 Hanif Abdul Rahman1,2,3*
Hanif Abdul Rahman1,2,3* Armah Tengah1,2,4Yusnani Mohd Yusof1Ly Slesman1Chang-Yau Hoon1
Armah Tengah1,2,4Yusnani Mohd Yusof1Ly Slesman1Chang-Yau Hoon1 Khadizah H. Abdul-Mumin1,2,5
Khadizah H. Abdul-Mumin1,2,5- 1Centre for Advanced Research, Universiti Brunei Darussalam, Gadong, Brunei
- 2Pengiran Anak Puteri Rashidah Sa’adatul Bolkiah Institute of Health Sciences, Universiti Brunei Darussalam, Gadong, Brunei
- 3School of Nursing, University of Michigan, Ann Arbor, MI, United States
- 4School of Health Sciences, Politeknik Brunei, Bandar Seri Begawan, Brunei
- 5School of Nursing and Midwifery, La Trobe University, Bundoora, VIC, Australia
Objective: To investigate predictors of life satisfaction and healthy aging with focus on gender differences among older people in Brunei Darussalam.
Methods: A cross-sectional study on older people recruited by proportionate sampling. Multiple linear regression stratified by gender was applied.
Results: 45.6% of life satisfaction of older women were strongly associated with self-perceived health, social relationship, and education level. For older men, 26.3% of the variance of life satisfaction was predicted by physical functioning or disability, and social relationship. For older women, 38.9% of the variance of health status can be explained with satisfaction with life, and difficulty to do daily tasks. For older men, 33.1% of the variance of health status can be accounted by income, number of children, presence of chronic illness, and diabetes.
Conclusion: This paper discusses the unique gender differences of older people from a global perspective. Policymakers and stakeholders need to account for local and contextual differences before adopting international guideline. Particularly, on the maintenance or further promotion social interactions, active engaging elderly in health maintenance, and physical and mental functioning of the older population.
Introduction
The world is rapidly aging as increasing longevity and decreasing fertility has become demographic trends [1, 2]. Research on aging has received considerable attention in medicine, public health and social sciences in recent decades. However, few had approached the importance of gender for successful aging [3]. It has become increasingly important to have gender-specific approaches to understand gender gaps among older adults. Prior evidences have suggested strong differences in disease distribution, clinical profiles, and socioeconomic status, among elderly men and women [4–7]. Aging population with higher chronic illnesses, disabilities, and dependency have significant economic and societal impact that will result in the rise of global burden of disease and disability [2, 8, 9]. There has been paramount efforts by government actors in collaboration with related stakeholders to increase period of “good health” and sustained sense of well-being to extend social productivity of older adults as much as possible [10].
Life satisfaction—a subjective feeling and attitude about one’s life at a particular point of time that could range from positive to negative—is one of the most important component of healthy aging [11]. Life satisfaction elicits a U-shaped pattern with age, meaning as a person grow older their overall satisfaction in life rises after a nadir at 50 years [12]. This corroborates with similar studies which demonstrated increasing life satisfaction with ageing [13–15] until it reaches a threshold at a certain point, which could differ by multitude of factors, and starts to decline [16, 17].
Successful aging is largely measured by subjective well-being, where life satisfaction is the major indicator [7]. There has been numerous studies investigating significant predictors of life satisfaction but gender-specific studies are scarce, which rendered limitations to enriching discussion and understanding of well-being and its determinants [7, 18–21]. Furthermore, prior evidence has established that healthy aging, is a strong contributor towards positive life satisfaction that affect elderly functioning and the primary focus of the current gerontological effort to achieve more positive outcome of aging [7].
Since the early 20th century, life expectancy has increased substantially and along with the concomitant decline in fertility rate, an ageing population is on the rise around the world. Brunei Darussalam (hereafter, Brunei) is no exception. A country is considered as an ageing population when 7 percent of the population are 65 years and above. According to the United Nation, Brunei’s older population will account for 7.7 per cent of the total population by 2025 [22]. This means in no time Brunei will have relatively higher proportion of its inhabitants being elderly compared to children [22]. By 2050, global life expectancy was estimated to increase by 4.5 years, an approximate six percent rise since 2015, and was predicted to increase continuously thereafter [22]. Still, questions remain as to whether these added years are experienced in good health and life satisfaction.
Therefore, this study was conducted with the purpose of investigating the predictors of life satisfaction and healthy aging with focus on gender differences.
Methods
Study Design
A cross-sectional study using interviewer-assisted questionnaire administration that was disseminated nationwide in all four districts of Brunei Darussalam.
Participant Selection and Setting
The study was conducted in January 2019 to January 2020 in all four districts in Brunei where the targeted participants were those within the age range of 50–75 years; held Brunei citizenship or permanent residency; lived at home or resided in an institution; lived in a household; oriented to place and persons and able to communicate in English and Malay. Adults aged 50 years or below and those who were cognitively impaired were excluded. The survey was conducted at the home where respondents reside.
The cut-off age for older adults varies chronologically, socially and scientifically or functionally. There is no uniformity across the population of the aging process. Classification of age of the older adults are also not specific, mainly due to genetics differences, lifestyle, and overall health [23]. Although the World Health Organization and the United Nation defined older persons chronologically as those population aged 60 years onwards, uniquely in Brunei early retirement age is set at 55 years old indicating the start of older adults age in Brunei [24, 25]. Sociologically, the status of such as being grandparents, and the physical aging appearance may also be used to define older persons age [26]. Similarly, functionally, in medical and healthcare, when reporting age-related or chronic health conditions, older adults are often categorized as those aged 50 years of age onwards [27]. Due to this varying, confusing and complex definitions, for the purpose of this study, older persons are defined as those aged from 50 years of age.
The Ministry of Home Affairs via the District offices granted permission to access the current population census of the four districts in Brunei. All eligible participants (n = 63,900) were then sectioned out from the total study population (n = 76,000). Minimum sample size was calculated with precision of 5% (d = 0.05). A minimum sample of 385 was required to achieve precision of 0.5 at 95% confidence interval [28]. Stratified proportionate sampling was employed to ensure recruitment of participants were proportional to district and gender of study population.
Data Collection Instruments
Data was collected by the appointed research assistants who were trained prior to data collections using a questionnaire adapted and developed from various validated and established tools including:
(1) Health and Retirement Study on Psychosocial and Lifestyle developed in the University of Michigan, United States (HRS) (Cronbach’s alpha ranged 0.77–0.89);
(2) English Longitudinal Survey on Aging (ELSA) jointly run by teams at University College London (UCL), the Institute for Fiscal Studies (IFS), NatCen Social Research and the University of Manchester in United Kingdom (Cronbach’s alpha ranged 0.89–0.90);
(3) Survey on Health, Aging and Retirement in Europe (SHARE) (Cronbach’s alpha range 0.69–0.88);
(4) Irish Longitudinal Study on Aging (TILDA) developed in Trinity College Dublin (Cronbach’s alpha 0.6–0.94);
(5) Korean Longitudinal Study of Aging (KLoSA) (Cronbach’s alpha 0.8–0.9);
(6) Japanese Study of Aging and Retirement (JSTAR) (Cronbach’s alpha 0.62–0.78).
A panel was formed to review the questions in the six questionnaires and decided to extract only relevant questions for the context of Brunei. The panel comprised of ten experts from different disciplines (Health, Economics, Business, Psychology, Social Studies, and Policy). All the relevant questions were compiled as one questionnaire that consists of:
(1) Demographics and family (8 items): Age of participants and spouse, marital status, living status, number of children, education level, and income level.
(2) Health status (20 items): overall health, satisfaction with life, ability to perform daily activities, and walking.
(3) Emotional conditions (16 items), social health (9 items), and physical health (12 items).
Each variable of interest (overall health and life satisfaction) was measured mainly using Likert-scale. For overall health, the item was scored from 1 = Very good to 4 = Poor. Satisfaction with current life was scored from 1 = Satisfied to 4 = Unsatisfied. The ability to perform daily activities items were measured dichotomously as Yes/No. The ability to walk during daily activities were scored from 1 = hardly walk to 6 = walk for more than 90 min. Emotional condition items were scored from 1 = Not at all to 4 = Always. Social health items were scored based on frequency (1 = Almost every day to every 2 months or more) and the number of persons involved (0 = None to 9 = 9 persons or more). Physical health was measured based on intensity of pain (0 = No pain to 4 = Severe pain).
The questionnaire was pre-tested on twenty elderly participants with the same inclusion criteria. Amendments to the questionnaire were made based on the feedback and comments given by the participants. In the actual data collection, two research assistants accompanied by a member of the research team collected the data. Participants were able to ask questions shall they require assistance. Full explanation of the study was offered and any questions regarding the study was answered prior to completing the questionnaire.
Data Analysis
All analyses were stratified by elderly men and women. Descriptive statistics were used to describe the sample. Univariate analysis using Chi-square test for independence and Independent t test were applied, where indicated. Multiple linear regression estimation was performed for male and female sample. First, a stepwise automatic variable selection procedure based on the Akaike Information Criterion (AIC) was computed to select variables to be included in the regression model. The significant variables selected were then checked for interaction effects and their likely multicollinearity using Variance Inflation Factor (VIF). Furthermore, residual plots were then used to check for assumptions for overall linearity, linearity of each numerical independent variable, normality, and equal variance. “Standardized” residual plots were further used to check for outliers. Hosmer-Lemeshow goodness-of-fit test was used to check for the fit of final model. All statistical analyses were performed using RStudio v1.1.383. All statistical tests are two-sided and a p-value < 0.05 is considered statistically significant.
Ethical Considerations
The research protocol of this study was reviewed by the Universiti Brunei Darussalam research ethics committee, which has approved that the present study conforms to ethical standards throughout the stages of the research process to ensure participants’ human rights were sufficiently safeguarded and protected (UBD/OAVCR/UREC/Apr18-04). Written informed consent was obtained from the participant prior to the study.
Results
In total, 429 elderly persons participated in the study. Table 1 presents characteristics of the sample segregated by gender where 50.1% were male and 49.9% were female. A significant portion of the sample were recruited from Brunei-Muara district (77.4%, p = 0.029). Majority (about 94%) of the sample were of ethic Malay origin and of Islamic belief (96%). One in four (about 24%) of the participants were membership of an organisation, clubs or societies where they mostly had activity 2 to 3 times every week (male = 35.9% and female 64.1%).
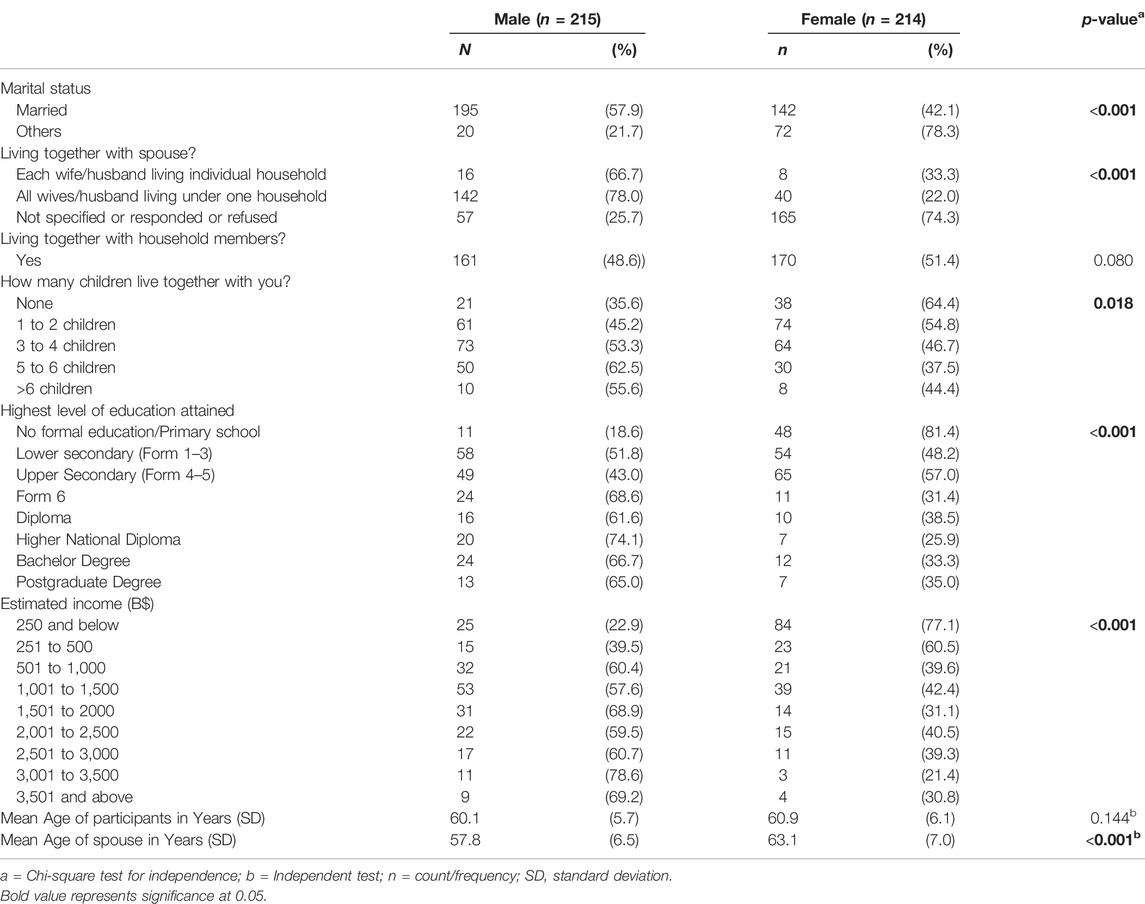
TABLE 1. Descriptive statistics of participants’ characteristics by gender (National Study of Elderly Person, Brunei, 2019).
Univariate analysis showed that male participants were significantly higher in terms of smoking, married status, and living with spouse compared to female participants (p < 0.001). Female participants had significantly higher in terms of having 1 to 2 children. On the other hand, male participants had significantly higher in terms of having 3 or more children (p = 0.018). Male participants also had significantly higher educational attainment where it was observed that proportion of male was higher from Form 6 (pre-university) and above (p < 0.001). Male participants also had significantly higher estimated income where it was observed that proportion of male was higher from B$501 and above (p < 0.001).
Table 2 illustrates the health perception, life satisfaction, and ability to do daily activities. Univariate analysis showed that elderly men (60.6%) had significantly higher perception of “very good” health compared to elderly women (39.4%) (p < 0.001). This is similar for life satisfaction where 79.0% of elderly men and 65.4% of women reported “satisfied” with life. Nonetheless, both genders were equally concern regarding the importance of health (p = 0.740) where more than 80% had undergone health screening or medical checks.
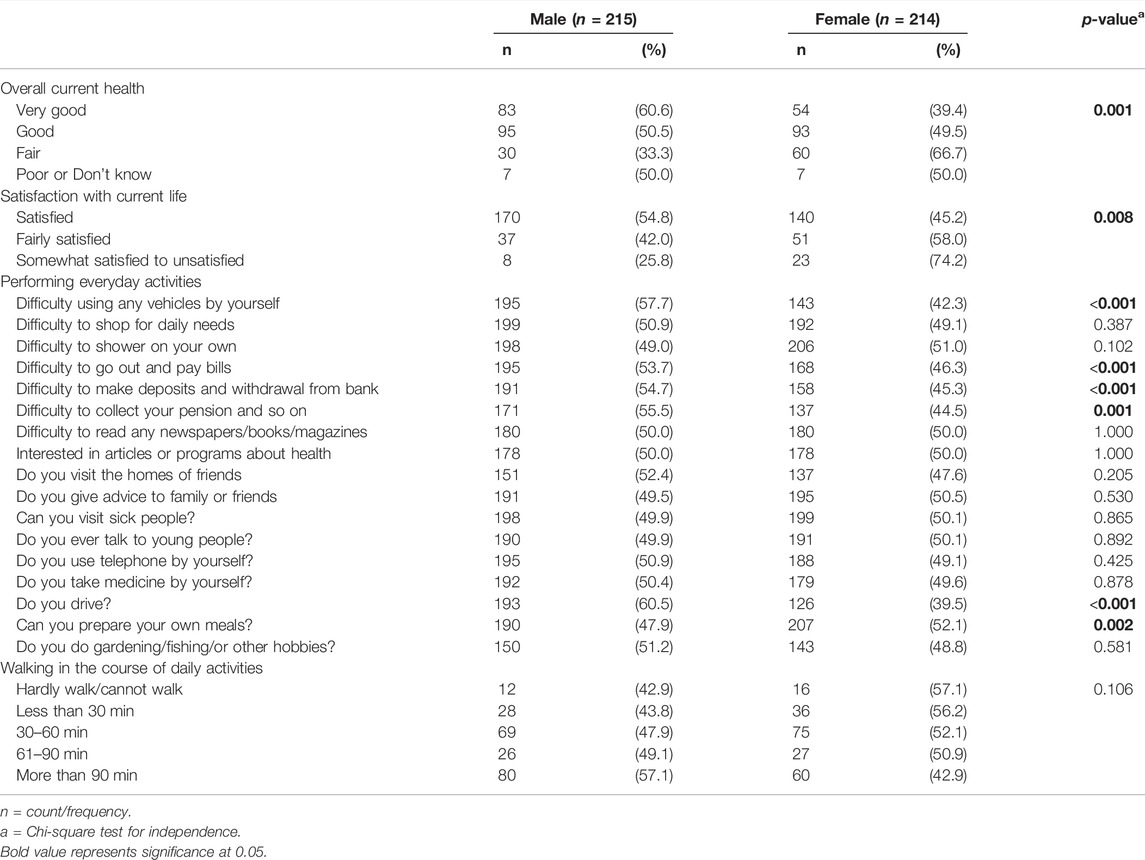
TABLE 2. Health perception, Satisfaction with life and daily activities of participants by gender (National Study of Elderly Person, Brunei, 2019).
In terms of performing daily activities, it was reported that current health problems did not impair physical functioning. Significantly higher male sample (61.8%) compared to female sample (38.2%) can still drive by themselves although they also had significantly higher report of difficulty when using vehicles (p < 0.001). They also reported significantly higher difficulty to go out and pay bills, make withdrawals or deposits, and collect pensions. On the other hand, female participants reported significantly higher difficulty in preparing meals for themselves.
Table 3 presents the mental and emotional conditions of participants as they currently perceived themselves compared to last week. The stratified analysis by gender revealed that emotional conditions among older adults were similar, in general. In conditions where there were significant differences, female participants exhibited higher emotional problems as compared to the past week, particularly in: “feeling frightened,” “feeling lonely,” “feel like crying,” “feeling sad,” “difficulty concentrating what I was doing,” and “something normally effortless became difficult to do.”
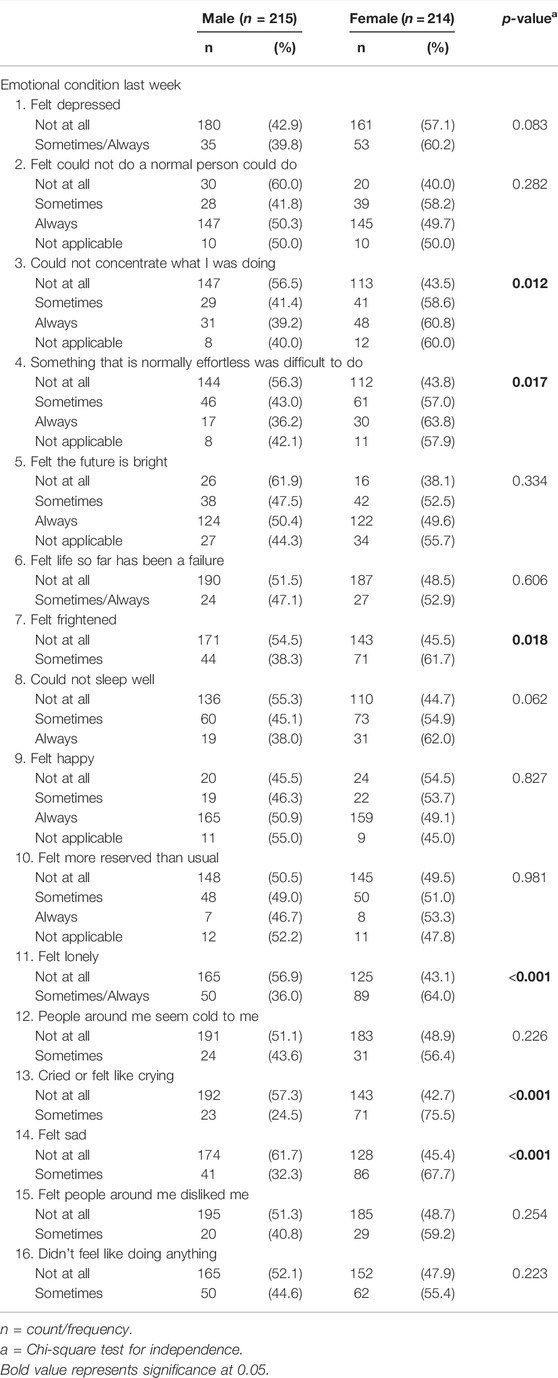
TABLE 3. Mental and Emotional conditions of participants last week by gender (National Study of Elderly Person, Brunei, 2019).
Table 4 illustrates the social health among the older adults. Univariate analysis showed that the spouse of male participants (61.0%) would be significantly more concern about them compared to spouse of female participants (39.0%) (p < 0.001). Similarly, male participants (59.4%) were significantly more concerned about their spouse if they had problem compared to female participants (40.6%) (p < 0.001). Both male and female participants reported visiting friends or relatives equally frequent, at least once a month. In addition, most of them had more than one close friend or relative that they could confide and call for help.
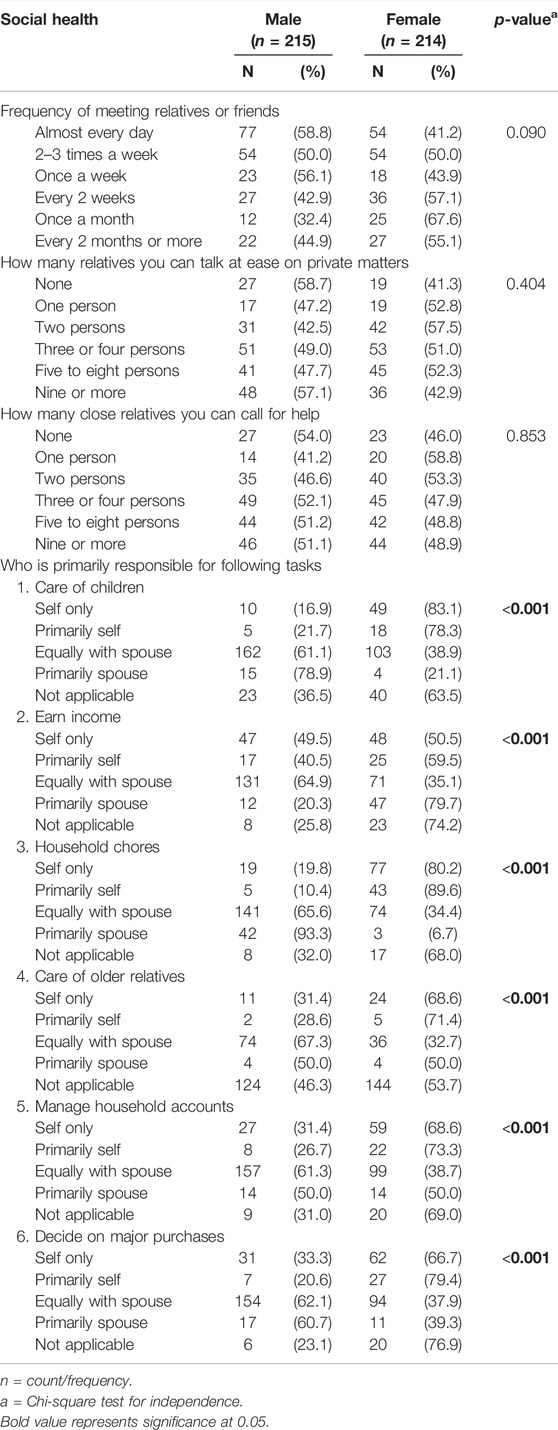
TABLE 4. Social health of older persons by gender (National Study of Elderly Person, Brunei, 2019).
In terms of caring for children, in situations where the task was equally shared with spouse, male participants (61.1%) reported significantly higher involvement compared to female participants (35.1%). Conversely, in situations where the task of caring for children were done by self or primarily self only, female participants (78.3–83.1%) reported significantly higher involvement compared to male participants (16.9%–21.7%). This was also consistent with further univariate analysis on other tasks including earning income, doing household chores, caring of older relatives, managing household accounts, and deciding on major purchases.
Table 5 presents physical health status of the sample. The results showed that male and female participants were equally suffering from musculoskeletal pain. However, there was significantly higher reports of shoulder pain, back pain, leg pain and knee pain from female participants. It was also observed that female participants (51.7%–70.7%) received significantly higher health services such as home-based nursing and medical assistance devices (for example, wheelchair) compared to male participants (29.3%–48.3%). Participants were equally reporting issues with vision and hearing, kidney, liver and heart problems, high blood pressure, diabetes, and psychiatric disorders.
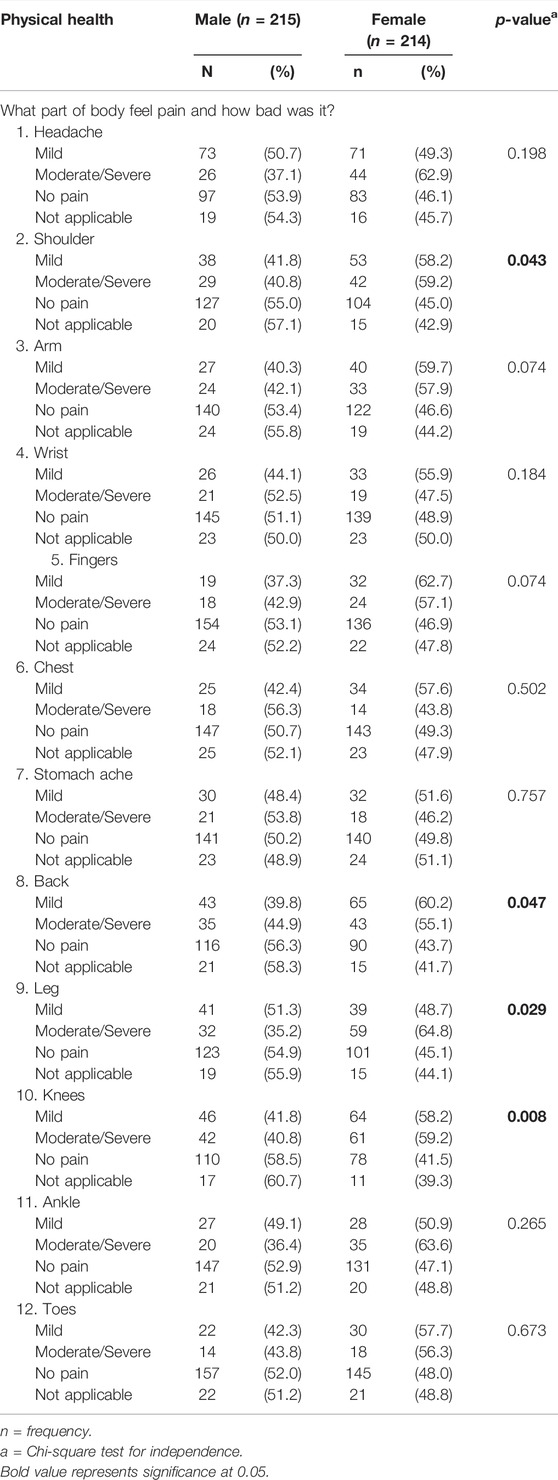
TABLE 5. Physical health of older persons by gender (National Study of Elderly Person, Brunei, 2019).
Table 6 demonstrates the correlates of perceived health and satisfaction with life among the older adults. For male participants, after adjusting for possible confounding factors, it was observed that number of children, estimated income, having chronic illness and diabetes were significantly associated with overall perceived health, explaining 33.1% of the total variance. Increase in number of children was observed to increase the perception of overall health. Conversely, increase in income, chronic illness and diabetes were observed to reduce the perception of overall health. In contrast, for female participants, 38.9% of the variance of overall perceived health could be explained by satisfaction with life and difficulty to do tasks that were normally easy.
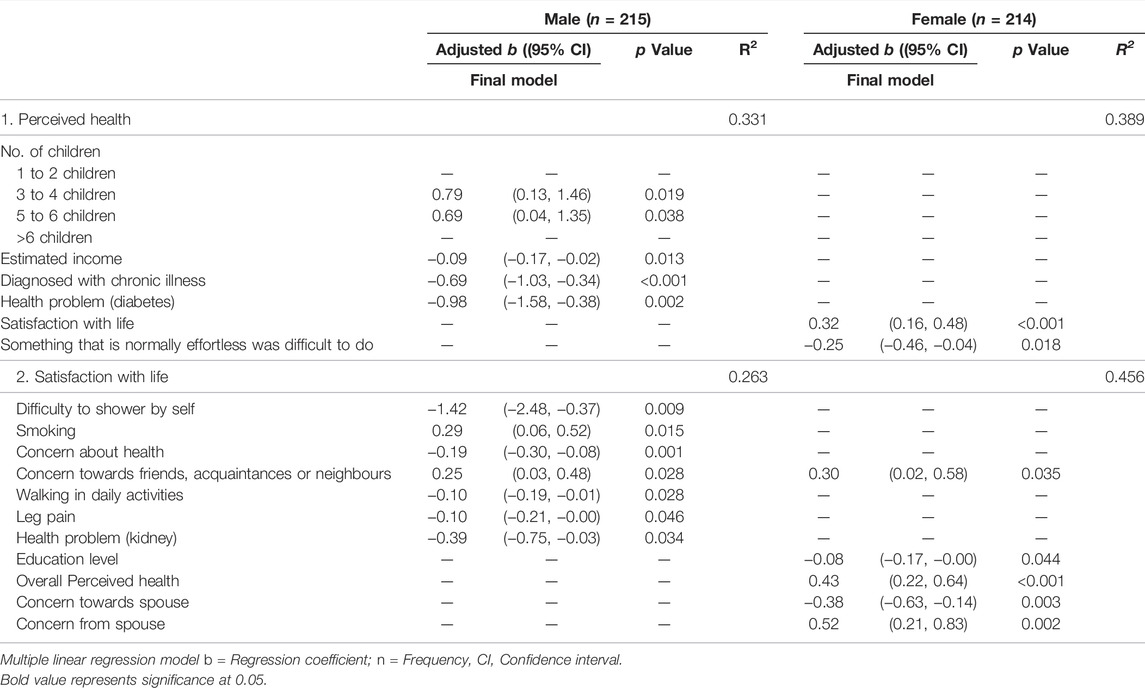
TABLE 6. Factors associated with perceived health among older person by gender (National Study of Elderly Person, Brunei, 2019).
Multiple regression was also applied for satisfaction with life. For female participants, 45.6% of the variance could be explained by having concern for friends, acquaintances or neighbours, education level, perceived health, and concern towards and from spouse, after adjusting for possible confounding factors. It was observed that higher concern for friends, acquaintances or neighbours, perceived health, and concern from spouse, increases satisfaction with life among female participants. In contrast, 26.3% of the variance for satisfaction with life among male participants could be explained by difficulty to have shower by themselves, smoking, being concern about health, having concern for friends, acquaintances or neighbours, walking as part of daily activity, leg pain and kidney problem. It was observed that smoking and having concern for friends, acquaintances or neighbours increases satisfaction with life among male participants.
Discussion
To the best of the authors’ knowledge, this is the first paper that reports gender differences of older adults in Brunei. This study discovered several important findings on gender differences among elderly person in Brunei in comparison with different countries worldwide. The rate of aging is rapidly comparable to Japan and Korea [29, 30]. First of all, elderly women generally show lower life satisfaction as they are not only susceptible to chronic illnesses and disabilities, but also receptive to burden associated with traditional female roles [31]. This is consistent, in the present study and previous studies [18, 19], where elderly women reported significantly lower life satisfaction than men. However, there is contradictory results revealed in several countries. In South Korea, elderly men reported lower life satisfaction than women [20]. In China, elderly women reported higher life satisfaction [21]. In Spain, life satisfaction is equally shared between men and women [3].
Life satisfaction is a complex, multi-dimensional phenomenon, and the differences based on gender could possibly be mediated by other predictors such as socioeconomic and sociocultural factors on gender roles, opportunities and disadvantages across life events [31]. In the present study, the highest predictor of life satisfaction among elderly women was positive self-perception of health, similar to a study in Brazil [31], together with other significant social factors including having concern for spouse friends, acquaintances or neighbours. In addition, we also revealed that women were still actively engaged in traditional gender roles such as care of children, household chores, and care of older relatives by themselves. Education level could also play an important part, where those with lower level of education were significantly more satisfied, which is congruent to a study in China [32] but in contrast to a study in Spain where higher education level contributed to higher life satisfaction [3]. For elderly men, there was overlapping predictors with women, however, major differences were variables more incline towards physical activities and abilities. The highest predictor of life dissatisfaction among men was difficulty to perform daily activities, particularly taking shower. In our results, men had significantly lower proportions of musculoskeletal pain or discomfort, and they generally were able to perform daily activities without assistance. This could explain why elderly men reported higher life satisfaction than female. In South Korea, elderly men reported lower level of physical health as well as lower social relationship, which had contributed to lower life satisfaction and increased mental health issues [20, 33].
Healthy aging is tightly intertwined with life satisfaction as shown in our results, similar to prior studies [34–36]. This is particularly evident for older women, as discussed above. The proportion of musculoskeletal discomfort as well as mental health and emotional conditions were significantly higher among older women. The high correlation between physical activity on mental health could explain this relationship. Previous studies have determined effects of exercise on mental health [37, 38], and the current Coronavirus disease 2019 (COVID-19) pandemic might deteriorate the situation further with mandated social isolation and restrictions on public movement [38]. The World Health Organization has recommended at least 150 min per week of moderate-intensity physical activity such as brisk walking and riding a bike, or at least 75 min per week of vigorous-intensity physical activity such as running or fast swimming, for older adults [39]. This include home-based physical activity such as aerobic exercises, bodyweight training, dance and active gaming to counter physical and mental side effects of COVID-19 regulations [40]. Furthermore, social participation has also been a critical indicator of positive health effects on older adults [5]. In Japan, a gender stratified analysis revealed that social participation improved physical and mental health of older women more than men, and overall benefits were recorded for both gender compared to non-participation [5]. Being active in various social activities such as sport groups, hobby clubs, gardening, recreational training, and so forth, have demonstrated positive effects in different older adults [5, 41, 42].
Moreover, in the present study, having more children were perceived as healthier among older men. Even though numerous studies have considered the association between health and number of children, very few have examined gender differences. We could only postulate that, in this population, older men may place importance in intergenerational transfers and support such as practical help and financial aid, while older women on emotional support and care [1]. Another reason might institute from culturally—what constitute healthy or successful aging—defined achievement. This could include pride of continuing the family line, as well as related benefits of self-esteem gained, economic and social security, that might outweigh burden of having fewer or no children such as continuing unwanted involvement in children’s lives, prolonged mental aggravations, and continuing financial demands from children [9].
The results of this study should be interpreted within its limitations. Cross-sectional nature of this study limits prospective causal inferences, and the self-reported data collected is subject to recall and reporting bias. In addition, the small sample size of this study limits generalizability to the study population. Even though we have investigated major domains of life satisfaction and healthy aging for older adults, future studies should include other dimensions that are no less salient such as spiritual experiences and perception of death [43] as well as emerging components such as gerontechnology and digital health, to provide a comprehensive and holistic approach towards successful aging.
In conclusion, this study has made large strides in understanding gender differences in life satisfaction and healthy aging, as well as providing epidemiologic estimates in socioeconomic status, physical health, mental and emotional conditions, and social health status for older men and women in Brunei. However, more efforts from policymakers and related stakeholders are still needed to close gender gaps among the older adults. This can be done by formulating appropriate and localized policies of ensuring living spaces, transportation, and communication services as well as community and other projects that can increase physical activity, social interaction and maintain relationships among older adults.
Data Availability Statement
The datasets generated and/or analysed during the current study are not publicly available due to institutional data sharing clause but are available from the corresponding author on reasonable request.
Ethics Statement
The studies involving human participants were reviewed and approved by the University Research Ethics Committee of Universiti Brunei Darussalam (UBD/OAVCR/UREC/Apr18-04). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
HR concept design, data analysis, writing, editing, and critical review manuscript, final approval, and consent to publish. AT study design, data collection, critical review, final approval, and consent to publish. YY study design, data collection, reviewed data analysis, critical review, final approval, and consent to publish. LS concept design, reviewed data analysis, critical review, final approval, and consent to publish. C-YH concept design, reviewed data analysis, critical review, final approval, and consent to publish. KA-M study design, data collection, critical review, final approval, and consent to publish.
Funding
This study was supported by the Faculty Block Funding of Centre for Advanced Research, Universiti Brunei Darussalam (UBD/RSCH/1.10/FICBF(b)/2018/004).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors would like to express sincere appreciation to all participants for their contribution and research assistants for collating the data.
References
1. Hämäläinen, H, and Tanskanen, AO. ‘Sandwich Generation’: Generational Transfers towards Adult Children and Elderly Parents. J Fam Stud (2019) 27(3):336–355. doi:10.1080/13229400.2019.1586562
2. Sato, Y, and Yanagita, M. The Unprecedented Era of Aging. Inflamm Regen (2019) 39(1):15. doi:10.1186/s41232-019-0104-2
3. Matud, MP, García, MC, and Fortes, D. Relevance of Gender and Social Support in Self-Rated Health and Life Satisfaction in Elderly Spanish People. Int J Environ Res Public Health (2019) 16(15):E2725. doi:10.3390/ijerph16152725
4. Kahn, JR, McGill, BS, and Bianchi, SM. Help to Family and Friends: Are There Gender Differences at Older Ages? J Marriage Fam (2011) 73(1):77–92. doi:10.1111/j.1741-3737.2010.00790.x
5. Tomioka, K, Kurumatani, N, and Hosoi, H. Positive and Negative Influences of Social Participation on Physical and Mental Health Among Community-Dwelling Elderly Aged 65–70 Years: a Cross-Sectional Study in Japan. BMC Geriatr (2017) 17(1):111. doi:10.1186/s12877-017-0502-8
6. Tomioka, K, Kurumatani, N, and Hosoi, H. Age and Gender Differences in the Association between Social Participation and Instrumental Activities of Daily Living Among Community-Dwelling Elderly. BMC Geriatr (2017) 17(1):99–10. doi:10.1186/s12877-017-0491-7
7. Corrao, S, Santalucia, P, Argano, C, Djade, CD, Barone, E, Tettamanti, M, et al. Gender-differences in Disease Distribution and Outcome in Hospitalized Elderly: Data from the REPOSI Study. Eur J Intern Med (2014) 25(7):617–23. doi:10.1016/j.ejim.2014.06.027
8. Kim, E-J, Jung, S-W, Kim, Y-E, Go, D-S, and Yoon, S-J. Assessing the Impact of Aging on Burden of Disease. Iran J Public Health (2018) 47:33–8. Available from: https://pubmed.ncbi.nlm.nih.gov/30186810.
9. Bocci, C, and Salvini, S. Elderly with and without Children: Do They Report Different Health Conditions? In: ASA CONFERENCE 2019 Statistics for Health and Well-being BOOK OF SHORT PAPERS; 2019 Sept 25–27; Brescia (2019).
10. Kämpfen, F, Wijemunige, N, and Evangelista, B. Aging, Non-communicable Diseases, and Old-Age Disability in Low- and Middle-Income Countries: a challenge for Global Health. Int J Public Health (2018) 63(9):1011–2. doi:10.1007/s00038-018-1137-z
12. Steptoe, A, Deaton, A, and Stone, AA. Subjective Wellbeing, Health, and Ageing. The Lancet (2015) 385(9968):640–8. doi:10.1016/s0140-6736(13)61489-0
13. Blanchflower, DG, and Oswald, AJ. The U-Shape without Controls: A Response to Glenn. Soc Sci Med (2009) 69(4):486–8. doi:10.1016/j.socscimed.2009.05.022
14. Blanchflower, DG, and Oswald, AJ. Is Well-Being U-Shaped over the Life Cycle? Soc Sci Med (2008) 66(8):1733–49. doi:10.1016/j.socscimed.2008.01.030
15. Blanchflower, DG, and Oswald, AJ. Well-being over Time in Britain and the USA. J Public Econ (2004) 88(7–8):1359–86. doi:10.1016/s0047-2727(02)00168-8
16. Baird, BM, Lucas, RE, and Donnellan, MB. Life Satisfaction Across the Lifespan: Findings from Two Nationally Representative Panel Studies. Soc Indic Res (2010) 99(2):183–203. doi:10.1007/s11205-010-9584-9
17. Puvill, T, Lindenberg, J, de Craen, AJM, Slaets, JPJ, and Westendorp, RGJ. Impact of Physical and Mental Health on Life Satisfaction in Old Age: a Population Based Observational Study. BMC Geriatr (2016) 16(1):194. doi:10.1186/s12877-016-0365-4
18. Jovanović, V, and Joshanloo, M. The Determinants of Life Satisfaction in Serbia: Findings from the Gallup World Poll. Intnl J Wellbeing (2019) 9(1):43–60. doi:10.5502/ijw.v9i1.751
19. George, LK. Still Happy After All These Years: Research Frontiers on Subjective Well-Being in Later Life. J Gerontol B Psychol Sci Soc Sci (2010) 65B(3):331–9. doi:10.1093/geronb/gbq006
20. Park, JH, Min, S, Eoh, Y, and Park, SH, The Elderly Living in Single-Person Households in South Korea: a Latent Profile Analysis of Self-Esteem, Life Satisfaction, and Depression. Qual Life Res (2020), 30, 1083–92. doi:10.1007/s11136-020-02693-1
21. Ng, ST, Tey, NP, and Asadullah, MN. What Matters for Life Satisfaction Among the Oldest-Old? Evidence from China. PLoS One (2017) 12(2):e0171799. doi:10.1371/journal.pone.0171799
22.United NationsDepartment of Economic and Social Affairs. World Population Ageing 2019. In: World Population Ageing 2019 Highlights. United Nation (2019). p. 5–11.
23. Levine, ME. Modeling the Rate of Senescence: Can Estimated Biological Age Predict Mortality More Accurately Than Chronological Age? J Gerontol A Biol Sci Med Sci (2013) 68(6):667–74. doi:10.1093/gerona/gls233
24.World Health Organization. Ageing (2022). Available from: https://www.who.int/health-topics/ageing#tab=tab_1 (Accessed July 1, 2022).
25.United Nation. New Measure of Population (2022). Available from: https://www.un.org/development/desa/pd/sites/www.un.org.development.desa.pd/files/unpd_egm_201902_s1_sergeischerbov.pdf (Accessed July 1, 2022).
26.The United Nation Refugee Agency. Older Persons (2022). Available from: https://emergency.unhcr.org/entry/43935/older-persons (Accessed July 1, 2022).
27.Centers for Disease Control and Prevention. Chronic Disease Indicators: Older Adults (2022). Available from: https://www.cdc.gov/cdi/definitions/older-adults.html#OLD3_2 (Accessed July 1, 2022).
28. Naing, L, Winn, T, and Rusli, BN. Practical Issues in Calculating the Sample Size for Prevalence Studies. Arch Orofac Sci (2006) 1:9–14.
29. Othman, A. Brunei to Exceed Japan in Ageing Population by 2065 (2020). Available from: https://borneobulletin.com.bn/brunei-exceed-japan-ageing-population-2065 (Accessed July 1, 2022).
30. Lovanxay, B. ICT as One of the Critical success Factors of Aging Society in ASEAN: Role and Cooperation of Japan. In: Proceedings of the 8th International Conference on Theory and Practice of Electronic Governance; 2014 Oct 27–30; Guimaraes, Portugal (2014). 510–1.
31. Pinto, JM, Fontaine, AM, and Neri, AL. The Influence of Physical and Mental Health on Life Satisfaction Is Mediated by Self-Rated Health: A Study with Brazilian Elderly. Arch Gerontol Geriatr (2016) 65:104–10. doi:10.1016/j.archger.2016.03.009
32. Pan, Y, Chan, SHW, Xu, Y, and Yeung, KC. Determinants of Life Satisfaction and Self-Perception of Ageing Among Elderly People in China: An Exploratory Study in Comparison between Physical and Social Functioning. Arch Gerontol Geriatr (2019) 84:103910. doi:10.1016/j.archger.2019.103910
33. Kang, J-P, and Yoon, J. A Study on Multi-Level Models in Life Satisfaction of Elderly Living Alone: Moderating Effect of Elderly’s Leisure Activity and Social Support. J Digit Converg (2017) 15(5):89–98.
34. Ghimire, S, Baral, BK, Karmacharya, I, Callahan, K, and Mishra, SR. Life Satisfaction Among Elderly Patients in Nepal: Associations with Nutritional and Mental Well-Being. Health Qual Life Outcomes (2018) 16(1):118. doi:10.1186/s12955-018-0947-2
35. Mehr, MM, Zamani-Alavijeh, F, Hasanzadeh, A, and Fasihi, T. Effect of Healthy Lifestyle Educational Programs on Happiness and Life Satisfaction in the Elderly: A Randomized Controlled Trial Study. Salmand (2019) 13(4):440–51. doi:10.32598/sija.13.4.440
36. Park, C-S, and Park, S-Y. Life Satisfaction of Elderly Living Alone Based on Their Physical, Mental and Subjective Oral Health Status. Korean J Heal Serv Manag (2016) 10(2):167–77. doi:10.12811/kshsm.2016.10.2.167
37. Battaglia, G, Bellafiore, M, Alesi, M, Paoli, A, Bianco, A, and Palma, A. Effects of an Adapted Physical Activity Program on Psychophysical Health in Elderly Women. Clin Interv Aging (2016) 11:1009–15. Available from: https://pubmed.ncbi.nlm.nih.gov/27536081. doi:10.2147/CIA.S109591
38. Callow, DD, Arnold-Nedimala, NA, Jordan, LS, Pena, GS, Won, J, Woodard, JL, et al. The Mental Health Benefits of Physical Activity in Older Adults Survive the COVID-19 Pandemic. Am J Geriatr Psychiatry (2020) 28(10):1046–57. doi:10.1016/j.jagp.2020.06.024
40. Hammami, A, Harrabi, B, Mohr, M, and Krustrup, P. Physical Activity and Coronavirus Disease 2019 (COVID-19): Specific Recommendations for home-based Physical Training. Manag Sport Leis. 27 2020: 26- 31. doi:10.1080/23750472.2020.1757494
41. Sanches, A, Guzzoni, V, Miranda Vc dos, R, Peressim, LB, Rocha, S, de Lima, PO, et al. Recreational Training Improves Cardiovascular Adaptations, Metabolic Profile and Mental Health of Elderly Women with Type-2 Diabetes Mellitus. Health Care Women Int (2020) 42:1279–97. doi:10.1080/07399332.2020.1821689
42. Park, S-A, Lee, A-Y, Son, K-C, Lee, W-L, and Kim, D-S. Gardening Intervention for Physical and Psychological Health Benefits in Elderly Women at Community Centers. Horttechnology (2016) 26(4):474–83. doi:10.21273/horttech.26.4.474
Keywords: older adults, predictors, gender, life satisfaciton, healthy ageing, Brunei
Citation: Abdul Rahman H, Tengah A, Mohd Yusof Y, Slesman L, Hoon C-Y and Abdul-Mumin KH (2022) Predictors of Satisfaction With Life and Health Status of Older People in Brunei: A Gender Comparative Study. Int J Public Health 67:1605042. doi: 10.3389/ijph.2022.1605042
Received: 30 April 2022; Accepted: 26 July 2022;
Published: 25 August 2022.
Edited by:
Nino Kuenzli, Swiss Tropical and Public Health Institute (Swiss TPH), SwitzerlandReviewed by:
Başaran Gençdoğan, Atatürk University, TurkeyAdesola Ojo Ojoawo, Obafemi Awolowo University, Nigeria
Copyright © 2022 Abdul Rahman, Tengah, Mohd Yusof, Slesman, Hoon and Abdul-Mumin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hanif Abdul Rahman, aGFuaWYucmFobWFuQHViZC5lZHUuYm4=
This Original Article is part of the IJPH Special Issue “Health in all Sustainable Development Goals.”