 Petr Michenka
Petr Michenka Lydie Fialová2
Lydie Fialová2 Lenka Šlegerová
Lenka Šlegerová- 1Third Faculty of Medicine, Charles University, Prague, Czechia
- 2Independent Researcher, Aberfeldy, United Kingdom
- 3Institute of Economic Studies, Faculty of Social Sciences, Charles University, Prague, Czechia
Objectives: Medical students in the Czech Republic were mandated by the law to take part in the COVID-19 pandemic response in order to expand healthcare capacity. Our study aimed to analyze student’s competencies defined in the legislation and compare them with competencies assigned to them in clinical settings during their deployment.
Methods: Online survey with statistical analysis of collected data.
Results: The survey was completed by 997 respondents. A major convergence between the system of credentials defined in the legal framework and the competencies that students performed were identified.
Conclusion: Medical students represented a valuable resource for addressing shortages of qualified healthcare staff in critical situation. However, the system of competencies and credentials must be aligned with the educational framework to clearly define acquisition of competencies during the course of medical studies and the legal framework regulating students’ deployment must ensure consistency of actual and formal competencies in order to guarantee high standards of care and safety of the patients.
Introduction
The pandemic situation represents serious strain on public health systems and requires increase in capacity as well as expansion of workforce in order to address healthcare needs of the population. In response to the COVID-19 (SARS-CoV2) pandemics, the discussion about the possibilities and limitations of employing medical students opened in many countries worldwide [1–4]. Although medical students had helped to tackle serious public health threats of the past, such as war or epidemics [5, 6], their role within healthcare systems in the times of crises and emergencies has rarely been addressed in practical, organizational, and legal terms as part of national emergency and pandemic preparedness plans. The aim of our study was to analyze the involvement of medical students in the pandemic response in the Czech Republic, focusing on the tension between the competencies and credentials of medical students and their assigned tasks in the clinical care during the pandemic response.
In the Czech Republic, the lack of qualified workers needed for effective pandemic response was most acutely experienced on the level of nursing care. This was caused by a combination of factors, such as increased hospital capacity demands, quarantine and isolation rules, government restrictions etc. [7]. Moreover, the altered spectrum of conditions of patients hospitalized during the pandemic—the provision of elective medical care was reduced and even canceled entirelym–have likely impacted the scope of competencies required to address patients’ needs.
To alleviate this problem the government declared the State of Emergency [8] which allowed for – and legitimized—the introduction of legally mandated “work obligation” for students of medical and nursing programmes [9]. In the history of the Czech Republic this was the first time the work obligation was applied selectively on one group of citizens for extended period of time. Previously, the work obligation was only activated during the massive flood events [10, 11].
The purpose of this crisis management tool was to rapidly mobilize qualified citizens to serve public good. There was a strong correlation between the timing of the work obligation and the development of the pandemic in the Czech Republic, especially over the first year of the pandemic (March 2020–March 2021) (Figure 1). The involvement of students during other periods of the pandemic was on a voluntary basis. Intensity of this deployment varied based on regional needs during the pandemic.
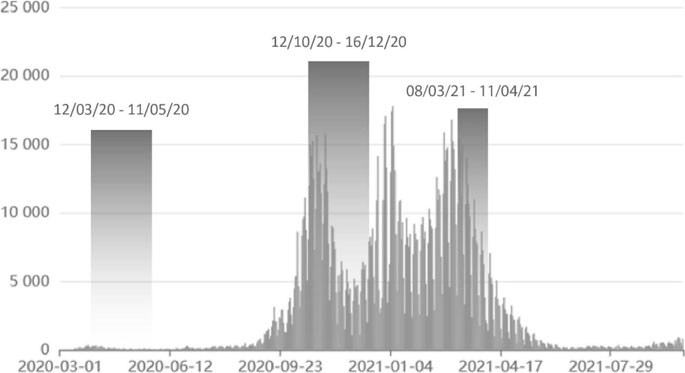
FIGURE 1. The timeline of COVID pandemic and the duration of the work obligation for medical students in the Czech Republic (Prague, Czechia. 2022, data: uzis.cz).
While coping with increased numbers of patients, increased workload, limited resources, especially of nursing staff and creation of new working positions, healthcare facilities appreciated the help of medical students filling newly emerged workforce gap. According to the participating medical faculties, medical students were involved in the following areas:
• Standard healthcare positions—hospital orderly, medical care assistant, nursing aid
• Newly established healthcare positions—triage, swab testing, vaccination assistant, etc.
• Administrative positions—medical storekeeper, swab system management, helpline operator, etc.
• Supporting positions—babysitter for children of hospital staff
In this situation there was a hypothesis regarding a discrepancy between the formal credentialing system defined in the national legislation (in effect from 2004 to January 2021) and competencies assigned to medical students during their involvement in provision of care. Our study, unique in its scope and content, was primarily focused on gathering data on the forms and extent of involvement of medical students in clinical care during the pandemic response in 2020–2021, and on surveying both positive and negative effects of their involvement. Based on the results and areas of concern identified through our research, we discuss the potential and limitations of deploying medical students in crisis situations and on the practical, organizational, and legal implications of such involvement for healthcare system and medical education.
The Organization of Medical Education and Credentials of Medical Students
Czech Republic is a Central European country with 10.702 942 inhabitants [12]. There are eight medical schools of four public and one state university, offering 6-year study programmes, and there are approximately 1865 graduates annually (i.e., 17.425 medical graduates per 100,000 inhabitants) [13]. The General Medicine programme is organized in preclinical section (years 1–3) and clinical section (years 4–6), with a minimum teaching time of 5500 h, awarding M.D. title (MUDr.) upon its completion.
Czech General Medicine curriculum is defined in the national legislation [14] and is in concordance with European framework [15]. It is accredited by the national authority, the National Accreditation Bureau for Higher Education [16], following standards of the European Association for Quality Assurance in Higher Education. The degree is recognized internationally, matching the European Qualifications Framework level 7 [17].
In order to qualify for any healthcare position, the acquisition of clinical skills and competencies must be confirmed by legally specified credentials issued by an educational institution [18]. Rather unusually in international comparison, medical students are endowed with credentials for two hospital positions in the course of their studies: Hospital Orderly (i.e., “Nursing aid”) after three successfully completed semesters; and Medical Care Assistant after four successfully completed semesters. Hospital Orderly performs auxiliary and service activities necessary for the provision of basic nursing, preventive, curative, and diagnostic care, mostly under supervision; while the Medical Care Assistants can also participate in basic nurse care provision independently and perform some procedures of advanced nursing care under supervision. This credentialing system was effective until 1. 1. 2021 when a new system was introduced in which medical students were granted credentials required to work as Practical Nurses after completion of eight semesters (120 weeks) of their medical study programme [19].
While this change reflected the shift in needs of healthcare to respond effectively to the pandemic during the data collection and the manuscript completion phase of our survey the executive orders necessary for its implementation were not finalized, and therefore this alteration was not reflected in our methodology.
Methods
The national online survey KORONA 2020/21 was conducted from 23 March to 28 April 2021. The survey aimed at all students of the Czech medical programmes involved in the pandemic response studying the medicine excluding English speaking programmes. Seven out of eight medical schools in the Czech Republic participated and distributed the survey to their students enrolled in the General Medicine programme in the academic year 2020/21. For comprehensibility testing, the survey was first distributed to the students of the 5th year of the Third Faculty of Medicine Charles University. The subsequent full-scale distribution was conducted by the Study Departments of the participating medical schools via enclosed, login requiring university IT systems, using institutional encrypted email lists. All medical students received an explanatory email written by the authors, stating the purpose of the survey and information about the authors. To increase the response rate, students were also informed about the ongoing survey in Academic Senate [20] social media groups.
The survey consisted of 52 compulsory questions with additional voluntary comment questions, and was divided into three parts: 1. Demography (gender, medical school, study year, additional health-related education); 2. Student involvement (questions on the work obligation, number of shifts in different healthcare facility types, salaries, as well as the effects of their involvement in the pandemic response on their education); 3. Clinical competencies (drawing on their definitions in the legal framework). At the time of the survey conduction no surveys similar in focus nor methodology were available, thus, the validity testing was not performed.
For medical facilities involved in the pandemic response the following classification reflecting the assumed scope of the medical care provided was used in the survey: inpatient acute (hospitals); inpatient long-term (psychiatric, rehabilitation and geriatric hospitals); nursing homes and hospices; outpatient care (GP and outpatient specialists); and pre-hospital (EMS + triage). Only respondents working at least five shifts (i.e., “contacts” within the healthcare facility; at least 20 h of working) in any type of medical care were included in our competence analysis; and each student was included in only one category when working in multiple settings (in the category with the widest spectrum of care provided). Responses of students who did not participate in activities related to the COVID-19 pandemic and could not be included in any of the categories; students with additional healthcare education; and students with outlying answers for the question on the number of completed shifts (more than three standard deviations from the mean) were also excluded.
The clinical competencies part of the survey was based on the Czech legislation of 2004, covering competencies of healthcare workers in four distinct categories: “Hospital orderly,” “Medical care assistant,” “Practical nurse,” and “General nurse” [21], which reflect the gradual degrees of expertise and proficiency, independence of practice, and supervision required. In cases where a particular competency was included in more than one healthcare worker category, only the most detailed wording of the competency was used (Table 1). In some cases, competencies were subdivided because of the wide scope of competencies included. Three competencies were omitted because of they were neither specific enough nor relevant to the care provided. For the evaluation of the clinical competencies a scoring system was used: fifty-six selected competencies were grouped and scored based on the proficiency level of the healthcare worker category from whom the competency was adopted: competency of the “General nurse” was assigned four points, “Practical nurse” three points, “Medical care assistant” two points, “Hospital orderly” one point. Students who performed the given clinical competency (either with or without supervision) were granted number of points equal to the level of the competency. The sum of points equals the total value of competency level achieved by the individual student.
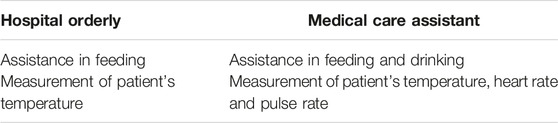
TABLE 1. Clinical competencies methodology, grey color: wording used (Prague, Czechia. 2022).
The distribution of the respondents among the medical faculties and study years was not balanced (Figure 2). Therefore, a sample balancing was used to weigh the data. Two sets of weights were assigned to each combination of the faculty and the study year. The first weighting set (balancing all the study years summed) was created by dividing the proportion of the respondents from each medical school and the study year by the real proportion of the medical students. This set was used to adjust the value of answers when the groups consisting of medical students from different study years were compared. The second weighting set (balancing each study year separately) reflected the disproportion between medical schools in the study years. This weighting set adjusted the answers when the variables across the study years were compared.
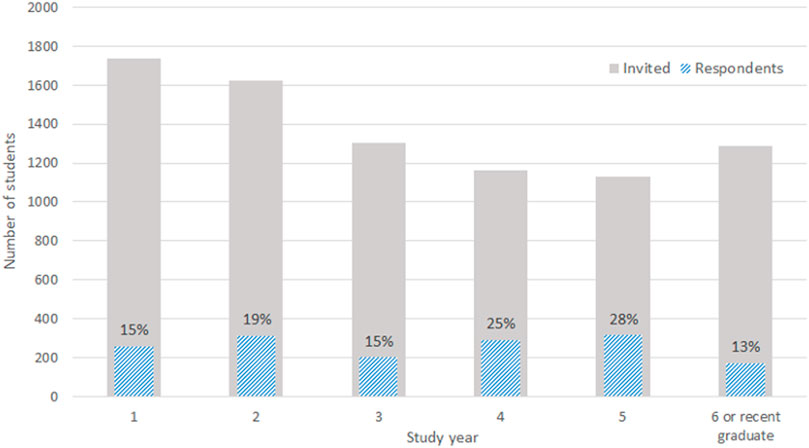
FIGURE 2. The real student distribution (grey) and the data distribution (blue) by the study years (source: Study departments of the participating medical faculties) (Prague, Czechia. 2022).
Differences among the groups were tested for several variables using the weighted Kruskal-Wallis test followed by the pairwise Wilcoxon rank-sum tests to identify the significantly different pairs. As the data shows non-normality, the Kruskal-Wallis test was used instead of the ANOVA test. The standard 5% significance level is used in reporting.
Results
A total of 8,248 students were reached, out of which 1,550 returned the survey, 431 respondents were excluded from further analysis (students not involved during the pandemic). Furthermore, 89 respondents were excluded from the competency analysis as they did not work for at least five shifts in a healthcare facility; additional 17 were excluded as they had additional healthcare education and 16 provided outlying answers; resulting in the dataset of 997 valid responses. Although the exact number of Czech students involved during the COVID-19 pandemic varied, based on the available data of the governmental Medical Committee, 2,396 medical students were involved in the pandemic response [22]. This results in the response rate of 41.6% among deployed students. Response rates varied between the study years (ranging from 13% to 28%, Figure 2). The dataset consisted of 35% males, 64% females and <1% unspecified which corresponds with a normal medical student’s gender distribution in the Czech Republic [23, 24].
Student Involvement
Students (n = 997) were often involved in more than one type of care setting at different times. The average number of shifts students worked varied across these settings: inpatient acute care (29.0; n = 710), inpatient long-term care (22.4; n = 112), nursing care homes (32.7; n = 39), outpatient care (26.5; n = 104), and pre-hospital care (32.6; n = 416). Within the category of inpatient acute care most of the students were involved in university hospitals (52.1%) and major regional hospitals (20.2%).
A negative effect of the involvement on the academic performance was reported mainly by 4th and 5th-year students, in 52% and 50%, respectively. The gain in theoretical knowledge was most positively reported by 1st-year students—67%, and a positive development in terms of clinical skills was mostly reported by 2nd-year students in 76% (Table 2).

TABLE 2. Effects of COVID involvement on medical students (Prague, Czechia. 2022).
Competency Analysis
On average, students (n = 997) achieved 60.6 competency points (CI: 54.3, 66.9), performed 20.5 competencies (CI: 18.4, 22.5) either independently or with supervision; with an average competency value of 2.96. The sum of competency points students achieved during their involvement did not constantly increase with the study years; however, an average value of the specific competencies did (Table 3). The mean value of the competency points was highest in the setting of acute inpatient care (73.6; n = 692), with the average number of the clinical competencies that students performed being 24.3.
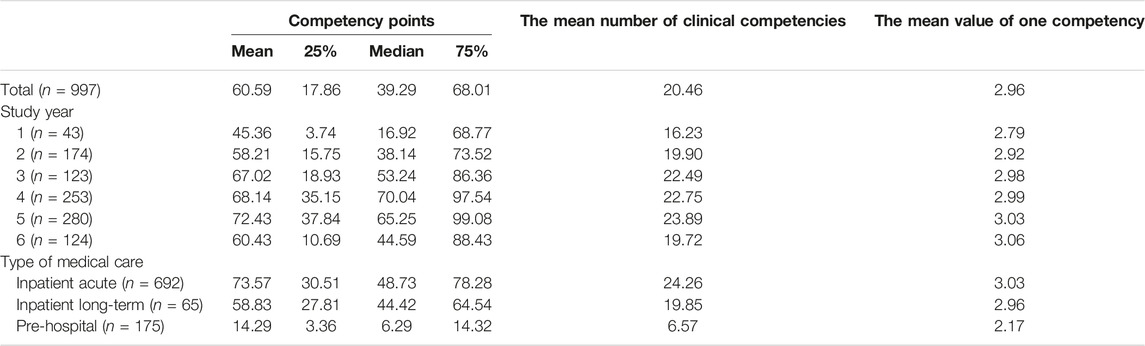
TABLE 3. Competency points of medical students (Prague, Czechia. 2022).
Both the competency points and the number of clinical competencies performed are highly correlated with the total sum of shifts covered (corr = 0.68 and 0.70, respectively), especially the number of shifts covered in inpatient acute care (corr = 0.70 and 0.70 respectively). In the acute care where the student exposure to nursing competencies was the highest, the following competencies were performed by more than half of the students (Table 4, n = 997), either independently or with supervision.
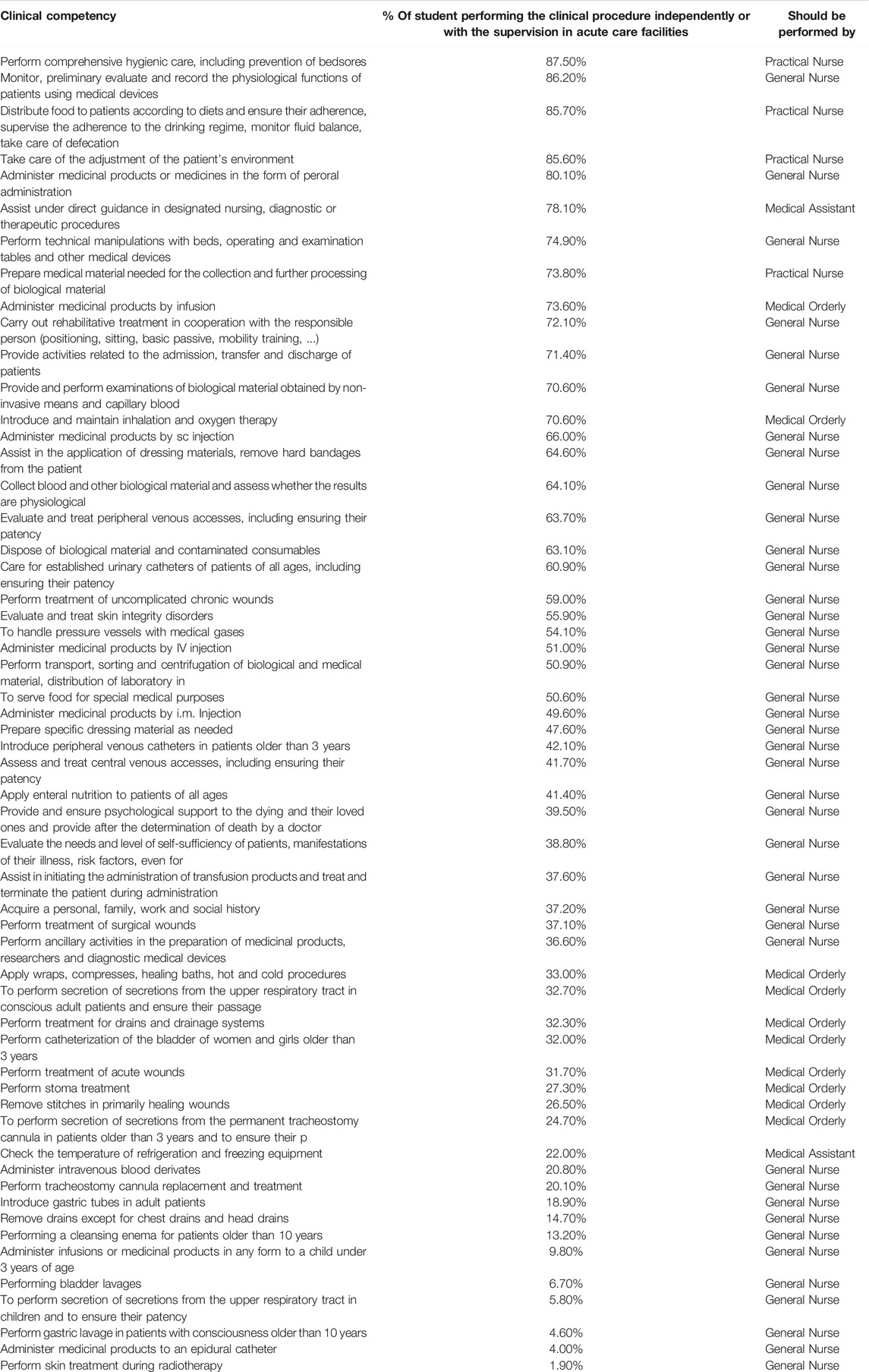
TABLE 4. Inpatient acute care: percentages of medical students performing clinical procedures with supervision or independently (quartiles differentiated) (Prague, Czechia. 2022).
Statistically significant differences in competency points exist both among the study years and the observed types of healthcare settings. Nevertheless, the differences are not significant for all possible combinations of the study years, i.e., 1st and 2nd study year (p-value = 0.083), 2nd and 3rd (p = 0.096), 2nd and 6th (p > 0.1), 3rd and 6th (p > 0.1), 4th and 5th (p > 0.1). There is also no significant difference between inpatient acute care and long-term care. For the number of competencies data entry, the insignificantly different pairs are the same as above with an additional pair of study years 1 and 6. For a robustness check, alternative sets of points were assigned to the General nurse, Practical nurse, Medical care assistant, Hospital orderly, i.e., 10-5-2-1 and 12-6-2-1, in contrast with the original 4-3-2-1 scheme. However, the statistical significance of the differences was not affected by this change.
International Context
In order to contextualize our findings, we conducted preliminary international background research (October 2020 to February 2021) with an aim to gather information on work obligation application and student involvement. Embassies and Ministries of Health of all European countries were contacted via emails with questions on credentials and student recruitment during COVID-19 (Supplementary Material S1) The research confirmed that no unified terminology, system of competency-based study outcomes, or credentialing for medical students exist in Europe in contrast to that existing for medical graduates [25, 26]. Detailed international analysis would highly extend focus of this article and it would be desirable to cover the area in further research [27].
Discussion
Our data suggest the national legal competency framework incorrectly defined the actual competency potential of medical students at all levels of student’s progression through medical school. Due to the lack of the alignment of educational and legal framework, healthcare facilities assigned competencies to students unsystematically. In general, majority of the reported clinical competencies were formally part of the nursing care skillsets. Drawing on the data (Table 4) we conclude that clinical competencies performed were mostly competencies formally corresponding to the highest level, i.e., “Practical Nurse” and “General Nurse.” It is nevertheless likely that during the crisis scenario with insufficiency of properly qualified workers, the required induction and adaptation process, lasting most commonly 3 months, was not adhered to suggesting students were not properly trained.
Using our methodology, the strong correlation between the study year and competency points can only be observed in the first three years of study years. Once in the clinical phase of the medical training the differences are statistically insignificant (Table 3). The most positive effect on clinical skills development was reported by the second-year students. This is understandable since the second-year students are already after their first contact with healthcare environment but did not have many opportunities to learn yet (more above). Thus, for them, the involvement during the pandemic facilitated and accelerated the clinical skill learning process the most. Interestingly, students of the final year reported a decrease in the absolute number of the competency points, which can be explained by several factors. Final year students had more study-related responsibilities (obligatory state exams) than the junior students and were exempted from work obligation in the 2020/21 academic year; consequently, the number of shifts staffed was lower. Also, a higher proportion of these students were involved in pre-hospital care with a relatively narrow spectrum of the care provided. However, it is important to highlight that both the sum of competency points and the spectrum of competencies reported by the final year students are still highly exceeding the official clinical competency framework. In terms of implication of the work obligation for the students it is nevertheless important to consider that more senior students’ years with the longest duration of the work obligation (4th and 5th study year) reported the most negative effects of the involvement on their studies. On the other hand, the reported positive effects are undeniable (Table 2). It is therefore highly desirable that the relevant authorities consider effects of these legal measures on medical education in greater detail—most importantly with emphasis on exposition of the students to clinical practice and the acquisition of competencies and skills [28–30]. Some students reported performance of competencies which would under normal conditions be exclusively assigned only to properly educated nursing staff (Table 4). This finding is further pronounced in the clinical study years (5th and 6th), where students could be profoundly involved in provision of healthcare. In some countries [31–34], a medical student with sufficient training can achieve a level of competencies nearly equivalent to the medical graduate working under supervision (e.g., “provisional doctor”). Therefore, an informed discussion with subsequent alignment of educational and legal framework should follow on a national level.
From crisis management point of view, in situations where an increased demand for healthcare workers is expected—especially over a longer duration—the capacity of potential workforce should be evaluated in advance [35]. This dimension of pandemic preparedness was not addressed sufficiently in the Czech Republic national pandemic response plans. Based on our analysis we recommend that instead of the year-based system of credentials currently used in the Czech legislation, a competency-based system aligned with the educational framework of study outcomes is more appropriate for assigning clinical competencies [36]. From our data, we conclude that the deployment of medical students has a strong potential to address shortages of qualified staff in critical situations in healthcare [37]. However, the legal framework for student’s deployment must be adjusted to reflect current medical educational frameworks of gradually acquired competencies and clinical skills. Vice versa, medical programmes should have official competency acquisition system reflected in the national legislation [38]. Additionally, medical education should reflect on the potential needs of healthcare system in critical situations and take them into consideration in curriculum design and development, to ensure relevant skills and competencies are acquired in a clearly defined and timely manner [39]. These adjustments have the potential to create more relevant, flexible, and effective system for assigning clinical competencies and improve crisis preparedness, while ensuring patient safety and quality of care. The probability of another large-scale pandemic is likely to increase in the upcoming decades [40], as is the likelihood of various health emergencies related to climate change, and the need for medical student involvement might reemerge [41].
Although introduction of the work obligation for medical students was a unique feature of pandemic response in the Czech Republic, the idea of students’ voluntary involvement during crisis situations periodically resonates abroad [42–45]. Available studies mostly focus on the sole potential of the students through mapping their willingness of being involved or general effects of the crisis situations on medical education [46–50]. Even recently, in Ukraine war, the government decided not to recruit full-time students without previous military experience for the service [51] and no data are available. Thus, relevant statistic, clinical or operational numbers or guidelines on potential involvement of medical students in healthcare provision are non-existent. Therefore, it would be highly desirable to focus efforts on these areas at domestic level and to implement necessary changes in national medical curricula and legislation.
From a wider perspective comprehensive international system of competency-based study outcomes in medical education would be beneficial. Currently complicated by differences in national legislations, medical curricula governance and non-uniform nomenclature [52, 53], if established, it could serve as an important factor for crisis preparedness and response effectiveness. This system would also facilitate student mobility, widen the opportunities for international collaboration in critical situation, as well as serve as a stimulus for modernization of medical school curricula to adapt to the evolving needs of population in health emergencies. International coordination of educational outcomes and legal frameworks governing medical competencies has the potential to impact healthcare provision in a global context and improve the preparedness for various crises in the future. Given its international significance, we call for a detailed comparative analysis of various national systems of clinical competences in medical education as a first step towards an informed debate about the benefits, potential risk factors, as well as ethical aspects of the deployment of medical student in healthcare [54].
Experience from the Czech Republic shows that medical students helped to alleviate the healthcare staff shortage and proved that the whole medical student community can significantly contribute to strengthen the healthcare system [55]. However, our analysis of their involvement uncovered an apparent convergence between the rigid competency system of credentials and the actual competencies and procedures that students performed during deployment in healthcare facilities. In conclusion, good clinical practice rests on evidence-based medicine. The same should be applied for setting of the proper inter/national legislation delineating medical students’ competencies, extent of their involvement in healthcare processes or their role in crisis situations. It is apparent that looking for an optimal solution will require additional data research, nevertheless, valuable lessons learned from the COVID pandemic can facilitate and inspire changes in processes to improve student experience [56], increase patients safety [57] and resilience of the healthcare systems [54].
Limitations
The value of the findings is limited by the methodology used. The situation in the Czech Republic was unique in both extent of students’ involvement and competencies granted to them. Since students operated in many different healthcare facilities it was not possible to interview supervising staff and instead, students were surveyed. A potential bias of students’ self-evaluation [58] was mitigated in survey design using quantitative reporting instead of qualitative reporting. Survey response rate is calculated using limited governmental sources. From the beginning, the survey’s target group were only the students who were involved in provision of the healthcare during the COVID-19 pandemic, thus, students not involved were not included in the analysis. Due to the high number of questions used in the survey, we decided not to measure how many times a single competency was performed, and the competencies are reported in “Performed/Not performed” manner rather than in three more detailed categories (“Performed independently/Performed under the supervision/Not performed”) which would have provided additional information on functioning of the adaptation process and assignment of the competencies on-site, but inconveniently prolonged the survey. A compromise was also made during the selection of the competencies from the legislation. It is possible that if clinical competencies of only nursing positions (General and Practical nurse) were analyzed, more accurate results on the “out of the legislation scope” would be achieved. Finally, for a competency sub-analysis, a spectrum of the care was used as a primary classification parameter instead of the time factor (i.e., the number of the shifts). This assumed that the scope of clinical competencies is directly related to the spectrum of the care provided in given healthcare facility and not to the time factor. Despise these limitations, the presented limits, we believe that the methodology allowed to accurately analyze the practical implications of the current legislation.
Ethics Statement
The survey was created and conducted in concordance with the Charles University Code of Ethics [59]. The survey was fully anonymous, the participation was voluntary, no identifiable data were collected or saved, and the purpose of the survey was clearly stated both in the introduction and in the e-mail sent to the potential participants.
Author Contributions
PM was the leader of the research group, the co-ordinator of the survey and of the article preparation process. LS performed all statistical tests and chose the methodology used. LF provided additional expertise regarding the public health impact and the textation corrections. DM was a guarantor of the project and supervised all of the activities.
Conflict of Interest
The authors declare that they do not have any conflicts of interest.
Acknowledgments
We want to thank vice-deans for the study affairs of the participating medical schools: Charles University, Ostrava University and Palacky University in Olomouc, Dr. Kostrhun of the IT department of the Third Faculty of Medicine and Dr. Kučera for their valuable insights.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.ssph-journal.org/articles/10.3389/ijph.2022.1605187/full#supplementary-material
Supplementary Material S1 | Collected answers of the international research (Prague, Czechia. 2022).
References
1. Mahase, E. Covid-19: Portugal Closes All Medical Schools after 31 Cases Confirmed in the Country. BMJ (2020) 368:m986. doi:10.1136/bmj.m986
2. Baker, D, Bhatia, S, Brown, S, Cambridge, W, Kamarajah, S, McLean, K, et al. Medical Student Involvement in the COVID-19 Response (2020).
3. Patrinely, J, Zakria, D, Berkowitz, S, Johnson, D, and Totten, D. COVID-19: the Emerging Role of Medical Student Involvement. Med Sci Educator (2020) 30(4):1641–3. doi:10.1007/s40670-020-01052-6
4. Bostock, N. Medical Students and Recently Retired Doctors Could Help Coronavirus Response, Says CMO [Internet]. Gponline.com (2020). Available from: https://www.gponline.com/medical-students-recently-retired-doctors-help-coronavirus-response-says-cmo/article/1676062 (cited June 27, 2022).
5. West, J. The Physiological Challenges of the 1952 Copenhagen Poliomyelitis Epidemic and a Renaissance in Clinical Respiratory Physiology. J Appl Physiol (2005) 99(2):424–32. doi:10.1152/japplphysiol.00184.2005
6. Diehl, H. The Role of Medical Education in the War. Acad Med (1942) 17(6):369–76. doi:10.1097/00001888-194211000-00005
7.Vládní Usnesení Související S Bojem. Vládní Usnesení Související S Bojem [Internet]. Prague, CZ: Government of the Czech Republic (2022). Available from: https://www.vlada.cz/cz/epidemie-koronaviru/dulezite-informace/vladni-usneseni-souvisejici-s-bojem-proti-epidemii-180608/ (cited Oct 23, 2022).
8.info@aion.cz A. 110/1998 Sb. Ústavní Zákon O Bezpečnosti ČR [Internet]. Zákony pro lidi (2022). Available from: https://www.zakonyprolidi.cz/cs/1998-110/zneni-20001201 (cited June 27, 2022).
9.Parliament of the Czech Republic. Resolution of the Government of the Czech Republic to Ensure the Provision of Health Services to Health Service Providers and to Ensure the Activities of Public Health protection Authorities for the Duration of the Emergency. 7. 409/2020 Sb. [Internet]. Psp.cz (2020). Available from: https://www.psp.cz/sqw/sbirka.sqw?cz=409&r=2020 (cited June 27, 2022).2022.
10. Šírek, A. Impacts of the Floods in 2002 on the Capital City of Prague [extended Abstract of Dissertation on the Internet]. Prague: Charles University (2020). p. 55 p. Available from: https://dspace.cuni.cz/bitstream/handle/20.500.11956/127395/130289688.pdf?sequence=1 (cited Oct 23, 2022).
11.Czech Hydrometeorological Institute. Vyhodnocení Povodní V Červnu a Červenci 2009 Na Území České Republiky [Internet]. ČINNOST POVODŇOVÉ SLUŽBY A SLOŽEK IZS. Prague: Czech Hydrometeorological Institute (2009). p. 61 p. Available from: https://www.chmi.cz/files/portal/docs/hydro/povodne/pov09/doc/06.pdf (cited Oct 23, 2022).
12.Obyvatelstvo | ČSÚ [Internet]. Czso.cz (2021). Available from: https://www.czso.cz/csu/czso/obyvatelstvo_lide (cited June 27, 2022).
13.QCM S. Data O Studentech, Poprvé Zapsaných a Absolventech Vysokých Škol, MŠMT ČR [Internet]. Msmt.cz (2021). Available from: https://www.msmt.cz/vzdelavani/skolstvi-v-cr/statistika-skolstvi/data-o-studentech-poprve-zapsanych-a-absolventech-vysokych (cited June 27, 2022).
14.info@aion.cz A. 187/2009 Sb. Vyhláška O Minimálních Požadavcích Na Studijní Programy Všeobecné Lékařství, Zubní Lékařství. farmac. [Internet]. Zákony pro lidi (2016). Available from: https://www.zakonyprolidi.cz/cs/2009-187 (cited June 27, 2022).
15.DIRECTIVE 2005/36/EC OF THE EUROPEAN PARLIAMENT AND OF THE COUNCIL on the recognition of professional qualifications. Directive 2005/36/EC of the European Parliament and of the council on the Recognition of Professional Qualifications (2005). Available from: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:02005L0036-20140117 (cited June 27, 2022).
16. Education, N. NAB [Internet]. Nauvs.cz. Available from: https://www.nauvs.cz/index.php/en/ (cited June 27, 2022).
17.QCM s.r.o. w. EQF. Národní Pedagogický Institut České Republiky (Dříve Národní Ústav Pro Vzdělávání) [Internet]. Nuv.cz. Available from: http://www.nuv.cz/eqf (cited June 27, 2022).
18.info@aion.cz A. 96/2004 Sb. Zákon O Nelékařských Zdravotnických Povoláních [Internet]. Zákony Pro Lidi (2021). Available from: https://www.zakonyprolidi.cz/cs/2004-96 (cited June 27, 2022).
19.info@aion.cz AIONCS. 585/2020 sb. Zákon, Kterým Se Mění Zákon Č. 96/2004 sb., O Podmínkách Získávání a Uznávání Způsobilosti K VÝKONU [Internet]. Zákony pro lidi. Available from: https://www.zakonyprolidi.cz/cs/2020-585 (cited Oct 23, 2022).
20.Academic Senate [Internet]. Wikipedia. Wikimedia Foundation (2022). Available from: https://en.wikipedia.org/wiki/Academic_senate (cited Oct 23, 2022).
21.info@aion.cz A. 55/2011 Sb. Vyhláška O Činnostech Zdravotnických Pracovníků a Jiných Odborných Pracovníků [Internet]. Zákony Pro Lidi (2021). Available from: https://www.zakonyprolidi.cz/cs/2011-55 (cited June 27, 2022).
22.Parlament České republiky. Poslanecká Sněmovna 2017 – 2021 [Internet]. PR, PS 2017-2021, VVVKM, Schůze Č. 44 (18. Listopadu 2020) (2022). Available from: https://www.psp.cz/sqw/text/text2.sqw?idd=72705 (cited Oct 23, 2022).
23.Czech Medical Chamber. Prague: Zdravotnický deník (2022). Available from: https://www.zdravotnickydenik.cz/2022/04/vice-nez-ctvrtina-absolventu-mediciny-kazdorocne-nenastoupi-do-zdravotnictvi/ (cited Oct 23, 2022). Více Než Čtvrtina Absolventů Medicíny Každoročně Nenastoupí Do Zdravotnictví [Internet].
24.Ministry of EducationYouth and Sports. Statistics of Education in the Czech Republic [Internet]. MŠMT ČR - Statistika školství. Available from: https://www.msmt.cz/vzdelavani/skolstvi-v-cr/statistika-skolstvi?lang=1 (cited Oct 23, 2022).
25. Bedoll, D, van Zanten, M, and McKinley, D. Global Trends in Medical Education Accreditation. Hum Resour Health (2021) 19:70. doi:10.1186/s12960-021-00588-x
26. Kovacs, E, Schmidt, AE, Szocska, G, Busse, R, McKee, M, and Legido-Quigley, H. Licensing Procedures and Registration of Medical Doctors in the European Union. Clin Med (Lond) (2014) 14(3):229–38. doi:10.7861/clinmedicine.14-3-229
27. Ross, M, and Cumming, A. (2008). The Tuning Project (Medicine) - Learning Outcomes/Competences for Undergraduate Medical Education in Europe. doi:10.13140/RG.2.1.4620.7765
28. Harries, AJ, Lee, C, Jones, L, Rodriguez, RM, Davis, JA, Boysen-Osborn, M, et al. Effects of the COVID-19 Pandemic on Medical Students: a Multicenter Quantitative Study. BMC Med Educ (2021) 21:14. doi:10.1186/s12909-020-02462-1
29. Hu, L, Wu, H, Zhou, W, Shen, J, Qiu, W, Zhang, R, et al. Positive Impact of COVID-19 on Career Choice in Pediatric Medical Students: a Longitudinal Study. Transl Pediatr (2020) 9(3):243–52. doi:10.21037/tp-20-100
30.TMS Collaborative. The Perceived Impact of the Covid-19 Pandemic on Medical Student Education and Training – an International Survey. BMC Med Educ (2021) 21:566. doi:10.1186/s12909-021-02983-3
31. Harvey, A. Covid-19: Medical Students and FY1 Doctors to Be Given Early Registration to Help Combat Covid-19. 2020.
32.Association of American Medical Colleges. Recommendations for Clinical Skills Curricula for Undergraduate Medical Education [Internet]. Recommendations for Clinical Skills Curricula for Undergraduate Medical Education (2005). Available from: https://store.aamc.org/recommendations-for-clinical-skills-curricula-for-undergraduate-medical-education-pdf.html (cited Oct 23, 2022).
33. Lindgren, S, Brännström, T, Hanse, E, Ledin, T, Nilsson, G, Sandler, S, et al. Medical Education in Sweden. Med Teach (2011) 33(10):798–803. doi:10.3109/0142159X.2011.570816
34. Scott, RW, and Fredriksen, K. Extracurricular Work Experience and its Association with Training and Confidence in Emergency Medicine Procedures Among Medical Students: a Cross-Sectional Study from a Norwegian Medical School. BMJ Open (2022) 12:e057870. doi:10.1136/bmjopen-2021-057870
35.CDC. Healthcare Workers. Centers for Disease Control and Prevention (2020). Available from: https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-recommendations.html (cited June 27, 2022).
36. Ryan, MS, Holmboe, ES, and Chandra, S. Competency-Based Medical Education: Considering its Past, Present, and a Post-COVID-19 Era. Acad Med (2022) 97(3S):S90–S97. doi:10.1097/ACM.0000000000004535
37. Wohlfarth, B, Gloor, B, and Hautz, WE. Challenges of Students and Residents of Human Medicine in the First Four Months of the Fight against the Covid-19 Pandemic - Implications for Future Waves and Scenarios. BMC Med Educ (2021) 21(1):554. doi:10.1186/s12909-021-02962-8
38. O'Byrne, L, and Gavin, B. Medical Students and COVID-19: the Need for Pandemic Preparedness. J Med Ethics (2020) 46:623–6. doi:10.1136/medethics-2020-106353
39. Müller, L, Heymanns, M, Harder, L, Winter, J, Gehring, S, Düber, C, et al. Medical Students’ Commitment during the SARS-CoV-2 Pandemic: Preparedness, Motivation, and Impact on Students’ Skills, (2020), PREPRINT (Version 1) available at Research Square. doi:10.21203/rs.3.rs-37069/v1
40. Marani, M, Katul, G, Pan, W, and Parolari, A. Intensity and Frequency of Extreme Novel Epidemics. Proc Natl Acad Sci (2021) 118(35):e2105482118. doi:10.1073/pnas.2105482118
41. Mash, S. Medical Students Urged to Volunteer as NHS winter Crisis Worsens [Internet]. The Guardian. Guardian News and Media (2018). Available from: https://www.theguardian.com/society/2018/jan/14/inexperienced-medical-students-urged-volunteer-nhs-winter-crisis-worsens (cited Oct 24, 2022).
42. Anderson, ES, and Patel, K. The Student Workforce: Untapped Possibilities. Clin Teach (2020) 17:549–50. doi:10.1111/tct.13217
43. ten Cate, O, Schultz, K, Frank, JR, Hennus, MP, Ross, S, Schumacher, DJ, et al. Questioning Medical Competence: Should the Covid-19 Crisis Affect the Goals of Medical Education? Med Teach (2021) 43(7):817–23. doi:10.1080/0142159X.2021.1928619
44. Miller, D, Pierson, L, and Doernberg, S. The Role of Medical Students during the COVID-19 Pandemic. Ann Intern Med (2020) 173(2):859–146. doi:10.7326/L20-1195
45. Hentze, I. COVID-19: Occupational Licensing during Public Emergencies [Internet]. Ncsl.org (2020). Available from: https://www.ncsl.org/research/labor-and-employment/covid-19-occupational-licensing-in-public-emergencies.aspx (cited June 28, 2022).
46. Herman, B, Rosychuk, RJ, Bailey, T, Lake, R, Yonge, O, and Marrie, TJ. Medical Students and Pandemic Influenza. Emerg Infect Dis (2007) 13(11):1781–3. doi:10.3201/eid1311.070279
47. Jain, N, Panag, DS, Srivastava, M, Mohan, S, Chodnekar, SY, Akbari, AR, et al. Fate and Future of the Medical Students in Ukraine: A Silently Bubbling Educational Crisis. Med Educ (2022) 56(8):779–82. doi:10.1111/medu.14818
48. Dobiesz, VA, Schwid, M, Dias, RD, Aiwonodagbon, B, Tayeb, B, Fricke, A, et al. Maintaining Health Professional Education during War: A Scoping Review. Med Educ (2022) 56(8):793–804. doi:10.1111/medu.14808
49. Lincango-Naranjo, E, Espinoza-Suarez, N, Solis-Pazmino, P, Vinueza-Moreano, P, Rodriguez-Villafuerte, S, Lincango-Naranjo, J, et al. Paradigms about the COVID-19 Pandemic: Knowledge, Attitudes and Practices from Medical Students. BMC Med Educ (2021) 21(1):128. doi:10.1186/s12909-021-02559-1
50. Michno, DA, Tan, J, Adelekan, A, Konczalik, W, and Woollard, ACS. How Can We Help? Medical Students' Views on Their Role in the COVID-19 Pandemic. J Public Health (Oxf) (2021) 43(3):479–89. doi:10.1093/pubmed/fdaa271
51.Verkhovna Rada adopts law “on introduction of amendments into Article 23 of Law of Ukraine “on Mobilization Training and mobilization” [Internet]. News - Verkhovna Rada Adopts Law “On Introduction of Amendments into Article 23 of Law of Ukraine “On Mobilization Training and Mobilization”. Information Department of the Verkhovna Rada of Ukraine Secretariat (2015). Available from: https://www.rada.gov.ua/en/news/News/109295.html (cited Oct 24, 2022).
52. Harden, RMMD. International Medical Education and Future Directions: A Global Perspective. 81. December: Academic Medicine (2006). p. S22–S29. doi:10.1097/01.ACM.0000243411.19573.58.12
53. Brouwer, E, Driessen, E, Hidayah Mamat, N, Devi Nadarajah, V, Somodi, K, and Frambach, J. Educating Universal Professionals or Global Physicians? A Multi-centre Study of International Medical Programmes Design. Med Teach (2020) 42(2):221–7. doi:10.1080/0142159X.2019.1676885
54. Stachteas, P, Vlachopoulos, N, and Smyrnakis, E. Deploying Medical Students during the COVID-19 Pandemic. Med Sci Educator (2021) 31(6):2049–53. doi:10.1007/s40670-021-01393-w
55. Rasmussen, S, Sperling, P, Poulsen, MS, Emmersen, J, and Andersen, S. The Lancet. Elsevier (2020). Available from: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)30923-5/fulltext (cited Oct 23, 2022). Medical Students for Health-Care Staff Shortages during the COVID-19 Pandemic [Internet].
56. Jaishankar, D, Dave, S, Tatineni, S, Alkureishi, M, Zhu, M, Chretien, K, et al. U.S. Medical Student Experiences during the COVID-19 Pandemic: A National Survey. Acad Med (2021) 9696(11):S207–S208. doi:10.1097/ACM.0000000000004272
57. Melnyk, BM, Gallagher-Ford, L, Zellefrow, C, Tucker, S, Thomas, B, Sinnott, LT, et al. The First U.S. Study on Nurses' Evidence-Based Practice Competencies Indicates Major Deficits that Threaten Healthcare Quality, Safety, and Patient Outcomes. Worldviews Evid Based Nurs (2018) 15(1):16–25. doi:10.1111/wvn.12269
58. Klassen, RM, and Klassen, JRL. Self-efficacy Beliefs of Medical Students: a Critical Review. Perspect Med Educ (2018) 7:76–82. doi:10.1007/s40037-018-0411-3
59.Code of Ethics [Internet]. Charles University. Academic Senate of Charles University (2019). Available from: https://cuni.cz/UKEN-731.html (cited Oct 24, 2022).
Keywords: medical students, COVID-19, medical education, clinical competencies, Czech Republic, legal framework, healthcare capacity, crisis preparedness
Citation: Michenka P, Fialová L, Šlegerová L and Marx D (2022) Analysis of Obligatory Involvement of Medical Students in Pandemic Response in the Czech Republic: Competencies, Experiences, and Legal Implications. Int J Public Health 67:1605187. doi: 10.3389/ijph.2022.1605187
Received: 05 July 2022; Accepted: 09 December 2022;
Published: 22 December 2022.
Edited by:
Nino Kuenzli, Swiss Tropical and Public Health Institute (Swiss TPH), SwitzerlandReviewed by:
Katarzyna Czabanowska, Maastricht University, NetherlandsKeren Dopelt, Ashkelon Academic College, Israel
Copyright © 2022 Michenka, Fialová, Šlegerová and Marx. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Petr Michenka, cGV0ci5taWNoZW5rYUBsZjMuY3VuaS5jeg==