 José Joaquín Mira1,2,3,4*†
José Joaquín Mira1,2,3,4*† Concepción Carratala-Munuera4,5†María Asunción Vicente3Maria Pilar Astier-Peña6,7
Concepción Carratala-Munuera4,5†María Asunción Vicente3Maria Pilar Astier-Peña6,7 Daniel García-Torres1,2Cristina Soriano8
Daniel García-Torres1,2Cristina Soriano8 Alicia Sánchez-García3
Alicia Sánchez-García3 Elisa Chilet-Rosell9Vicente F. Gil-Guillén4,5Adriana López-Pineda4,5‡
Elisa Chilet-Rosell9Vicente F. Gil-Guillén4,5Adriana López-Pineda4,5‡ Virtudes Pérez-Jover3,10,11‡
Virtudes Pérez-Jover3,10,11‡- 1Alicante-Sant Joan Health District, Alicante, Spain
- 2ATENEA Research, Foundation for the Promotion of Health and Biomedical Research of Valencia Region (FISABIO), San Juan de Alicante, Spain
- 3Health Psychology Department, Miguel Hernandez University of Elche, Elche, Spain
- 4RICAPPS—Red de Investigación en Cronicidad, Atención Primaria y Prevención y Promoción de la Salud, Sant Joan Alacant, Spain
- 5Clinical Medicine Department, Miguel Hernandez University of Elche, Elche, Spain
- 6Universitas Health Centre, Zaragoza, Spain
- 7Public Health Service of Aragon, University of Zaragoza, Grupo de Investigación en Bioética de Aragón, Instituto de Investigación Sanitaria de Aragón, Aragón, Spain
- 8Centro de Salud de Mutxamel, Mutxamel, Spain
- 9Public Health, History of Medicine and Gynecology Department, Miguel Hernandez University of Elche, Elche, Spain
- 10Calitè Research, Applied Psychology Research Centre, Miguel Hernández University, Elche, Spain
- 11Hospital Psychology Research Group, Instituto de Investigación Sanitaria y Biomédica de Alicante (ISABIAL), Hospital General Universitario de Alicante, Alicante, Spain
Objectives: This study aimed to evaluate gender-based disparities in preventable adverse events due to low-value practices (LVPs) in primary care.
Methods: A retrospective cohort study in Alicante, Spain.
Results: A total of 1,516 patient records were examined, finding that older individuals and women experienced more LVP-related events. Female patients faced a higher volume of such events than males with the same health issue. Interaction analysis revealed patients treated by male physicians had more severe events, while those attended by females experienced milder ones. Adverse events were more frequent in LVPs associated with gender-based reasons.
Conclusion: These results highlight the need for tailored healthcare professional awareness programs on overuse’s impact on safety. Addressing outcome differences between male and female patients should inform awareness campaigns.
Introduction
Despite the rising costs in developed Western societies, patient outcomes remain suboptimal [1], and adverse events continue to pose a significant challenge across all healthcare systems [2–4]. Due to its role in orchestrating patient flow within the healthcare system, primary care is pivotal in achieving favorable patient outcomes [5]. Although less studied, one of the causes of adverse events in primary care is directly related to recommending, administering, or prescribing healthcare services that are unlikely to benefit patients [6–8], which we consider as overuse [9].
The volume of patients subjected to low-value practices (LVPs) in the United States, Canada, Australia, and Sweden reach up to 80%, depending on the type of practice [10]. In Primary Care in Spain [11], nearly 6 out of 10 adult patients and 4 out of 10 pediatric patients annually receive at least one prescription classified as overuse. Examining only the overage in expenses resulting from unnecessary prescriptions of benzodiazepines, NSAIDs, lipid-lowering agents, paracetamol, and ibuprofen within a single year, reveals an annually total surpassing 290 million euros. This constitutes 2.8% of the entire Spanish pharmaceutical expenditure in 2018 [12], accounting solely for the cost of the prescribed medications. The continued occurrence of overuse in primary care is frequently linked to various factors, including limited time, constrained access to comprehensive patient data, defensive medical practices, and the approval of prescription decisions either made by healthcare colleagues or requested by patients [7, 13–15].
Recent studies also highlight differences in the frequency of LVPs between male and female patients [16]. Moreover, the number of adverse events due to overuse has been suggested higher in women [8]. Although it is known that women are negatively affected by a gender bias in the therapeutic effort, and they experience greater delays in diagnosis [17–19], the male and female difference has not yet been investigated in relation to overuse, which means that interventions aimed at reducing it do not consider the differential impact on female patients, who could be particularly and negatively affected by its consequences. Therefore, the overarching aim of this research is to assess if there are differences among male and female patients treated by male or female family physicians with regard the occurrence of preventable adverse events due to LVPs in the primary care setting.
In this study, we reach out to test the following hypotheses developed based on the results of previous studies within primary care [8, 20, 21].
H1. A higher number of LVPs are identified among female patients compared to male patients within similar age groups and reasons for consultation.
H2. Male and female family physicians are responsible of a similar number of LVPs among their patients.
H3. A higher number of preventable adverse events related to LVPs are identified among female patients compared to male patients within similar age groups and reasons for consultation.
H4. Male and female family physicians are involved in a similar number of preventable adverse events related to LVPs among their patients.
H5. Preventable adverse events stemming from overuse, either due to conditions or symptoms more commonly found in patients of a specific sex or those attributed to gender-related reasons, exhibit similarity.
Methods
Design
A retrospective cohort study in which a random selection of patients attending primary care consultations in Alicante province (Spain) was performed. The STROBE checklist was used as a guide for reporting the study [22]. The study protocol was published first [23].
Primary Care in Spain
Spanish primary care is a cornerstone of the country’s healthcare system, offering accessible, and comprehensive healthcare services to individuals who require ongoing medical attention, often due to chronic illnesses. This level of care ensures universal access to quality healthcare for individuals of all ages. Preventive care, early intervention, and continuity of care is provided by multidisciplinary teams of family physicians, pediatricians, nurses, and allied health professionals.
Definitions
In this study, overuse was defined as continuing to do what should not be done (e.g., ignoring the “Do Not Do” recommendations). The LVPs considered in the study were derived from the Spanish Commitment to Quality initiative list of recommendations [24, 25], formulated according to the Choosing Wisely campaign’s methodology to mitigate overuse [26–28]. Adverse event was defined as injury resulting from medical management or a complication, rather than the underlying disease, leading to extended hospitalization and/or disability at discharge from medical care [27]. Gender bias in health refers to unjustifiable differences in treatment between women and men based on scientific evidence. This bias arises from assuming gender differences where there are none or ignoring genuine differences that necessitate a distinct approach according to evidence [28].
Ethics
The Research Ethic Board of the Sant Joan Hospital approved the study protocol reference 21/061. It was registered on ClinicalTrials.gov https://clinicaltrials.gov/study/NCT05233852 (NCT05233852).
Procedure
A group of reviewers (n = 40) was formed and trained in the study LVPs identification and data collection procedures. Training was provided using anonymized records. During the training, all reviewers assessed the same cases, and concordance was measured using Cohen’s kappa coefficient. A score of 0.63 or higher was deemed acceptable, while a score of 0.84 or higher was considered excellent. Training concluded once an excellent level of concordance was reached. The list of reviewers involved in this study is provided in Supplementary Material S1.
Each reviewer independently assessed selected medical records and recorded study data. Upon identifying an LVP, the reviewer evaluated potential adverse events and, if present, assessed severity and harm extent using the Woods et al [29] scale, where higher scores indicate greater severity and a stronger relationship between the practice and harm. Events with scores above 3 were classified as adverse events, while those above 4 were attributed to LVPs. A blinded recording system was employed.
Data Collection
Data were extracted from the primary care electronic medical records database, Abucasis, between 15 March 2023 and 31 August 2023. In Alicante, as well as in the rest of Spain, all the information about a patient is registered in a unique electronic medical record. Data from medical records were collected using an electronic data collection platform, which incorporated a trigger tool to facilitate the identification and recording of adverse events. This tool, previously used in the SOBRINA study [8], was based on recommendations by Rosenberg et al [29]. The LVPs considered in this study were agreed in a previous study [30] (Table 1). An online consensus technique involving 33 health professionals from family medicine, cardiology, intensive care, and geriatrics was conducted to reach a consensus on LVPs considering three aspects: 1) if it was still a relatively frequent LVP in primary care; 2) its frequency of application was different between men and women, with a probable association with sex or gender; and 3) if the LVP could cause a severe adverse event in the patient. Panelists marked their level of agreement/disagreement on a scale of 0 (strongly disagree) to 10 (strongly agree). The resulting score was the sum of the three scales. The LVPs that yielded a score of 20 points, or more were retained (consensus criterion) and those scoring under 10 points discarded. Then, a select group of panelists were asked to review the final list of LVPs. Additionally, during a session with experts (clinicians and gender bias in health researchers), there was a debate and consensus reached on whether the differences between men and women that could be observed in these previously selected LVPs should be attributed to the presence of gender inequalities in healthcare. In cases where treatment (or test) is indicated for a condition or symptoms that are more prevalent in patients of a specific sex, it was assumed that the risk of overtreatment (or overuse) in patients of that particular sex is higher than in the other. However, when there is no evidence that the symptoms or prevalence of the condition for which the treatment is provided differ between sex, it was assumed that differences in practice application are due to gender-related reasons. We used a scale ranging from −5, entirely attributable to belief on that are more prevalent in patients of a specific sex, to +5, entirely attributable to gender bias. Table 1 shows the outcome of this consensus among experts.
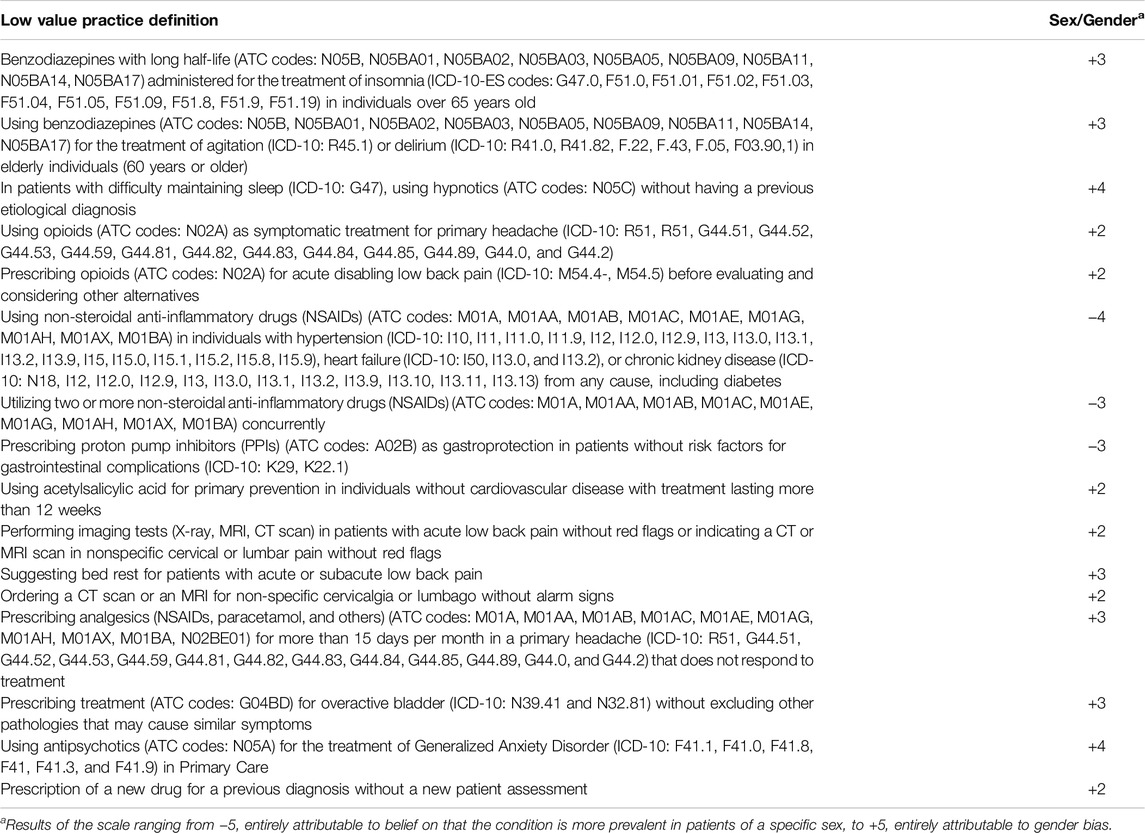
Table 1. Low value practices considered in this study (Gender Bias in Overuse in Primary Care, Spain, 2023).
Sample
The proportion of medical records with at least one LVP was expected to be 50% [8]. With an alpha risk of 0.05 and an accuracy of 2.5%, the minimum required sample size was determined to be 1,538 medical records (50% of which were from women). The study sample was stratified by age group and sex, considering the visit frequencies recorded in the National Health System’s primary care information system for 2018. Study participants were divided into three age groups: 18–59 years, 60–74 years, and >75 years, based on reference ages from prior studies [30]. A simple random sampling method with k = 5 was used to select the medical records of patients attended in the past 3 years.
Data Analysis
Considering the higher frequency of female patients attending primary care consultations [31, 32] (In Spain, 9.6 vs. 5.7 visits per year in 2022 [33]) the adjusted LVPs and preventable adverse events rates have been calculated to correct for this effect in the interpretation of the data. The chi-square test with Yates correction were used to compare the frequency of LVPs in men and women, and the Cochran-Mantel-Haenszel test to analyze differences in the adjusted rate between the sexes. To analyze the relationship between the presence of an adverse event (dependent variable) and the corresponding independent variables such as age, the number of daily medications, patient’s gender, physician’s gender, and their interaction, a Generalized Linear Mixed Model (GLMM) was used. This model accounts for random effects to cover cases where the same patient is affected by more than one adverse event. Statistical significance for all tests was determined at p < 0.05 (two-tailed). The analyses were conducted using the SPSS statistical software and the RStudio V.1.1.463 programming language.
Results
In total, 1,538 electronic medical records were reviewed, but after exclusions (due to missing data), a total of 1,516 patients were included, being 911/1,516 (60.1%) female (Table 2). The mean age of patients attended during the study period was for male 56.4 years (SD 19.4) and female patients 55.2 years old (DT 20.8). They were taking an average of 3.7 medications daily (range 1–25). A total of 245 (68.1%) patients treated by male family physicians were taking less than five drugs per day, while 115 (31.9%) were taking five or more drugs daily. In the case of patients treated by female family physicians, 769 (67.85%) were taking less than five drugs per day and 365 (32.1%) were taking five or more drugs per day. The most frequent main diagnoses in this sample were hypertension, and Type 2 Diabetes.
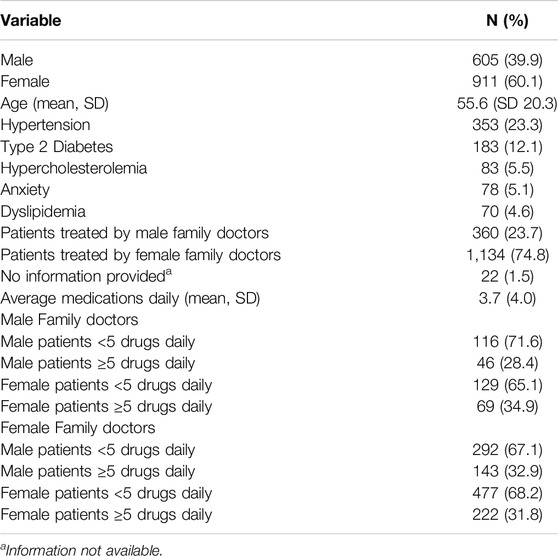
Table 2. Descriptive characteristics of the sample (N = 1,516) (Gender Bias in Overuse in Primary Care, Spain, 2023).
H1. A higher number of LVPs are identified among female patients.
The prevalence of patients suffering LVPs was 465/1,516, 30.7%. A total of 221/605 (36.5%) LVPs occurred in male patients, meanwhile 417/911 (45.7%) LVPs occurred in female patients (p-value = 0.022). As the patient’s age increased, the frequency of LVPs also increased (p-value = 0.024). The number of patients who experienced at least one LVP was 465 (male patients 170/605, 28.1% and female patients 295/911, 32.4%). Among 286 patients, two or more LVPs were registered (103/605, 17.0% male patients; 183/911, 20.1% female patients).
The data confirm H1, with the LVPs considered in this study being more frequent among women than among male patients.
H2. Male and female family physicians are responsible of a similar number of LVPs.
A total of 156/360 (43.3%) LVPs were observed in patients treated by male physicians and 482/1,134 (42.5%) in patients treated by female physicians (p-value = 0.950). Analyzing these LVPs considering both the patient’s sex and the professional’s sex (Table 3), it was observed that only when the family doctor was female, female patients experienced more LVPs than male patients.
The findings suggest rejecting, at least partially, H2, as there was a higher frequency of LVPs among female patients treated by female family physicians compared to male patients treated by the same female family physicians.

Table 3. Frequency of low value practices between male and female patients being treated by male and female family physicians (Gender Bias in Overuse in Primary Care, Spain, 2023).
H3. A higher number of preventable adverse events related to LVPs are identified among female patients.
During the review of electronic medical records, a total of 124 adverse events were identified among 105 patients subjected to one or multiple LVPs in the study (124/638, 19.4%), of which 35/221 (15.8%) were experienced by male patients and 89/417 (21.3%) by female patients.
A total of 26 (26/105, 24.7%) patients experienced two or more preventable adverse events related to the included LVPs in the study. These occurrences of experiencing more than one adverse event related to LVPs were concentrated in individuals aged 60 or older. Among male patients, six (19.35%) of them experienced more than one adverse event, all of whom were treated by male physicians. Among female patients, 20 (27.03%) of them experienced more than one adverse event, of which 6 were treated by male physicians (30%) and 14 by female physicians (70%) (p-value = 0.465). The severity tendency of the adverse events was slightly higher in the case of female patients, but the difference was not statistically significant (p-value = 0.058).
The data allow us to accept H3 because the data trend suggests that female patients experience a higher volume of preventable adverse events related to LVPs than males treated for the same health issue.
H4. Male and female family physicians are involved in a similar number of preventable adverse events related to LVPs.
When analyzing the interaction between patient sex and physician sex a higher proportion of patients attended by male physicians experienced an adverse event compared to those attended by female physicians (p-value<0.000), and in cases where a female physicians attended, female patients experienced more adverse events than male patients (p-value<0.002) (Table 4). The severity of adverse events suffered by male and female patients were higher when the patients were attended by male family physicians (p-value<0.000). Most adverse events were related to medication (99, 79.8%). No differences were identified in the nature of the adverse events suffered by patients when treated by male and female family physicians (p-value = 0.286).
As the patient’s age and the number of daily medications taken by the patient increase, the number of adverse events tends to rise. An interaction effect was observed between the patient’s sex and the family physician’s sex, such that when both the physician and the patient are female, there is a significant increase in the probability of adverse events. However, when the patient is male, being attended by a female physician reduces the probability of experiencing an adverse event.
Based on suggestive data indicating that therapeutic decisions made by male or female family practice had a differentiated effect in terms of the occurrence of preventable adverse events related to LVPs among their patients of either sex, H4 was rejected.
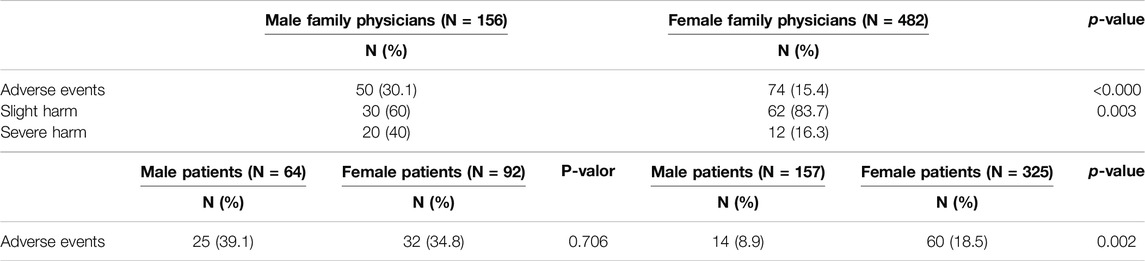
Table 4. Frequency of adverse events related to low value practices in male and female patients when treated by male or female family physicians (Gender Bias in Overuse in Primary Care, Spain, 2023).
H5. Overuse-related adverse events attributed to sex/gender reasons exhibit similarities in specific conditions.
Despite a similar frequency of unnecessary prescriptions or tests for both men and women, whether related to LVPs associated with conditions more prevalent in female patients or influenced by gender-based reasons, a higher number of adverse events occurred in cases linked to LVPs potentially driven by gender bias (Table 5). Consequently, H5 was rejected based on the data.
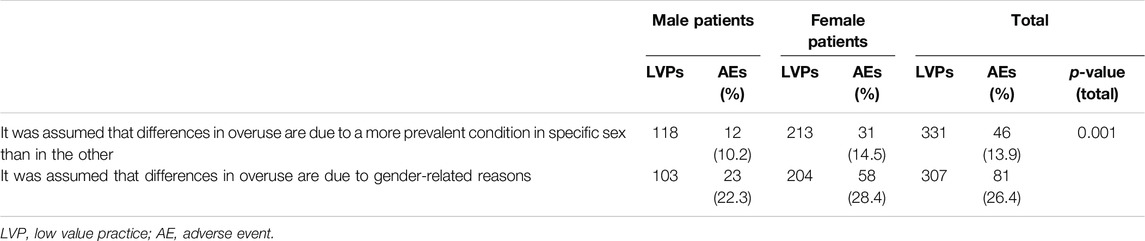
Table 5. Frequency of adverse events related to unnecessary prescriptions or tests associated with conditions more prevalent in female patients or influenced by gender-based reasons (Gender Bias in Overuse in Primary Care, Spain, 2023).
Discussion
The data from this study supports the notion that overutilization poses a risk to patient safety [34]. Additionally, it suggests rejecting the assumption that the frequency of LVPs and the number of preventable adverse events involving male and female family physicians are similar; rather, it supports the idea that women experience a higher number of LVPs and related adverse events. The data suggests an interaction effect between the patient’s and physician’s gender regarding the frequency of both severe and mild adverse events, deserving further attention. This interaction may be specific to the type of LVPs studied in this research. Furthermore, LVPs influenced by gender-based conceptions are more likely to result in unsafe care.
The extent and number of LVPs and their economic impact have been studied for years in various countries and healthcare levels [10, 35, 36]. Some recent studies have emerged identifying the impact of LVPs in terms of patient safety, linking LVPs to the occurrence of preventable adverse events [37]. In one of these initial studies on this topic, our group found that female patients experienced more adverse events related to LVPs than males [8]. In this second study, we aimed to delve deeper into this issue that affects women’s health.
To address this issue, first, a set of LVPs was identified where these differences between males and females could be more pronounced. Second, a review of a set of medical records of patients of both sexes was conducted to describe the frequency at which male and female patients experienced preventable adverse events related to these LVPs.
In this study, women, whose medical records were analyzed, experienced a higher volume of these LVPs during the primary care they received. This data suggests that utilization play a significant role in overutilization. It also corroborates previous observations indicating gender differences that negatively impact the quality of care received by women [8]. This study further delves into analyzing the discrepancy in LVPs frequency between men and women, specifying that when a female patient is treated by a female physician, there is a higher likelihood (up to 7% more) of experiencing one of the LVPs analyzed in this study. These results could be due to family physicians, as suggested in other studies [38], assuming differences between men and women when there are none.
It is not new, the fact that some diseases are more often attributed to men and others to women generating a bias in diagnostic criteria and access to complementary tests or treatments [8]. However, the higher number of adverse events in those cases suspected of gender bias is a novel finding. There is evidence that shows that gender, as a social construct, has a substantial impact on health behaviors, access to and use of health systems, and health system responses [39]. Gender bias can be defined as a systematic error in the social construction of the disease’s history and symptoms, which produces inequitable responses to health problems from the health services, as well as discriminatory responses by professionals [38].
The strategies designed to reduce overutilization could consider these findings and refine their approach, recognizing that female patients have a higher probability of receiving an LVP than male patients. One possible explanation is the higher utilization or healthcare-seeking behavior among women due to a persistent gender bias in our society, where they often take responsibility for family health. Another explanation lies in the recent feminization of the medical profession, which might result in a younger female workforce and therefore, less experience among these female physicians compared to their male counterparts. It could also be attributed to patients exerting more pressure on female physicians than on male physicians to undergo diagnostic tests or specific treatments. This could be influenced by the different status assigned to female professionals, owing to the enduring gender biases [19], as opposed to their male counterparts.
Data collected reveals that nearly a quarter of LVPs ultimately result in a preventable adverse event [8]. In other words, in 2 out of every 10 LVPs, harm is caused by an action on the patient through a treatment that should not have been initiated. Similar to other studies, we have also observed that among older patients, a higher number of preventable adverse events occurred [2, 3]. In this case, the data also suggests that in more severe adverse events, the involvement of male family physicians is higher than that of female physicians. Furthermore, female patients, when treated by female family physicians, exhibited a higher proportion of mild adverse events than male patients.
We know that overutilization poses a threat to the survival of healthcare systems. Moreover, its risk to patients is becoming increasingly evident. In the majority of preventable adverse events identified, the severity of the damage was mild. However, nearly two out of ten resulted in severe permanent consequences for the patient. Both in hospitals and primary care, it has been emphasized that LVPs were not as innocuous as previously thought. Indicating, for example, a test when it’s unnecessary opens up possibilities of initiating equally unnecessary treatments, risking the patient and burdening the healthcare system with unnecessary costs, to the detriment of other patients in need of care.
Considering the latest data indicating that around 7% of patients in primary care in Spain experience an adverse event in a year, the findings of this study clearly point to overutilization as a risk factor, given that the frequency of adverse events associated with LVPs is nearly 3 times higher than expected. Other studies conducted in various countries suggest rates of adverse events in primary care ranging between 1% and 24% [40], with the most common frequency being around 6%–7%, and 1.6% considered as severe events [2].
LVPs pose a threat to the sustainability of healthcare systems due to the increased costs they entail [41–43]. Initiatives implemented to reduce overuse have yielded diverse outcomes [44, 45]. The debate on overutilization and its impact on individuals and systems has expanded, verifying that multicomponent interventions are the most effective in reducing overuse. These interventions, combining various elements, should incorporate information regarding biases based on sex/gender related belief that contribute to women receiving more LVPs, especially when some culminate in adverse events.
Implications
These findings have implications for the content of programs aimed at raising awareness among professionals about the impact of overuse on health outcomes. Given these data, it is advisable to address these potential differences in outcomes between male and female patients when planning awareness campaigns. Some examples highlight that collaboration between patients, caregivers, and clinicians yields positive outcomes in primary care, and a similar approach could be pursued in this case to reduce overuse and concurrently enhance patient safety [46]. Decision aids aimed at increasing patient safety could consider these results to prioritize situations where differences between men and women are more pronounced. Moreover, in clinical practice, particularly concerning these LVPs, clinicians should consider that an unnecessary indication may have an unexpected and negative impact leading to adverse events. Therefore, when making decisions, they should acknowledge that a low-value indication is not harmless and may negatively affect patient safety. They should assess whether the therapeutic approach is disproportionately affecting female patients compared to male patients, inadvertently impacting their health status. Finally, patient schools (e.g., patient experts) and informal caregiver education could serve as suitable platforms to educate both groups about the risks of LVPS in terms of patient safety. In essence, as patient safety remains a challenge for all primary care professionals [47], this data suggests initiating discussions about how overuse compromises patient safety. Despite practices that may seem inconsequential, they can result in a suboptimal level of care.
These results raise new questions. For instance, to what extent do defensive medicine practices causing overuse differ between male and female professionals, and which patient profiles are more susceptible? Additionally, do decision aids integrated into digital systems reduce disparities in LVPs between male and female patients? Studies on overutilization have identified the frequency of various LVPs in different countries. However, transnational comparisons of these LVPs have not been conducted and could be valuable in determining which strategies are more effective in reducing overuse, considering diverse factors, among male and female patients.
Limitations
The sample size was calculated for a set of LVPs and not to determine the impact of gender on the outcome variables for each individual LVP. This study did not delve into differentiating whether the found differences were due to sex (biological) or gender (social) issues. Since the medical record system (Abucasis) does not include data on race, ethnic group, or socioeconomic status, these variables could not be considered. The clinical experience of the professionals who attended to the patients whose medical records were reviewed could not be determined since such information is not encoded and accessing it would have compromised the anonymization of the data. The data extraction for professionals was limited to gender. Professionals did not review their own histories, all coding and recording of information relied on the work of the reviewers. These data were collected from a limited number of cases of each LVP. More work is needed to understand the drivers of low-value care on males and females when attended by male and female family physicians.
Conclusion
The prescriptions and tests considered of low value for the patient, as studied in this research, correspond to common and frequent situations in primary care. They represent a small part of the myriad of conditions addressed at this healthcare level, showcasing only a fraction of the broader reality within primary care settings. Consequently, they serve as a mere sample, underscoring a much larger reality where overuse poses a severe challenge for professionals, patients and healthcare systems. This issue not only jeopardizes patients but also poses a risk, as although the majority of safety incidents are deemed minor and lack permanent consequences, our findings indicate that in some cases, they significantly impact patients’ health. Moreover, these results prompt a deeper reflection and exploration into the influence that gender differences—stemming from both biological and social reasons—might have on overuse and the frequency and nature of associated safety incidents.
Ethics Statement
The studies involving humans were approved by the Sant Joan Hospital, Alicante, Spain. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because in Spain, scientific legislation allows exemptions for epidemiological studies involving the review of clinical records, provided that the data are entirely anonymized. These exemptions apply when it is ensured that patient information has been fully de-identified, removing any details that could lead to the direct or indirect identification of individuals. This practice aligns with ethical and legal protocols established to safeguard the privacy and confidentiality of patient medical information within the context of scientific research.
Author Contributions
JJM, CC-M, AL-P, and VP-J wrote the initial draft of the manuscript and conducted the research and investigation process. CS, AS-G, EC-R, VFG-G, MAV, and MPA-P contributed to the appropriate interpretation of the data, the discussion, and the conclusions. DG-T conducted statistical analysis and data curation. All authors contributed to the article and approved the submitted version.
Funding
The authors declare that financial support was received for the research, authorship, and/or publication of this article. This work is supported by Project Prometeu 2021/061 granted by Conselleria de Innovación, Universidades, Ciencia y Sociedad Digital, Generalitat Valenciana. AS-G was supported by a predoctoral contract for training in research by Miguel Hernández University of Elche (2022/PER/00002). Throughout the composition of this manuscript, JJM benefited from an augmented research activity contract granted by the Carlos III Health Institute (reference INT22/00012).
Conflict of Interest
The authors declare that they do not have any conflicts of interest.
Acknowledgments
The reviewers of the medical records made this study possible. Domingo Orozco, Lourdes Luzón, Johanna Caro, Clara Isabel Pérez Ortiz, Juan Vicente Quintana, Caridad Almazán, Concepción Celaya, Teresa Hernández, Yolanda Agra, Josep Basora, Eva Moreno, Laura Medina, Ana Peiró, Neus Carrillero, Irene Carrillo, Mercedes Guilabert, AV have contributed their ideas to identifying low-value practices and potential gender biases. Prof. Paulo Sousa (Portugal), Prof. Andrea Gecková (Slovakia), Prof. Susanna Tella (Finland), Prof. Bojana Knežević (Croatia) are part of the external scientific committee of the Overgend project and have contributed improvements to the project’s work protocol.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.ssph-journal.org/articles/10.3389/ijph.2024.1607030/full#supplementary-material
References
1. Kwiatkowski, LR, Jolles, DR, and Edwards, C. Overuse, Underuse, and Misuse: Improving Effective Primary Care at a Federally Qualified Health Center. Nurs Forum (2022) 57(4):703–9. Epub 2022 Mar 8. PMID: 35258107. doi:10.1111/nuf.12718
2. Panagioti, M, Khan, K, Keers, RN, Abuzour, A, Phipps, D, Kontopantelis, E, et al. Prevalence, Severity, and Nature of Preventable Patient Harm Across Medical Care Settings: Systematic Review and Meta-Analysis. BMJ (2019) 366:l4185. doi:10.1136/bmj.l4185
3. Gandhi, TK, Weingart, SN, Borus, J, Seger, AC, Peterson, J, Burdick, E, et al. Adverse Drug Events in Ambulatory Care. N Engl J Med (2003) 348(16):1556–64. PMID: 12700376. doi:10.1056/NEJMsa020703
4. Khalil, H, and Huang, C. Adverse Drug Reactions in Primary Care: A Scoping Review. BMC Health Serv Res (2020) 20(1):5. PMID: 31902367; PMCID: PMC6943955. doi:10.1186/s12913-019-4651-7
5. Starfield, B, Shi, L, and Macinko, J. Contribution of Primary Care to Health Systems and Health. Milbank Q (2005) 83(3):457–502. PMID: 16202000; PMCID: PMC2690145. doi:10.1111/j.1468-0009.2005.00409.x
6. Powell, AA, Bloomfield, HE, Burgess, DJ, Wilt, TJ, and Partin, MR. A Conceptual Framework for Understanding and Reducing Overuse by Primary Care Providers. Med Care Res Rev (2013) 70(5):451–72. Epub 2013 Aug 5. PMID: 23916984. doi:10.1177/1077558713496166
7. Olry de Labry Lima, A, Marcos Marcos, J, Marquina Marquez, A, González, VMLÁ, Matas, HA, and Bermúdez, TC. Evidence for Deprescription in Primary Care Through an Umbrella Review. BMC Fam Pract (2020) 21(1):100. PMID: 32513110; PMCID: PMC7278115. doi:10.1186/s12875-020-01166-1
8. Mira, JJ, Carrillo, I, Pérez-Pérez, P, Astier-Peña, MP, Caro-Mendivelso, J, Olivera, G, et al. Avoidable Adverse Events Related to Ignoring the Do-Not-Do Recommendations: A Retrospective Cohort Study Conducted in the Spanish Primary Care Setting. J Patient Saf (2021) 17:e858–e865. doi:10.1097/PTS.0000000000000830
9. Chassin, MR, and Galvin, RW. The Urgent Need to Improve Health Care Quality. Institute of Medicine National Roundtable on Health Care Quality. JAMA (1998) 280:1000–5. doi:10.1001/jama.280.11.1000
10. Brownlee, S, Chalkidou, K, Doust, J, Elshaug, A, Glasziou, P, Heath, I, et al. Evidence for Overuse of Medical Services Around the World. Lancet (2017) 390:156–68. doi:10.1016/S0140-6736(16)32585-5
11. Mira, JJ, Carrillo, I, Gea Velázquez de Castro, MT, Silvestre, C, Olivera, G, Caro-Mendivelso, J, et al. SOBRINA Spanish Study—Analysing the Frequency, Cost and Adverse Events Associated With Overuse in Primary Care: Protocol for a Retrospective Cohort Study. BMJ Open (2019) 9:e023399. doi:10.1136/bmjopen-2018-023399
12. Cheikh-Moussa, K, Caro Mendivelso, J, Carrillo, I, Astier-Peña, MP, Olivera, G, Silvestre, C, et al. Frequency and Estimated Costs of Ten Low-Value Practices in the Spanish Primary Care: A Retrospective Study. Expert Opin Drug Saf (2022) 21(7):995–1003. Epub 2022 Jan 20. PMID: 35020555. doi:10.1080/14740338.2022.2026924
13. Green, AR, Tung, M, and Segal, JB. Older Adults' Perceptions of the Causes and Consequences of Healthcare Overuse: A Qualitative Study. J Gen Intern Med (2018) 33:892–7. doi:10.1007/s11606-017-4264-y
14. Malterud, K, Aamland, A, and Fosse, A. How Can Task Shifting Put Patient Safety at Risk? A Qualitative Study of Experiences Among General Practitioners in Norway. Scand J Prim Health Care (2020) 38(1):24–32. Epub 2020 Jan 23. PMID: 31969033; PMCID: PMC7054920. doi:10.1080/02813432.2020.1714143
15. Mira, JJ, Carrillo, I, Silvestre, C, Pérez-Pérez, P, Nebot, C, Olivera, G, et al. Drivers and Strategies for Avoiding Overuse. A Cross-Sectional Study to Explore the Experience of Spanish Primary Care Providers Handling Uncertainty and Patients’ Requests. BMJ Open (2018) 8:e021339. doi:10.1136/bmjopen-2017-021339
16. Pendrith, C, Bhatia, M, Ivers, NM, Mecredy, G, Tu, K, Hawker, GA, et al. Frequency of and Variation in Low-Value Care in Primary Care: A Retrospective Cohort Study. CMAJ Open (2017) 5(1):E45–E51. PMID: 28401118; PMCID: PMC5378544. doi:10.9778/cmajo.20160095
17. Ayanian, JZ, and Epstein, AM. Differences in the Use of Procedures Between Women and Men Hospitalized for Coronary Heart Disease. N Engl J Med (1991) 325:221–5. doi:10.1056/NEJM199107253250401
18. Ramlakhan, JU, Foster, AM, Grace, SL, Green, CR, Stewart, DE, and Gagliardi, AR. What Constitutes Patient-Centred Care for Women: A Theoretical Rapid Review. Int J Equity Health (2019) 18:182. doi:10.1186/s12939-019-1048-5
19. Roter, DL, and Hall, JA. Women Doctors Don't Get the Credit They Deserve. J Gen Intern Med (2015) 30(3):273–4. PMID: 25361687; PMCID: PMC4351279. doi:10.1007/s11606-014-3081-9
20. Ralston, A, Fielding, A, Holliday, E, Ball, J, Tapley, A, van Driel, M, et al. Low-Value' Clinical Care in General Practice: A Cross-Sectional Analysis of Low Value Care in Early-Career GPs' Practice. Int J Qual Health Care (2023) 27:0. Epub ahead of print. PMID: 37757860. doi:10.1093/intqhc/mzad081
21. Spees, LP, Young, LA, Rees, J, Mottus, K, Leeman, J, Boynton, MH, et al. A Cost Analysis of Rethink the Strip: De-Implementing a Low-Value Practice in Primary Care. Med Care (2023) 61(10):708–14. Epub 2023 Sep 7. PMID: 37943526; PMCID: PMC10478673. doi:10.1097/MLR.0000000000001899
22. von Elm, E, Altman, DG, Egger, M, Pocock, SJ, Gøtzsche, PC, Vandenbroucke, JP, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Lancet (2007) 370(9596):1453–7. PMID: 18064739. doi:10.1016/S0140-6736(07)61602-X
23. Carrillo, I, Lopez-Pineda, A, Pérez-Jover, V, Mira, JJ, Vicente, MA, Fernández, C, et al. Epidemiological Study on Gender Bias and Low-Value Practices in Primary Care: A Study Protocol. BMJ Open (2023) 13:e070311. doi:10.1136/bmjopen-2022-070311
24. Ministerio de Sanidad. Compromiso por la Calidad de las Sociedades Científicas en España (2018). Available from: https://www.mscbs.gob.es/organizacion/sns/planCalidadSNS/cal_sscc.htm (Accessed February 11, 2020).
25. García-Alegría, J, Vázquez-Fernández del Pozo, S, Salcedo-Fernández, F, García-Lechuz Moya, JM, Andrés Zaragoza-Gaynor, G, López-Orive, M, et al. Compromiso por la Calidad de las Sociedades Científicas en España. Rev Clin Esp (2017) 217:212–21. doi:10.1016/j.rce.2017.02.008
26. Centers for Disease Control and Prevention. Maintaining Essential Health Services during COVID-19 in Low Resource, Non-U.S. Settings (2020). Updated Sept. 18.
27. Cassel, CK, and Guest, JA. Choosing Wisely: Helping Physicians and Patients Make Smart Decisions About Their Care. JAMA (2012) 307:1801–2. doi:10.1001/jama.2012.476
28. Born, KB, and Levinson, W. Choosing Wisely Campaigns Globally: A Shared Approach to Tackling the Problem of Overuse in Healthcare. J Gen Fam Med (2019) 20:9–12. doi:10.1002/jgf2.225
29. Rosenberg, A, Agiro, A, Gottlieb, M, Barron, J, Brady, P, Liu, Y, et al. Early Trends Among Seven Recommendations From the Choosing Wisely Campaign. JAMA Intern Med (2015) 175(12):1913–20. doi:10.1001/jamainternmed.2015.5441
30. Perez-Jover, V, Sanchez-García, A, López-Pineda, A, Carrillo, I, Mira, J, and Carratalá-Munuera, C. Identification of Low-Value Practices Susceptible to Gender Bias in Primary Care Setting. Aten Prim (2024) 25:205. doi:10.1186/s12875-024-02456-8
31. Wang, Y, Hunt, K, Nazareth, I, Freemantle, N, and Petersen, I. Do Men Consult Less Than Women? An Analysis of Routinely Collected UK General Practice Data. BMJ Open (2013) 3:e003320. doi:10.1136/bmjopen-2013-003320
32. Redondo-Sendino, Á, Guallar-Castillón, P, Banegas, JR, and Rodríguez-Artalejo, F. Gender Differences in the Utilization of Health-Care Services Among the Older Adult Population of Spain. BMC Public Health (2006) 6:155. doi:10.1186/1471-2458-6-155
33. Ministerio de Sanidad. Portal Estadístico. Área de Inteligencia de Gestión (2024). Available from: https://pestadistico.inteligenciadegestion.sanidad.gob.es/publicoSNS/C/sistema-de-informacion-de-atencion-primaria-siap/actividad/ordinaria (Accessed January 11, 2023).
34. Lipitz-Snyderman, A, and Korenstein, D. Reducing Overuse-Is Patient Safety the Answer? JAMA (2017) 317:810–1. doi:10.1001/jama.2017.0896
35. Chalmers, K, Gopinath, V, Brownlee, S, Saini, V, and Elshaug, AG. Adverse Events and Hospital-Acquired Conditions Associated With Potential Low-Value Care in Medicare Beneficiaries. JAMA Health Forum (2021) 2(7):e211719. PMID: 35977201; PMCID: PMC8796970. doi:10.1001/jamahealthforum.2021.1719
36. San Jose-Saras, D, Vicente-Guijarro, J, Sousa, P, Moreno-Nunez, P, and Aranaz-Andres, JM, Health Outcomes Research Group of the Instituto Ramón y Cajal de Investigación Sanitaria (IRYCIS). Inappropriate Hospital Admission as a Risk Factor for the Subsequent Development of Adverse Events: A Cross-Sectional Study. BMC Med (2023) 21(1):312. PMID: 37592294; PMCID: PMC10433586. doi:10.1186/s12916-023-03024-0
37. Badgery-Parker, T, Pearson, SA, Dunn, S, and Elshaug, AG. Measuring Hospital-Acquired Complications Associated With Low-Value Care. JAMA Intern Med (2019) 179:499–505. doi:10.1001/jamainternmed.2018.7464
38. Tasa-Vinyals, E, Mora, M, and Raich, RM. Gender Bias in Medicine: Concept and State of the Art. C Med Psicosom (2015) 113:14–25.
39. Ruiz-Cantero, MT, Vives-Cases, C, Artazcoz, L, Delgado, A, García Calvente, MM, Miqueo, C, et al. A Framework to Analyse Gender Bias in Epidemiological Research. J Epidemiol Community Health (2007) 61(Suppl. 2):ii46–ii53. doi:10.1136/jech.2007.062034
40. Panesar, SS, deSilva, D, Carson-Stevens, A, Cresswell, KM, Salvilla, SA, Slight, SP, et al. How Safe Is Primary Care? A Systematic Review. BMJ Qual Saf (2016) 25(7):544–53. Epub 2015 Dec 29. PMID: 26715764. doi:10.1136/bmjqs-2015-004178
41. Korenstein, D, Chimonas, S, Barrow, B, Keyhani, S, Troy, A, and Lipitz-Snyderman, A. Development of a Conceptual Map of Negative Consequences for Patients of Overuse of Medical Tests and Treatments. JAMA Intern Med (2018) 178:1401–7. doi:10.1001/jamainternmed.2018.3573
42. Swensen, SJ, Kaplan, GS, Meyer, GS, Nelson, EC, Hunt, GC, Pryor, DB, et al. Controlling Healthcare Costs by Removing Waste: What American Doctors Can Do Now. BMJ Qual Saf (2011) 20:534–7. doi:10.1136/bmjqs.2010.049213
43. Shrank, WH, Rogstad, TL, and Parekh, N. Waste in the US Health Care System: Estimated Costs and Potential for Savings. JAMA (2019) 322:1501–9. doi:10.1001/jama.2019.13978
44. Baron, RJ, Lynch, TJ, and Rand, K. Lessons From the Choosing Wisely Campaign’s 10 Years of Addressing Overuse in Health Care. JAMA Health Forum. (2022) 3(6):e221629. doi:10.1001/jamahealthforum.2022.1629
45. John, A, Kurbanova, N, Ulbing, A, and Qayyum, R. Measuring the Effectiveness of Choosing Wisely Campaign on Laboratory Testing for Hospitalized Patients. Jt Comm J Qual Patient Saf (2022) 48(10):529–33. Epub 2022 Jun 24. PMID: 35858933. doi:10.1016/j.jcjq.2022.06.011
46. Morris, RL, Ruddock, A, Gallacher, K, Rolfe, C, Giles, S, and Campbell, S. Developing a Patient Safety Guide for Primary Care: A Co-Design Approach Involving Patients, Carers and Clinicians. Health Expect (2021) 24(1):42–52. Epub 2020 Nov 3. PMID: 33142022; PMCID: PMC7879544. doi:10.1111/hex.13143
Keywords: overuse, low value practice, adverse events, patient safety, primary care
Citation: Mira JJ, Carratala-Munuera C, Vicente MA, Astier-Peña MP, García-Torres D, Soriano C, Sánchez-García A, Chilet-Rosell E, Gil-Guillén VF, López-Pineda A and Pérez-Jover V (2024) Gender Disparities in Adverse Events Resulting From Low-Value Practices in Family Practice in Spain: A Retrospective Cohort Study. Int J Public Health 69:1607030. doi: 10.3389/ijph.2024.1607030
Received: 28 December 2023; Accepted: 03 July 2024;
Published: 16 July 2024.
Edited by:
Daniela Husarova, University of Pavol Jozef Šafárik Kosice, SlovakiaReviewed by:
Michaela Kosticova, Comenius University, SlovakiaOne reviewer who chose to remain anonymous
Copyright © 2024 Mira, Carratala-Munuera, Vicente, Astier-Peña, García-Torres, Soriano, Sánchez-García, Chilet-Rosell, Gil-Guillén, López-Pineda and Pérez-Jover. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: José Joaquín Mira, am9zZS5taXJhQHVtaC5lcw==
†These authors share first authorship
‡These authors have contributed equally to this work and share last authorship