 Ziying Yang1
Ziying Yang1 Manping Tang
Manping Tang- 1School of Finance, Southwestern University of Finance and Economics, Chengdu, Sichuan, China
- 2Institute of Chinese Financial Studies, Southwestern University of Finance and Economics, Chengdu, China
- 3College of Management, Sichuan Agricultural University, Chengdu, Sichuan, China
Objectives: This study aimed to examine whether China’s Targeted Poverty Alleviation (TPA) program mitigates depression and explores the mechanisms through which the TPA program affects individuals’ depression.
Methods: Using the data from the China Family Panel Studies (CFPS) survey from 2012 to 2020, we employ a Difference-in-Difference model to analyze the effect of the TPA program on individuals’ depression levels.
Results: Our findings indicate that the TPA program reduces depression scores by 0.116 points, accounting for 6.82% of the standard deviation of depression scores. Further analyses indicate that these effects are mediated through improvements in local medical conditions, reductions in household healthcare spending, increases in household entertainment expenditures, and greater likelihood of living in family.
Conclusion: This study showed that the TPA program significantly mitigates individuals’ depression levels. The possible channels include (1) improving local medical conditions, (2) cutting down household healthcare spending, (3) increasing household entertainment expenses, and (4) increasing the likelihood of living in family.
Introduction
Research indicates that poverty is associated with mental health issues such as depression [1, 2]. However, existing literature on poverty alleviation has predominantly focused on economic outcomes such as income [3, 4], consumption [5, 6], and access to credit [7]. Little attention has been given to how poverty alleviation programs impact mental health. Given the significant role of mental health in overall wellbeing and the notable success of China’s Targeted Poverty Alleviation (TPA) program (See more details about the program in the Supplementary File S1), this study aims to fill this gap by investigating whether and how the TPA program mitigates depression.
We hypothesize that the TPA program alleviates depression through several mechanisms. Introduced by President Xi Jinping in November 2013 and fully implemented by 2015, the TPA program targeted households with per capita incomes below the national poverty line, with the goal of lifting all such households out of poverty by 2020. The program contributes to reducing depression by increasing household income, thereby alleviating financial stress and allowing for higher expenditures on entertainment [8, 9]. Moreover, by enrolling the poor in the social security system and improving local healthcare infrastructure, the TPA program reduces healthcare expenditures and enhances access to medical treatment, thereby further alleviating financial stress. Additionally, the TPA program helps create employment opportunities for those households covered by the TPA program in their hometowns, so that individuals in these households can find jobs in their hometown. As a result, they can live with family, which is associated with family happiness and lower levels of depression [10].
To empirically examine the impact of the TPA program on depression levels, we utilize data from the China Family Panel Studies (CFPS) survey conducted by the Institute of Social Science Survey (ISSS) at Peking University from 2012 to 2020. Employing a Difference-in-Difference (DID) model, our analysis demonstrates a statistically significant reduction in depression levels attributable to the TPA program. Specifically, the TPA program reduces depression scores by 0.116 points, accounting for 6.82% of the standard deviation of depression scores. Further analyses indicate that these effects are mediated through improvements in local medical conditions, reductions in household healthcare spending, increases in household entertainment expenditures, and greater likelihood of living in family.
This study contributes to the literature in several ways. Firstly, it provides a comprehensive evaluation of the effects of China’s TPA program, expanding beyond its economic impacts. While previous studies have highlighted income increases [11, 12], consumption enhancements [6], and improved access to credit [7], our study is among the first to examine its effects on depression among the poor in China.
Secondly, our research contributes to the broader literature on poverty alleviation programs and mental health. Existing studies have explored the impact of poverty alleviation efforts on mental health through different lenses, such as microfinance-based programs and monetary poverty alleviation programs for children and adolescents [13, 14]. By identifying specific mechanisms through which the TPA program affects depression, our study enriches this literature and provides insights applicable to similar programs globally.
Finally, our findings hold practical implications for policymakers worldwide, offering insights into designing effective anti-poverty policies that also address mental health issues. Poverty has long been a global problem [15]. China has nearly one-fifth of the world’s population. With the TPA program, China successfully lifted all rural poor households out of poverty by 2020. China eradicated extreme poverty 10 years ahead of the first target of the UN 20230 Agenda for Sustainable Development [16]. This is a huge success against poverty, which can provide for other countries in eradicating poverty. For example, Pakistan and some African countries are considering adopting China’s poverty alleviation model. Our study underscores the importance of integrating mental health considerations into poverty alleviation strategies, thereby contributing to broader efforts aimed at poverty reduction and enhancing wellbeing globally.
Methods
Data and Sample
The dataset for this study is derived from the China Family Panel Studies (CFPS) survey from 2012 to 2020, conducted by Institute of Social Science Survey (ISSS) at Peking University. This longitudinal survey was conducted biennially. To ensure sample representativeness, CFPS employs a multi-stage probability sampling method using implicit stratification. This approach is akin to methods used in well-known surveys such as the Panel Study of Income Dynamics (PSID), the National Longitudinal Surveys of Youth (NLSY), and the Health and Retirement Study (HRS) in the United States. Previous research has established that the CFPS survey provides a near-nationally representative sample [17].
The data set includes: (1) household information, such as household income, assets, expenses, and family size; (2) individual’s demographic information, such as age, marriage status, health, education, social status, and living in family or not; (3) other individual’s information, such as depression conditions, and perception of local medical condition. We exclude observations with missing values for the key variables. Finally, our sample consists of 129,713 individual-year observations, covering 13,405 households in 551 counties from 31 provinces in China.
Variable Definitions and Summary Statistics
The definitions of the variables in this study are presented in Table 1. Specifically, we construct measurement of individual depression based on the Center for Epidemiological Studies Depression (CESD) scales. The CFPS used CESD-8: (1) I am in a low spirit. (2) I find it difficult to do anything. (3) I cannot sleep well. (4) I feel happy. (5) I feel lonely. (6) I have a happy life. (7) I feel sad. (8) I feel that I cannot continue with my life. Respondents were asked to pick one of the following options for each question: 1. Never (less than 1 day), 2. Sometimes (1-2 days), 3. Often (3-4 days, and 4. Most of the time (5–7 days). CESD-8 has been widely used to assess depressive symptoms [18]. Unlike other questions, in questions (4) and (6), the larger the score is, the less depressive the individual is. To address the inconsistency, we first reverse the meaning of values in questions (4) and (6). Then, we compute the total score of the 8 questions. Finally, we rescale the score by min-max normalization and then multiply by 10. The final score measures an individual’s depression level (
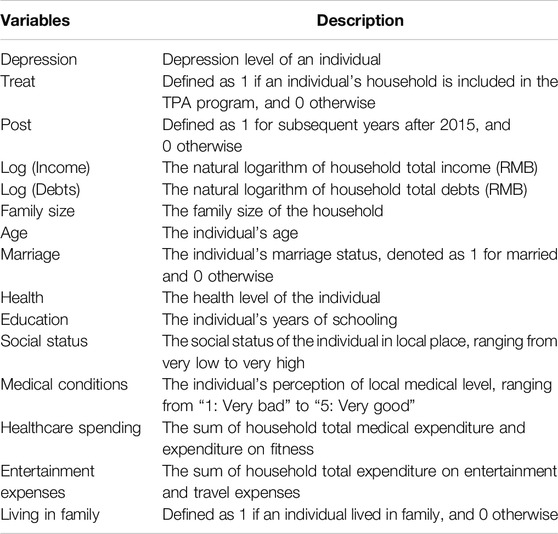
Table 1. Variable definitions (China, 2024).
In addition, following the literature [19], we construct treatment status based on household income per capita and China’s income poverty lines. The Chinese government implemented the TPA program at the end of 2014, and those households whose income per capita is below the national income poverty line were covered by the program. Thus, the treatment variable
Table 2 presents the summary statistics of variables. All continuous variables are winsorized at 1% and 99% to exclude the effect of outliers. The mean of
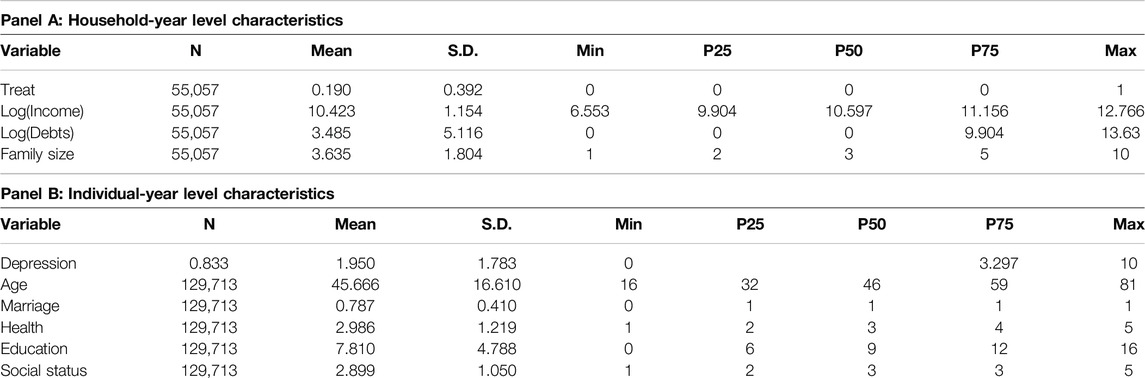
Table 2. Summary statistics (China, 2024).
Empirical Model
To examine the impact of the TPA program on individual’s depression, we set a Difference-in-Difference (DID) model as follows:
where
Results
Main Results
Table 3 displays the estimation results of Equation 1, with column (1) excluding control variables and column (2) including them. As shown in both columns, the coefficients of
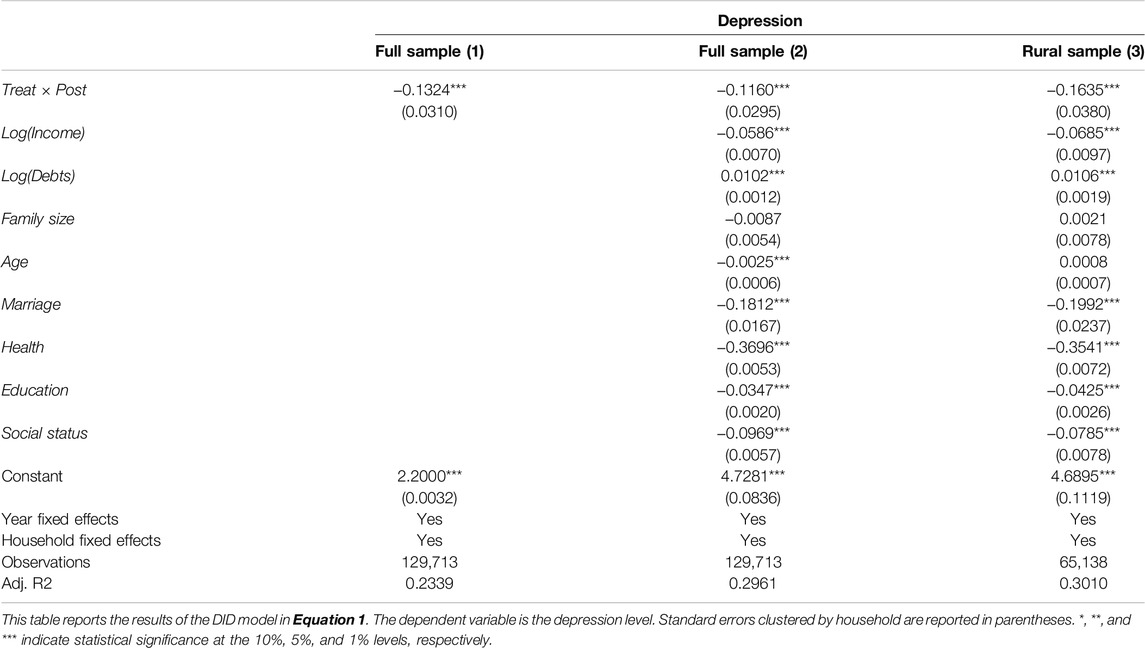
Table 3. Effect of Targeted Poverty Alleviation program on depression (China, 2024).
Our results are robust to (1) changing the definition of treatment group, (2) correcting sample selection bias with propensity score matching (PSM) approach. In addition, our DID model also satisfied the basic assumption of common trend. Finally, we conduct a placebo test to exclude that our findings are not driven by other unobserved or omitted factors. See more details about the robustness checks in Supplementary File S2.
Mechanisms Analyses
In this subsection, we try to explore four mechanisms through which the TPA program may affect individuals’ depression levels: (1) by improving local medical conditions, (2) by cutting down household healthcare spending, (3) by increasing household entertainment expenses, and (4) by increasing the likelihood living in family.
To conduct mechanisms analyses, we set following mediating model [20]:
where
If
Improving Medical Conditions
Medical conditions indeed play a crucial role in influencing individuals’ depressive symptoms. Improved medical infrastructure and access to healthcare services can enhance the identification and management of mental health issues. This improvement enables healthcare professionals to deploy more effective interventions promptly, potentially alleviating symptoms more efficiently.
Moreover, enhanced medical conditions contribute to better treatment outcomes for individuals suffering from illnesses and diseases. Effective treatment reduces anxiety associated with health concerns, thereby potentially decreasing overall levels of depression among affected individuals.
Therefore, if the Targeted Poverty Alleviation (TPA) program succeeds in enhancing medical conditions, it could potentially lead to a reduction in individuals’ depression. This underscores the broader impact that comprehensive poverty alleviation strategies can have on mental health outcomes through improved healthcare access and quality.
Given that the actual medical conditions are difficult to measure, we use individuals’ perceptions of the local medical level as a proxy of local medical conditions. For measurement of local medical conditions, the CFPS survey asked respondents to answer “What do you think of the level of medical expertise there? 1. Very bad. 2. Bad. 3. Fair. 4. Good. 5. Very good.” Then, we estimate Equations 2, 3. The estimation results are shown in columns (1) and (2) of Table 4. We can find that the coefficient of
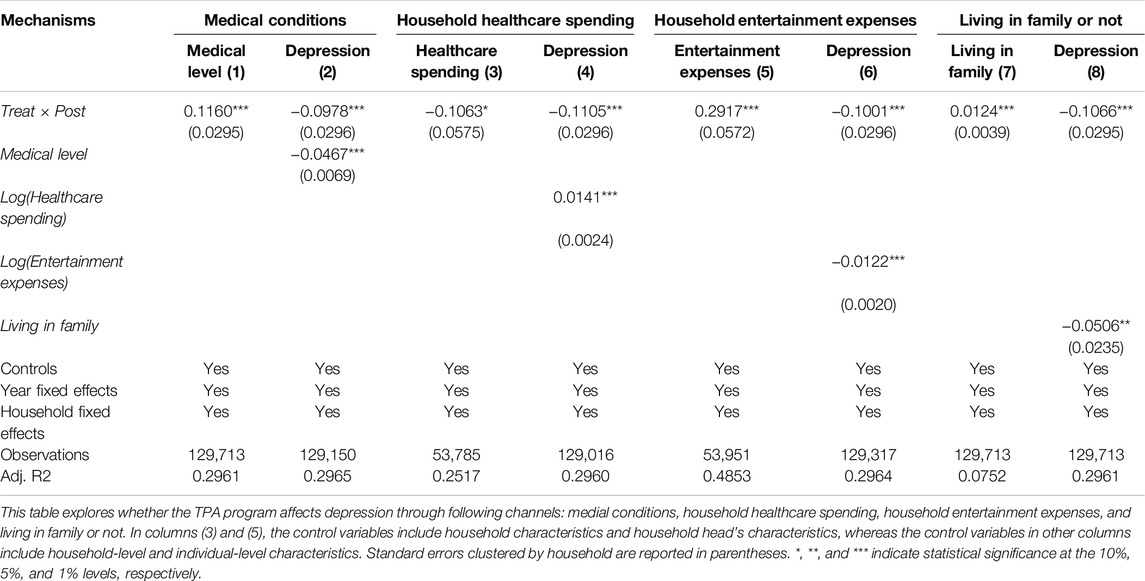
Table 4. Mechanism analyses (China, 2024).
Cutting Down Household Healthcare Spending
In impoverished families, healthcare expenditures often represent a significant financial burden, contributing to heightened levels of depression and anxiety [8]. The Targeted Poverty Alleviation (TPA) program facilitated reforms in healthcare and extended social security coverage to include poor households, potentially alleviating this economic strain. By analyzing household healthcare spending data and employing Equations 2, 3 to assess the mediating effect, we examine whether reduced healthcare spending serves as a viable mechanism.
In CFPS survey, there are two questions: (1) In the past year, the total direct medical expenditure (excluding that was reimbursed or reimbursable but including that was paid by or borrowed from relatives) was ___________ Yuan; (2) In the past year, the total expenditure on fitness (e.g., bodybuilding, physical exercise, and health-related apparatus and products) as ________ Yuan. We use the sum of the two questions’ values to measure household healthcare spending. As demonstrated in column (3) of Table 4, we find a significantly negative coefficient for
These findings underscore the TPA program’s role in mitigating individuals’ depression by alleviating financial pressures related to healthcare expenditures within poor households.
Increasing Household Entertainment Expenses
The Targeted Poverty Alleviation (TPA) program has been shown to increase rural household income and consumption [6], which includes expenditures on household entertainment. Research indicates that engagement in entertainment activities and travel contributes positively to mental health [21, 22]. Therefore, household entertainment expenses represent a plausible mechanism through which the TPA program may alleviate depression.
In CFPS survey, there are two questions: (1) In the past month, the total expenditure on entertainment (including purchasing books, newspapers, magazines, VCDs, and DVDs, and going to cinemas and bars, and so on) was _____Yuan; (2) In the past year, the total expenditure on tourism was _____ Yuan. The household entertainment expenses are measured by 10 times value in question (1) plus value in question (2). The mechanism check results are presented in columns (5) and (6) of Table 4. Column (5) reveals a significant increase in household entertainment expenses attributable to the TPA program, while column (6) demonstrates a negative association between household entertainment expenditures and individuals’ depression levels. These empirical findings provide support for the hypothesis that augmenting household entertainment expenses serves as a viable pathway through which the TPA program reduces depression.
Increasing the Likelihood Living in Family
Research indicates that living with family is associated with increased family happiness and lower levels of depression [10]. Therefore, if the Targeted Poverty Alleviation (TPA) program increases the likelihood of individuals living with their families, it could potentially reduce depression. The TPA program focused on poverty alleviation through industrial development, which generated local employment opportunities and encouraged individuals to remain in their hometowns. Additionally, infrastructure improvements supported by the TPA program, such as enhanced transportation networks, facilitated individuals living with their families.
For measurement of living in family, the CFPS survey asked to answer “You have just mentioned that “Load the name of each family member” is “not/still” living in this family. Please confirm again that whether or not he/she is living in this family. Short-term absence, i.e., the person will return within 3 months, is treated as living in this family. 1. Yes. 0. No.” We estimate the mediating model using Equations 2, 3, with results presented in columns (7) and (8) of Table 4. Column (7) demonstrates that the TPA program increases the probability of individuals living with their families. Column (8) shows a negative relationship between living with family and depression levels. These findings provide empirical evidence supporting the hypothesis that increasing the likelihood of individuals living with their families is a valid mechanism through which the TPA program reduces depression.
Discussion
This study investigates the impact of the Targeted Poverty Alleviation (TPA) program on mitigating depression and explores the mechanisms through which it affects individuals’ mental health. Using data from the China Family Panel Studies (CFPS) survey spanning 2012 to 2020, we employ a Difference-in-Difference (DID) model to estimate these effects. Our findings reveal that the TPA program significantly reduces individuals’ levels of depression. Specifically, the program lowers depression scores by 0.116 points, which represents a 6.82% decrease relative to the standard deviation of depression scores.
Furthermore, the mechanism analyses indicate that the TPA program influences individuals’ depression levels through several channels: (1) improving local medical conditions, (2) reducing household healthcare spending, (3) increasing household entertainment expenses, and (4) enhancing the likelihood of living in family.
Our results have important implications for policymakers who aim to improve the poor’s mental health. Policymakers should incorporate medical conditions, poor households’ healthcare spending, household entertainment, and likelihood to live with family into the poverty alleviation policies so that the policies can better serve the poor by improving their mental health. For example, China implements some local employment programs (such 以工代赈). This kind of programs can increase local employment and income. They can also enable the poor to have more time living with their family and improve family happiness. In addition, the governments can initiate programs which constructing entertainment facilities. This kind of programs can not only provide local employment opportunities, but also increase entertainment activities, which ultimately decreases depression.
There are two limitations in our study. First, although we explore various channels through which the TPA program affects depression levels, it is worth to note the possibility of reverse causality or omitted variable bias in the mediation analysis. Future research can be devoted to investigate between these channels and depression. Second, we examine the overall impact of TPA on depression. However, TPA program has five batches, including industrial development, relocation, eco-compensation, education, and social security. Different batches may have heterogeneous effects on depression. Future research can explore how each batch affects individuals’ depression level.
Author Contributions
ZY: conceptualization, formal analysis, data curation, writing–original draft. CX: methodology, formal analysis, investigation, writing–review and editing. MT: methodology, resources, writing–review and editing. All authors contributed to the article and approved the submitted version.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of Interest
The authors declare that they do not have any conflicts of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.ssph-journal.org/articles/10.3389/ijph.2024.1607106/full#supplementary-material
References
1. Najman, JM, Hayatbakhsh, MR, Clavarino, A, Bor, W, O'Callaghan, MJ, and Williams, GM. Family Poverty OVER the Early LIFE Course and Recurrent Adolescent and Young Adult Anxiety and Depression: A Longitudinal Study. Am J Public Health (2010) 100(9):1719–23. doi:10.2105/AJPH.2009.180943
2. Ridley, M, Rao, G, Schilbach, F, and Patel, V. Poverty, Depression, and Anxiety: Causal Evidence and Mechanisms. Science (2020) 370(6522):eaay0214. doi:10.1126/science.aay0214
3. Meng, L. Evaluating China's Poverty Alleviation Program: A Regression Discontinuity Approach. J Public Econ (2013) 101:1–11. doi:10.1016/j.jpubeco.2013.02.004
4. Tang, J, Gong, J, Ma, W, and Rahut, DB. Narrowing Urban–Rural Income Gap in China: The ROLE of the Targeted Poverty Alleviation Program. Econ Anal Policy (2022) 75:74–90. doi:10.1016/j.eap.2022.05.004
5. Yin, Z, and Guo, P. The Impact of Targeted Poverty Alleviation Policy on Consumption: Evidence from China Household Finance Survey. J Management World (2021) 2021(4):64–84.
6. Chang, Q, Ma, W, Vatsa, P, and Li, J. Has the Targeted Poverty Alleviation Program Improved Household Welfare in Rural China? J Policy Model (2022) 44(5):1041–56. doi:10.1016/j.jpolmod.2022.08.005
7. Yin, Z, Guo, P, and Zhang, L. Active Spring FROM the Source: The Impact of Targeted Poverty Alleviation Policy on Household Credit in Rural China. J Management World (2020)(2) 59–71.
8. Guan, N, Guariglia, A, Moore, P, Xu, F, and Al-Janabi, H. Financial Stress and Depression in Adults: A Systematic Review. PloS one (2022) 17(2):e0264041. doi:10.1371/journal.pone.0264041
9. Bushman, BJ, Baumeister, RF, and Phillips, CM. Do People Aggress to Improve Their Mood? Catharsis Beliefs, Affect Regulation Opportunity, and Aggressive Responding. J Personal Soc Psychol (2001) 81(1):17–32. doi:10.1037/0022-3514.81.1.17
10. Napa, W, Granger, J, Kejkornkaew, S, and Phuagsachart, P. Family Happiness Among People in a Southeast Asian CITY: Grounded Theory Study. Nurs & Health Sci (2020) 22(2):292–9. doi:10.1111/nhs.12688
11. Li, F, Zhang, Y, and Zheng, X. Impact of Targeted Poverty Alleviation: Micro Tracking DATA of POOR Populations. Econ Res J (2020)(8) 171–87.
12. Huang, W, and Zhu, W. Multidimensional Evaluation of the Consolidation and Expansion of Targeted Poverty Alleviation: An Empirical Analysis of Poverty Alleviation Practice in B CITY of G Province in China. J Management World (2021)(10) 111–27.
13. Javed, A, and Naeem, F. Can Microfinance-Based Poverty Alleviation Programs HELP Patients WITH Severe Mental Illness? World Social Psychiatry (2021) 3(3):171–5. doi:10.4103/wsp.wsp_57_21
14. Zaneva, M, Guzman-Holst, C, Reeves, A, and Bowes, L. The Impact of Monetary Poverty Alleviation Programs on Children’s and Adolescents’ Mental Health: A Systematic Review and Meta-Analysis Across Low-Middle-And High-Income Countries. J Adolesc Health (2022) 71(2):147–56. doi:10.1016/j.jadohealth.2022.02.011
15. Liu, Y, Liu, J, and Zhou, Y. Spatio-temporal Patterns of Rural Poverty in China and Targeted Poverty Alleviation Strategies. J Rural Stud (2017) 52:66–75. doi:10.1016/j.jrurstud.2017.04.002
16. United Nations (UN). Transforming Our World: The 2030 Agenda for Sustainable Development. New York, NY, USA: United Nations (2015).
17. Zhang, X, Chen, X, and Zhang, X. The Impact of Exposure to Air Pollution on Cognitive Performance. Proc Natl Acad Sci (2018) 115(37):9193–7. doi:10.1073/pnas.1809474115
18. Bi, K, Chen, P, and Chen, S. Validating the 8-ITEM Center for Epidemiological Studies Depression Scale-Chinese (CESD-Chinese): DATA FROM the China Family Panel Studies (CFPS) (2023).
19. Chen, H, Chen, J, and Ma, C. For a Healthy China: Has TPA Improved the Utilization of Medical Services? J World Economy (2020)(12) 76–101.
20. MacKinnon, DP, Lockwood, CM, Hoffman, JM, West, SG, and Sheets, V. A Comparison of Methods to TEST Mediation and Other Intervening Variable Effects. Psychol Methods (2002) 7(1):83–104. doi:10.1037/1082-989x.7.1.83
21. Hyun, S, Lee, Y, and Park, S. No Travel Worsens Depression: Reciprocal Relationship Between Travel and Depression Among Older Adults. Ann Gen Psychiatry (2022) 21(1):31. doi:10.1186/s12991-022-00405-2
Keywords: targeted poverty alleviation, depression, mental health, mechanisms, difference-in-difference model
Citation: Yang Z, Xiong C and Tang M (2024) Can Targeted Poverty Alleviation Program Reduce Depression? Evidence From China. Int J Public Health 69:1607106. doi: 10.3389/ijph.2024.1607106
Received: 18 January 2024; Accepted: 20 August 2024;
Published: 30 August 2024.
Edited by:
Franco Mascayano, New York State Psychiatric Institute (NYSPI), United StatesReviewed by:
Pedro Goldberg, Columbia University, United StatesTwo reviewers who chose to remain anonymous
Copyright © 2024 Yang, Xiong and Tang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Manping Tang, dGFuZ21wLnNjYXVAZ21haWwuY29t