled in epidemiology and crisis management [26–28].
To better manage Ecuador’s health system, technical skills and public health experience should be prioritized over political considerations in minister selection. Ideal candidates would possess:
• Advanced public health qualifications.
• Proven experience in public health policy formulation and evaluation.
• Active public health research engagement.
• Strong leadership and communication skills to articulate a public health vision and make informed, evidence-based decisions.
Recent ministers have lacked communication competencies, resulting in fewer public health campaigns and diminishing the perception of health ministers as public health advocates.
Selecting health ministers is a nuanced task influenced by social, political, and contextual variables, particularly in developing nations like Ecuador. However, the logic and some of the evidence underscores that this process must be approached thoughtfully, prioritizing technical expertise over political considerations, to ensure sustainable public health progress [29–33]. While the public often expects a Minister of Health to be an effective administrator, adept at managing public procurement and addressing operational challenges, what Ecuador urgently requires is a leader with expertise in prevention, health promotion, and ensuring equitable access to healthcare services.
These competencies are often lacking in physicians focused on curative, private-sector roles. This commentary highlights systemic issues, not as a complaint but as a reflection on persistent shortcomings. For example, despite a 25-year national malnutrition prevention program, Ecuador still has one of the region’s highest malnutrition rates. Even during economic booms, investment favored hospital infrastructure over essential primary healthcare. This manuscript urges Ecuadorian authorities to address these issues and adopt the recommended steps for strengthening national health leadership, shifting towards a comprehensive public health focus for sustainable health improvements.
Author Contributions
Conceptualization: EO-P; methodology: EO-P, JI-C, and JV-G; software: JV-G and IS; validation: EO-P, JI-C, and WC; investigation: JI-C, JV-G, and IS; resources: JI-C, JV-G, and IS; data curation: JI-C; writing–original draft preparation: JV-G and IS; writing–review and editing: JI-C and EO-P; visualization: JI-C and EO-P; supervision: EO-P; project administration: JV-G and EO-P; funding acquisition: EO-P. All authors contributed to the article and approved the submitted version.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of Interest
The authors declare that they do not have any conflicts of interest.
References
1. Ministerio de Salud Publica. Atribuciones y Responsabilidades – Normatización – Ministerio de Salud Pública (2024). Available from: https://www.salud.gob.ec/atribuciones-y-responsabilidades-normatizacion/(Accessed September 14, 2024).
2. Ministerio de Salud Publica. Misión, Visión, Principios y Valores – Ministerio de Salud Pública (2024). Available from: https://www.salud.gob.ec/valores-mision-vision-principios-valores/ (Accessed September 14, 2024).
3. Dimoliatis, ID. A Master of Public Health Must Be the Minimum Prerequisite for a Health Minister: A Timely Proposal to Discuss the Necessary Qualifications of the Ideal Health Minister. J Epidemiol Community Health (2003) 57:755. doi:10.1136/jech.57.9.755
4. Ministerio de Salud Publica. Maestría en Salud Pública – Región Xalapa – Ministerio de Salud Pública. Ministerio de Salud Publica (2024). Available from: https://www.salud.gob.ec/maestria-en-salud-publica-region-xalapa/ (Accessed September 14, 2024).
5. Taché, S. The Master's in Public Health: A Better Preparation for Understanding the Health Care System. West J Med (2001) 175:59. doi:10.1136/ewjm.175.1.59
6. Pearce, N. The Ideal Minister of (Public) Health. J Epidemiol Community Health (2002) 56:888–9. doi:10.1136/jech.56.12.888-a
7. Jeppsson, A, Östergren, P-O, and Hagström, B. Restructuring a Ministry of Health – An Issue of Structure and Process: A Case Study From Uganda. Health Policy Plan (2003) 18:68–73. doi:10.1093/heapol/18.1.68
8. Berman, P, Azhar, A, and Osborn, EJ. Towards Universal Health Coverage: Governance and Organisational Change in Ministries of Health. BMJ Glob Health (2019) 4:e001735. doi:10.1136/bmjgh-2019-001735
9. Sheikh, K, Sriram, V, Rouffy, B, Lane, B, Soucat, A, and Bigdeli, M. Governance Roles and Capacities of Ministries of Health: A Multidimensional Framework. Int J Health Policy Manag (2020) 10:237–43. doi:10.34172/ijhpm.2020.39
10. Edgren, L. The Meaning of Integrated Care: A Systems Approach. Int J Integr Care (2008) 8:e68. doi:10.5334/ijic.293
11. Goniewicz, K, Carlström, E, Hertelendy, AJ, Burkle, FM, Goniewicz, M, Lasota, D, et al. Integrated Healthcare and the Dilemma of Public Health Emergencies. Sustainability (2021) 13:4517. doi:10.3390/su13084517
12. Kaplan, G, Bo-Linn, G, Carayon, P, Pronovost, P, Rouse, W, Reid, P, et al. Bringing a Systems Approach to Health. NAM Perspect (2013) 3. doi:10.31478/201307a
13. Moore, S, Mawji, A, Shiell, A, and Noseworthy, T. Public Health Preparedness: A Systems-Level Approach. J Epidemiol Community Health (2007) 61:282–6. doi:10.1136/jech.2004.030783
14. Organización Panamericana de la Salud. Boletin Epidemiologico - Situacion del Colera en el Ecaudor. OPS (1991) 12:1–24.
15. Goldman, ML. La Descentralización del Sistema de Salud del Ecuador: Un Estudio Comparativo de “Espacio de Decisión” y Capacidad Entre Los Sistemas Municipales de Salud de Quito, Guayaquil y Cuenca. FLACSO Ecuad (2009) 1:1–51.
16. Jiménez Barbosa, WG, Granda Kuffo, ML, Ávila Guzmán, DM, Cruz Díaz, LJ, Flórez Parra, JC, Mejía, LS, et al. Transformaciones del Sistema de Salud Ecuatoriano. Univ Salud (2017) 19:126. doi:10.22267/rus.171901.76
17. Ortiz-Prado, E, Espín, E, Vásconez, J, Rodríguez-Burneo, N, Kyriakidis, NC, and López-Cortés, A. Vaccine Market and Production Capabilities in the Americas. Trop Dis Trav Med Vaccin (2021) 7:11–21. doi:10.1186/s40794-021-00135-5
18. Gonzalez, MA. IESS y Salud, Agobiados por la Corrupción, Comprarán Juntos Sus Medicinas. Primicias (2020). Available from: https://www.primicias.ec/noticias/politica/iess-msp-compraran-juntos-medicamentos/(Accessed September 14, 2024).
19. Ortiz, S. Caso Encuentro Revela la Ruta Opaca Para Comprar Fármacos. Diario Expreso (2024). Available from: https://www.expreso.ec/actualidad/caso-encuentro-revela-ruta-opaca-comprar-farmacos-209136.html (Accessed September 14, 2024).
20. El, D, and Grupo, ESA. Fiscalía de Ecuador Imputa a Ministra de Salud Por Sobreprecio En Ambulancias. El Diario Ecuador (2009). Available from: https://www.eldiario.ec/noticias-manabi-ecuador/137733-fiscalia-de-ecuador-imputa-a-ministra-de-salud-por-sobreprecio-en-ambulancias/ (Accessed September 14, 2024).
21. Poblete, JC. Viteri Compareció Ayer en el Caso Ambulancias. El Comercio (2009). Available from: https://www.elcomercio.com/actualidad/viteri-comparecio-ayer-caso-ambulancias.html (Accessed September 14, 2024).
22. Telégrafo, E. Ex Ministro de Salud Sentenciado a Tres Años de Prisión. El Telégrafo (2013). Available from: https://www.eltelegrafo.com.ec/noticias/informacion/1/ex-ministro-de-salud-sentenciado-a-tres-anos-de-prision (Accessed September 14, 2024).
23. Spicer, N, Agyepong, I, Ottersen, T, Jahn, A, and Ooms, G. It’s Far Too Complicated’: Why Fragmentation Persists in Global Health. Glob Health (2020) 16:60. doi:10.1186/s12992-020-00592-1
24. Stange, KC. The Problem of Fragmentation and the Need for Integrative Solutions. Ann Fam Med (2009) 7:100–3. doi:10.1370/afm.971
25. Cairney, P, St.Denny, E, and Boswell, J. Why Is Health Improvement Policy So Difficult to Secure? Open Res Eur (2022) 2:76. doi:10.12688/openreseurope.14841.2
26. Khatri, RB, Endalamaw, A, Erku, D, Wolka, E, Nigatu, F, Zewdie, A, et al. Preparedness, Impacts, and Responses of Public Health Emergencies Towards Health Security: Qualitative Synthesis of Evidence. Arch Public Health (2023) 81:208. doi:10.1186/s13690-023-01223-y
27. Osti, T, Gris, AV, Corona, VF, Villani, L, D'Ambrosio, F, Lomazzi, M, et al. Public Health Leadership in the COVID-19 Era: How Does It Fit? A Scoping Review. BMJ Lead (2024) 8:174–82. doi:10.1136/leader-2022-000653
28. Goh Chun Chao, G, Anwar, KN, Ahmad, MH, Kunasagran, PD, Binti Mujin, SM, Bujang, Z, et al. Public Health Leadership During COVID-19 Pandemic: A Systemic Review. Malays J Med Health Sci (2023) 19.
29. Ortiz-Prado, E, Fernandez Naranjo, RP, Vasconez, E, Simbaña-Rivera, K, Correa-Sancho, T, Lister, A, et al. Analysis of Excess Mortality Data at Different Altitudes During the COVID-19 Outbreak in Ecuador. High Alt Med Biol (2021) 22:406–16. doi:10.1089/ham.2021.0070
30. Hayes, KT, Heiman, HJ, and Honoré, PA. Developing a Management and Finance Training for Future Public Health Leaders. Front Public Health (2023) 11:1125155. doi:10.3389/fpubh.2023.1125155
31. Kruk, ME, Gage, AD, Arsenault, C, Jordan, K, Leslie, HH, Roder-DeWan, S, et al. High-quality Health Systems in the Sustainable Development Goals Era: Time for a Revolution. Lancet Glob Health (2018) 6:e1196–252. doi:10.1016/S2214-109X(18)30386-3
32. National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Population Health and Public Health Practice; Committee on Community-Based Solutions to Promote Health Equity in the United States The Root Causes of Health Inequity. In: JN Weinstein, A Geller, Y Negussie, and A. Baciu Editors: Communities in Action: Pathways to Health Equity. National Academies Press US (2017). Available from: https://www.ncbi.nlm.nih.gov/books/NBK425845/ (Accessed July 3, 2024).
Keywords: public health leadership, health policy, health system, infant mortality, Ecuador
Citation: Ortiz-Prado E, Suárez Sangucho IA, Cañizares Fuentes WR, Vasconez-Gonzalez J and Izquierdo-Condoy JS (2025) The Imperative of Public Health Expertise in Ecuadorian Health Leadership: A Call for Competency-Based Appointments. Int J Public Health 69:1607894. doi: 10.3389/ijph.2024.1607894
Received: 24 August 2024; Accepted: 20 December 2024;
Published: 07 January 2025.
Edited by:
Lyda Osorio, University of the Valley, ColombiaCopyright © 2025 Ortiz-Prado, Suárez Sangucho, Cañizares Fuentes, Vasconez-Gonzalez and Izquierdo-Condoy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Esteban Ortiz-Prado, ZS5vcnRpenByYWRvQGdtYWlsLmNvbQ==