 Sohela Moussaoui1,2,3*
Sohela Moussaoui1,2,3* Nicolas Vignier2,4,5
Nicolas Vignier2,4,5 Stephanie Guillaume2Florence Jusot2,6Antoine Marsaudon2
Stephanie Guillaume2Florence Jusot2,6Antoine Marsaudon2 Jérôme Wittwer1,2Paul Dourgnon2
Jérôme Wittwer1,2Paul Dourgnon2- 1PHARes Team, National Institute of Health and Medical Research (INSERM) U1219 Bordeaux Population Health Centre Recherche (BPH), Bordeaux University, Bordeaux, France
- 2Institut de Recherche et de Documentation en Économie de la Santé, Paris, France
- 3Department of Family Practice, Sorbonne Université, Paris, France
- 4Hôpitaux Universitaires Paris Seine-Saint-Denis, Bobigny, France
- 5National Institute of Health and Medical Research (INSERM) U1137 Infection, Antimicrobiens, Modélisation, Evolution, Paris, France
- 6Mixed Research Unit (UMR) 8007 Laboratoire d’Economie de Dauphine (LEDA), Paris, France
Objectives: This study aimed to explore the associations between mental health status and experienced pain among undocumented migrants (UMs) in France.
Methods: We used data from the multicentric cross-sectional “Premier Pas” study conducted in the Parisian and Bordeaux regions from February to April 2019. Participants over 18 years of age were recruited from sixty-three sites. Pain was assessed through two variables: overall pain and musculoskeletal pain. Mental health conditions, including anxiety, sleep disorders, depression, and posttraumatic stress disorder (PTSD) were evaluated. Logistic regression models were used to explore associations, controlling for social determinants of health (SDHs).
Results: Our findings revealed significant associations between mental health status and pain among the 1,188 included participants. Sleep disorder was associated to higher odds of musculoskeletal pain (aOR = 2.53, 95% CI [1.20–5.33], p = 0.014). Stratified results indicated that among women, depression was associated to higher odds of pain (aOR = 4.85, 95% CI [1.53–13.36], p = 0.007).
Conclusion: This large study confirms the connection between mental health status and pain among UMs, providing valuable evidence for clinicians to address mental health issues in this population.
Introduction
The term undocumented migrants (UMs) refers to individuals without formal residence recognition, resulting in an irregular migration status [1]. Some UMs may have held temporary permits that have expired, whereas others enter a country without permission or are denied asylum. The exact number of UMs in Europe and France is uncertain, with varying estimates. In France, UMs are prohibited from legal employment, often resorting to informal jobs that lack essential protections and rights [2].
Migrants and individuals in ethnic minority groups experience health disadvantages due to intersecting factors such as racial identity and socioeconomic status, particularly vulnerable groups such as women and sex workers [3].
Research on health disparities between UMs and regular residents (including documented migrants) in Europe is limited. However, evidence shows that UMs face numerous health challenges [4]. Compared with the majority population, UMs report poorer self-perceived health and are at increased risk for mortality from non-communicable diseases, such as cardiovascular issues and cancers [1, 4–9]. High rates of maternal mortality and adverse birth outcomes, including preterm birth and low birth weight, have also been noted among UMs [1, 10]. Furthermore, undocumented women often have limited access to contraception and family planning services, resulting in higher rates of unintended pregnancies and poorer maternal and child health outcomes [1, 11].
Mental health is another critical area, as UMs are more likely to have risk factors for conditions such as depression, anxiety, and posttraumatic stress disorder (PTSD) than both the general population and documented migrants are [1, 4, 12, 13].
In France, UM faces a greater burden of HIV and other infectious diseases, including significant rates of dental infections and chronic hepatitis B [14]. Healthcare for UMs is a polarizing issue in France [15]. The Aide Médicale d’Etat (AME, State Medical Aid) provides means-tested healthcare access, with residence in the country for more than 3 months and low income required for eligibility [16]. Nearly half of eligible individuals do not apply for this program, resulting in limited access [17–20]. AME holders often face discrimination, leading to unmet health needs [21]. Barriers to care increase the likelihood of delayed diagnoses, and while some non-governmental organizations (NGOs) offer support, their capacity for follow-up and preventive care is limited [19, 21–26].
Chronic pain, particularly musculoskeletal pain, contributes significantly to mental illness [27]. A positive association between pain and mental health has been described, although the causal pathway remains unclear [28–31]. Bidirectional relationships exist, with similar risks for developing mental illness due to pain and vice versa [32]. Both pain and mental illness share biological mechanisms and brain regions [33, 34]. Behavioral factors can also explain this relationship. For example, the fear–avoidance model suggests that negative thought patterns can lead to fear of movement, perpetuating a cycle of pain, disability, and depression [35]. The relationship between pain and mental health seems to vary according to gender, with the effect being stronger among females [36, 37].
In the general population, social determinants of health (SDHs), such as income or employment status, have been identified as key factors associated with pain [38]. For example, associations between food insecurity and site-specific pain, such as musculoskeletal pain, have been described in the general population [39–41]. Socioeconomically deprived individuals are more likely to experience chronic pain, more severe pain, and a greater degree of pain-related disability [40, 42].
In immigrant populations, associations between mental health and SDHs have been described [2, 43–46]. Poor working conditions are linked to adverse health outcomes and pain in immigrants [2, 43, 47–49].
For UMs in Europe, few studies have provided evidence on the associations between SDHs and mental health [4, 13, 50]. Some studies indicate that postmigration housing insecurity is associated with worse mental health in adult UMs [51, 52]. Food insecurity and a longer duration of residence in the host country are also linked to poorer mental health among UMs in the United States (U.S.) [53]. Additionally, the type of work contract may influence health outcomes for UM workers [54]. Conversely, social support and community engagement are protective factors for the mental health of UMs in Europe [51, 52, 55]. Gaining documented status has positive effects on the mental health of UMs in Switzerland [50, 56].
The literature describes associations between mental health and pain in various immigrant groups, with stronger links to conditions such as depression, PTSD or anxiety in immigrant populations than in the general population [46]. Among UMs in the U.S., associations between pain and psychological distress, such as anxiety and depression, have been described [57]. In France, however, data on UMs remain limited, and the relationship between pain and mental health in this group has not been studied.
Immigrant populations face migration-related stressors, such as physical and verbal violence, which worsen the effects of displacement, including limited resource availability and exclusion from citizenship-oriented health policies [58, 59]. The literature describes a high prevalence of depression, anxiety, stress, sleep disorders, and PTSD among immigrants during and after migration [60, 61]. PTSD and depression are particularly prevalent among UMs compared with the general population and are influenced by low socioeconomic status and integration policies [51, 62].
UMs experiencing social isolation, abuse, or financial instability are at increased risk of mental health issues such as anxiety, depression or sleep disorders [50, 52, 58, 63, 64]. Access to psychosocial healthcare is often hindered by a lack of insurance, taboos about mental health, and distrust in practitioners’ abilities to treat mental health conditions [55, 58, 63]. Since UMs may not spontaneously report mental health difficulties, healthcare professionals need to actively inquire about the needs of these individuals [12].
Pain is a frequent reason for consultation, which initiates first contact with the healthcare system in the host country [65, 66]. The literature suggests that pain is often experienced by UMs, with musculoskeletal pain being the most frequently reported type in healthcare settings [58, 67].
UMs often earn an income through manual and physically demanding occupations that can induce, maintain or increase musculoskeletal pain [2, 3, 68].
Among UMs, mental health and pain are often associated with SDHs. It is therefore worth investigating whether the relationship between pain and mental health persists once SDHs are controlled for. We hypothesized that this relationship would persist after controlling for SDHs. Our main objective was to explore whether the association between mental health and pain remained among UMs in France after adjusting for SDHs.
Methods
Study Design and Participants
Premier Pas was a multicentric cross-sectional study carried out in the Parisian and Bordeaux regions of France between February and April 2019. This study, which was based on multidisciplinary approaches, sought to better understand the experiences of UMs living in France and to assess their health status and access to rights and healthcare. The inclusion criteria consisted of being undocumented and over 18 years old. The questionnaire was translated into fourteen different languages to interact with participants: French, English, Spanish, Russian, Albanian, Portuguese, Arabic, Dari, Chinese, Tamil, Pashto, Bengali, Pulaar, and Bambara [17–19]. Individuals were recruited from 63 sites that provide support or assistance for individuals experiencing social deprivation and immigrants [19]. The structures included “Espace Solidarité Insertion,” which offers daytime shelter, social and health services for homeless people, various NGOs, and Hospital Health Access Sites (“Permanence d’Accès aux Soins de Santé”). The latter provide social assistance and healthcare to vulnerable populations, but their geographic scope is limited to certain cities. Additionally, another type of structure included was local health insurance centers (“Caisses Primaires d’Assurance Maladie”), which operate at a departmental level and deliver various social subsidies and indemnities for registered beneficiaries for claims ranging from sickness, pregnancy, disability or death. Point of Access to Rights (“Point d’accès aux droits”), which are free and permanent reception sites, provide information and resources for legal or administrative problems and were also included as recruitment sites. Finally, three more recruitment sites were included: public baths, free health centers of Doctors of the World (“CASO”) and maternal and child protection centers (“Protection Maternelle et Infantile”), which is a departmental service that is responsible for protecting the health of mothers and newborns.
Data Collection
Dependent Variables
Data on pain experienced at the time of the study were collected, and the pain experienced included abdominal, musculoskeletal, headache/migraine, and chest or pelvic pain. A binary variable, “all pain,” was created (musculoskeletal or abdominal, or headache/migraine or chest or pelvic pain) from the variables related to the different types of pain. As we were more interested in the experience of pain than its mechanism or cause, this grouping seemed justified and, at the same time, enabled us to increase the power of our analyses.
Owing to the sample size, the comparative analyses were performed only on musculoskeletal pain and on the variable “all pain.”
Independent Variables
Mental health was assessed through several questions. The participants were asked if they were currently experiencing various conditions, including mental health conditions. If a participant answered “yes” for a mental health condition, then follow-up questions were asked to clarify whether they were experiencing a sleep disorder or anxiety. For depression, we used the Patient Health Questionnaire-9 (PHQ-9) and a cutoff score of 10 or more to estimate moderate to severe depression [69]. PTSD was assessed with the Primary Care PTSD Screen for DSM-5 (PC-PTSD-5) [70]. A score of three or above was used as the threshold for diagnosing PTSD. Depression and PTSD were assessed with the PHQ-9 and the PC-PTSD-5, respectively, for all participants regardless of their answers to the general question.
Our literature review, described in the introduction, helped identify confounders related to pain and mental health. We categorized these determinants into coherent groups according to the following: demographic characteristics (age and gender), migration characteristics (region of origin, time since arrival in France, motives for migration), social characteristics (current job, job in the country of origin, fluency in French), the family environment (isolation), material living conditions (housing type, food insecurity) and access to care (“Aide Médicale de l’Etat”, AME”). The latter is a specific means-tested publicly funded health insurance for UMs that covers medical expenses at 100% of real costs with some excluded treatments [71].
Data Analysis
In the first stage, we described the prevalence of different types of pain using percentages and then compared the categories of pain according to different mental health conditions via a chi-square test. The data were weighted on the basis of the probability of inclusion.
In the second step, we performed univariate analyses via logistic regression for musculoskeletal pain and the variable “all pain,” with pain as the dependent variable and mental health as the main independent variable. When an association was significant in the univariate analysis, we performed multivariate analyses. A difference was considered significant when the p-value of the crude odds ratio (OR) for the univariate result was <0.200.
To address collinearity and avoid overadjustment in the multivariate analyses, we used a hierarchical regression method. Blockwise selection was used, with pain as the dependent variable and mental health as the independent variable, and the different categories were added step by step. In this six-step process, we added each group of variables sequentially, monitoring how the coefficients changed to ensure that the models remained robust. To avoid weighing down the models and reducing their performance, we added only the variables with a p-value of the crude OR of less than 0.200 to the model. Alternatively, within a group of variables for which all the crude ORs were greater than or equal to 0.200, we selected the variable with the smallest p-value.
For power purposes, the age categories “18–29 years” and “30–39 years” were grouped together into the category “18–39 years” in some analyses when there were small numbers in one category.
In the final step, analyses were performed to stratify by gender, as the literature has shown that associations between pain and mental health are influenced by gender [36, 37].
The threshold of significance was 0.05 and 95% confidence intervals were used. All analyses were performed with Stata software.
Results
A total of 1,223 participants were included in the Premier Pas study, and 1,188 answered questions related to current health conditions. Overall, 28.8% of the participants were women, and the mean age was 37.1 years (95% confidence interval (CI) [36.5–37.7]). In terms of geographic origin, 62.5% of the participants were from sub-Saharan Africa, and 23.7% were from North Africa. Approximately half of the individuals in the sample were registered beneficiaries of the AME at the time of the study. A total of 37.8% of the participants had arrived less than 1 year before the time of the survey, and 33.9% had lived in France for at least 3 years. More than half of the participants were fluent in French (56.4%). Regarding material living conditions, 42.5% of the participants had precarious housing, and 30.7% reported often facing food insecurity. Table 1 displays all the characteristics of the population.
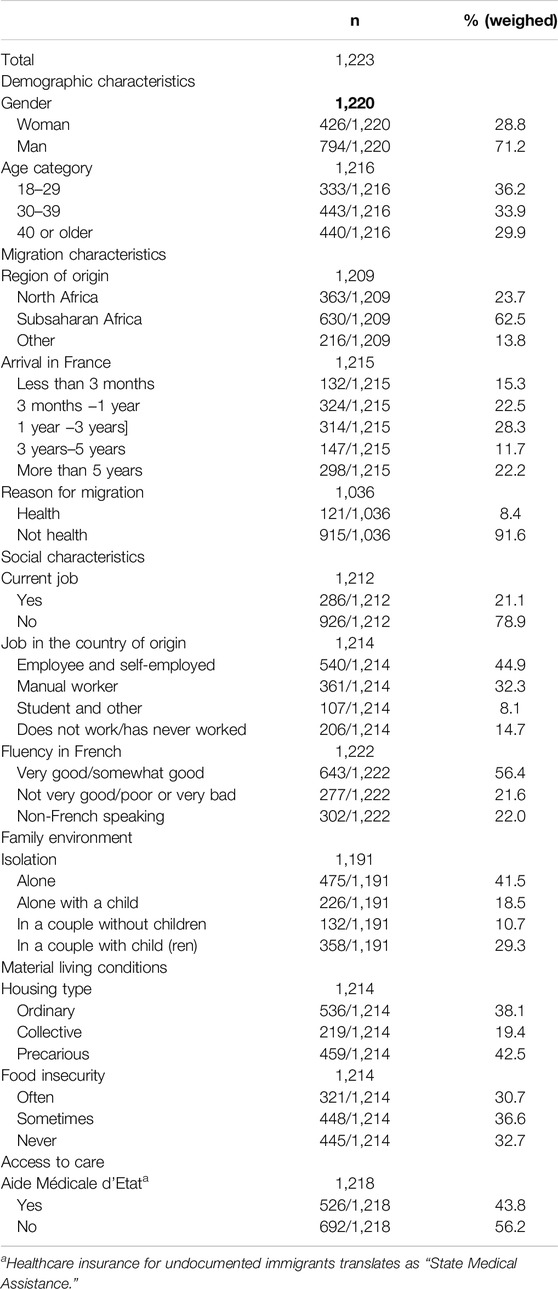
Table 1. Description of the population (Premiers Pas, France, 2019).
A total of 14.3% of the participants reported experiencing pain (n = 176) regardless of the type, 8.3% (n = 103) reported experiencing musculoskeletal pain, 3.5% (n = 48) reported experiencing abdominal pain, 2.7% (n = 37) reported experiencing headache, 1.2% reported experiencing pelvic pain (n = 25) and 1.8% reported experiencing chest pain (n = 12).
No differences were found between women and men except in pelvic pain, for which the rate was greater among women (Figure 1).
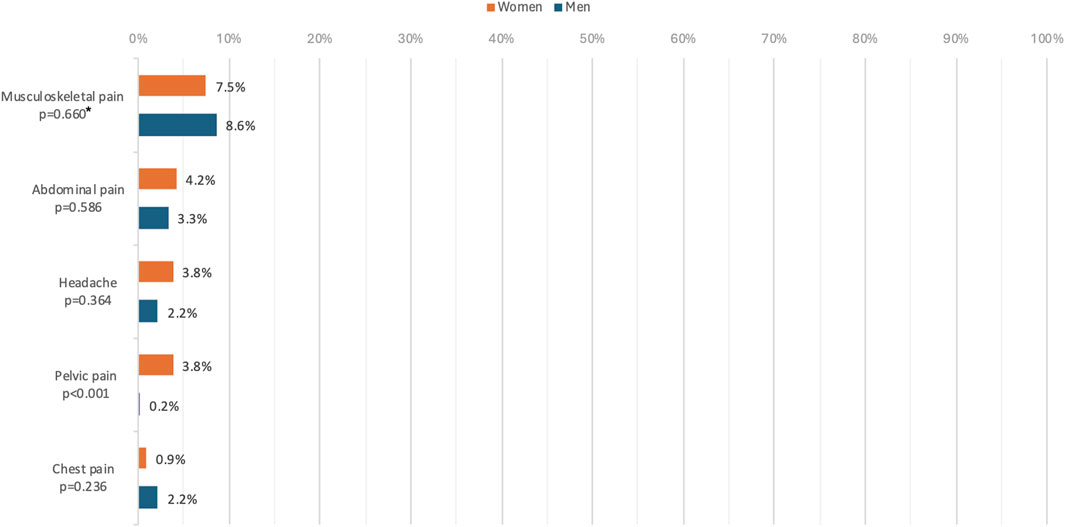
Figure 1. Rates of the different types of pain by gender (Premiers Pas, France, 2019). N = 1118, p*: p-value of the chi-2 test.
In terms of mental health, 11.5% of the participants reported having anxiety (n = 131), 15% reported having sleep disorders (n = 176), 29.5% had moderate to severe depression (n = 384, PHQ-9 score), and 16.2% had PTSD (n = 210, PC-PTSD-5 score).
In terms of gender, no differences were found between women and men. The proportions are reported for the following conditions: anxiety (10.6% n = 50/418 and 11.4%, n = 78/767), sleep disorders (14.5%, n = 72/418 and 15.0%, n = 102/767), depression (32.9%, n = 164/367 and 27.9%, n = 219/663) and PTSD (18.7%, n = 85/409 and 15.0%, n = 123/764).
Pain and Mental Health
Table 2 presents crude and adjusted associations between pain (all pain and musculoskeletal pain) and mental health. Individuals who were depressed, those with sleep disorder and those with anxiety were more likely to report pain. Individuals with PTSD had significantly higher likelihood of overall pain, at bivariate level and not in multivariate one. No difference was observed between musculoskeletal pain and PTSD.
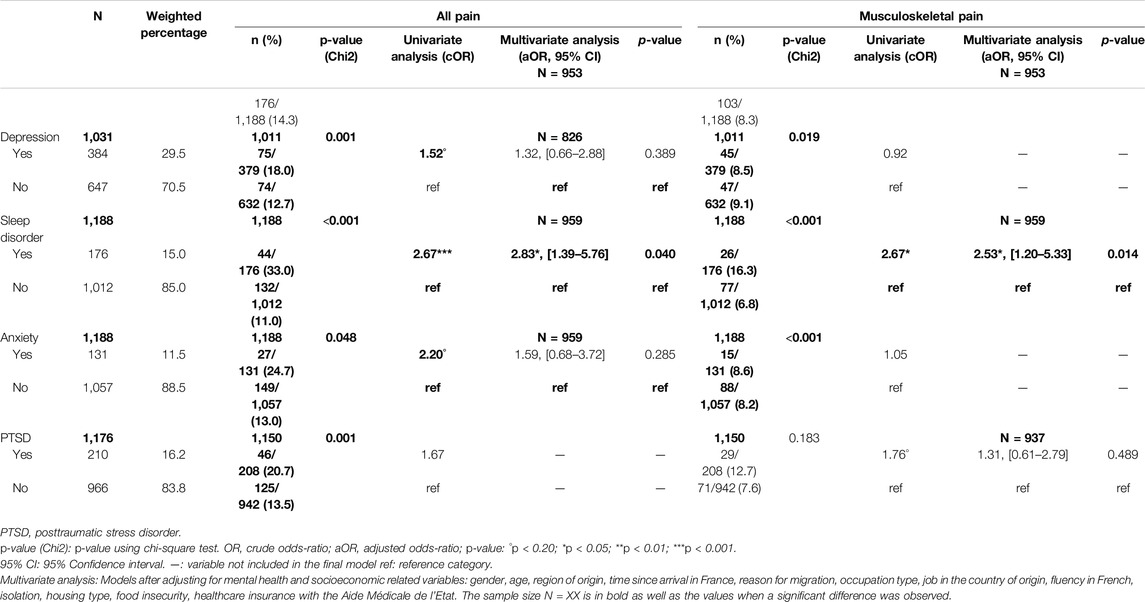
Table 2. Prevalence, univariate and multivariate analyses for pain and mental health-related variables, Premiers Pas, France, 2019.
Multivariate analyses were performed when the univariate association was significant. The multivariate analyses controlling for socioeconomic indicators revealed that sleep disorder was associated with higher odds of overall pain (adjusted odds ratio (aOR) = 2.83, 95% CI [1.39–5.76], p = 0.040). Sleep disorder was also associated with higher odds of musculoskeletal pain (aOR = 2.53, 95% CI [1.20–5.33], p = 0.014).
Stratified Analyses by Gender
As shown in Table 3, among women, those with depression had significantly higher odds of overall pain after controlling for socioeconomic variables (aOR = 4.85, 95% CI [1.53–13.36], p = 0.007). No associations were found between mental health and musculoskeletal pain among women.
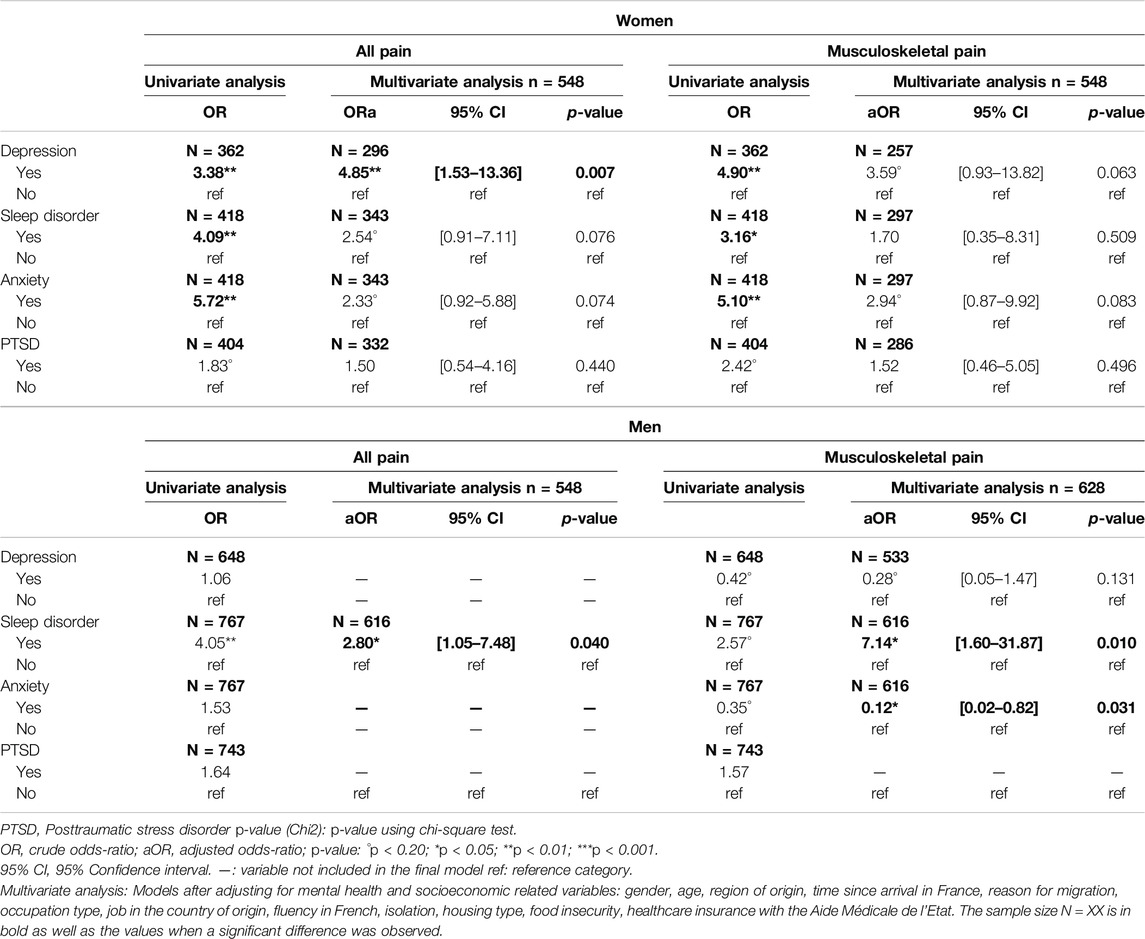
Table 3. Univariate and multivariate analyses for musculoskeletal pain, abdominal pain and headache with mental health-related variables, stratified by gender (Premiers Pas, France, 2019).
Among men, those with sleep disorder had significantly higher odds of overall pain after controlling for socioeconomic variables (aOR = 2.80 95% CI [1.05–7.48], p = 0.040). Sleep disorder (aOR = 7.14, 95% CI [1.60–31.87], p = 0.010) and anxiety (aOR = 0.12, 95% CI [0.02–0.82], p = 0.031) were associated with musculoskeletal pain.
Discussion
Main Results
Overall, clear associations between several mental health conditions and pain were revealed after controlling for SDHs. These results are consistent with the international literature [62, 72]. Similar to our study, a Swedish study revealed that a higher risk of chronic and severe pain among immigrants was significantly influenced by depression [73]. In another cohort study of Syrian refugees in Norway 12 months after their arrival in Northern Europe, poor mental health was a predictor of chronic pain at follow-up [72]. Finally, studies also support that trauma and pain, especially joint pain, are connected [74].
The rationale for including the “all pain” variable was that our study addressed the experience of pain and its relationship with mental health. The experience of pain, rather than its mechanism or cause, was the focus of this work, and this grouping made sense to us. Moreover, the inclusion of this variable increased the power of our analyses. This grouping and the results are also coherent from the perspective of screening UMs who visit clinics for pain. When UMs visit a clinic because they are experiencing pain, they should be screened for mental health problems, as they are more at risk.
Gender Stratification
We stratified the data by gender to verify whether the relationship between mental health and pain varied according to gender on the basis of the literature [36, 37]. Our results confirmed this hypothesis, as some associations remained only for women or men. Depression was associated with higher odds of overall pain among women, and sleep disorder was associated with higher odds of overall pain and musculoskeletal pain among men. The associations found in our study were in line with those described in the literature in the general population [36, 37, 75].
Surprisingly, after controlling for socioeconomic indicators, a negative association appeared for men. Anxiety was associated with lower odds of musculoskeletal pain among men. The association usually reported in the literature is that anxiety is a risk factor for musculoskeletal pain [76]. Nevertheless, among veterans, it appears that when anxiety is associated with PTSD, pain perceptions can be reduced [74]. In our study, no association between anxiety and PTSD was found, possibly because of a lack of power. Some associations, such as that between sleep disorder and musculoskeletal pain, among women have been described in the literature but were not found in our population [36, 77].
In addition to musculoskeletal pain and headaches, men had lower rates of reported pain than women did. One reason for this result could be the variation in pain verbalization depending on gender. Pain may be less easily expressed by men not because of biological differences but because of gender performativity [78]. Moreover, the verbalization of anxiety also appears to be gender biased. Male participants appear to be less inclined to express their anxiety but would be more comfortable doing so in certain contexts, such as in online forums or to women in their close circle (to their spouse, mother, etc.) [79].
Social Determinants of Health
In our study, the multivariate models were adjusted for SDHs. The role of SDHs in pain has been described, and migration seems to play a role [39, 58, 80, 81]. However, how migration affects the association between pain and mental health is unclear. The allostatic load theory explains how migration-related exposures play a role in the accumulation of somatic damage and increase the risk of several diseases [82, 83]. Migration-related stressors such as poor safety, a poor physical environment or poor access to healthcare are associated with chronic pain among immigrants [72].
Mutual Maintenance
Our results highlight the importance of identifying when pain is experienced by UMs not only because of its prevalence but also because it can be associated with mental health conditions. Our study was observational, so a causal pathway cannot be established between pain and mental health. However, it seems that they can both maintain each other mutually. The “mutual maintenance theory” suggests that chronic pain may exacerbate and maintain PTSD, whereas PTSD may exacerbate and maintain chronic pain [84]. This mutual maintenance occurs through specific mechanisms, such as reminders of trauma, depression and reduced activity levels. This relationship seems to extend further and has an impact on treatment for both mental health conditions and pain. Physical pain may interfere with a patient’s ability to respond to treatment, and the presence of a mental health condition could also interfere with effective pain management [74].
Perspectives
The pain expressed by the participants was self-assessed, and the causes of pain were not explored. Several underlying hypotheses may explain the cause of pain. The pain experienced could be linked to an unperceived or undiagnosed health problem, and reduced access to healthcare may increase the risk of delayed diagnosis or even non-diagnosis of the cause of pain [26]. In cases where pain can be explained by a physical or organic cause, whether a mental health problem exists must still be investigated, as it may accompany or even maintain the pain [84]. There are situations where pain cannot be medically explained and may either be part of a psychiatric syndrome or remain medically unexplained [85]. Regardless of the cause of the pain, its treatment can be challenging. Few studies have evaluated the impact of pain treatment on reported pain and mental health among immigrants [86, 87]. A study conducted in Norway among refugees from Syria aimed to assess two different interventions to reduce pain and posttraumatic symptoms: the “Physiotherapy Activity a pain Awareness Intervention” (PAAI), which consists of a combination of psychomotor and general physiotherapy, and the “Teaching Recovery Technique” (TRT), which involves cognitive behavioral therapy [86]. The PAAI had no effect on either chronic pain or mental health symptoms after 8 and 12 weeks. One reason that the authors proposed was that the intervention was not sufficiently adapted for the participants and their situations. A large proportion of participants in the intervention group could not attend the sessions. The qualitative analyses revealed that it was difficult to combine the sessions with other activities of daily life, thereby potentially contributing to additional stress [88]. The TRT significantly improved general mental health but did not help reduce chronic pain [89].
Strengths
The key strength of this study lies in its recruitment of a diverse population and its focus on mental health issues within this vulnerable group. Moreover, to our knowledge, our study is the first to focus on UMs not exclusively recruited in healthcare settings in France. Very little is known in terms of the public health of this population. Thus, this study is highly important, as it provides insights into this hard-to-reach and hard-to-study population. One of the factors that enabled recruitment was the use of diverse languages and the inclusion of numerous sites outside care settings. Even though the sample size was not large, the results of this study are still substantial if we consider that this population is difficult to approach, especially outside healthcare settings. The results presented in this article are the first to document the relationship between pain and mental health in this population.
Limitations
Unfortunately, the lack of power did not allow us to further explore the implications of PTSD and depression on the different types of reported pain. Additionally, the small sample size of women did not allow us to explore associations between mental health and musculoskeletal pain. For some results, such as the association between sleep disorder and musculoskeletal pain, the CIs were large. Thus, even if the value was significant, the uncertainty was high, and the estimate was less precise because of the size of the 95% CI. A larger sample size might have reduced this uncertainty.
Furthermore, our study does not represent all UMs across France because recruitment took place in two regions. However, our results are representative, as UMs are geographically concentrated in urban regions, particularly in the Parisian region [90]. Future research with larger samples should thoroughly investigate immigration-related factors, including a wide range of sociodemographic and health-related factors that may contribute to health status among immigrants.
Pain could have been studied in more detail, for example, by examining the intensity of the pain or by asking how the pain affected the participants’ lives. Self-assessment of subjective health, such as pain, is influenced by culture, as expectations and norms for a given health dimension can be very heterogeneous [91]. As a result, the subjective self-assessment of pain in this study did not allow us to compare subjective health states between individuals, especially to compare samples from different countries or regions. This can lead to serious misunderstandings about the health status of populations, particularly those that are the most economically disadvantaged. This bias, known as the “DIF” (Differential Item Functioning) effect, can be corrected via more advanced methods, such as “Anchoring Vignettes,” which can be used to detect and correct possible comparability problems. This method was not used in our study, as the study design was not initially intended to study pain in depth. Future studies could be carried out using this type of method to better study pain.
The PHQ-9 and PC-PTD-5 were used in different languages. In this study, interviews were conducted in French (75%), Arabic (8%), English (7%), Spanish (4%), Russian (2%), and Portuguese (2%), accounting for 99% of the questionnaires collected [19]. Although the PHQ-9 has been validated in these languages, this was not the case for the PC-PTSD-5 [92–96]. The PHQ-9 has been validated in French, Arabic, English, Spanish, Russian and Portuguese. The PC-PTSD-5 has only been validated in English but not in French or other languages [70]. For those languages, no suitable and validated scale to measure PTSD symptoms was found in the literature. Thus, PTSD symptoms may have been over- or underestimated in our study, leading to measurement bias for this indicator.
Since our study did not aim to establish causality, the lack of specific time frames does not undermine the relevance of our findings. Moreover, recall bias would have been a challenge. The PHQ-9 and PC-PTSD-5 were administered to all individuals, and anxiety and sleep disorders can rarely be ignored, as these symptoms often have a major impact on quality of life. Thus, the risk of over- or underestimating the prevalence of mental health conditions in our study was reduced. Moreover, since our study was essentially conducted outside care settings, the risk of overestimating mental health conditions if the participants were seeking health services also remained low.
Conclusion
Our study confirms the link between mental health and perceived pain in this large sample of UMs in France. These results could have a direct impact on the care provided to UMs. This study encourages practitioners to systematically ask questions pertaining to mental health when a patient is experiencing pain to implement targeted interventions, especially when the pain remains medically unexplained. The results call for more specific studies on the associations between certain types of pain and certain mental disorders and the development of treatment algorithms that consider the social and psychological context of UMs.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors upon request.
Ethics Statement
This study involving human participants was reviewed and approved by the Institute for Research and Documentation in Health Economics. Informed consent for participation was obtained from each participant in accordance with the national legislation and the institutional requirements. The study was conducted under the control of the CNIL (Commission Nationale de l’Informatique et des Libertés, registration number: 2203002 v 0).
Author Contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. The Premiers Pas study was funded by the National Research Agency (Agence nationale de la Recherche, AnR) in 2016 (grant number ANR-16-CE36-0008).
Conflict of Interest
The authors declare that they do not have any conflicts of interest.
Acknowledgments
The authors thank all the participants who took the time to answer the survey. We would also like to thank the National Research Agency that financed this study.
References
1. PICUM. Migration Status: A Key Structural Social Determinant of Health Inequalities for Undocumented migrants Brussels, Belgium (2023). Available from: https://picum.org/wp-content/uploads/2023/12/Migration-status_A-key-structural-social-determinant-of-health-inequalities-for-undocumented-migrants_EN.pdf (Accessed October 12, 2024).
2. Hargreaves, S, Rustage, K, Nellums, LB, McAlpine, A, Pocock, N, Devakumar, D, et al. Occupational Health Outcomes Among International Migrant Workers: A Systematic Review and Meta-Analysis. Lancet Glob Health (2019) 7(7):e872–82. doi:10.1016/S2214-109X(19)30204-9
3. Michele, LV, Nele, V, and Johan, W. Undocumented Migrant Workers. Belgium (2004). Available from: https://picum.org/wp-content/uploads/2021/11/Undocumented-Migrant-Workers-in-Europe.pdf (Accessed February 16, 2024).
4. de Vito, E, de Waure, C, Specchia, M, and Ricciardi, W. Public Health Aspects of Migrant Health: A Review of the Evidence on Health Status for Undocumented Migrants in the European Region. Copenhagen (2015).
5. Wahlberg, A, Källestål, C, Lundgren, A, and Essén, B. Causes of Death Among Undocumented Migrants in Sweden, 1997–2010. Glob Health Action (2014) 7(1):24464. doi:10.3402/gha.v7.24464
6. Piccoli, L, and Wanner, P. The Political Determinants of the Health of Undocumented Immigrants: A Comparative Analysis of Mortality Patterns in Switzerland. BMC Public Health (2022) 22(1):804. doi:10.1186/s12889-022-13188-8
7. Lafaut, D, Vandenheede, H, Surkyn, J, and Coene, G. Counting the Non-Existing: Causes of Death of Undocumented Migrants in Brussels-Capital Region (Belgium), 2005–2010. Arch Public Health (2019) 77(1):42. doi:10.1186/s13690-019-0369-6
8. Fiorini, G, Cerri, C, Bini, S, Rigamonti, AE, Perlini, S, Marazzi, N, et al. The Burden of Chronic Noncommunicable Diseases in Undocumented Migrants: A 1-Year Survey of Drugs Dispensation by a Non–Governmental Organization in Italy. Public Health (2016) 141:26–31. doi:10.1016/j.puhe.2016.08.009
9. Gray, B, and van Ginneken, E. Health Care for Undocumented Migrants: European Approaches. Issues Int Health PolicyThe Commonw Fund (2012) 33:1–12.
10. Gieles, NC, Tankink, JB, van Midde, M, Düker, J, van der Lans, P, Wessels, CM, et al. Maternal and Perinatal Outcomes of Asylum Seekers and Undocumented Migrants in Europe: A Systematic Review. Eur J Public Health (2019) 29(4):714–23. doi:10.1093/eurpub/ckz042
11. de Jong, L, Pavlova, M, Winters, M, and Rechel, B. A Systematic Literature Review on the Use and Outcomes of Maternal and Child Healthcare Services by Undocumented Migrants in Europe. Eur J Public Health (2017) 27(6):990–7. doi:10.1093/eurpub/ckx181
12. Schoevers, MA, van den Muijsenbergh, METC, and Lagro-Janssen, ALM. Self-Rated Health and Health Problems of Undocumented Immigrant Women in the Netherlands: A Descriptive Study. J Public Health Pol (2009) 30(4):409–22. doi:10.1057/jphp.2009.32
13. Martin, F, and Sashidharan, SP. The Mental Health of Adult Irregular Migrants to Europe: A Systematic Review. J Immigr Minor Health (2023) 25(2):427–35. doi:10.1007/s10903-022-01379-9
14. Vignier, N, Moussaoui, S, Marsaudon, A, Wittwer, J, Jusot, F, and Dourgnon, P. Burden of Infectious Diseases Among Undocumented Migrants in France: Results of the Premiers Pas Survey. Front Public Health (2022) 10:934050. doi:10.3389/fpubh.2022.934050
15. Cailhol, J, Vignier, N, Vandentorren, S, Moussaoui, S, and Feral-Pierssens, AL. French Political Bargaining Over Undocumented Migrants’ Health. Lancet (2023) 403:140–1. doi:10.1016/s0140-6736(23)02718-6
16. Code de l’Action Sociale et des Familles: Articles L251-1 à L251-3. Chapitre Ier: Droit à l’Aide Médicale de l’Etat (2019). Available from: https://www.legifrance.gouv.fr/codes/id/LEGISCTA000006157607 (Accessed March 21, 2023).
17. Wittwer, J, Raynaud, D, and Jusot, F. Protéger la Santé des Personnes Étrangères en Situation Irrégulière en France L’Aide Médicale de l’État, une Politique d’Accès aux Soins mal Connue. Paris, France: Questions de l’Economie de la Santé, 243 (2019).
18. Jusot, F, Dourgnon, P, Wittwer, J, and Sarhiri, J. Access to State Medical Aid by Undocumented Immigrants in France: First Findings of the “Premiers Pas” Survey. Paris, France: Questions de l’Economie de la Santé 245 (2019).
19. Dourgnon, P, Guillaume, S, Jusot, F, and Wittwer, J. A Study of Undocumented Immigrants’ Access to Health Coverage and Care in France: The “Premiers Pas” Survey. Paris, France: Questions d’Économie de la santé, 244 (2019).
20. Doctors of the World. Observatoire de l’Accès aux Droits et aux Soins dans les Programmes de Médecins du Monde en France - Rapport 2019 (2020). Available from: https://www.medecinsdumonde.org/app/uploads/2022/04/MDM-RAPPORT-OBS2020.pdf (Accessed March 21, 2023).
21. Défenseur des droits. Études and Résultats - Les Refus de soins Discriminatoires: Tests dans Trois Spécialités Médicales (2019). Available from: https://www.defenseurdesdroits.fr/sites/default/files/atoms/files/etres-refussoins-num-21.10.19.pdf (Accessed March 21, 2023).1–17.
22. Défenseur des Droits. Les Refus de Soins Opposés aux Bénéficiaires de la CMU-C, l’ACS et l’AME. Les refus de Soins Opposés aux Bénéficiaires de la CMU-C, l’ACS et l’AME. Rapport Remis au Premier Ministre Mars. (2014), 1–47. Available from: https://www.defenseurdesdroits.fr/sites/default/files/atoms/files/ddd_r_20140301_refus_soins.pdf (Accessed March 21, 2023).
23. Vignier, N, Spira, RD, Bouchaud, O, du Loû, AD, and Chauvin, P. Refusal to Provide Health Care to Sub-Saharan African Migrants in France. Lancet Public Health (2018) 3(1):e12. doi:10.1016/S2468-2667(17)30246-3
24. Garance, P, Stéphanie, V, Pierre, C, Vignier, 1 N, and Cécile, V. Refusal to Provide Healthcare Because of CMU and AME Reported by Homeless Women Living With Their Family Housed in Île-de-France. Bull Epidémiologique Hebdomadaire (2019) 341–50. Available from: http://beh.santepubliquefrance.fr/beh/2019/17-18/2019_17-18_4.html (Accessed March 21, 2023).
25. Vignier, N, Desgrées du Loû, A, Pannetier, J, Ravalihasy, A, Gosselin, A, Lert, F, et al. Access to Health Insurance Coverage Among Sub-Saharan African Migrants Living in France: Results of the ANRS-PARCOURS Study. PLoS One (2018) 13(2):e0192916. doi:10.1371/journal.pone.0192916
26. Dourgnon, P, Jusot, F, Marsaudon, A, Sarhiri, J, and Wittwer, J. Just a Question of Time? Explaining Non-Take-Up of a Public Health Insurance Program Designed for Undocumented Immigrants Living in France. Health Econ Pol L (2023) 18(1):32–48. doi:10.1017/S1744133122000159
27. Vigo, D, Thornicroft, G, and Atun, R. Estimating the True Global Burden of Mental Illness. Lancet Psychiatry (2016) 3(2):171–8. doi:10.1016/S2215-0366(15)00505-2
28. Thomtén, J, Soares, JJF, and Sundin, Ö. Pain Among Women: Associations With Socio-Economic Factors Over Time and the Mediating Role of Depressive Symptoms. Scand J Pain (2012) 3(2):62–7. doi:10.1016/j.sjpain.2011.12.003
29. Swanson, SA, Zeng, Y, Weeks, M, and Colman, I. The Contribution of Stress to the Comorbidity of Migraine and Major Depression: Results From a Prospective Cohort Study. BMJ Open (2013) 3(3):e002057. doi:10.1136/bmjopen-2012-002057
30. Martin, MS, Maddocks, E, Chen, Y, Gilman, SE, and Colman, I. Food Insecurity and Mental Illness: Disproportionate Impacts in the Context of Perceived Stress and Social Isolation. Public Health (2016) 132:86–91. doi:10.1016/j.puhe.2015.11.014
31. Gureje, O, Von Korff, M, Kola, L, Demyttenaere, K, He, Y, Posada-Villa, J, et al. The Relation Between Multiple Pains and Mental Disorders: Results From the World Mental Health Surveys. Pain (2008) 135(1):82–91. doi:10.1016/j.pain.2007.05.005
32. Bondesson, E, Larrosa Pardo, F, Stigmar, K, Ringqvist, Å, Petersson, IF, Jöud, A, et al. Comorbidity Between Pain and Mental Illness – Evidence of a Bidirectional Relationship. Eur J Pain (2018) 22(7):1304–11. doi:10.1002/ejp.1218
33. Hooten, WM. Chronic Pain and Mental Health Disorders. Mayo Clin Proc (2016) 91(7):955–70. doi:10.1016/j.mayocp.2016.04.029
34. Vadivelu, N, Kai, AM, Kodumudi, G, Babayan, K, Fontes, M, and Burg, MM. Pain and Psychology-A Reciprocal Relationship. Ochsner J (2017) 17(2):173–80.
35. Leeuw, M, Goossens, MEJB, Linton, SJ, Crombez, G, Boersma, K, and Vlaeyen, JWS. The Fear-Avoidance Model of Musculoskeletal Pain: Current State of Scientific Evidence. J Behav Med (2007) 30(1):77–94. doi:10.1007/s10865-006-9085-0
36. Bonvanie, IJ, Oldehinkel, AJ, Rosmalen, JGM, and Janssens, KAM. Sleep Problems and Pain. Pain (2016) 157(4):957–63. doi:10.1097/j.pain.0000000000000466
37. Tsang, A, Von Korff, M, Lee, S, Alonso, J, Karam, E, Angermeyer, MC, et al. Common Chronic Pain Conditions in Developed and Developing Countries: Gender and Age Differences and Comorbidity With Depression-Anxiety Disorders. J Pain (2008) 9(10):883–91. doi:10.1016/j.jpain.2008.05.005
38. Karran, EL, Grant, AR, and Moseley, GL. Low Back Pain and the Social Determinants of Health: A Systematic Review and Narrative Synthesis. Pain (2020) 161(11):2476–93. doi:10.1097/j.pain.0000000000001944
39. Men, F, Urquia, ML, and Tarasuk, V. Pain-Driven Emergency Department Visits and Food Insecurity: A Cross-Sectional Study Linking Canadian Survey and Health Administrative Data. CMAJ Open (2022) 10(1):E8–18. doi:10.9778/cmajo.20210056
40. Mills, SEE, Nicolson, KP, and Smith, BH. Chronic Pain: A Review of Its Epidemiology and Associated Factors in Population-Based Studies. Br J Anaesth (2019) 123(2):e273–83. doi:10.1016/j.bja.2019.03.023
41. Grol-Prokopczyk, H. Sociodemographic Disparities in Chronic Pain, Based on 12-Year Longitudinal Data. Pain (2017) 158(2):313–22. doi:10.1097/j.pain.0000000000000762
42. Jablonska, B, Soares, JJF, and Sundin, Ö. Pain Among Women: Associations With Socio-Economic and Work Conditions. Eur J Pain (2006) 10(5):435–47. doi:10.1016/j.ejpain.2005.06.003
43. Sterud, T, Tynes, T, Mehlum, IS, Veiersted, KB, Bergbom, B, Airila, A, et al. A Systematic Review of Working Conditions and Occupational Health Among Immigrants in Europe and Canada. BMC Public Health (2018) 18(1):770. doi:10.1186/s12889-018-5703-3
44. Ferrie, JE, Shipley, MJ, Stansfeld, SA, and Marmot, MG. Effects of Chronic Job Insecurity and Change in Job Security on Self Reported Health, Minor Psychiatric Morbidity, Physiological Measures, and Health Related Behaviours in British Civil Servants: The Whitehall II Study. J Epidemiol Community Health (1978)2002) 56(6):450–4. doi:10.1136/jech.56.6.450
45. Syed, HR, Dalgard, OS, Dalen, I, Claussen, B, Hussain, A, Selmer, R, et al. Psychosocial Factors and Distress: A Comparison Between Ethnic Norwegians and Ethnic Pakistanis in Oslo, Norway. BMC Public Health (2006) 6(1):182. doi:10.1186/1471-2458-6-182
46. Soares, JJF, and Grossi, G. Experience of Musculoskeletal Pain. Scand J Caring Sci (1999) 13(4):254–66. doi:10.1111/j.1471-6712.1999.tb00549.x
47. Hagose, M, Burton-Jeangros, C, Fakhoury, J, Consoli, L, Refle, JE, and Jackson, Y. Working Conditions and Self-Reported Health Among Undocumented and Newly Regularized Migrants in Geneva: A Cross-Sectional Study. Int J Public Health (2023) 68:1606394. doi:10.3389/ijph.2023.1606394
48. Lee, H, Ahn, H, Park, CG, Kim, SJ, and Moon, SH. Psychosocial Factors and Work-Related Musculoskeletal Disorders Among Southeastern Asian Female Workers Living in Korea. Saf Health Work (2011) 2(2):183–93. doi:10.5491/SHAW.2011.2.2.183
49. Xiao, H, McCurdy, SA, Stoecklin-Marois, MT, Li, C, and Schenker, MB. Agricultural Work and Chronic Musculoskeletal Pain Among Latino Farm Workers: The MICASA Study. Am J Ind Med (2013) 56(2):216–25. doi:10.1002/ajim.22118
50. Fakhoury, J, Burton-Jeangros, C, Consoli, L, Duvoisin, A, Courvoisier, D, and Jackson, Y. Mental Health of Undocumented Migrants and Migrants Undergoing Regularization in Switzerland: A Cross-Sectional Study. BMC Psychiatry (2021) 21(1):175. doi:10.1186/s12888-021-03149-7
51. Andersson, LMC, Hjern, A, and Ascher, H. Undocumented Adult Migrants in Sweden: Mental Health and Associated Factors. BMC Public Health (2018) 18(1):1369. doi:10.1186/s12889-018-6294-8
52. Myhrvold, T, and Småstuen, MC. The Mental Healthcare Needs of Undocumented Migrants: An Exploratory Analysis of Psychological Distress and Living Conditions Among Undocumented Migrants in Norway. J Clin Nurs (2017) 26(5–6):825–39. doi:10.1111/jocn.13670
53. Hadley, C, Galea, S, Nandi, V, Nandi, A, Lopez, G, Strongarone, S, et al. Hunger and Health Among Undocumented Mexican Migrants in a US Urban Area. Public Health Nutr (2008) 11(2):151–8. doi:10.1017/S1368980007000407
54. Sousa, E, Agudelo-Suárez, A, Benavides, FG, Schenker, M, García, AM, Benach, J, et al. Immigration, Work and Health in Spain: The Influence of Legal Status and Employment Contract on Reported Health Indicators. Int J Public Health (2010) 55(5):443–51. doi:10.1007/s00038-010-0141-8
55. Teunissen, E, Sherally, J, van den Muijsenbergh, M, Dowrick, C, van Weel-Baumgarten, E, and van Weel, C. Mental Health Problems of Undocumented Migrants (UMs) in The Netherlands: A Qualitative Exploration of Help-Seeking Behaviour and Experiences With Primary Care. BMJ Open (2014) 4(11):e005738. doi:10.1136/bmjopen-2014-005738
56. Refle, JE, Fakhoury, J, Burton-Jeangros, C, Consoli, L, and Jackson, Y. Impact of Legal Status Regularization on Undocumented Migrants’ Self-Reported and Mental Health in Switzerland. SSM Popul Health (2023) 22:101398. doi:10.1016/j.ssmph.2023.101398
57. Garcini, LM, Brown, R, Ziauddin, K, Chen, MA, Saucedo, L, LeRoy, AS, et al. Chronic Pain and Psychological Distress Among Undocumented Latinx Immigrants in the USA. J Gen Intern Med (2021) 36(3):585–91. doi:10.1007/s11606-020-05910-2
58. Chauvin, P, Parizot, I, Drouot, N, Tomasino, A, and Simonnot, N. European Survey on Undocumented Migrant’s Access to Health Care (2007). Available from: http://inserm-00416004v2 (Accessed March 23, 2023).
59. Dourgnon, P, Pourat, N, and Rocco, L. European Immigrant Health Policies, Immigrants’ Health, and Immigrants’ Access to Healthcare. Health Policy (New York) (2023) 127:37–43. doi:10.1016/j.healthpol.2022.12.012
60. Constance, P, Paul, D, Florence, J, Antoine, M, Jérôme, W, and Stéphanie, G. In France, One Out of Six Undocumented Immigrants Suffers From Post-Traumatic Stress Disorder. 2022;(266):1–8.
61. Priebe, S, Giacco, D, and El-Nagib, R. Public Health Aspects of Mental Health Among Migrants and Refugees: A Review of the Evidence on Mental Health Care for Refugees, Asylum Seekers and Irregular Migrants in the WHO European Region. Copenhagen: WHO Regional Office for Europe (2016). Available from: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&ved=2ahUKEwi1ltS48fL4AhXfX_EDHegQA-sQFnoECAoQAQ&url=https%3A%2F%2Fwww.euro.who.int%2F__data%2Fassets%2Fpdf_file%2F0003%2F317622%2FHEN-synthesis-report-47.pdf&usg=AOvVaw2pd5eR2EzpFjaT7SinFvf- (Accessed July 12, 2022).
62. Malmusi, D, Palència, L, Ikram, UZ, Kunst, AE, and Borrell, C. Inequalities by Immigrant Status in Depressive Symptoms in Europe: The Role of Integration Policy Regimes. Soc Psychiatry Psychiatr Epidemiol (2017) 52:391–8. doi:10.1007/s00127-017-1348-2
63. Woodward, A, Howard, N, and Wolffers, I. Health and Access to Care for Undocumented Migrants Living in the European Union: A Scoping Review. Health Policy Plan (2014) 29(7):818–30. doi:10.1093/heapol/czt061
64. Herroudi, L, Knuppel, I, and Blavier, A. Post-Migration Journey: Asylum, Trauma and Resilience, Different Trajectories – A Comparison of the Mental Health and Post-Migration Living Difficulties of Documented and Undocumented Migrants in Belgium. Int J Soc Psychiatry (2024) 70(1):201–8. doi:10.1177/00207640231204212
65. Finley, CR, Chan, DS, Garrison, S, Korownyk, C, Kolber, MR, Campbell, S, et al. What Are the Most Common Conditions in Primary Care? Systematic Review. Can Fam Physician (2018) 64(11):832–40.
66. Halley, E, Giai, J, Chappuis, M, Tomasino, A, Henaine, R, and Letrilliart, L. Health Profile of Precarious Migrants Attending the Médecins Du Monde’s Health and Social Care Centres in France: A Cross-Sectional Study. Int J Public Health (2021) 66:66. doi:10.3389/ijph.2021.602394
67. Jackson, Y, Paignon, A, Wolff, H, and Delicado, N. Health of Undocumented Migrants in Primary Care in Switzerland. PLoS One (2018) 13(7):e0201313. doi:10.1371/journal.pone.0201313
68. Barron, P, Bory, A, Chauvin, S, Jounin, N, and Tourette, L. State Categories and Labour Protest: Migrant Workers and the Fight for Legal Status in France. Work, Employment Soc (2016) 30(4):631–48. doi:10.1177/0950017016631451
69. Kroenke, K, Spitzer, RL, and Williams, JBW. The PHQ-9: Validity of a Brief Depression Severity Measure. J Gen Intern Med (2001) 16(9):606–13. doi:10.1046/j.1525-1497.2001.016009606.x
70. Prins, A, Bovin, MJ, Smolenski, DJ, Marx, BP, Kimerling, R, Jenkins-Guarnieri, MA, et al. The Primary Care PTSD Screen for DSM-5 (PC-PTSD-5): Development and Evaluation Within a Veteran Primary Care Sample. J Gen Intern Med (2016) 31(10):1206–11. doi:10.1007/s11606-016-3703-5
71. Legal and Administrative Information Directorate (Prime Minister). What Is State Medical Assistance (AME)? Available from: https://www.service-public.fr/particuliers/vosdroits/F3079?lang=en (Accessed July 3, 2023).
72. Strømme, EM, Igland, J, Haj-Younes, J, Kumar, BN, Fadnes, LT, Hasha, W, et al. Chronic Pain and Mental Health Problems Among Syrian Refugees: Associations, Predictors and Use of Medication Over Time: A Prospective Cohort Study. BMJ Open (2021) 11(9):e046454. doi:10.1136/bmjopen-2020-046454
73. Dragioti, E, Tsamakis, K, Larsson, B, and Gerdle, B. Predictive Association Between Immigration Status and Chronic Pain in the General Population: Results From the SwePain Cohort. BMC Public Health (2020) 20(1):1462. doi:10.1186/s12889-020-09546-z
74. Beck, JG, and Clapp, JD. A Different Kind of Comorbidity: Understanding Posttraumatic Stress Disorder and Chronic Pain. Psychol Trauma (2011) 3(2):101–8. doi:10.1037/a0021263
75. Andreucci, A, Campbell, P, Mundy, LK, Sawyer, SM, Kosola, S, Patton, GC, et al. Sleep Problems Increase the Risk of Musculoskeletal Pain in Boys But Not Girls: A Prospective Cohort Study. Eur J Pediatr (2020) 179(11):1711–9. doi:10.1007/s00431-020-03667-8
76. Garnæs, KK, Mørkved, S, Tønne, T, Furan, L, Vasseljen, O, and Johannessen, HH. Mental Health Among Patients With Chronic Musculoskeletal Pain and Its Relation to Number of Pain Sites and Pain Intensity, a Cross-Sectional Study Among Primary Health Care Patients. BMC Musculoskelet Disord (2022) 23(1):1115. doi:10.1186/s12891-022-06051-9
77. McBeth, J, Wilkie, R, Bedson, J, Chew-Graham, C, and Lacey, RJ. Sleep Disturbance and Chronic Widespread Pain. Curr Rheumatol Rep (2015) 17(1):469. doi:10.1007/s11926-014-0469-9
78. Samulowitz, A, Gremyr, I, Eriksson, E, and Hensing, G. “Brave Men” and “Emotional Women”: A Theory-Guided Literature Review on Gender Bias in Health Care and Gendered Norms Towards Patients With Chronic Pain. Pain Res Manag (2018) 2018:6358624–14. doi:10.1155/2018/6358624
79. Gough, B, Robertson, S, and Luck, H. Engendered Expressions of Anxiety: Men’s Emotional Communications With Women and Other Men. Front Sociol (2021) 6:697356. doi:10.3389/fsoc.2021.697356
80. Bui, Q, Doescher, M, Takeuchi, D, and Taylor, V. Immigration, Acculturation and Chronic Back and Neck Problems Among Latino-Americans. J Immigr Minor Health (2011) 13(2):194–201. doi:10.1007/s10903-010-9371-3
81. Simon, MH, Heenan, PE, Frampton, C, Bayer, S, Keenan, JI, Boer de, NK, et al. Economic Living Standard and Abdominal Pain Mediate the Association Between Functional Gastrointestinal Disorders and Depression or Anxiety. Neurogastroenterology and Motil (2023) 35(1). doi:10.1111/nmo.14465
82. Tuggle, AC, Cohen, JH, and Crews, DE. Stress, Migration, and Allostatic Load: A Model Based on Mexican Migrants in Columbus, Ohio. J Physiol Anthropol (2018) 37(1):28. doi:10.1186/s40101-018-0188-4
83. Kumar, BN, Bernadette, N, and Diaz, E. Migrant Health: A Primary Care Perspective. In: Chapter 2: Migration Health Theories: Healthy Migrant Effect and Allostatic Load. In: Can Both Be True? Migrant Health: A Primary Care Perspective. Boca Raton, FL: CRC Press (2019). (WONCA family medicine).
84. Sharp, TJ, and Harvey, AG. Chronic Pain and Posttraumatic Stress Disorder: Mutual Maintenance? Clin Psychol Rev (2001) 21(6):857–77. doi:10.1016/s0272-7358(00)00071-4
85. Kirmayer, LJ, Groleau, D, Looper, KJ, and Dao, MD. Explaining Medically Unexplained Symptoms. Can J Psychiatry (2004) 49(10):663–72. doi:10.1177/070674370404901003
86. Hasha, W, Fadnes, LT, Igland, J, Vårdal, R, Giusti, LM, Strømme, EM, et al. Two Interventions to Treat Pain Disorders and Post-Traumatic Symptoms Among Syrian Refugees: Protocol for a Randomized Controlled Trial. Trials (2019) 20(1):784. doi:10.1186/s13063-019-3919-x
87. Liedl, A, Müller, J, Morina, N, Karl, A, Denke, C, and Knaevelsrud, C. Physical Activity Within a CBT Intervention Improves Coping With Pain in Traumatized Refugees: Results of a Randomized Controlled Design. Pain Med (2011) 12(2):234–45. doi:10.1111/j.1526-4637.2010.01040.x
88. Hasha, W, Igland, J, Fadnes, LT, Kumar, B, Haj-Younes, J, Strømme, EM, et al. The Effect of Physiotherapy Group Intervention in Reducing Pain Disorders and Mental Health Symptoms Among Syrian Refugees: A Randomized Controlled Trial. Int J Environ Res Public Health (2020) 17(24):9468. doi:10.3390/ijerph17249468
89. Hasha, W, Igland, J, Fadnes, LT, Kumar, BN, Heltne, UM, and Diaz, E. Effect of a Self-Help Group Intervention Using Teaching Recovery Techniques to Improve Mental Health Among Syrian Refugees in Norway: A Randomized Controlled Trial. Int J Ment Health Syst (2022) 16(1):47. doi:10.1186/s13033-022-00557-4
90. Institut National de la Statistique et des Etudes Economiques. The Geographical Location of Immigrants – A High Concentration in the Paris Urban Area (2016). Available from: https://www.insee.fr/en/statistiques/2121531 (Accessed December 9, 2023).
91. Lardjane, S, and Dourgnon, P. Les Comparaisons Internationales d’état de Santé Subjectif Sont-Elles Pertinentes ? Une Évaluation par la Méthode des Vignettes-Étalons. Economie et Statistique (2017)(403–404) 165–77.
92. Summaka, M, Zein, H, Abbas, LA, Elias, C, Elias, E, Fares, Y, et al. Validity and Reliability of the Arabic Patient Health Questionnaire-9 in Patients With Spinal Cord Injury in Lebanon. World Neurosurg (2019) 125:e1016–22. doi:10.1016/j.wneu.2019.01.234
93. Arthurs, E, Steele, RJ, Hudson, M, Baron, M, and Thombs, BD, Canadian Scleroderma Research Group (CSRG). Are Scores on English and French Versions of the PHQ-9 Comparable? An Assessment of Differential Item Functioning. PLoS One (2012) 7(12):e52028. doi:10.1371/journal.pone.0052028
94. Diez-Quevedo, C, Rangil, T, Sanchez-Planell, L, Kroenke, K, and Spitzer, RL. Validation and Utility of the Patient Health Questionnaire in Diagnosing Mental Disorders in 1003 General Hospital Spanish Inpatients. Psychosom Med (2001) 63(4):679–86. doi:10.1097/00006842-200107000-00021
95. Rancans, E, Trapencieris, M, Ivanovs, R, and Vrublevska, J. Validity of the PHQ-9 and PHQ-2 to Screen for Depression in Nationwide Primary Care Population in Latvia. Ann Gen Psychiatry (2018) 17:33. doi:10.1186/s12991-018-0203-5
Keywords: transients and migrants, pain, anxiety, sleep disorder, depression
Citation: Moussaoui S, Vignier N, Guillaume S, Jusot F, Marsaudon A, Wittwer J and Dourgnon P (2025) Pain as a Symptom of Mental Health Conditions Among Undocumented Migrants in France: Results From a Cross-Sectional Study. Int J Public Health 69:1607254. doi: 10.3389/ijph.2024.1607254
Received: 08 March 2024; Accepted: 12 December 2024;
Published: 06 January 2025.
Edited by:
Matthias Richter, Martin Luther University of Halle-Wittenberg, GermanyReviewed by:
Anna-Clara Hollander, Karolinska Institutet (KI), SwedenTwo reviewers who chose to remain anonymous
Copyright © 2025 Moussaoui, Vignier, Guillaume, Jusot, Marsaudon, Wittwer and Dourgnon. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sohela Moussaoui, c29oZWxhLm1vdXNzYW91aUBzb3Jib25uZS11bml2ZXJzaXRlLmZy