 Barbara Maria Bürkin1,2*
Barbara Maria Bürkin1,2* Katarzyna Czabanowska3,4
Katarzyna Czabanowska3,4 Suzanne Babich3,5
Suzanne Babich3,5 Núria Casamitjana6
Núria Casamitjana6 Marta Vicente-Crespo7,8
Marta Vicente-Crespo7,8 Luis Eugenio De Souza9
Luis Eugenio De Souza9 John P. Ehrenberg10
John P. Ehrenberg10 Axel Hoffmann1,2Rajesh Kamath11
Axel Hoffmann1,2Rajesh Kamath11 Anja Matthiä1,2Fredros Okumu12
Anja Matthiä1,2Fredros Okumu12 Elizeus Rutebemberwa13,14
Elizeus Rutebemberwa13,14 Marco Waser1,2
Marco Waser1,2 Nino Kuenzli1,2Julia Bohlius1,2
Nino Kuenzli1,2Julia Bohlius1,2- 1Department Education and Training, Swiss Tropical and Public Health Institute, Allschwil, Switzerland
- 2University of Basel, Basel, Switzerland
- 3Department of International Health, Institute of Care and Public Health Research, Faculty of Health, Medicine and Life Sciences, Maastricht University, Maastricht, Netherlands
- 4Department of Health Policy Management, Institute of Public Health, Medical College, Jagiellonian University, Krakow, Poland
- 5Department of Community and Global Health, Richard M. Fairbanks School of Public Health, Indiana University at Indianapolis, Indianapolis, United States
- 6ISGlobal, Hospital Clinic—Universitat de Barcelona, Barcelona, Spain
- 7Research and Related Capacity Strengthening Division, African Population and Health Research Center, Nairobi, Kenya
- 8School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
- 9Collective Health Institute, Federal University of Bahia, Salvador, Bahia, Brazil
- 10Arboretum Frutales Mayas Non-Governmental Organization Cholul, Mérida, Colima, Mexico
- 11Department of Health Innovation, Prasanna School of Public Health, Manipal Academy of Higher Education, Manipal, India
- 12Department of Environmental Health and Ecological Sciences, Ifakara Health Institute, Ifakara, Tanzania
- 13African Field Epidemiology Network (AFENET), Kampala, Uganda
- 14Department of Health Policy, Planning and Management, School of Public Health, Makerere University, Kampala, Uganda
Objectives: This Delphi study intended to develop competencies for transformational leadership in public health, including behavioral descriptions (descriptors) tailored to individuals and their contexts.
Methods: The study involved five rounds, including online “e-Delphi” consultations and real-time online workshops with experts from diverse sectors. Relevant competencies were identified through a literature review, and experts rated, ranked, rephrased, and proposed descriptors. The study followed the Guidance on Conducting and REporting DElphi Studies (CREDES) and the COmpeteNcy FramEwoRk Development in Health Professions (CONFERD-HP) reporting guidelines.
Results: Our framework comprises ten competencies for transformational public health leadership (each with its descriptors) within four categories, and also describes a four-stage model for developing relevant competencies tailored to different contexts.
Conclusion: Educators responsible for curriculum design, particularly those aiming to align curricula with local goals, making leadership education context-specific and -sensitive, may benefit from the proposed framework. Additionally, it can help strengthen links between education and workforce sectors, address competency gaps, and potentially reduce the out-migration of graduates in the health professions.
Introduction
Leadership in a complex and interconnected world is particularly successful if it is adaptable and open to change. Leaders might benefit from pursuing a transformational approach [1, 2]. In the aftermath of COVID-19, contemporary environmental, social and technological trends necessitate transformational leaders adept at handling critical ethical issues. This includes managing resource allocation implications in public health crises, balancing individual privacy rights with public health surveillance, addressing health disparities in underserved communities or navigating the ethical incorporation of emerging technologies, like artificial intelligence, into public health decision-making.
Transformational leaders can emerge at any level [3], in any context, position or sector [2]. They take a whole-system view, deal well with uncertainty, stimulate reflection, and guide their teams to shape the future [4, 5]. Their individual leadership qualities are supported by context-dependent qualities of different world regions, expanding the scope to a global dimension [6, 7]. Transformational leaders in public health may emerge naturally, but it should also be possible to train them with different educational approaches that focus on acquiring competency-specific behaviors to improve public health leadership across a wide range of positions, environments, and contexts [8–10].
Existing competency frameworks categorize “leadership” into a separate domain and describe its behaviors [8, 11–17], but most do not explicitly cultivate transformational leadership competencies and none acknowledge that optimal leadership must be developed in context. Only Kouzes and Posner’s framework can be said to be oriented to transformational leadership [15]. However, its scope is limited to organizational development without providing clear methodology [15]. We need a competency framework to develop transformational leaders in public health, leaders capable of adapting to the changing demands of a rapidly evolving world [18]. The Delphi technique is a common and comprehensive technique to systematically define competencies [8, 11, 12, 14, 16, 19–25] (Box 1) by leveraging and reflecting the collective insights of diverse experts, allowing for anonymous input to foster consensus, and iteratively refining ideas. We did a Delphi study to develop and define competencies for transformational leadership in public health and to generate behavioral descriptions (descriptors) for individual, context-specific and context-sensitive competencies.
Methods
Planning and Design
The Delphi process consisted of five rounds (Figure 1), including three asynchronous online “e-Delphi” consultations and two real-time online workshops with a selected group of experts. Our study report follows Guidance on Conducting and REporting DElphi Studies (CREDES) [26], adheres to The COmpeteNcy FramEwoRk Development in Health Professions (CONFERD-HP) [27] and follows internationally accepted recommendations [28–31] (Figure 1). We identified relevant competencies through literature review and invited experts to evaluate, rank and suggest changes. We defined consensus through a stepwise process. We statistically analyzed expert responses from the first two Delphi Rounds, supplemented by qualitative content analysis. In Delphi Round 3, we also conducted a consensus vote. We analyzed video recordings and group notes to track the process and deal with non-consensus and divergent voting results. After each round, the research team determined saturation and group consensus.
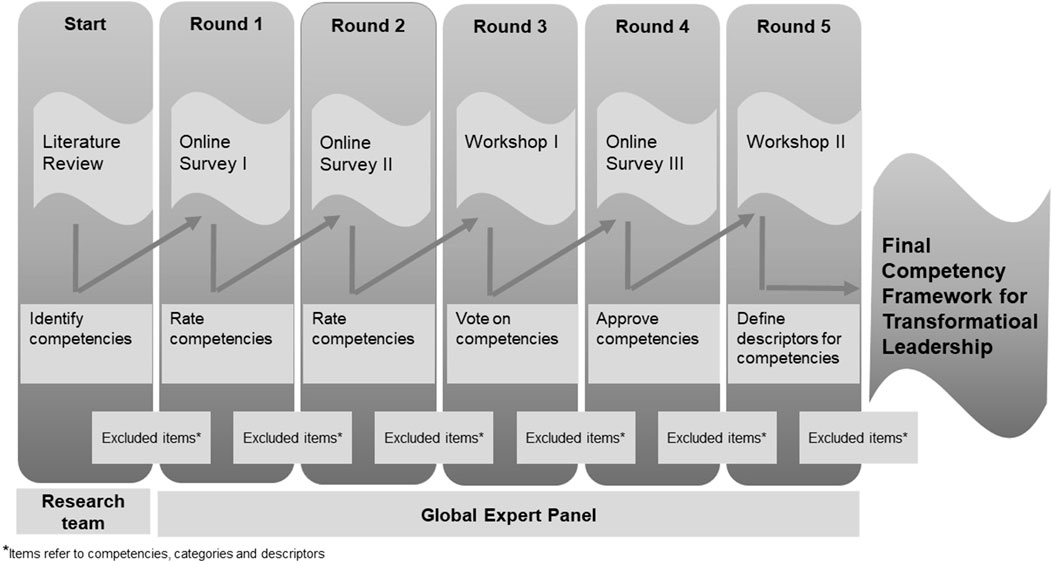
FIGURE 1. Delphi process. Competencies for transformational leadership in public health—an international Delphi consensus study (Allschwil, Switzerland, 2023).
Study Setting
We collected data from an international group of experts from 30 countries in low and middle income countries as well as high income countries, using the web-based platform EvaSys [32]. To reduce bias, we conducted anonymous online survey rounds with selected experts combined with two real-time workshops via the Zoom videoconferencing software [33], after which experts used a chat-based application to anonymously rank statements via voting [32].
Literature Review
To date, there was no consensus-based competency framework for transformational leadership. We based our study on the WHO-ASPHER Competency Framework [11] and other referenced frameworks [8, 12, 14, 16, 19–22, 24, 25]. We chose these frameworks for their approach to consensus-based competency development. Additionally, we selected them for explicitly defining domains or competencies in leadership and management. We singled out relevant framework references listed in the WHO-ASPHER Competency Framework and tabulated them, then categorized the key domains and competencies in the field of management and leadership. To ensure the competency framework to be innovative, applicable in practice and most importantly transformative, we considered transformation-oriented theories such as Theory U [2] in the consensus-based development of the descriptors (Supplementary Box S9).
Composition of Expert Panel
Members of our research team and network suggested and nominated transformational leaders from their professional and scientific trajectories as experts for this study. We specifically asked our research partner Consortium for Advanced Research Training in Africa for nominations. Our sampling frame included global experts in public health. Although this approach only allowed for partial representativeness, and in our case skewed towards African experts, we aimed to gather a diverse pool of expertise (Supplementary Table S3) [26]. Following Van Loo and Semeijn’s (2004) methods to defining and measuring competences, we included experts from different perspectives or relevant research fields for competency development, e.g., education, labor, human resources, or organization, research and development and policy [10]. Following Van Loo and Semeijn’s (2004) approach, we included experts from different perspectives or relevant fields of research for competency development, e.g., education, work, human resources or organization, research and development and policy [10].
These practices ensured that our resulting list of competencies would be based on reality and need, increasing the likelihood that graduates would be able to work across sectors [14]. Our focus on diversity of gender, age, professional background and geography within experts and in contextual considerations ensured our framework was broadly applicable. Public health was not explicitly offered as a perspective. Rather, we assumed that all experts, selected by snowball sampling, worked in public health or related research fields (Supplementary Table S3).
A formal letter and video invitation was sent to 87 people. Willingness to participate in subsequent Delphi rounds (online surveys and online workshops) was a prerequisite for participation. After each session of the online survey, we reminded experts who had not responded. Of those invited, 60 agreed to participate (69%). Median age of experts in Delphi Round 1 was 46–56 years; 59% (n = 26) were women (men: n = 18, 41%). Among the 44 experts in Delphi Round 1, 33% were from Europe, 29% from Africa, 21% from North-Central or South America, and 14% from Asia. Of the 43 people who indicated their workplace, 35% were from Africa, 30% from Europe, 21% from North-Central or South America, and 14% from Asia. Perspectives could overlap, and so 55% (n = 24) of experts offered an “Education” perspective, 52% (n = 23) a “Research and Development” perspective, 21% (n = 9) a “Policy” perspective, and 12% (n = 5) a “Human Resource or organizational” perspective.
Delphi Process
Developing the Survey Instruments
We used an iterative process to develop the questionnaire for Delphi Round 1 and launched it on the EvaSys software platform with the support of a specialist. The research team, a co-researcher, and three external laypersons reviewed and piloted the questionnaire, whereupon the research team approved the final version in two consultation sessions [26]. The questionnaire sought expert information, study details and information on transformational leadership competencies. Central in our approach was asking experts to rate competencies we had compiled from the previous literature review of competency frameworks (Supplementary Figures S3–S6).
Delphi Rounds 1 and 2 Online Survey
Experts ranked their agreement on the importance of the Competencies for Transformational Leadership on a 7-point Likert scale (1 = not important, 2 = low, 3 = slightly, 4 = neutral, 5 = moderately, 6 = very, 7 = extremely important), and also scored the individual work context in which they considered these competencies valuable (these latter data were not part of this study).
Experts could suggest alternative wording and add competencies, make general comments about competencies and comment on their categorization in “Knowing,” “Doing” and “Being” in Delphi Round 2 [34]. We circulated newsletters after the online surveys, reporting clustered recurring themes and arguments (called ‘Golden Nuggets’). These newsletters ensured quality, transparency, clarity and plausibility by explaining our decisions to adjust competencies and categories (Supplementary Boxs S6, S7).
Delphi Round 3—Consensus Workshop
We organized an online Zoom workshop and randomly formed diverse groups of experts. We aimed to gather different perspectives and discuss the classification of competencies into categories derived from the qualitative analysis of the previous two rounds. We appointed experts from our collaborative scientific community 1 week before the workshop to act as group moderators (facilitating the discussion in small groups) or rapporteurs (documenting and presenting the results of the discussion in plenary). The workshop started with a questionnaire asking all experts to anonymously categorize the revised list of competencies. Results were then used to discuss how to categorize the competencies assigned to each group. To ensure a comprehensive consideration of all competencies and to avoid compartmentalization within groups, we assigned each competency twice. All groups then discussed their findings in plenary, allowing all experts to actively consolidate and build consensus (Supplementary Figures S1, S2).
Delphi Round 4—Online Survey
We transferred the fourth version of the consolidated competency list to an anonymous, voluntary survey. We invited all experts to approve the final list and comment (optionally) (Tables 1, 2).
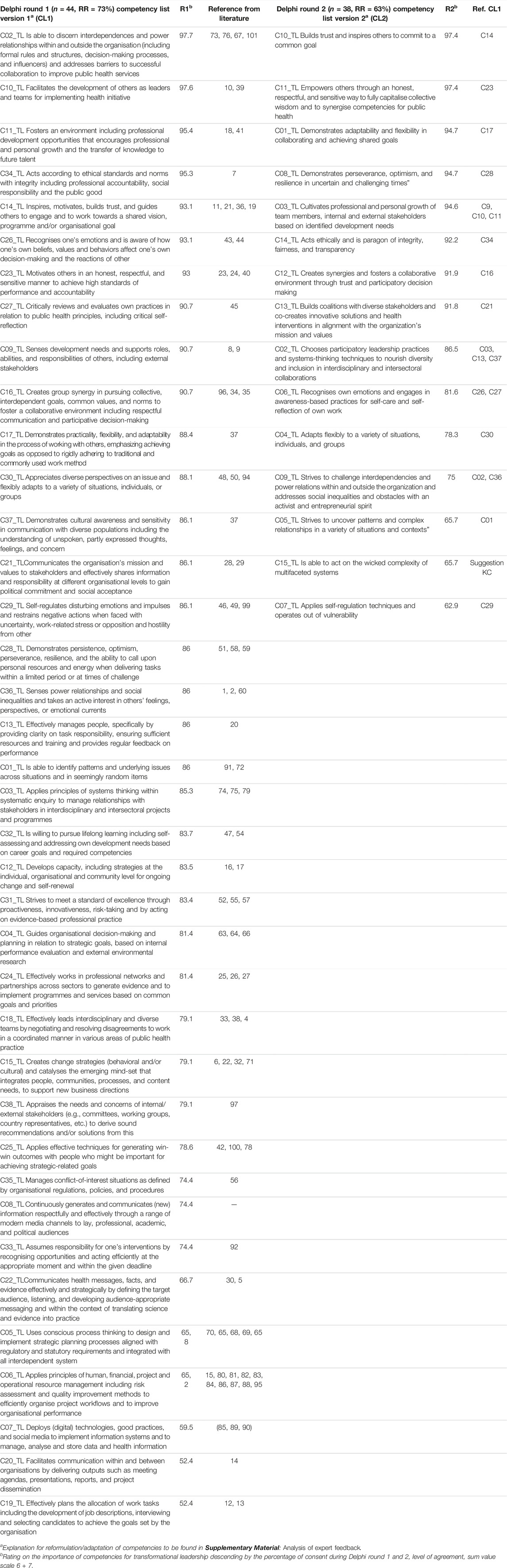
TABLE 1. Evolution path of final competency lists version 1 & 2 for transformational leadership over five rounds of adjusted e-Delphi. Competencies for transformational leadership in public health—an international Delphi consensus study (Allschwil, Switzerland, 2023).
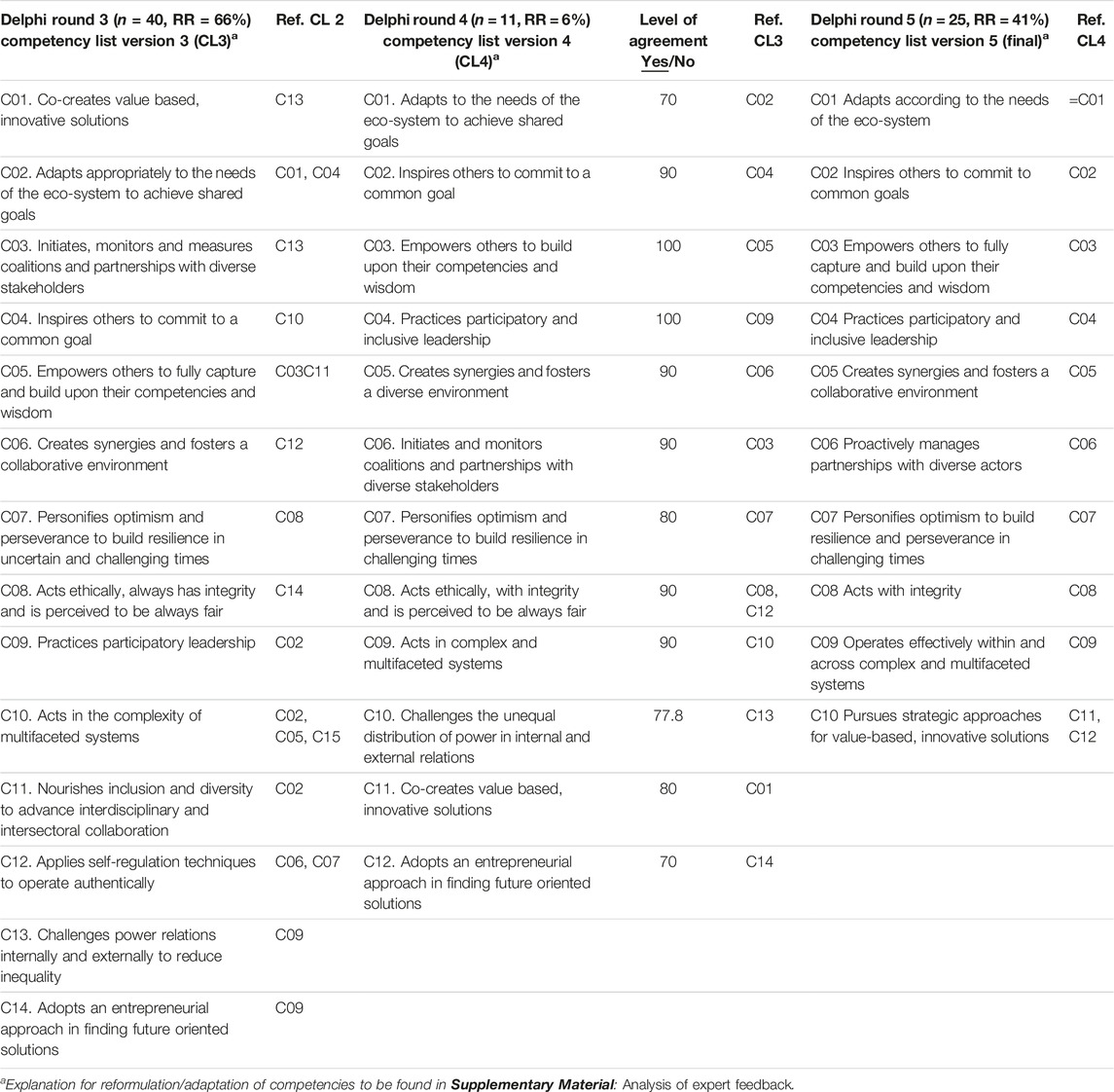
TABLE 2. Evolution path of final competency lists version 3–5 for transformational leadership over five rounds of adjusted e-Delphi. Competencies for transformational leadership in public health—an international Delphi consensus study (Allschwil, Switzerland, 2023).
Box 1 Relevant competency-based frameworks in public health (Allschwil, Switzerland, 2023).
• The WHO-ASPHER Competency Framework for the Public Health Workforce in the European Region [11] combined literature review, several rounds of expert and stakeholder exchanges, and a consensus survey. Leadership and systems thinking, comprise one of its ten domains. Transformational leadership is not a key focus.
• The Regional Core Competency Framework for Public Health (RCCFPH) for the Americas [12] was developed under the guidance of a Regional Steering Group and six Expert Committees within three Regional Workshops and an external meeting. Leadership is considered an “attribute” and a cross-cutting dimension within each domain.
• The Doctor of Public Health (DrPH) Core Competency Model [13] was developed in a modified Delphi process comprising three Delphi rounds and additional conference calls, followed by participation of an advisory panel and seven working groups on individual competency domains to illustrate domains and competencies in a uniform model. Generalist leadership management and research skills were emphasized.
• The National Aboriginal and Torres Strait Islander Public Health Curriculum Framework [14] was developed after consulting the national network of Indigenous academics, practitioners, policymakers, and after holding special learning forum and receiving feedback from Indigenous students. The six public health core competencies do not include leadership.
• The Leadership Practices Inventory [15] one of the most widely used inventories, consolidated thousands of stories, each an answer to the question of what the leader does when they perform their best. The inventory focuses on leadership behavior within five practices “Model the Way,” “Inspire a Shared Vision,” “Challenge the Process,” “Enable Others to Act,” and “Encourage the Heart.”
• The Core Competencies for Public Health Professionals [16] were the product of steady revision and review over many years to ensure their relevance and timeliness. Leadership and systems thinking skills made up one of eight domains that described skill areas within public health.
Delphi Round 5—Operationalization Workshop
We developed a stage model (see Figure 3) to reflect the gradual acquisition of skills. We drew on the Dreyfus scale [35] which we adapted: we defined four stages of transformational leadership instead of the five levels described by Dreyfus. We discarded the “novice” and “advanced beginner” stages as irrelevant and started with “competent” as the first stage. The latter stages were not formally described because both contextual understanding (novice) and emotional closeness should be present for the development of transformational leadership competencies.
We added the “transformational leadership stage”—the highest achievable level [35, 36]. We extracted appropriate examples of behavior (descriptors) from the competency frameworks we used to create our initial list of competencies (version 1) as well as from the feedback on our suggested reformulations from the online questionnaire rounds. Finally, we synthesized and thematically organized the descriptors assigned to the ten competencies [11, 12, 15–17, 37].
We held a second online Zoom workshop to harmonize competency descriptors. To prepare, experts elaborated descriptors for their assigned competencies. During the workshop, the groups each discussed descriptors for two competencies and their allocation to the stage model of competency development (Tables 1, 2).
Data Analysis
For Delphi Round 1, we set a threshold of 85% agreement for each competency to determine the inclusion or exclusion of competencies [38]. We chose this conservative threshold because of the large number of initial competencies. Experts could suggest additional competencies and increase the number for Delphi Round 2. The 85% threshold required experts to score 6 or 7 for a competency on a 7-point Likert scale. For Delphi Round 2, we lowered the threshold to 80% for the following reasons: 1) competencies scored high in Delphi Round 2, 2) the number of competencies dropped from 38 in Delphi Round 1 to 15 in Delphi Round 2 and 3) we needed to provide sufficient basis for discussion in Delphi Round 3. We sorted the competencies according to level of agreement, color-coded corresponding passages and identified synergies between the competencies that achieved 85% (Delphi Round 1) or 80% (Delphi Round 2). We then reordered competencies by descending agreement scores, analyzed and selected relevant text passages from open-ended responses (competencies, categories, comments, and recommendations). We clustered responses by content and extracted alternative formulations for competencies. We grouped similar comments and recommendations into Golden Nuggets, supported with text examples. To systematically assess written comments we applied conventional (using coding categories) and summative (counting and comparisons) qualitative content analysis [39]. We counted how often certain terms appeared in selected segments. We then created a coding scheme consisting of categories, subcategories, and describing indicators and definitions. We reviewed and piloted the coding scheme within the response texts and conducted a conventional analysis by coding with the real text [26]. We consolidated Likert scale ratings of all competencies and revised the competency list after Delphi Rounds 1 and 2. We determined means, median and mode, standard deviations, and inter-quartile ranges to describe aggregated ratings. We synthesized the workshop data (online survey, consensus vote, minutes, and video recordings) into a word table (Delphi Round 3). We jointly discussed and evaluated the plausibility and relevance of feedback from Delphi Round 4 and developed version 5 of the competency list. We analyzed data from the operationalization workshop (Delphi Round 5) to define the most suitable descriptors for each competency. Here we transcribed video recordings and used them together with group protocols to adapt and complement descriptors. All descriptors were critically reviewed by a specialist for gender and diversity aspects [26] (Tables 1, 2). Additional information: We analyzed Delphi Round 1 and 2 data similarly. We used the same coding scheme to analyze free text. During each Delphi round, experts and the team refined the Competency Framework for Transformational Leadership and adjusted the competency list (Supplementary Figures S1, S2).
Ethical Considerations
We received an ethics waiver from the Ethics Committee Northwest and Central Switzerland (Req-2020-01425). Experts were informed of the aims, purpose, procedures, potential risks, and benefits of the study. We explained that the study was voluntary and that they could withdraw at any time without consequence.
No personal identifiers or names were used in the analysis or in the research reports. During the real-time consensus workshop, particular attention was paid to confidentiality by anonymizing the thematic inputs.
Results
Literature Review
Our research team analyzed the WHO-ASPHER Competency Framework [11] and related frameworks [8, 12–25], and extracted and reviewed a draft list of 100 competencies for transformational leadership (Supplementary Table S1). We chose the subordinate categories “Knowing,” “Being” and “Doing” and distinguished between “Educational Context,” and “Transition” and “Professional Context” [34, 37] to indicate transformational leadership resulted from the process by which individuals developed competencies. We chose category-related clusters and adjusted thematic overlaps by merging and consolidating competencies until there were only 38 which we transferred into a draft questionnaire (Supplementary Box S1).
Delphi Procedure Results
In five rounds of adjusted e-Delphi, we condensed the initial 38 competencies into 10 competencies and 4 categories constituting the final Transformational Leadership Competency Framework (Figure 2). This development path includes versions 1 to 5. We identified four competency stages (Figure 3) and systematically developed corresponding descriptors as part of a self-assessment tool (Supplementary File—Self-assessment Tool—Competencies for Transformational Leadership). Tables 1, 2 show the ratings and the evolution path of the final competencies, including list version 1–5 for all rounds. We described our results in the order we obtained them below.
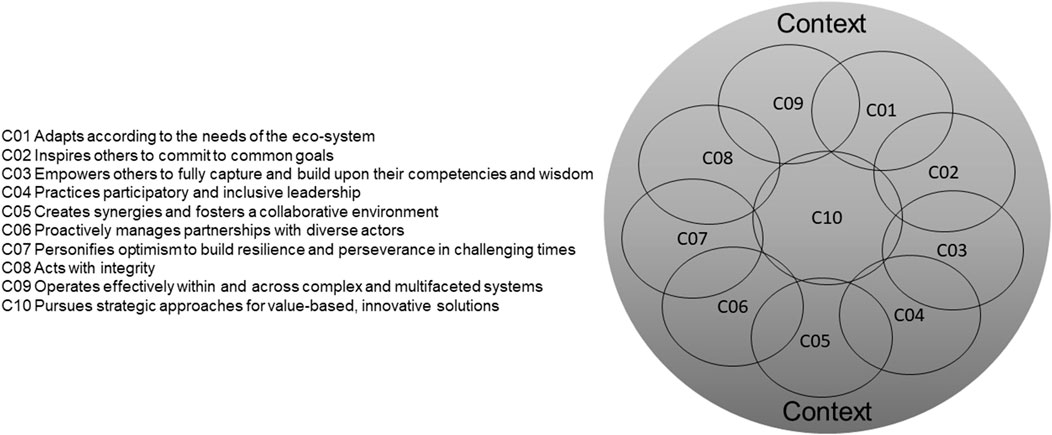
FIGURE 2. Final competency framework. Venn diagram demonstrating individual competencies as interrelated, overlapping and context-dependent. Competencies for transformational leadership in public health—an international Delphi consensus study (Allschwil, Switzerland, 2023).
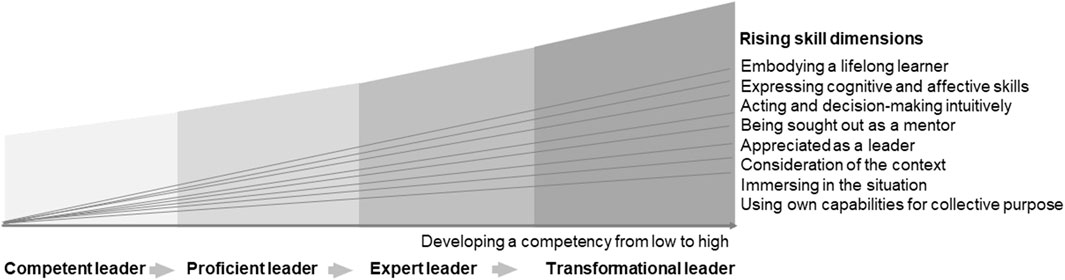
FIGURE 3. Developmental stages of competency development. Competencies for transformational leadership in public health—an international Delphi consensus study (Allschwil, Switzerland, 2023).
Of the 38 competencies in Delphi Round 1, over 85% of experts agreed on 20 competencies. The categories of “Knowing,” “Being,” and “Doing” were discarded after Delphi Round 1 since experts concluded that it was not appropriate to assign competencies to these categories. After analyzing the feedback from Delphi Round 1, we reduced the number of potentially relevant competencies to 15 and generated the following new thematic categories: “Process,” “Context,” “Self,” “Systems Thinking,” “Relationships,” and “Mind-set.” Our qualitative analysis of experts’ written responses in Delphi Round 2 confirmed the appropriateness of these categories (Supplementary Figures S1, S2). Newsletter 1 (after Delphi Round 1) and Newsletter 2 (after Delphi Round 2) synthesized the qualitative analysis with illustrative examples. Of 15 competencies in Delphi Round 2, over 80% of experts agreed on 10 competencies. The broad agreement of the group led to the conclusion that saturation had been reached, meaning that no further competencies should be added. Our analysis of the Likert-scale ratings and the qualitative data analysis of open-ended feedback by the research team resulted in an adapted list of 14 competencies after Delphi Round 2.
In Delphi Round 3 (Consensus workshop), we then asked groups to assign single competencies to the before mentioned categories. Results from the workshop were as follows: 1) all competencies are context-specific and -sensitive, thus experts no longer consider “Context” as a single category; 2) context forms a superordinate thematic circle and precedes all other categories to reflect the complexity of different working contexts; 3) context determines the level to which the performance of competencies can be realized; 4) categories cannot be made distinct, since they are interrelated and merge (gradient); 5) the categories “Self” and “Mind-set” should be combined. After Delphi Round 3, we reduced the competency list from 14 to 12 and adjusted the competency framework (Figure 2) for the Context superordinate for three reasons: 1) to make clear that context determines the level at which a competency can be performed; 2) to illustrate that the relevance of a competency depends on its context; and 3) to highlight the possibility single competencies can be proportionally assigned (weighted by context) to the four categories of “Process,” “Self/Mind-set,” “Systems Thinking,” and “Relationships.”
Delphi Round 4 closed the process of developing the competency list with a voluntary and anonymous EvaSys survey round. Two of the 12 remaining competencies after the Consensus workshop received 100% agreement. The research team assessed agreement on the competencies and the open-ended comments and arrived at 10 final competencies (Supplementary Box S8). In Delphi Round 5 we assigned literature-based behavioral examples (descriptors) to each of the 10 final competencies [2, 11–13, 15–17, 37] (Supplementary Box S9). In parallel, we used the Dreyfus scale as an example when we developed the Developmental stages of competency development (Figure 3) to classify descriptors [35, 36]. We asked experts to identify descriptors for the ten core competencies of transformational leadership and assign them to the stage Competent leader (Stage 1), Proficient leader (Stage 2), Expert leader (Stage 3), and Transformational leader (Stage 4). Experts in the operationalization workshop agreed that they could not assign descriptors to the stages model because stages are not distinct. Instead, they agreed it would be best to take a cumulative approach to assessing degrees of transformational leadership by using the number of transformative behaviors an individual exhibits to quantify their level of competency attainment. We thus drafted a self-assessment tool to estimate the level of competency reached: Users rate themselves on a scale for each descriptor and are scored by cumulative points. We will validate this tool in a follow-up project once we define the numerical ranges that will help us determine how to assign the user to the appropriate stage (Figure 3).
Discussion
Our international Delphi consensus study generated the first set of transformational leadership competencies and behavioral descriptors for public health. This unique framework integrates context as a key factor in developing a fluid, integrated concept of transformational leadership competencies.
Strengths and Limitations of the Study
While experts came from 30 countries, engagement must be regarded as partial and incomplete, especially as there was an overrepresentation of African experts. This limitation might restrict the applicability and robustness of the competencies due to the absence of perspectives from broader and more diverse contexts. Some experts who attended the first workshop did not return for the second. It is possible our results are skewed towards the views of those experts who were most interested in the study. Real-world testing of the competency framework will show whether the competencies are indeed context-specific and context-sensitive. Future researchers could seek mandatory consent to participate in all rounds of Delphi in advance to avoid this problem. Our study was strengthened by the mix of synchronous and asynchronous phases: the asynchronous phases offered experts a high degree of anonymity, while the synchronous phases allowed experts to discuss and take positions within the group.
We singled out the work of Kouzes and Posner [15] and the WHO-ASPHER Framework [11] because of the thematic relevance of their descriptors and their classification into levels. The five overarching practices (Leadership Practices Inventory) Kouzes and Posner describe were key to the development of our competency framework, and particularly our descriptions of practices [15]. However, the Leadership Practices Inventory [15] does not include transparent, open-access representations of their methodological approach to developing the practices they described and their accompanying behaviors. Our study aligns with the WHO-ASPHER Competency Framework [11], the DrPH Core Competency model [8, 13], the Leadership Practices Inventory [15] and the Core Competencies for Public Health Professionals [16] in their approach to define behavioral descriptions for competencies. The WHO-ASPHER framework provides level descriptors for each levels (competent, proficient, expert), but we decided to take a cumulative approach to guide our assessment of the degree to which competencies are achieved and mastered. Our experts agreed, after the second Delphi workshop (Delphi Round 5), that the stages would overlap too much to be clearly divided into “Competent leader,” “Proficient leader,” “Expert leader” and “Transformational leader” (see Figure 3).
Most competency frameworks assume the sequence of competencies is static and usually do not acknowledge the influence of context on the expression of individual competencies. In contrast, our study did not assume that a fixed list of competencies would be universally relevant and globally applicable, so we integrated context, using it as a starting point to determine the relevance of competencies and to direct the acquisition/development of competencies. Though the Australian Framework does explicitly address local context (Aboriginal and Torres Strait Islander health in urban, rural and remote contexts) [14], as does the Doctor of Public Health (DrPH) Core Competency Model [8, 13], which emphasizes the national context and is contextually anchored in research practice-relevant skills, we exceeded their scope by including a high degree of global contextualization, facilitated by our multinational and multiperspective panel of experts from 30 countries. Our framework is complementary to existing competency frameworks in public health that address core public health tasks such as surveillance and monitoring because we claim that transformational leadership is not confined to a single domain within a defined category (see the category “Relations and Interactions” in the WHO-ASPHER Framework) [11] but rather a dimension that cross-cuts domains (see Regional Core Competency Framework for Public Health (RCCFPH) [12]). Drawing on this transformational leadership may lead to more unisonous execution of core public health tasks.
Significance of the Study: Possible Mechanisms and Practical Implications
Transformational leadership competencies matter in the specific situations where they are applied. This makes them globally valuable and relevant across different work cultures. We anticipate that our framework will be of interest to educators who are responsible for curriculum design, and especially those who want to align curricula with local goals and contextualize leadership education. In practice, the framework and its accompanying descriptors should guide the selection and alignment of curricular elements such as learning objectives, methods, activities and assessments. Specifically, this involves examining curricula to assess whether they teach the skills necessary for students to develop certain competencies. This comparison includes evaluating the content and methods used in educational programs (such as textbooks or lesson plans) against a list of skills (descriptors) required for a specific task or job (Supplementary File–Self-assessment Tool: Competencies for Transformational Leadership).
Context sensitivity and specificity is of overriding relevance, especially in countries where educators seek to stem the out-migration of graduates in the health professions [1, 6, 7, 40, 41]. To successfully develop transformational leaders, educators must teach students how to adapt their current knowledge to use in a new ecosystem [18, 42–44]. Our 10 competencies for transformational leadership are intended to constitute a transversal qualification, emphasizing specific behaviors, rather than being taught as distinct units in a course.
To support the transfer of this framework to the real-world environment, we recommend educational curricula incorporate transformational leadership competencies as follows:
i. Transition from intended to emergent learning by complementing research and teaching with a practical transformation-based orientation [4].
ii. Support students along the trajectory of individual development by helping them to reflect and collaborate.
iii. Provide methods and tools to aid students in thinking systematically about transformative work in their particular contexts [1, 2, 4, 19, 25, 41, 45–47].
Our framework for transformational leadership can aid policymakers who want to 1) individualize education and training institutions or 2) provide necessary resources for innovative learning methods. The framework can also 3) be used as an instrument to guide efforts to strengthen transnational health systems by providing demand-driven education.
Public Health managers can use our framework to 1) determine transformational leadership competencies of the workforce, 2) to identify training needs, 3) mix and match teams by competencies, 4) develop job descriptions or interview questions, 5) design performance reviews and 6) continuous quality management. In practice, this is achieved by using the supplementary competency assessment tool (Supplementary File—Self-assessment Tool: Competencies for Transformational Leadership). This self-assessment can take place in a direct exchange in the form of an interview or anonymously via a survey. For this, the frequency of demonstrating competency-related behaviors (descriptors) is used as an approach to quantify the level of competency attainment by an individual.
Unanswered Questions and Future Research
We still need to know more about how to design educational systems that cultivate qualified transformational leaders competent to enter the workforce. To further improve the Competency Framework for Transformational Leadership, researchers should test the self-assessment tool in real-world settings to ensure its suitability for determining competencies. Researchers should seek to define value ranges for the individual stages of each competency and refine its descriptors, they should also determine the importance and relevance of single competencies in various contexts. Then the next group of researchers can determine which curricular elements (e.g., experiential learning, access to networks and partnerships, mentorship, replacement programs) most successfully support students in obtaining the necessary tools, competencies, and know-how to meet challenges in their work as transformational leaders [6, 12].
Conclusion
Using a Delphi process, we successfully developed a framework of 10 competencies and their descriptors for four categories and four stages of competency in transformational leadership for public health. Public health educators can use our context-specific and context-sensitive framework to determine the degree to which transformational leadership competencies are achieved and mastered, optimize teaching curricula, strengthen links between educational and workforce sectors, tailor curricula to specific contexts, and potentially stem the tide of emigrating graduates. The competency framework could be applied to leadership development in domains extending beyond public health. Professionals can use it to benchmark workforce performance and systematically reveal competency gaps the educational sector can then address.
Author Contributions
In this Delphi study on competencies for transformational leadership in public health, each author contributed to the research process in significant ways. BB, KC, and NK conceptualized and designed the study, guided the selection of experts, and facilitated the Delphi process. AM, MW, and PG contributed to the development and refinement of the survey instrument, ensuring its accuracy and consistency for use in the Delphi study. BB conducted the literature review, identified relevant competencies, and organized the data collection and analysis. KC, JB, and NK contributed to the interpretation of results, development of the competency framework, and manuscript writing. All authors BB, KC, SB, NC, MV-C, LD, JE, AH, RK, AM, FO, ER, MW, NK, and JB reviewed and revised the manuscript critically, ensuring its intellectual integrity and scientific rigor. Collectively, the authors collaborated closely, providing expertise from their respective fields to shape the study’s findings and conclusions. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that they do not have any conflicts of interest.
Acknowledgments
We would like to express our deepest gratitude to all the experts who generously shared their time, expertise and insights in the development of the Competency Framework for Transformational Leadership in Public Health. Their dedication and invaluable contributions have been instrumental in shaping the foundation of this publication. The experts participating in the Delphi study included: Dr. A. Hassan (National Institutes of Health, Islamabad, Pakistan). Dr. A. Krolewiecki (Universidad Nacional de Salta, Salta, Argentina). Dr. A. Johnson (Carnegie Corporation New York, United States). Prof. A. Omigbodun (College of Medicine, University of Ibadan, Ibadan, Nigeria). Prof. A. Elliott (Medical Research Council/Uganda Virus Research Institute and London School of Hygiene and Tropical Medicine Uganda Research Unit). Dr. A. Cichowska Myrup (World Health Organization, Geneva, Switzerland). Prof. B. Sripa (Khon Kaen University, Khon Kaen, Thailand). Dr. B. Bonfoh (Centre Suisse de Recherches Scientifiques en Côte d'Ivoire, Abidjan, Côte d'Ivoire). BTT Ha (Hanoi University of Public Health, Hanoi, Vietnam). Dr. B. Kuwane (Youth Health Africa, Johannesburg, South Africa). Prof. C. Vlassoff (University of Ottawa, Ottawa, Canada). Dr. C. Kyobutungi (African Population and Health Research Center, Nairobi, Kenya). Mr. C. Meyer (World Health Organization, Geneva, Switzerland). Prof. D. de Savigny (Swiss Tropical and Public Health Institute, Allschwil, Switzerland). Prof. D. Dambadarjaa (Mongolian National University of Medical Sciences, Ulaanbaatar, Mongolia). Dr. E. Gitau (African Population and Health Research Center, Nairobi, Kenya). Dr. F. Käser (Swiss Academy of Sciences (SCNAT), Bern, Switzerland). Dr. F. Karimi (African Population and Health Research Center, Nairobi, Kenya). Prof. I. Günther (ETH Zurich, Zurich, Switzerland). Ms. I. Nüssli (H.I. Executive Consulting (H.I.E.C), Zurich, Switzerland). Prof. J. Pommier (European Centre for Disease Prevention and Control (ECDC), Stockholm, Sweden). Professor J. Middleton (Association of Schools of Public Health in the European Region, Brussels, Belgium). Prof. J. Igumbor (University of the Witwatersrand, Johannesburg, South Africa). Prof. Laurent Goetschel (swisspeace and University of Basel, Basel, Switzerland). Prof. L. Rispel (School of Public Health, University of the Witwatersrand, Johannesburg). Ms. K. Sørensen (Global Health Literacy Academy, Risskov, Denmark), Dr. L. Magaña (Association of Schools and Programs of Public Health, Washington, D.C., United States). LG Cuervo (Pan American Health Organization, Washington, D.C., United States). Dr. M. Gyapong (University of Health and Allied Sciences, Hohoe, Ghana). Dr. M. Mentz-Coetzee (University of Pretoria, Pretoria, South Africa). M. Krayer von Krauss (World Health Organization, Geneva, Switzerland). Dr. N. Jean-Baptiste (Julius Baer Foundation, Zurich, Switzerland). Prof. N. Khunthikeo (Khon Kaen University, Khon Kaen, Thailand). Dr. N. Salgado de Snyder (Instituto Nacional de Salud Pública, Cuernavaca, México). Dr. OM. Agunbiade (Obafemi Awolowo University, Ile-Ife, Nigeria). Mr. PA. Rodríguez Feria (Universidad de los Andes, Bogotá, Colombia; Maastricht University, Maastricht, Netherlands). PM Venticich (Maastricht University, Maastricht, Netherlands.). Prof. R. Sáenz Madrigal (Universidad de Costa Rica, San José, Costa Rica). Dr. S. Kounnavong (Lao Tropical and Public health Institute, Vientiane, Lao PDR). S. Falabella (ESE: O, Universidad de Chile, Santiago de Chile, Chile). Prof. S. Kinyanjui (KEMRI-Wellcome Trust Research Programme, Kilifi, Kenya). Dr. S. Hostettler (†) (École Polytechnique Fédérale de Lausanne (EPFL), Lausanne, Switzerland). Dr. S. Kounnavong (Lao Tropical and Public health Institute, Vientiane, Lao PDR). Prof. S. Fonn (University of the Witwatersrand Johannesburg, South Africa; University of Gothenburg, Gothenburg, Sweden). Prof. T. Breu (University of Bern, Bern, Switzerland). Prof. T. Ndung’u (Africa Health Research Institute, Durban, South Africa). Prof. T. Chirwa (School of Public Health, University of the Witwatersrand, Johannesburg). Prof. T. Stepurko (National University of Kyiv-Mohyla Academy, Kyiv, Ukraine). Prof. XN. Zhou (Chinese Center For Disease Control and Prevention, Beijing, China). We would also like to acknowledge the pivotal role played by the Swiss Tropical and Public Health Institute (Swiss TPH). Thanks to P. Gschwind, who was instrumental in designing the questionnaire in EvaSys. The institutional support of Swiss TPH was outstanding in enabling and facilitating the research process and ensuring the overall outcome of this study. We would like to express our gratitude to all those who, in various capacities, contributed to the realization of this study. Their collective efforts have not only led to the development of this Competency Framework, but have also strengthened the collaborative networks that will support future research projects.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.ssph-journal.org/articles/10.3389/ijph.2024.1606267/full#supplementary-material
References
1. Frenk, JC, Bhutta, L, Cohen, ZA, Jordan, C, Evans, N, Fineberg, T, et al. Health Professionals for a New Century: Transforming Education to Strengthen Health Systems in an Interdependent World. The lancet (2010) 376(9756):1923–58. doi:10.1016/S0140-6736(10)61854-5
2. Scharmer, O. The Essentials of Theory U: Core Principles and Applications. Oakland: Berrett-Koehler Publishers (2018).
3. Maxwell, JC. The 5 Levels of Leadership: Proven Steps to Maximize Your Potential. New York, Nashville: Center Street (2011).
4. Scharmer, CO. Theory U: Learning From the Future as It Emerges (Exerpt). Oakland: Berrett-Koehler Publishers (2009).
5. Chattopadhyay, S. Transformative Learning: Building the Foundation for Next Stage Organizations (2019). Available from: https://medium.com/age-ofemergence/transformative-learning-building-the-foundation-for-next-stageorganizations-f32600cf5d4a (Accessed October 6, 2020).
6. Ndejjo, R, Ssemugabo, C, Osuret, J, Zziwa, EB, Fonn, S, Alfvén, T, et al. Positioning Africa’s Public Health Doctoral Students to Lead Societal Transformation and Development. BMJ Glob Health (2022) 7(2):e007996. doi:10.1136/bmjgh-2021-007996
7. Oni, T, Yudkin, JS, Fonn, S, Adongo, P, Kaseje, M, Ajuwon, A, et al. Global Public Health Starts at Home: Upstream Approaches to Global Health Training. Lancet Glob Health (2019) 7(3):e301–2. doi:10.1016/S2214-109X(18)30558-8
8. Calhoun, JG, McElligott, JE, Weist, EM, and Raczynski, JM. Core Competencies for Doctoral Education in Public Health. Am J Public Health (2012) 102(1):22–9. doi:10.2105/AJPH.2011.300469
10. Van Loo, J, and Semeijn, J. Defining and Measuring Competences: An Application to Graduate Surveys. Qual Quantity (2004) 38(3):331–49. doi:10.1023/b:ququ.0000031320.86112.88
11. World Health Organization. WHO-ASPHER Competency Framework for the Public Health Workforce in the European Region. Europe: WHO Regional Office for Europe (2020).
12. World Health Organization. Core Competencies for Public Health: A Regional Framework for the Americas. Washington (DC): Pan American Health Organization (2013).
13. ASPH Education Committee. Doctor of Public Health (DrPH) Core Competency Model. version 1.3. Washington: ASPH (2009).
14. Public Health Indigenous Leadership in Education (PHILE) Network 2016. National Aboriginal and Torres Strait Islander Public Health Curriculum Framework. Canberra: PHILE (2017).
15. Kouzes, JM. In: BZ Posner, editor. The Leadership challenge: How to Make Extraordinary Things Happen in Organizations. 5th. San Francisco: Jossey-Bass (2012).
16. Public Health Foundation. Council on Linkages Between Academia and Public Health Practice. In: Core Competencies for Public Health Professionals (2014).
18. Yukl, G, and Lepsinger, R. Leading Change: Adapting and Innovating in an Uncertain World. Leadersh Action (2006) 26(2):3–7. doi:10.1002/lia.1154
19. Verderame, MF, Freedman, VH, Kozlowski, LM, and McCormack, WT. Competency-Based Assessment for the Training of PhD Students and Early-Career Scientists. eLife (2018) 7:e34801. doi:10.7554/eLife.34801
20. Foldspang, A, Birt, CA, and Otok, R. ASPHER’s European List of Core Competences for the Public Health Professional. Brussels: ASPHER (2018).
21. Public Health Association of New Zealand. Generic Competencies for Public Health in Aotearoa-New Zealand. New Zealand: Public Health Association of New Zealand (2007).
22. Public Health Agency of Canada. Core Competencies for Public Health Canada. Ottawa: Public Health Agency of Canada (2008).
23. OECD. Education at a Glance 2014: OECD Indicators. Paris: OECD Publishing (2014). doi:10.1787/eag-2014-en
24. Public Health England HPHA, Public Health Wales, NHS Scotland. Public Health Skills and Knowledge Framework (PHSKF). London: Public Health England (2016).
25. Durette, B, Fournier, M, and Lafon, MJ. The Core Competencies of PhDs. Stud Higher Edu (2016) 41(8):1355–70. doi:10.1080/03075079.2014.968540
26. Jünger, S, Payne, SA, Brine, J, Radbruch, L, and Brearley, SG. Guidance on Conducting and REporting DElphi Studies (CREDES) in Palliative Care: Recommendations Based on a Methodological Systematic Review. Palliat Med (2017) 31(8):684–706. doi:10.1177/0269216317690685
27. Batt, AM, Tavares, W, Horsley, T, Rich, JV, and Williams, B. CONFERD-HP: Recommendations for Reporting COmpeteNcy FramEwoRk Development in Health Professions. Br J Surg (2023) 110(2):233–241. doi:10.1093/bjs/znac394
28. Murphy, M, Black, N, Lamping, D, McKee, C, Sanderson, C, Askham, J, et al. Consensus Development Methods, and Their Use in Clinical Guideline Development. Health Technol Assess (1998) 2(3):1–88. doi:10.3310/hta2030
29. Hasson, F, Keeney, S, and McKenna, H. Research Guidelines for the Delphi Survey Technique. J Adv Nurs (2000) 32(4):1008–15. doi:10.1046/j.1365-2648.2000.01567.x
30. Powell, C. The Delphi Technique: Myths and Realities. J Adv Nurs (2003) 41(4):376–82. doi:10.1046/j.1365-2648.2003.02537.x
31. Hsu, C, and Sandford, BA. The Delphi Technique: Making Sense of Consensus. Pract Assess Res Evaluation (2007) 12(1):10. doi:10.7275/pdz9-th90
34. Anderson, D, and Anderson, LA. Beyond Change Management: Advanced Strategies for Today's Transformational Leaders. John Wiley and Sons (2002).
35. Dreyfus, SE. The Five-Stage Model of Adult Skill Acquisition. Bull Sci Technol Soc (2004) 24(3):177–81. doi:10.1177/0270467604264992
36. Koo, D, and Miner, K. Outcome-Based Workforce Development and Education in Public Health. Annu Rev Public Health (2010) 31:253–69. doi:10.1146/annurev.publhealth.012809.103705
37. Boyatzis, R, and Boyatzis, RE. Competencies as a Behavioral Approach to Emotional Intelligence. J Manag Dev (2009) 28:749–70. doi:10.1108/02621710910987647
38. Niederberger, M, and Spranger, J. Delphi Technique in Health Sciences: A Map. Front Public Health (2020) 8:457. doi:10.3389/fpubh.2020.00457
39. Hsieh, H-F, and Shannon, SE. Three Approaches to Qualitative Content Analysis. Qual Health Res (2005) 15(9):1277–88. doi:10.1177/1049732305276687
40. World Health Organization. Open Mindsets: Participatory Leadership for Health. Geneva: World Health Organization (2016).
41. Drago-Severson, E, and Blum-DeStefano, J. Leadership for Transformational Learning: A Developmental Approach to Supporting Leaders' Thinking and Practice. J Res Leadersh Edu (2014) 9(2):113–41. doi:10.1177/1942775114527082
42. Hill, LA, Tedards, E, and Swan, T. Drive Innovation With Better Decision-Making. Brighton: Harvard Business Review (2021). p. 70–9.
44. Van Schalkwyk, SC, Hafler, J, Brewer, TF, Maley, MA, Margolis, C, McNamee, L, et al. Transformative Learning as Pedagogy for the Health Professions: A Scoping Review. Med Educ (2019) 53(6):547–58. doi:10.1111/medu.13804
45. Crossouard, B, Andres, L, Bengtsen, SS, Castano, LG, Keefer, JM, and Pyhalto, KJFLR. Drivers and Interpretations of Doctoral Education Today: National Comparisons. Frontline Learn Res (2015) 3(3):5–22. doi:10.14786/flr.v3i3.177
46. Scharmer, CO, and von Ameln, F. Upgrading Change Management: Claus Otto Scharmer on the Legacy and Future of Change Management. Gruppe Interaktion Organisation Z Angew Organisationspsychologie (Gio) (2019) 50(2):193–6. doi:10.1007/s11612-019-00464-2
47. Scharmer, O. Vertical Literacy: Reimagining the 21st-Century University (2019). Available from: https://medium.com/presencing-institute-blog/vertical-literacy-12-principles-for-reinventing-the-21st-century-university-39c2948192ee (Accessed May 1, 2020).
Keywords: transformational leadership, competencies, competency framework, Delphi study, context
Citation: Bürkin BM, Czabanowska K, Babich S, Casamitjana N, Vicente-Crespo M, De Souza LE, Ehrenberg JP, Hoffmann A, Kamath R, Matthiä A, Okumu F, Rutebemberwa E, Waser M, Kuenzli N and Bohlius J (2024) Competencies for Transformational Leadership in Public Health—An International Delphi Consensus Study. Int J Public Health 69:1606267. doi: 10.3389/ijph.2024.1606267
Received: 01 June 2023; Accepted: 19 January 2024;
Published: 23 February 2024.
Edited by:
L. Suzanne Suggs, University of Italian Switzerland, SwitzerlandReviewed by:
Reviewed by two reviewers who chose to remain anonymousCopyright © 2024 Bürkin, Czabanowska, Babich, Casamitjana, Vicente-Crespo, De Souza, Ehrenberg, Hoffmann, Kamath, Matthiä, Okumu, Rutebemberwa, Waser, Kuenzli and Bohlius. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Barbara Maria Bürkin, YmFyYmFyYS5idWVya2luQHN3aXNzdHBoLmNo