 Francisco Javier Muñoz-Vela1,2
Francisco Javier Muñoz-Vela1,2 Luciano Rodríguez-Díaz3
Luciano Rodríguez-Díaz3 Juan Gómez-Salgado4,5*Francisco Javier Fernández-Carrasco6
Juan Gómez-Salgado4,5*Francisco Javier Fernández-Carrasco6 Regina Allande-Cussó7Juana María Vázquez-Lara3Javier Fagundo-Rivera8
Regina Allande-Cussó7Juana María Vázquez-Lara3Javier Fagundo-Rivera8- 1Nursing, University of Malaga, Málaga, Andalusia, Spain
- 2Regional University Hospital of Malaga, Málaga, Andalusia, Spain
- 3Nursing Department, Faculty of Health Sciences of Ceuta, University of Granada, Ceuta, Spain
- 4Sociology, Social Work and Public Health, Faculty of Labour Sciences, University of Huelva, Huelva, Spain
- 5Escuela de Posgrado, Universidad de Especialidades Espíritu Santo, Guayaquil, Ecuador
- 6Nursing and Physiotherapy Department, Faculty of Nursing, University of Cádiz, Cádiz, Spain
- 7Nursing, University of Seville, Seville, Andalucia, Spain
- 8Centro Universitario de Enfermería Cruz Roja, University of Seville, Seville, Andalucia, Spain
Objectives: The aim of this study was to explore the impact of the 2020–2022 pandemic on the levels of fear and anxiety in pregnant women and to identify risk and protective factors.
Methods: A systematic review was conducted. Electronic databases were consulted for studies published between January 2020 and August 2022. The methodological quality was assessed using a critical appraisal tool for non-randomised studies.
Results: Seventeen studies were included in the review. A high prevalence of levels of fear and anxiety were observed. Risk factors such as unplanned pregnancy, poor support from partners, or intolerance of uncertainty were identified for high levels of fear. Regarding anxiety, risk factors such as maternal age, social support, financial status, or concern about being able to maintain antenatal follow-ups were identified.
Conclusion: The COVID-19 pandemic had a significant impact on the mental health of pregnant women through increased levels of fear and anxiety. It has not been possible to establish a relationship between significant factors such as gestational age or health emergency control measures with high levels of fear or anxiety.
Introduction
The year 2020 will go down in history as the year of the COVID-19 pandemic. This disease affected the global population and was of greater concern to certain vulnerable groups, such as healthcare professionals, who have had a higher level of exposure to the virus (1) and pregnant women, due to already existing concomitant diseases or life-threatening conditions (2). This population group’s cardiorespiratory and immune systems undergo substantial changes to accommodate the growing pregnancy. This fact characterises pregnancy as a period of particular vulnerability to infectious diseases (3-6). In this regard, there was differing research about the level of vulnerability of pregnant women compared to non-pregnant women during the first weeks of the pandemic. At the beginning, some research suggested that there was no increased threat for pregnant women during COVID-19 infection (7,8). However, more recent studies showed an increased risk of ICU admissions, hospitalisation (9) and, although vertical transmission is extremely rare (8,10), there does appear to be an increased risk for the development of pre-eclampsia, threatened preterm delivery, or low birth weight (11,12).
The fear of potential risk and lack of control caused by the COVID-19 pandemic has led to a perception of increased risk, according to the Perceived Risk Theory (13,14), as defined by other theories such as the Protection Motivation Theory (15) and the Health Belief Model (16), which propose two different aspects of risk perception: the subjective likelihood of contracting a disease or condition (perceived vulnerability) and the degree to which we are concerned (perceived severity) about the derived consequences. Given that the emergence of COVID-19 and its pandemic nature has exacerbated fears around the world, the situation of special vulnerability together with the uncertainty of its possible consequences on the unborn child make women during pregnancy a population group of special susceptibility to fear (17). Therefore, there is a need to assess these levels of anxiety and fear as attitudinal factors that may be relevant to adopt protective behaviours.
In this sense, many studies have focused on the impact of this COVID-19 pandemic on mental health (18,19). Also, previous studies have found that public health emergencies (e.g., 2003 SARS-CoV) triggered a range of emotional stress responses that involved high levels of anxiety and other negative emotions (20). In this line, during the SARS outbreak, higher levels of anxiety were associated with an increased likelihood of using at least five out of seven preventive measures (17). Further, a study developed during the 2009 influenza A (H1N1) pandemic showed how higher anxiety levels were significantly associated with lower use of more appropriate and consistent protective behaviours, but with a higher tendency to disinfect at home (21).
It has been shown that common psychological reactions to health crises are more likely to persist over time (22), and it has been argued that whenever fear or anxiety become chronic or irrational, they play a key role in the development of mental illnesses or psychological disorders such as stress or depression (23). Some research associates the presence of stress in pregnancy with alterations in the functioning of the newborn’s stress regulatory systems (24). Also, women’s experiences of fear of childbirth seemed to be related to their emotional wellbeing, stress symptoms, and impact on daily life. In addition, social circumstances, such as lack of social support, unemployment, and economic problems influence the likelihood of developing fear of childbirth (25,26). In this sense, it is suggested that those women for whom COVID-19 had a greater psychological impact were more likely to suffer from depression, with consequences both in the prenatal and postnatal period (27).
In this context, the aim of this review was to describe the impact of the COVID-19 pandemic on the levels of anxiety and fear in pregnant women, a group of particular vulnerability for the development of mental health problems.
Methods
Research Design
A literature review to assess the mental health of pregnant women during the pandemic was conducted using the systematic review format, following the criteria of the updated PRISMA 2020 (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines (28). The implemented protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO) with code CRD42022355698.
Search Strategy
For the development of the research question, the standardised structure for formulating research questions, PECOT, has been followed (Table 1).
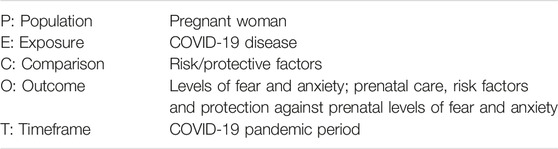
TABLE 1. PECOT format: Keywords (Spain, 2022).
Research Question
How Has COVID-19 Influenced Anxiety and Fear Levels During COVID-19 in Pregnant Women?
The following Medical Subject Headings (MeSH) descriptors were used to create the search string: pregnant woman, pregnancy, COVID-19, anxiety, and fear. In order to expand the search scope, free terms were added to the search using the Boolean operators AND and OR (Table 2).

TABLE 2. Terminology used in the search (MeSH terms) (Spain, 2022).
Table 3 shows the search process that was conducted on 2 September 2022 in the different databases (Pubmed, Scopus, Web of Science, and PsycInfo) using the different search strings and filtering from January 2020 to August 2022.
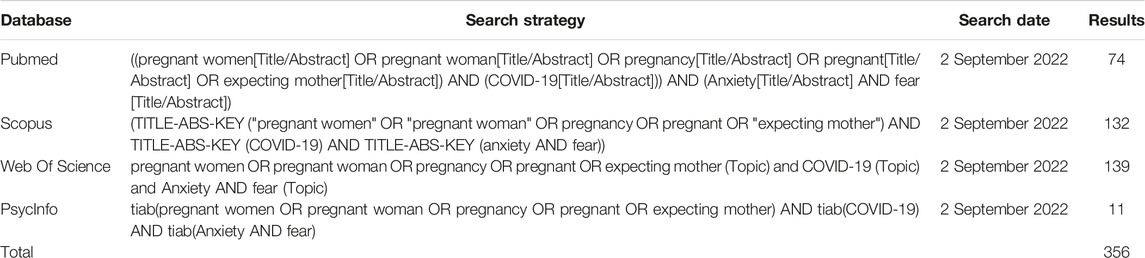
TABLE 3. Search strategy carried out in the different databases (Spain, 2022).
Selection Criteria
The following inclusion and exclusion criteria were used for the selection of articles.
Inclusion Criteria
- Research carried out between January 2020 and August 2022 (COVID-19 pandemic period).
- Type: meta-analysis, descriptive studies, correlational studies, cohort or case-control studies.
- Articles assessing the following indicators: levels of fear, levels of anxiety, comparison of levels of fear or anxiety before vs. during the COVID-19 pandemic, comparison according to prenatal care, risk and protective factors against prenatal levels of fear and anxiety.
Exclusion Criteria
- Articles of low methodological quality after assessment using a quality assessment tool.
- Articles on research involving pregnant women with pre-pregnancy mental illnesses.
- Articles assessing the indicators outlined in the inclusion criteria, but in non-prenatal periods.
Data Collection and Extraction
The search was carried out independently by two reviewers using the agreed descriptors and the combination of the Boolean operators indicated in the search strategy. Subsequently, the articles were read and selected according to the inclusion criteria and applying the exclusion criteria. In case of disagreement over the inclusion of an article between the two co-authors, an online meeting was held with a third independent reviewer and, through a feedback process, a decision was made on whether or not to include the specific article.
Methodological Quality Assessment
The assessment of methodological quality was performed independently by both reviewers using the critical appraisal tool of the Joanna Briggs Institute (JBI) tool for non-randomised studies at the University of Adelaide (29). This tool allows for the assessment of the methodology used in the research by identifying the absence of bias in its design, process, or analysis. In the present review, the version for cross-sectional quantitative studies consisting of eight items was used, and the cut-off point was set by consensus of both researchers at 6/8 to be considered eligible for inclusion.
Results
In the previously mentioned databases and using the search strings in Table 3, a total of 356 articles were identified. After removing duplicate articles (165), a total of 191 articles remained eligible. Then, 113 articles were excluded after reading the title and abstract.
Subsequently, 60 articles were eliminated after reading the full text for different reasons: type of study (n = 10), low methodological quality (n = 15), not related to the objective of the review (n = 18), no or little data analysis (n = 5), the study population was postpartum women (n = 9), no details of the instrument used (n = 1), or full text not available (n = 2). Figure 1 details the process followed for the identification, screening, and selection of the studies included in this review.
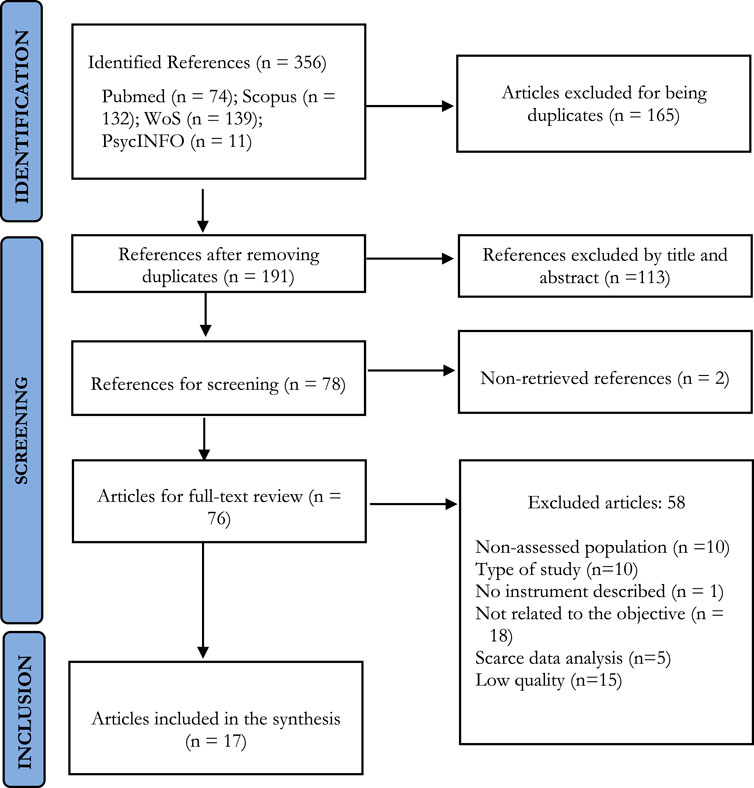
FIGURE 1. Identification of studies via databases (Spain, 2022).
Finally, 17 articles were included in the review (30-46) that measured levels of fear or anxiety in pregnant women during the COVID-19 pandemic.
Main Results
In order to synthesise the articles included in the review, Table 4 has been drawn up to display the main characteristics of the studies, including information on the author(s), location, main objective, type of research, sample, tools used, main results, and methodological quality.
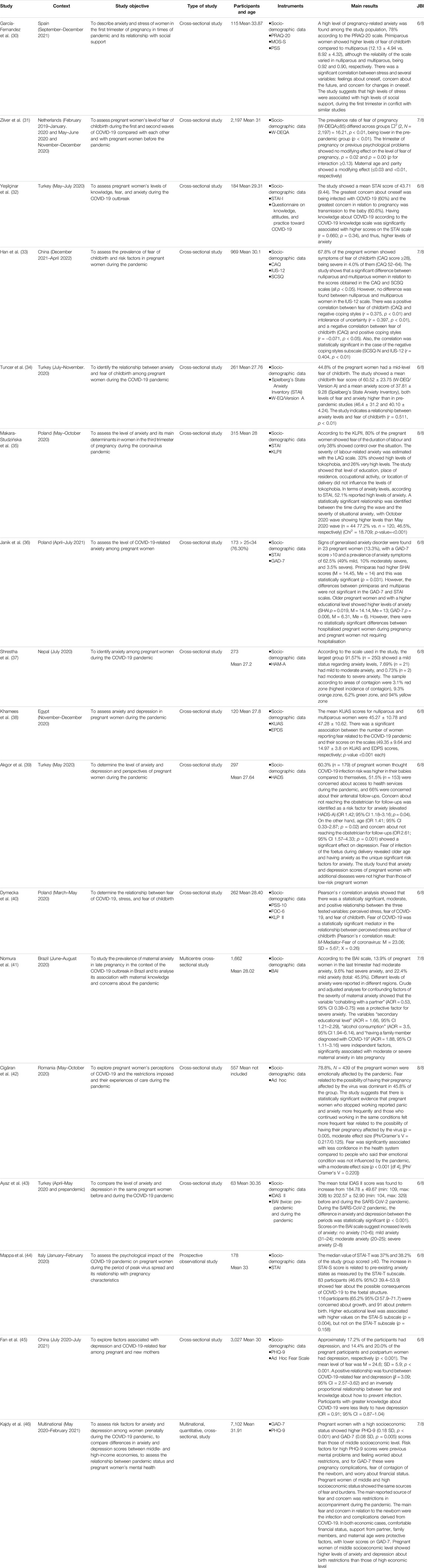
TABLE 4. Characteristics of the studies included in the systematic review (Spain, 2022).
The origins of the different studies were varied: four of them had been carried out in Turkey (32,34,39,43); three in Poland (35,36,40); two in China (33,45); and the following countries were represented with one study each: Spain (30); Romania (42); Brazil (41); Egypt (38); Nepal (37); the Netherlands (31); and Italy (44). Finally, one multinational study was also included (46).
By way of summary, all studies included the pregnant female population in the antenatal period during the COVID-19 pandemic, which is the focus of the present study. However, two of the studies also included women during the pre-pandemic period (31,43) and one study also included women during the postpartum period (45).
Of the total of 17 studies included in the analysis, 15 were quantitative cross-sectional studies (30-45) and 2 were quantitative multicentre cross-sectional studies (41,46).
Assessing the levels of fear and anxiety in pregnant women was the main objective of this review and both variables were identified in 7 (31-34,40,42,45) and 13 (30,32,34-39,41-44,46) studies, respectively. Other factors related to the psychological impact that the COVID-19 pandemic had on the pregnant women were: stress (30,40) or depression (38,39,43,45,46). Both fear and anxiety were assessed using different measurement tools: fear was assessed using, W-DEQ-A (34), FOC-6 (40), and ad hoc Fear scale (42,45). On the other hand, anxiety was assessed with STAI (32,35,36,44), GAD-7 (36,46), PRAQ-20 (30), KLP-II (35,40), HAM-A (37), Kuas, Spielberg’s State Anxiety Inventory (34), HADS (39), BAI (41), and IDAS II (43). Lastly, the PSS (30) and PSS-10 (40) were used to measure stress.
In addition, other factors that were assessed in the different studies required the use of other scales such as the Social Support MOS-S (33), the Questionnaire on Knowledge, Attitude, and Practices toward COVID-19 (32), the CAQ for engaged behaviour (33), the IUS-12 for intolerance of uncertainty (33), the SCS-Q for coping skills (33), the EPDS for postpartum depression (38), and the PHQ-9 for the assessment of depression (45,46).
In relation to the sample collection period, thirteen studies were conducted in 2020 (31–46). Of these, two had also collected data in 2021 (45,46) and one study had collected pre-pandemic period data (43); five studies had collected data during 2021 (30,33,36,45,46) and one study included data from 2022 (33).
After the initial discussion on the inclusion of articles, a consensus was reached on 17 studies. To these, one article was added though doubts arose about its inclusion, leaving the decision to the discretion of a third reviewer. It was finally excluded it as it did not assess fear or anxiety but other mental health disorders.
Among the studies analysed, the methodological and quality assessment showed 11 studies with a score of 6, which was the minimum required in the selection criteria. In addition, 4 studies obtained a score of 7, and 2 studies a maximum score of 8.
Level of Fear
Fear levels in pregnancy have been studied by many researchers in the pre-pandemic period as pregnant women are considered a high-risk vulnerable group compared to a non-pregnant population due to both physical and psychological changes that occur during pregnancy.
However, to date, no clear definition of fear in pregnant women has been identified. Fear of childbirth (FOC) seems to be used as a general term, which has led to considerable heterogeneity around the presence of many types of anxiety and fear among women during pregnancy. Thus, it can be concluded that FOC seems to be an expression for different emotional difficulties during pregnancy or in the postpartum period.
In this context, and given the lack of knowledge about women’s fear of the unpredictability of COVID-19, the unavailability of reliable and valid scales to assess fear in a pandemic context, the lack of specific questions related to fear of COVID-19 in the different scales available and, consequently, the lack of discriminatory properties of these scales, the results of the present study are clinically relevant, as it has been determined to assess the association between the general fear of pregnant women during pregnancy and childbirth and a limited number of variables related to gestation during the COVID-19 pandemic period.
One of the studies, conducted by Zilver et al. (31), showed lower levels of fear of childbirth in the first months of the pandemic compared to the pre-pandemic period. Possible explanations for these results include: the study included only nulliparous women; less stress and pressure on daily life due to the recent implementation of teleworking in the first months of the pandemic; better sleep levels; increased physical exercise; greater family support; optimisation of sleeping hours. However, the other six studies assessing fear in pregnancy during the pandemic (32-34,40,42,45) showed opposing results to the ones found by Zilver et al. (31), but showed similar results among them. Makara-Studzińska et al. (35) suggested that 80% of pregnant women were fearful of the length of labour, and Tuncer et al. (34) indicated that 44.8% of pregnant women had an intermediate level of fear during the pandemic. Khamees et al. (38) indicated that 77.5% of pregnant women thought that the pandemic would be a threat to their health. Cigaran et al. (42) reported that 45% of pregnant women showed fear related to the possibility that the pregnancy would be affected by the coronavirus infection, and the study by Fan et al. (45) reported a prevalence of fear of childbirth during the pandemic of 67.8%, i.e., more than half of the pregnant women had fear of childbirth during the pandemic. In this same study, a prevalence of 67.8% was reported; more than half of the participants indicated that thoughts of COVID-19 frightened them and that they felt nervous when they thought about it (45). Yesilcinar et al. (32) reported, between May and July 2020, that 77.6% of pregnant women had fear of coronavirus transmission and 67.6% stated that the COVID-19 pandemic had had an impact on mental health.
Among the main factors associated with fear during the pandemic, parity stands out, with Han et al. (33) showing that there was a significant difference between nulliparous and multiparous women in levels of fear of pregnancy during the last months of the pandemic, suggesting nulliparity as a main risk factor along with others such as unplanned pregnancy, poor support from partners, negative behaviours, or fear of the unknown. In the same vein, Makara-Studzinska et al. (35) observed that age had an influence on the severity of tokophobia or fear of pregnancy, indicating that older women showed lower levels than younger women. They also suggested that financial status correlated with levels of tokophobia, being higher in women with lower financial status.
Level of Anxiety
Anxiety is defined as an unpleasant and unclear emotional state related to the anticipation of external danger or originating from within the body (35). A total of eight different tools or scales were used to measure anxiety levels in the different studies included in the present review, which may justify the existence of such disparate results due to a bias in their quantification.
Garcia Fernandez et al. (30) found a pregnancy-related anxiety level of 78%, which are very high figures in contrast to other studies, such as the one by Nomura et al. (41) with a sample of 1,662 pregnant women in the last trimester of pregnancy of which 13.9% had moderate anxiety levels and 9.6% had severe anxiety, also reporting different levels of anxiety in different regions. There is, however, a wide variability in the prevalence of anxiety in the different samples of the studies conducted during the COVID-19 pandemic. This could be explained by the different phases through which the pandemic has evolved, by the impact of different disease control and prevention measures in each region, by the differences in anxiety levels in the phases of the gestational period, or by the different pre-existing anxiety levels between nulliparous and multiparous women. In fact, Nomura et al. (41), as well as Garcia Fernandez et al. (30), with a sample of 1,662 and according to the BAI scale, found different levels of anxiety in different regions of Brazil. Janik et al. (36) found a prevalence in anxiety symptoms of 62.5% in the months of April to July 2021 and primiparous obtained higher scores in the SHAI scale, being statistically significant (p = 0.031). Makara-Studzinska et al. (35), between May and October 2020, identified a statistically significant influence of the time during the wave on the severity of situational anxiety, with the October 2020 wave yielding higher levels of anxiety than the May 2020 wave.
Along these lines, the different studies included in the review have identified a series of factors associated with higher levels of anxiety: parity, training or educational level, maternal age 4,036, greater knowledge about COVID-19 (32), concern about maintaining follow-up of the pregnancy (39), loneliness or lack of a companion during pregnancy, alcohol consumption, and having a relative diagnosed with COVID-19 (41). All these risk factors have increased anxiety levels during the pandemic and there is no doubt that pregnant women have a series of needs in terms of information, family, and work based on their own personal or health characteristics, needs which are increased by pandemic situations and that can affect the wellbeing of both the woman and the foetus. In this sense, Cigaran et al. (42) reported that 78% of pregnant women were emotionally affected by the pandemic. Fear related to the possibility of the pregnancy being affected by the virus was dominant in 45.8% of pregnant women, and women who stopped working reported panic and anxiety more frequently than those who continued working under the same conditions, with this difference being statistically significant. The most common personal concern related to the pandemic was risk to the foetus (39), and it was identified that concern about maintaining antenatal follow-up was a risk factor for both anxiety and depression.
While some factors were shown to predispose to increased levels of fear or anxiety in pregnant women, there are other factors that may be considered protective, such as living with a partner (41), having a comfortable financial status, family support, or maternal age (46).
Discussion
Through the present review, levels of fear and anxiety in pregnant women during the COVID-19 pandemic have been made visible and possible risk or resilience factors have been identified.
The analysed studies showed a high prevalence of fear levels, with between 44.8% and 80% of pregnant women showing intermediate to high levels of fear during the COVID-19 pandemic. The manifestation of fear levels is common during pregnancy, with women experiencing some level of fear during pregnancy and in the postpartum period, around 14% according to some pre-pandemic studies (39,47). Thus, the impact of the global COVID-19 pandemic has clearly contributed to higher levels of fear (31,34,48) despite the different characteristics of the studied populations: gestational age, regions, maternal age, parity, the use of different measurement tools and study methods, problems with definitions of fear in pregnant women, or even the different phases of the pandemic from its onset in late 2019 to the present day when, for different reasons, this disease is already part of our lives. These are some of the factors that may have influenced the wide variability in the prevalence of gestational fear during the pandemic.
According to a systematic review, the prevalence of fear in pregnancy was 14% before the pandemic (47), and other studies correlated mild and high levels of fear of childbirth with prolonged labour, caesarean section, increased use of epidural analgesia, antenatal and postpartum depression, or axiety (49-53). The fear of being infected by a virus whose consequences were scientifically unknown or without a specific treatment, together with social distancing as the main measure to avoid spread of the virus, contributed to social isolation, isolation from other family members, from friends, from work colleagues, or from the health system itself. In this line, a series of factors associated with higher levels of fear have been identified in the analysed studies, such as nulliparity (30,31,46), unplanned pregnancy, poor support from partners (46), maternal age (31,46), financial status (46), or negative behaviours (33). All of these risk factors have increased their impact during the COVID-19 epidemic and, as reported by Cigăran et al. (42), in 45.8% of women fear is related to the possibility of the pregnancy being affected by the virus.
There are a number of factors with no clear evidence of a modifying effect. Pregnancy trimester or gestational age, educational level, place of residence, professional activity, or place of maternity care do not appear to influence the levels of fear (31,35). In relation to whether educational level may affect the prevalence of fear, the study by Makara-Studzińska et al. (35) in Poland showed no modifying effect in this regard. However, Fan et al. (45) in China reported that knowledge about infection prevention was statistically significantly associated with lower levels of fear, with the level of knowledge reported by the sample being moderate. Also, the study by Yeşilçinar et al. (32) stated that having greater knowledge about COVID-19 resulted in higher levels of anxiety. These, a priori, contradictory results may be due to the different behaviour of pregnant women in relation to the assimilation of information, or availability of it. Fan et al. (45) also associated higher COVID-19 knowledge with lower likelihood of depression, which allowed them to positively link fear with depression.
With regard to anxiety, the present study aimed at assessing the levels of anxiety in pregnant women and also the factors that may protect or predispose this population to anxiety during pregnancy. This was done given the consequences that such a psychological state may have for gestation in terms of threat of preterm birth, low birth weight, neurodevelopmental abnormalities, depression, nausea or vomiting during pregnancy, or low Apgar scores (39,54-56).
According to the reviewed literature, anxiety levels during the pandemic in pregnant women ranged from 45.9% (41) to 62% (30,36). Therefore, around two-thirds of pregnant women showed signs of anxiety, an increase of between 30% and 37% (57,58) in anxiety levels in relation to pre-pandemic studies. Despite the use of different tools in the measurement of anxiety levels, all of them reported higher scores than pre-pandemic studies (30, 32-38). Dagklis et al. (59), during confinement and using the Greek version of the State-Trait Anxiety Inventory, reported a prevalence of anxiety states of 34.2%, indicating a significant increase in anxiety levels during confinement (p < 0.001). At the same time, this study reported differences between the three trimesters of pregnancy and higher anxiety levels in the first week of quarantine, which gradually decreased in the second week and reached almost normal levels in the third week (59). Similar data were provided by the study conducted by Mappa et al. (44) in Italy days before the total closure decreed by the Italian government during March 2020. In both studies, there was a positive linear correlation between STAI-T and STAI-S, which may indicate that levels of anxiety in pregnancy are related to pre-existing levels of anxiety, in line with studies that determined an altered mental health status as the main risk factor for increased anxiety levels (44,60,61).
The work in Poland by Makara-Studzińska et al. (35) reported elevated anxiety levels in 52% of pregnant women and related the severity of anxiety to the time during the wave. In this regard, only the study in Brazil by Nomura et al. (51) reported different levels of anxiety in different regions, which, on the other hand, could be due to the different phases of the pandemic in a country as large as Brazil or to differences in financial status in a country with such economic inequality. Thus, Kajdy et al. (46) in an international multicentre study, identified financial status concern as a risk factor for high GAD-7 scores, but also identified a number of protective factors with lower GAD-7 scores, such as partner support, support from family members, older maternal age, or comfortable financial status.
Khamees et al. (38) in Egypt reported similar levels of anxiety between nulliparous and multiparous women, 45.27% vs. 47.28%. In this sense, there is controversy about the higher or lower levels of anxiety among nulliparous versus multiparous pregnant women. Some studies have found no statistically significant differences according to the number of pregnancies in the context of the COVID-19 pandemic. However, an association has been found between anxiety and educational level (36), which may be due to the greater awareness of older mothers of the threats of a disease with so much clinical variability. In relation to gestational age, contrary to what might be thought, the included studies have not shown statistically significant differences. The results in this sense have been contradictory in pre-pandemic periods, as some authors had reported higher levels in the first and third trimester (62), yet another study reported similar levels of anxiety (63).
Finally, there are a number of factors such as unplanned pregnancy, poor spousal support, negative behaviours, intolerance to the unknown, age, or financial status that act as risk factors for fear levels. In relation to anxiety, maternal age, social support, financial status, having a family member diagnosed with COVID-19, educational level, knowledge of COVID-19, or concern about maintaining prenatal consultations have been identified as risk factors for higher levels of anxiety.
Some of the limitations and weaknesses to be taken into account when interpreting the results of this study are as follows: very heterogeneous measurement tools were used, and all the included studies were cross-sectional; the characteristics of the population in terms of obstetrics (high or low risk) were not defined in the analysed studies; the lack of standardised scales for pregnant women during the 2020–2022 pandemic; and the samples were mostly collected online and in very heterogeneous periods from a pandemic context point of view.
Conclusion
Based on the reviewed research, it can be concluded that the COVID-19 pandemic has had an impact on the mental health of pregnant women through increased levels of fear and anxiety. The analysed studies show a statistically significant relationship between levels of fear and anxiety in pregnant women during the pandemic.
Finally, based on the reviewed literature, it has not been possible to establish a relationship between significant factors such as gestational age, measures to control the health emergency, or difficulty of access to health services and high levels of fear or anxiety. There is a high degree of heterogeneity of risk factors, which points to the need for better observational research. In this sense, further research is needed to assess levels based on these factors in order to be able to define an association and try to avoid bias in the analyses. With the clear objective of minimising anxiety and fear in a period of special vulnerability, further study of predisposing or protective factors in contexts of special difficulty is needed.
Author Contributions
Conceptualization, FM-V, LR-D, JG-S, FF-C, RA-C, JV-L, and JF-R; Data curation, FM-V, LR-D, and JV-L; Formal analysis, FM-V, LR-D, JG-S, FF-C, RA-C, JV-L, and JFR; Investigation, FM-V, LR-D, JG-S, FF-C, RA-C, JV-L, and JF-R; Methodology, FM-V, LR-D, JG-S, FF-C, RA-C, JV-L, and JF-R; Project administration, FM-V, LR-D, and JV-L; Resources, FM-V, LR-D, JG-S, FF-C, RA-C, JV-L, and JF-R; Software, FM-V, LR-D, JG-S, FF-C, RA-C, JV-L, and JF-R; Supervision, FM-V, LR-D, and JV-L; Validation, FM-V, LR-D, JG-S, FF-C, RA-C, JV-L, and JF-R; Visualization, FM-V, LR-D, JG-S, FF-C, RA-C, JV-L, and JF-R; Writing—original draft, FM-V, LR-D, JG-S, FF-C, RA-C, JV-L, and JF-R; Writing—review and editing, FM-V, LR-D, JG-S, FF-C, RA-C, JV-L, and JF-R. All the authors have intellectually contributed to the work, met the conditions of authorship, and approved its final version.
Conflict of Interest
The authors declare that they do not have any conflicts of interest.
References
1. Afonso, P. O Impacto da Pandemia COVID-19 na Saúde Mental. Acta Med Port (2020) 33(5):356–7. doi:10.20344/AMP.13877
2. Du, RH, Liang, LR, Yang, CQ, Wang, W, Cao, TZ, Li, M, et al. Predictors of Mortality for Patients with COVID-19 Pneumonia Caused by SARS-CoV-2: a Prospective Cohort Study. Eur Respir J (2020) 55(5):2000524. doi:10.1183/13993003.00524-2020
3. Amerio, A, Aguglia, A, Odone, A, Gianfredi, V, Serafini, G, Signorelli, C, et al. Covid-19 Pandemic Impact on Mental Health of Vulnerable Populations. Acta bio-medica: Atenei Parmensis (2020) 91(9-S):95–6. doi:10.23750/abm.v91i9-S.10112
4. Ho, CS, Chee, CY, and Ho, RC. Mental Health Strategies to Combat the Psychological Impact of Coronavirus Disease 2019 (COVID-19) beyond Paranoia and Panic. Ann Acad Med Singapore (2020) 49(3):155–60. doi:10.47102/annals-acadmedsg.202043
5. García-Iglesias, J, Gómez-Salgado, J, Martín-Pereira, J, Fagundo-Rivera, J, Ayuso-Murillo, D, Martínez-Riera, JR, et al. Impacto del SARS-CoV-2 (Covid-19) en la salud mental de los profesionales sanitarios: una revisión sistemática. Rev Esp Salud Publica (2020) 94(1):e1–e20. Available: https://medes.com/publication/152295 (Accessed Oct 03, 2022).
6. Liu, H, Wang, LL, Zhao, SJ, Kwak-Kim, J, Mor, G, and Liao, AH. Why Are Pregnant Women Susceptible to COVID-19? an Immunological Viewpoint. J Reprod Immunol (2020) 139:103122. doi:10.1016/j.jri.2020.103122
7. Longman, RE, and Johnson, TRB. Viral Respiratory Disease in Pregnancy. Curr Opin Obstet Gynecol (2007) 19(2):120–5. doi:10.1097/GCO.0B013E328028FDC7
8. Qiao, J. What Are the Risks of COVID-19 Infection in Pregnant Women? The Lancet (2020) 395(10226):760–2. doi:10.1016/S0140-6736(20)30365-2
9. Rodríguez-Blanco, N, Vegara-Lopez, I, Aleo-Giner, L, and Tuells, G. Scoping Review of Coronavirus Case Series (SARS-CoV, MERS-CoV and SARS-CoV-2) and Their Obstetric and Neonatal Results. Revista Española de Quimioterapia (2020) 33(5):313–26. doi:10.37201/REQ/064.2020
10. Schwartz, DA, and Graham, AL. Potential Maternal and Infant Outcomes from (Wuhan) Coronavirus 2019-nCoV Infecting Pregnant Women: Lessons from SARS, MERS, and Other Human Coronavirus Infections. Viruses (2020) 12(2):194. doi:10.3390/V12020194
11. DeBolt, CA, Bianco, A, Limaye, MA, Silverstein, J, Penfield, CA, Roman, AS, et al. Pregnant Women with Severe or Critical Coronavirus Disease 2019 Have Increased Composite Morbidity Compared with Nonpregnant Matched Controls. Am J Obstet Gynecol (2021) 224(5):510.e1–10.e12. doi:10.1016/J.AJOG.2020.11.022
12. Martinez-Portilla, RJ, Sotiriadis, A, Chatzakis, C, Torres-Torres, J, Espino y Sosa, S, Sandoval-Mandujano, K, et al. Pregnant Women with SARS-CoV-2 Infection Are at Higher Risk of Death and Pneumonia: Propensity Score Matched Analysis of a Nationwide Prospective Cohort (COV19Mx). Ultrasound Obstet Gynecol (2021) 57(2):224–31. doi:10.1002/UOG.23575
13. Schaller, M. The Behavioural Immune System and the Psychology of Human Sociality. Philosophical Trans R Soc B: Biol Sci (2011) 366(1583):3418–26. doi:10.1098/RSTB.2011.0029
14. Karimi-Zarchi, M, Neamatzadeh, H, Dastgheib, SA, Abbasi, H, Mirjalili, SR, Behforouz, A, et al. Vertical Transmission of Coronavirus Disease 19 (COVID-19) from Infected Pregnant Mothers to Neonates: A Review. Fetal Pediatr Pathol (2020) 39(3):246–50. doi:10.1080/15513815.2020.1747120
15. Kotlyar, AM, Grechukhina, O, Chen, A, Popkhadze, S, Grimshaw, A, Tal, O, et al. Vertical Transmission of Coronavirus Disease 2019: a Systematic Review and Meta-Analysis. Am J Obstet Gynecol (2021) 224(1):35–53.e3. doi:10.1016/J.AJOG.2020.07.049
16. Mullins, E, Hudak, ML, Banerjee, J, Getzlaff, T, Townson, J, Barnette, K, et al. Pregnancy and Neonatal Outcomes of COVID-19: Coreporting of Common Outcomes from PAN-COVID and AAP-SONPM Registries. Ultrasound Obstet Gynecol (2021) 57(4):573–81. doi:10.1002/UOG.23619
17. Villar, J, Ariff, S, Gunier, RB, Thiruvengadam, R, Rauch, S, Kholin, A, et al. Maternal and Neonatal Morbidity and Mortality Among Pregnant Women with and without COVID-19 Infection: The INTERCOVID Multinational Cohort Study. JAMA Pediatr (2021) 175(8):817–26. doi:10.1001/JAMAPEDIATRICS.2021.1050
18. Li, S, Wang, Y, Xue, J, Zhao, N, and Zhu, T. The Impact of COVID-19 Epidemic Declaration on Psychological Consequences: A Study on Active Weibo Users. Int J Environ Res Public Health (2020) 17(6):2032. doi:10.3390/ijerph17062032
19. Bhattacharjee, A, and Ghosh, T. COVID-19 Pandemic and Stress: Coping with the New Normal. J Prev Health Promot (2022) 3(1):30–52. doi:10.1177/26320770211050058
20. Sattari, M, Bashirian, S, Masoumi, SZ, Shayan, A, Jenabi, E, Ghelichkhani, S, et al. Evaluating Clinical Course and Risk Factors of Infection and Demographic Characteristics of Pregnant Women with COVID-19 in Hamadan Province, West of Iran. J Res Health Sci (2020) 20(3):e00488. doi:10.34172/JRHS.2020.22
21. McAlonan, GM, Lee, AM, Cheung, V, Cheung, C, Tsang, KW, Sham, PC, et al. Immediate and Sustained Psychological Impact of an Emerging Infectious Disease Outbreak on Health Care Workers. Can J Psychiatry (2007) 52(4):241–7. doi:10.1177/070674370705200406
22. Leung, GM, Lam, TH, Ho, LM, Ho, SY, Chan, BH, Wong, IO, et al. The Impact of Community Psychological Responses on Outbreak Control for Severe Acute Respiratory Syndrome in Hong Kong. J Epidemiol Community Health (2003) 57(11):857–63. doi:10.1136/jech.57.11.857
23. Leung, GM, Ho, LM, Chan, SK, Ho, SY, Bacon-Shone, J, Choy, RY, et al. Longitudinal Assessment of Community Psychobehavioral Responses during and after the 2003 Outbreak of Severe Acute Respiratory Syndrome in Hong Kong. Clin Infect Dis (2005) 40(12):1713–20. doi:10.1086/429923
24. Cowling, BJ, Ng, DM, Ip, DK, Liao, Q, Lam, WW, Wu, JT, et al. Community Psychological and Behavioral Responses through the First Wave of the 2009 Influenza A(H1N1) Pandemic in Hong Kong. J Infect Dis (2010) 202(6):867–76. doi:10.1086/655811
25. Rúger-Navarrete, A, Vázquez-Lara, JM, Antúnez-Calvente, I, Rodríguez-Díaz, L, Riesco-González, FJ, Palomo-Gómez, R, et al. Antenatal Fear of Childbirth as a Risk Factor for a Bad Childbirth Experience. Healthcare (2023) 11:297. doi:10.3390/healthcare11030297
26. Lu, W, Wang, H, Lin, Y, and Li, L. Psychological Status of Medical Workforce during the COVID-19 Pandemic: A Cross-Sectional Study. Psychiatry Res (2020) 288:112936. doi:10.1016/j.psychres.2020.112936
27. Rogers, JP, Chesney, E, Oliver, D, Pollak, TA, McGuire, P, Fusar-Poli, P, et al. Psychiatric and Neuropsychiatric Presentations Associated with Severe Coronavirus Infections: a Systematic Review and Meta-Analysis with Comparison to the COVID-19 Pandemic. The Lancet Psychiatry (2020) 7(7):611–27. doi:10.1016/S2215-0366(20)30203-0
28. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 Statement: an Updated Guideline for Reporting Systematic Reviews. BMJ (2021). 372. 71. doi:10.1136/bmj.n71
29.E Aromataris, and Z Munn, editors. JBI Manual for Evidence Synthesis. Adelaide: Australia: Joanna Briggs Institute (2020). doi:10.46658/JBIMES-20-01
30. García-Fernández, R, Liébana-Presa, C, Marqués-Sánchez, P, Martínez-Fernández, MC, Calvo-Ayuso, N, and Hidalgo-Lopezosa, P. Anxiety, Stress, and Social Support in Pregnant Women in the Province of Leon during COVID-19 Disease. Healthcare (Basel, Switzerland) (2022) 10(5):791. doi:10.3390/healthcare10050791
31. Zilver, S, Hendrix, Y, Broekman, B, de Leeuw, RA, de Groot, C, and van Pampus, MG. Fear of Childbirth in Pregnancy Was Not Increased during the COVID-19 Pandemic in the Netherlands: a Cross-Sectional Study. Acta Obstetricia Gynecologica Scand (2022) 101(10):1129–34. doi:10.1111/aogs.14409
32. Yeşilçinar, İ, Güvenç, G, Kinci, MF, Bektaş Pardes, B, Kök, G, and Sivaslioğlu, AA. Knowledge, Fear, and Anxiety Levels Among Pregnant Women during the COVID-19 Pandemic: A Cross-Sectional Study. Clin Nurs Res (2022) 31(4):758–65. doi:10.1177/10547738221085662
33. Han, L, Bai, H, Lun, B, Li, Y, Wang, Y, and Ni, Q. The Prevalence of Fear of Childbirth and its Association with Intolerance of Uncertainty and Coping Styles Among Pregnant Chinese Women during the COVID-19 Pandemic. Front Psychiatry (2022) 13:935760. doi:10.3389/fpsyt.2022.935760
34. Tuncer, SK, Alp Yılmaz, F, Karakurt, P, and Yıldız Çiltaş, N. The Relationship between the Fear of Childbirth and Anxiety during the Covid-19 Pandemic. Galician Med J (2022) 29(2):E202222. doi:10.21802/gmj.2022.2.2
35. Makara-Studzińska, M, Zaręba, K, Kawa, N, and Matuszyk, D. Tokophobia and Anxiety in Pregnant Women during the SARS-CoV-2 Pandemic in Poland-A Prospective Cross-Sectional Study. Int J Environ Res Public Health (2022) 19(2):714. doi:10.3390/ijerph19020714
36. Janik, K, Cwalina, U, Iwanowicz-Palus, G, and Cybulski, M. An Assessment of the Level of COVID-19 Anxiety Among Pregnant Women in Poland: A Cross-Sectional Study. J Clin Med (2021) 10(24):5869. doi:10.3390/jcm10245869
37. Shrestha, D, Saha, R, Manandhar, N, Adhikari, A, and Dahal, J. Anxiety Among Pregnant Women about Corona Virus Infections during COVID-19 Pandemic at a Tertiary Care Center in Nepal: A Descriptive Cross-Sectional Study. J Nepal Med Assoc (2021) 59(234):152–5. doi:10.31729/jnma.5377
38. Khamees, RE, Taha, OT, and Ali, T. Anxiety and Depression during Pregnancy in the Era of COVID-19. J Perinatal Med (2021) 49(6):674–7. doi:10.1515/jpm-2021-0181
39. Akgor, U, Fadıloglu, E, Soyak, B, Unal, C, Cagan, M, Temiz, BE, et al. Anxiety, Depression and Concerns of Pregnant Women during the COVID-19 Pandemic. Arch Gynecol Obstet (2021) 304(1):125–30. doi:10.1007/s00404-020-05944-1
40. Dymecka, J, Gerymski, R, Iszczuk, A, and Bidzan, M. Fear of Coronavirus, Stress and Fear of Childbirth in Polish Pregnant Women during the COVID-19 Pandemic. Int J Environ Res Public Health (2021) 18(24):13111. doi:10.3390/ijerph182413111
41. Nomura, R, Tavares, I, Ubinha, AC, Costa, ML, Opperman, ML, Brock, M, et al. Impact of the COVID-19 Pandemic on Maternal Anxiety in Brazil. J Clin Med (2021) 10(4):620. doi:10.3390/jcm10040620
42. Cigăran, RG, Botezatu, R, Mînecan, EM, Gică, C, Panaitescu, AM, Peltecu, G, et al. The Psychological Impact of the COVID-19 Pandemic on Pregnant Women. Healthcare (Basel, Switzerland) (2021) 9(6):725. doi:10.3390/healthcare9060725
43. Ayaz, R, Hocaoğlu, M, Günay, T, Yardımcı, OD, Turgut, A, and Karateke, A. Anxiety and Depression Symptoms in the Same Pregnant Women before and during the COVID-19 Pandemic. J Perinatal Med (2020) 48(9):965–70. doi:10.1515/jpm-2020-0380
44. Mappa, I, Distefano, FA, and Rizzo, G. Effects of Coronavirus 19 Pandemic on Maternal Anxiety during Pregnancy: a Prospectic Observational Study. J Perinatal Med (2020) 48(6):545–50. doi:10.1515/jpm-2020-0182
45. Fan, H, Choi, E, Ko, R, Kwok, J, Wong, J, Fong, D, et al. COVID-19 Related Fear and Depression of Pregnant Women and New Mothers. Public Health Nurs (Boston, Mass.) (2022) 39(3):562–71. doi:10.1111/phn.13035
46. Kajdy, A, Sys, D, Pokropek, A, Shaw, SW, Chang, TY, Calda, P, et al. Risk Factors for Anxiety and Depression Among Pregnant Women during the COVID-19 Pandemic: Results of a Web-Based Multinational Cross-Sectional Study. Int J Gynaecol Obstet (2022) 160:167–86. doi:10.1002/ijgo.14388
47. O'Connell, MA, Leahy-Warren, P, Khashan, AS, Kenny, LC, and O'Neill, SM. Worldwide Prevalence of Tocophobia in Pregnant Women: Systematic Review and Meta-Analysis. Acta Obstetricia Gynecologica Scand (2017) 96(8):907–20. doi:10.1111/aogs.13138
48. Lebel, C, MacKinnon, A, Bagshawe, M, Tomfohr-Madsen, L, and Giesbrecht, G. Elevated Depression and Anxiety Symptoms Among Pregnant Individuals during the COVID-19 Pandemic. J Affective Disord (2020) 277:5–13. doi:10.1016/j.jad.2020.07.126
49. Sitras, V, Šaltytė Benth, J, and Eberhard-Gran, M. Obstetric and Psychological Characteristics of Women Choosing Epidural Analgesia during Labour: A Cohort Study. Plos One (2017) 12(10):e0186564. doi:10.1371/journal.pone.0186564
50. Lukasse, M, Schroll, AM, Karro, H, Schei, B, Steingrimsdottir, T, Van Parys, AS, et al. Prevalence of Experienced Abuse in Healthcare and Associated Obstetric Characteristics in Six European Countries. Acta Obstetricia Gynecologica Scand (2015) 94(5):508–17. doi:10.1111/aogs.12593
51. Lara-Cinisomo, S, Zhu, K, Fei, K, Bu, Y, Weston, AP, and Ravat, U. Traumatic Events: Exploring Associations with Maternal Depression, Infant Bonding, and Oxytocin in Latina Mothers. BMC Women's Health (2018) 18(1):31. doi:10.1186/s12905-018-0520-5
52. Sheen, K, and Slade, P. Examining the Content and Moderators of Women's Fears for Giving Birth: A Meta-Synthesis. J Clin Nurs (2018) 27(13-14):2523–35. doi:10.1111/jocn.14219
53. Dencker, A, Nilsson, C, Begley, C, Jangsten, E, Mollberg, M, Patel, H, et al. Causes and Outcomes in Studies of Fear of Childbirth: A Systematic Review. Women And Birth (2019) 32(2):99–111. doi:10.1016/j.wombi.2018.07.004
54. Misri, S, Abizadeh, J, Sanders, S, and Swift, E. Perinatal Generalized Anxiety Disorder: Assessment and Treatment. J Women's Health (2015) 24(9):762–70. doi:10.1089/jwh.2014.5150
55. Durankuş, F, and Aksu, E. Effects of the COVID-19 Pandemic on Anxiety and Depressive Symptoms in Pregnant Women: a Preliminary Study. J Maternal-Fetal Neonatal Med (2022) 35(2):205–11. doi:10.1080/14767058.2020.1763946
56. Mahase, E. China Coronavirus: WHO Declares International Emergency as Death Toll Exceeds 200. BMJ (2020) 368:m408. doi:10.1136/bmj.m408
57. Dennis, CL, Falah-Hassani, K, and Shiri, R. Prevalence of Antenatal and Postnatal Anxiety: Systematic Review and Meta-Analysis. Br J Psychiatry (2017) 210(5):315–23. doi:10.1192/bjp.bp.116.187179
58. Cella, D, Choi, SW, Condon, DM, Schalet, B, Hays, RD, Rothrock, NE, et al. PROMIS® Adult Health Profiles: Efficient Short-form Measures of Seven Health Domains. Value In Health (2019) 22(5):537–44. doi:10.1016/j.jval.2019.02.004
59. Dagklis, T, Tsakiridis, I, Mamopoulos, A, Athanasiadis, AP, and Papazisis, G. Anxiety during Pregnancy in the Era of the COVID-19 Pandemic. SSRN Electron J (2020). doi:10.2139/SSRN.3588542
60. Liu, CH, Erdei, C, and Mittal, L. Risk Factors for Depression, Anxiety, and PTSD Symptoms in Perinatal Women during the COVID-19 Pandemic. Psychiatry Res (2021) 295:113552. doi:10.1016/j.psychres.2020.113552
61. Asmundson, G, Paluszek, MM, Landry, CA, Rachor, GS, McKay, D, and Taylor, S. Do pre-existing Anxiety-Related and Mood Disorders Differentially Impact COVID-19 Stress Responses and Coping? J Anxiety Disord (2020) 74:102271. doi:10.1016/j.janxdis.2020.102271
62. Da Costa, D, Larouche, J, Dritsa, M, and Brender, W. Variations in Stress Levels over the Course of Pregnancy: Factors Associated with Elevated Hassles, State Anxiety and Pregnancy-specific Stress. J Psychosomatic Res (1999) 47(6):609–21. doi:10.1016/s0022-3999(99)00064-1
Keywords: anxiety, mental health, COVID-19, pregnant women, fear of childbirth
Citation: Muñoz-Vela FJ, Rodríguez-Díaz L, Gómez-Salgado J, Fernández-Carrasco FJ, Allande-Cussó R, Vázquez-Lara JM and Fagundo-Rivera J (2023) Fear and Anxiety in Pregnant Women During the COVID-19 Pandemic: A Systematic Review. Int J Public Health 68:1605587. doi: 10.3389/ijph.2023.1605587
Received: 13 November 2022; Accepted: 13 February 2023;
Published: 24 February 2023.
Edited by:
Nino Kuenzli, Swiss School of Public Health (SSPH+), SwitzerlandReviewed by:
Zuzana Skodova, Comenius University, SlovakiaSecil Ozkan, Gazi University, Türkiye
Maria Do Rosário Martins, Instituto Politécnico de Viana do Castelo, Portugal
Copyright © 2023 Muñoz-Vela, Rodríguez-Díaz, Gómez-Salgado, Fernández-Carrasco, Allande-Cussó, Vázquez-Lara and Fagundo-Rivera. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Juan Gómez-Salgado, amdzYWxnYWRAZ21haWwuY29t