 Gabriela P. Peralta1†
Gabriela P. Peralta1† Anne-Linda Camerini2†
Anne-Linda Camerini2† Sarah R. Haile1
Sarah R. Haile1 Christian R. Kahlert3,4
Christian R. Kahlert3,4 Elsa Lorthe5Laura Marciano2,6Andres Nussbaumer4
Elsa Lorthe5Laura Marciano2,6Andres Nussbaumer4 Thomas Radtke1Agne Ulyte1
Thomas Radtke1Agne Ulyte1 Milo A. Puhan1‡
Milo A. Puhan1‡ Susi Kriemler1*‡
Susi Kriemler1*‡- 1Epidemiology, Biostatistics and Prevention Institute (EBPI), University of Zurich, Zurich, Switzerland
- 2Institute of Public Health, Università della Svizzera Italiana, Lugano, Switzerland
- 3Department of Infectious Diseases and Hospital Epidemiology, Children’s Hospital of Eastern Switzerland, St. Gallen, Switzerland
- 4Department of Infectious Diseases and Hospital Epidemiology, Cantonal Hospital St. Gallen, St. Gallen, Switzerland
- 5Unit of Population Epidemiology, Department of Primary Care Medicine, Geneva University Hospitals, Geneva, Switzerland
- 6Harvard T. H. Chan School of Public Health and Dana-Farber Cancer Institute, Boston, MA, United States
Objectives: To describe changes in adherence to recommendations for physical activity (PA), screen time (ST), and sleep duration over the first two waves of the pandemic in Switzerland, and to assess the associations of these lifestyle behaviours with life satisfaction and overall health as well-being indicators.
Methods: In this observational study, we included 2,534 participants (5–16 years) from four Swiss cantons. Participants, or their parents, completed repeated questionnaires and reported on their (child’s) lifestyle and well-being, between June 2020 and April 2021. We used linear and logistic regression models to assess the associations between lifestyle and well-being.
Results: The percentage of children meeting the recommendations for PA and ST decreased from the pre-pandemic period to the first wave, with a slight recovery during the second wave. Participants meeting all three recommendations during the second wave were more likely to report excellent health (OR: 1.65 [95% CI: 1.00–2.76]) and higher life satisfaction (β: 0.46 [0.16–0.77]) in early 2021 than participants not meeting any recommendation.
Conclusion: We showed a substantial impact of the COVID-19 pandemic on children’s and adolescents’ lifestyle, and a positive association between meeting lifestyle recommendations and well-being.
Introduction
Lifestyle, including screen time (ST), physical activity (PA), and sleep, is a key predictor of physical and emotional well-being in children and adolescents [1–3]. Thus, understanding how lifestyle behaviours have changed as the COVID-19 pandemic and its related restrictive measures evolved, is of utmost relevance. Like many countries, the Swiss government imposed a lockdown between March and May 2020 [4]. During that period, classroom teaching was interrupted, and then continued with a partial return to class (i.e., alternating face-to-face and online classes) until the start of the summer break. In August 2020, schools reopened as normal, though with continued prevention measures (e.g., mask wearing, class level quarantine following a single positive case) in place. In autumn and early winter 2020, Switzerland experienced a second wave with one of the highest infections rates worldwide [5]. Although classroom teaching in primary and secondary education was still secured, sports clubs, gyms, and other leisure institutions were closed to some extent (i.e., open only for children under age 16 years) or had restrictions in place, such as no mixing of groups, small group sizes and the banning of sports competitions until early 2021 [6]. Following the decrease of infections, in March 2021 most restrictions were lifted and all extracurricular activities such as rehearsals and training for cultural and sports activities were permitted without restrictions for children and adolescents [6].
There is substantial evidence showing that COVID-19 restrictions during the first wave in spring 2020 resulted in a drastic reduction of PA and an increase in ST among children and adolescents, as well as in a delay of sleep onset and offset resulting in a subtle increase of sleep duration [7]. Also, studies conducted during the pandemic reported an association between changes in lifestyle behaviours and well-being. Maintaining adequate levels of PA was associated with better well-being, while higher levels of ST were related to decreased emotional well-being [8–11], which is in line with research from the pre-pandemic period [1, 12]. However, an important limitation of previous research is the fact that most studies evaluated lifestyle changes only during the period when strict lockdown measures were in place. Very few studies extended their assessment beyond June 2020 [10, 13, 14], and only one small (n = 19) longitudinal study assessed lifestyle changes up to 2021 [15]. In addition, studies assessing the associations between lifestyle behaviours and well-being before and during the pandemic were mostly based on a single-behaviour approach and assessed time dedicated to each behaviour rather than adherence to (inter-)national recommendations for children and adolescents [16–18]. There is pre-pandemic evidence supporting that meeting recommendations for more than one lifestyle behaviour is more beneficial for children’s and adolescents’ health and development than meeting the recommendations for a single behaviour [19–22]. A recent study using pre-pandemic data reported that a combination of lower ST and higher PA appears to have joint and positive associations with mental well-being in adolescents [23]. However, the study could not account for the contribution of sleep duration to this association.
Therefore, we aimed to describe changes in adherence to international recommendations for PA, ST, and sleep duration over the first two waves of the COVID-19 pandemic (March–May 2020 and October 2020–January 2021) in children and adolescents aged 5–16 years, and to assess the combined associations of these lifestyle behaviours with overall health and life satisfaction in early 2021.
Methods
Study Design and Participants
This observational study is part of Corona Immunitas, a research network that investigates the spread and impact of COVID-19 pandemic in Switzerland [24]. We included children and adolescents from four Swiss cantons participating in this network: Ticino (TI), St. Gallen (SG), Graubünden (GR), and Zurich (ZH), which collected data on lifestyle behaviours and well-being at similar time points during the pandemic. These cantons belong to three out of four language regions (German, Italian and Romansch) in Switzerland and comprise 30% of the Swiss population [25]. In TI, SG, and GR, participants were recruited based on a representative sample of children and adolescents drawn from the Swiss Federal Registry. In ZH, the data came from the Ciao Corona study [26], a cohort of school-aged children from 55 schools. Primary schools were randomly selected from the list of all schools in the canton of ZH and matched with the geographically closest secondary school.
Out of a sample of 3,458 eligible children and adolescents, we included 2,534 participants aged 5–16 years with the first assessment completed between June 2020 and January 2021 and follow-up assessments between January and April 2021, and who provided data on lifestyle behaviours and well-being measures (Supplementary Figure S1). In ZH, parents were asked to complete the questionnaires together with their child. In the other three cantons, parents completed the questionnaires for children aged 5–13 years, while adolescents aged 14–16 years completed the questionnaires on their own. See further details on participant recruitment and data collection in the Supplementary Material.
The study was approved by the Ethics Committee of all cantons (TI: 2020-01514; SG/GR: 2020-01247; ZH: 2020-01336). All participants and/or their parents provided informed consent.
Measures
Lifestyle
In all cantons, PA, ST, and sleep for the period before the pandemic (i.e., before March 2020) and during the lockdown in the first wave (i.e., between 16 March and 10 May 2020) were assessed retrospectively in the first assessment. Participants from TI, GR and GR reported on their lifestyle for the period during the second wave (i.e., between October 2020 and January 2021) also in the first assessment, while in ZH this was reported in a separate assessment (Figure 1).
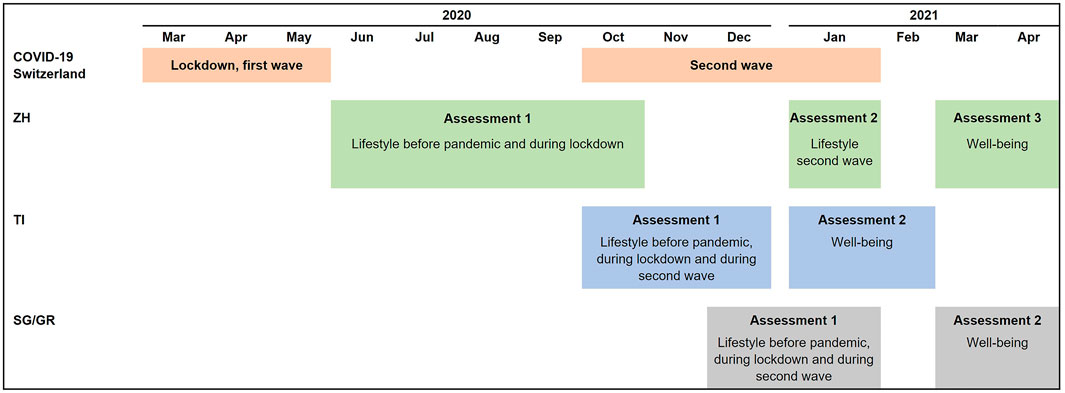
FIGURE 1. Details on data collection per canton (Corona Immunitas, Switzerland, 2020–2021). Abbreviations: GR, Graubünden: SG, St. Gallen; TI, Ticino; ZH, Zurich. In TI, SG and GR, participants completed questionnaires following a rolling enrolment. Therefore, participants were invited to the second assessment 3 months after the first assessment.
PA was assessed by asking how many hours per week, on average, participants spent with PA (at least with light sweating). Weekly hours were converted to daily hours. ST was assessed by asking how many hours, on average, participants spent with electronic media (e.g., smartphone, computer, PlayStation, Xbox, Nintendo, TV) on a typical weekday and on a typical weekend day. Sleep was assessed by asking how many hours, on average, participants slept on a typical weekday and on a typical weekend day. For ST and sleep, we calculated a weighted average as follows: [(weekday*5) + (weekend day*2)]/7. The questions were similar to those used in previous studies assessing lifestyle in children and adolescents [19]. The exact wording of the questions can be found in Supplementary Table S1.
For each time-point, i.e., before the pandemic, during the first wave, and during the second wave, we analysed lifestyle in terms of adherence to international recommendations: ≥1 h/day of PA, ≤2 h/day of ST, and age-specific sleep duration (10–13 h/night for 5 years; 9–11 h/night for 6–13 years; 8–10 h/night for 14–16 years) [16–18]. We also grouped participants into one of the following recommendation adherence patterns: none, PA only, sleep only, ST only, PA and sleep, PA and ST, sleep and ST, and all three.
Well-Being
We measured current life satisfaction and overall health as indicators of well-being in a follow-up assessment between January and April 2021. This was the second assessment in TI, SG and GR and the third assessment in ZH. Well-being was thus measured two to 3 months after the assessment of lifestyle behaviours with reference to the second wave (Figure 1).
We assessed life satisfaction with the Cantril ladder [27], a visual scale for rating how children and adolescents perceive their life on a 11-point scale ranging from “0-the worst possible life” to “10-the best possible life.” We assessed overall health by asking “How would you rate your/your child’s health?” Respondents were asked to describe their (child’s) health status on a scale from “1-poor” to “4-excellent.”
Both items have been widely used in epidemiological research [28, 29]. We analysed life satisfaction as a continuous variable and overall health as a binary variable (“excellent” vs. lower ratings).
Covariates
We collected participants’ sex, age, height, and weight in the first assessment. We also collected information on parents’ nationality (at least one Swiss; both non-Swiss) and educational level (high: at least one with preparatory high school to university; low/medium: both up to apprenticeship or professional school). We used height and weight to derive age- and sex-specific body mass index (BMI) z-scores by using the World Health Organization child growth standards, and categorised it as underweight, normal weight, and overweight according to the guidelines [30]. We categorised participants’ age according to stages of development: 5–9 years, 10–12 years, and 13–16 years [31]. The three age-groups cover primary school-aged children, tweens, and teens, respectively.
Statistical Analysis
Changes in lifestyle behaviours during the first and second waves were analysed by descriptive statistics, stratified by age category. We calculated 95% confidence intervals for percentages using the Wilson method [32]. In supplementary analyses, we also stratified changes by sex and analysed lifestyle behaviours as continuous variables.
We analysed the associations of the number of recommendations met and the adherence patterns during the second wave with overall health and life satisfaction in early 2021 using multivariable logistic and linear regression, respectively. We adjusted the models for child’s sex, age category, BMI category, parents’ nationality, parents’ educational level, completion of the questionnaire by parents (i.e., parent report) and canton. To account for previous lifestyle, we also adjusted the models for the number of recommendations met/adherence patterns before the pandemic and during the lockdown of the first wave. We tested interactions between lifestyle behaviours at the second wave and age category. However, the Akaike information criterion and the p-value for the likelihood ratio test comparing models with and without interactions indicated that models without interactions fit the data best (data available on request). p-values for the adjusted models were interpreted according to levels of significance, as previously recommended [33].
Missing data were reported in the Table 1 and Supplementary Table S2 footnotes. We performed the statistical analysis in R (version 4.0.3) [34] and used ggplot2 [35] and patchwork [36] packages to produce graphs.
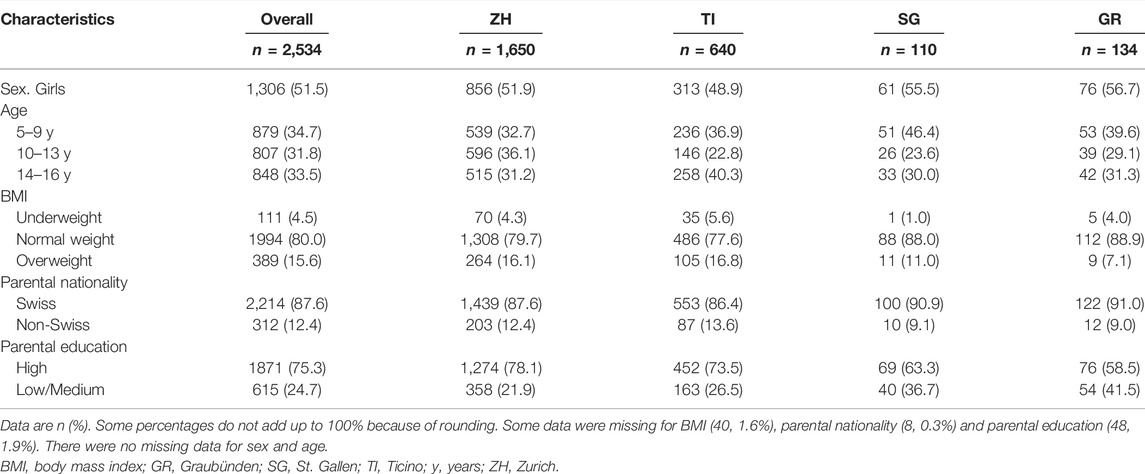
TABLE 1. Characteristics of the study sample (Corona Immunitas, Switzerland, 2020–2021).
Results
Description of the Study Sample
We included 2,534 children and adolescents Compared to the study sample, children and adolescents excluded from the analyses were more likely to have both parents of non-Swiss origin and with low/medium education level (Supplementary Table S2). Table 1 shows the main characteristics of the study sample. Most participants had a normal BMI (80%), at least one Swiss parent (87.6%) and at least one parent with high education level (75.3%).
In the follow-up assessment between January and April 2021, 43% of participants reported excellent health. The median life satisfaction score was 8.0 (P25–P75: 7.0–9.0). Older adolescents (13–16 years) were less likely to report excellent health and had a lower median life satisfaction than younger participants (Table 2).

TABLE 2. Description of participants’ well-being measures between January and April 2021 by age group (Corona Immunitas, Switzerland, 2020–2021).
Changes in PA, ST, Sleep, and Number of Recommendations met
Across all age groups, we observed a decrease in the percentage of participants meeting the individual recommendations for PA and ST between the pre-pandemic period and the lockdown period (Figure 2; Supplementary Table S3). While these percentages tended to increase during the second wave, they remained below the pre-pandemic levels among the 10- to 12-year-olds and the 13- to 16-year-olds. In the 5- to 9-year-olds, PA levels, too, remained below the pre-pandemic level, but the percentage of children in that age group meeting the recommendations for ST returned to levels observed for the pre-pandemic period. Adherence to recommendations for sleep also changed over time but the pattern was less consistent among age groups. Among the 10- to 12-year-olds and the 13- to 16-year-olds, the percentage of compliant participants increased slightly during the lockdown, but during the second wave it was lower than before the pandemic. For the 5- to 9-year-olds, the percentage of compliant children tended to remain stable.
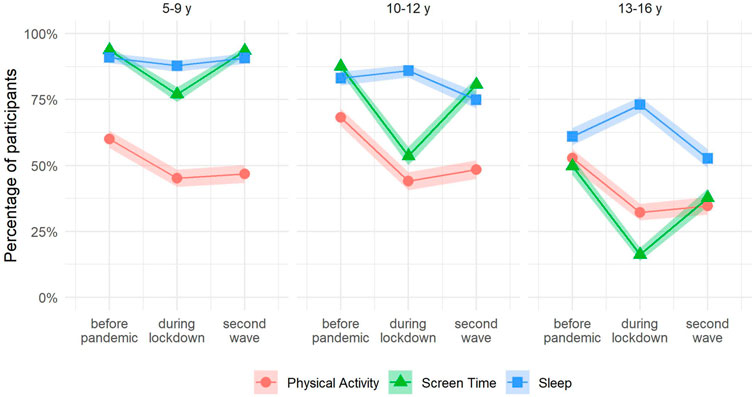
FIGURE 2. Prevalence of participants meeting recommendations for physical activity, screen time and sleep duration by age group (Corona Immunitas, Switzerland, 2020–2021). Abbreviations: PA, physical activity; sleep, sleep duration; ST, screen time; y, years. Time points: before pandemic: before March 2020; during lockdown: between 16 March and 10 May 2020; second wave: between October 2020 and January 2021. Shaded area represents 95% confidence intervals. We classified participants as meeting recommendations according to international guidelines: ≥1 h/day of PA, ≤2 h/day of ST, and the recommended range by age-groups for sleep duration (i.e., 10–13 h/nigh of sleep for age 5 years, 9–11 h/night for ages 6–13 years, 8–10 h/night for ages 14–16 years).
The percentage of participants meeting all three recommendations decreased during the lockdown period and increased again during the second wave (Figure 3; Supplementary Table S4). Yet, it remained below the percentages observed for the pre-pandemic period. At all-time points, the 13- to 16-year-olds reported the highest percentage of participants not meeting any of the recommendations.
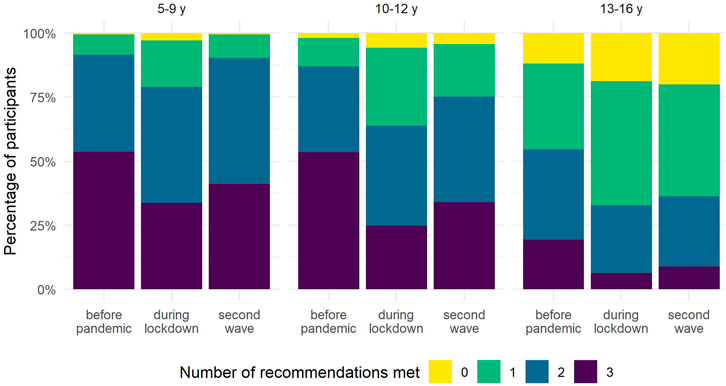
FIGURE 3. Number of recommendations met by age group (Corona Immunitas, Switzerland, 2020–2021). Abbreviations: y, years. Time points: before pandemic: before March 2020; during lockdown: between 16 March and 10 May 2020; second wave: between October 2020 and January 2021.
We observed a similar pattern of change for boys and girls (Supplementary Figures S2, S3). For all age groups and time points, girls were less likely to meet PA recommendations. We observed a similar trend in changes using lifestyle behaviours as continuous variables as described when categorising the variables in terms of adherence to the recommendations (Supplementary Tables S5, S6).
Associations of Number of Recommendations Met and Adherence Patterns With Well-Being
Table 3 shows the adjusted associations of recommendations met and adherence patterns measured with reference to the second wave with well-being between January and April 2021 (unadjusted associations are presented in Supplementary Table S7). We found that participants meeting recommendations for PA, ST, and sleep during the second wave were almost twice as likely to report excellent health (OR: 1.65, 95% CI: 1.00 to 2.76, p-value: 0.054), though the association was weak. Furthermore, those meeting recommendations for all three lifestyle behaviours had, on average, a 0.46 (95% CI: 0.16 to 0.77, p-value: 0.003) unit higher life satisfaction score than those not meeting any recommendation. The ORs for excellent health and the regression coefficients for life satisfaction increased relative to the number of recommendations met (Table 3).
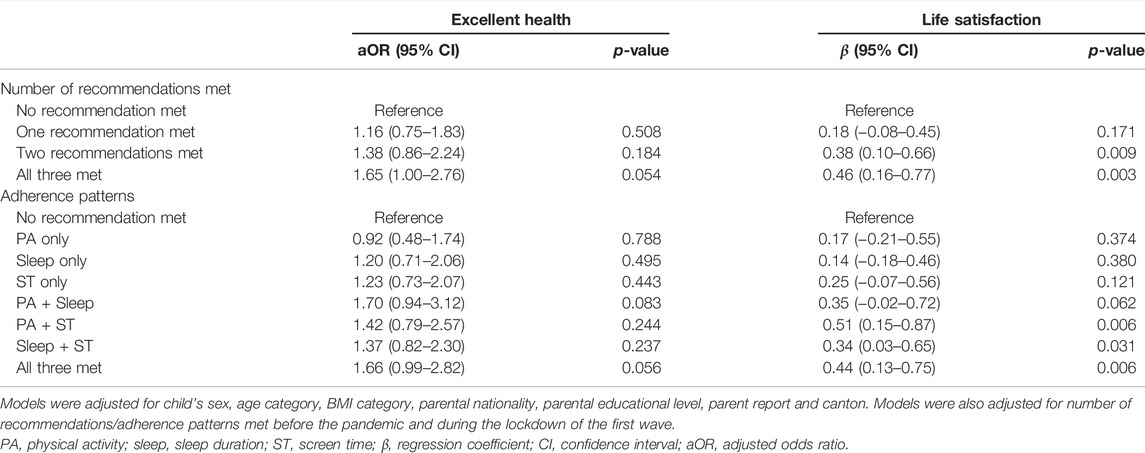
TABLE 3. Adjusted associations of number of recommendations met and adherence patterns during the second wave of the pandemic with well-being in early 2021 (Corona Immunitas, Switzerland, 2020–2021).
We also observed an association between adherence patterns of lifestyle behaviours during the second wave and well-being in early 2021 (Table 3). In addition to participants meeting the recommendations for all three lifestyle behaviours, participants meeting recommendations for PA and sleep, PA and ST, and sleep and ST had higher average life satisfaction scores than those not meeting any recommendation. We observed a similar pattern for self-reported health, but evidence for an association with the combination of PA and sleep was weak, and there was little evidence for an association with the rest of combinations of lifestyle behaviours.
Discussion
In this observational study, we found that the first two waves of the COVID-19 pandemic affected lifestyle behaviours in 5- to 16-year-olds in Switzerland. During the lockdown period between March and May 2020, the percentage of children and adolescents meeting the recommendations for PA and ST decreased notably. Although it partially recovered during the second wave of the pandemic between October 2020 and January 2021, the percentage remained below the pre-pandemic period, especially for PA and for those aged 10 years or older. Changes in sleep duration were less marked and they were heterogeneous among age groups. Furthermore, we found an association between the number of recommendations met for lifestyle behaviours during the second wave and well-being assessed between January and April 2021. Participants meeting the recommendations for all three lifestyle behaviours or for combinations of two of them in the second wave had a higher life satisfaction score and were more likely to report excellent health, than those not meeting any recommendation.
Our findings of worsened lifestyle behaviours during the lockdown period are in line with previous cross-sectional and longitudinal studies in children and adolescents [7]. In contrast to previous studies, we did not only analyse early phases of the pandemic but extended our assessment until early 2021. This allowed us to show that, despite the reopening of schools and extracurricular activities for children and adolescents up to 16 years of age, children and adolescents continued to have a more sedentary lifestyle during the second wave of the pandemic compared to the pre-pandemic period, but partially recovered from strict containment measures during the lockdown period. During the second wave, schools were open and classroom teaching was secured for primary and secondary students, which probably played an important role in the reduction of ST during that period. However, since extracurricular activities such as sports training continued to have strict restrictions on place including reduced times and numbers of participants, the options to be physically active were still limited, especially indoors and during the winter months. In addition, due to the high incidence of cases during the second wave, parents may have felt less confident letting their children participate in group or indoor activities. Also, it is possible that the increase in screen-related leisure activities resulted in the reduction of PA at least in part, as evidenced by the negative association between total ST and PA [37]. The shift towards a more sedentary lifestyle during the pandemic, despite some recovery during the second wave, is of concern for children’s and adolescents’ health and development. A cohort study of children in Austria reported that COVID-19 mitigation measures in 2020 were associated with an increase in the proportion of children with overweight and in a reduction of cardiorespiratory fitness [38], which may be partially explained by the reduction of PA and a concomitant increase in sedentary behaviour. Another study in school-aged children in China showed that home confinement during the pandemic was associated with an increase in the prevalence of myopia likely due to significantly decreased time spent outdoors and increased ST [39]. It is also worrying that the pandemic exacerbated the sedentary lifestyle of older adolescents. Only a small percentage of adolescents aged 13–16 years, met recommendations for PA and ST before the pandemic, and even a lower percentage met recommendations for all three lifestyle behaviours. Restrictions during the lockdown period resulted in only 32% and 16% of older adolescents complying with PA and ST recommendations, respectively. The shift towards an even more sedentary lifestyle during the pandemic may place adolescents at an increased risk for deleterious long-term health effects such as cardio-metabolic risk and mental health problems.
We found that the pandemic also led to a change in adherence to recommendations for sleep in adolescents, but not in children aged 5–9 years. During the lockdown, the percentage of adolescents aged 10–12 and 13–16 years meeting the recommendations for sleep was slightly higher than before the pandemic, consistent with previous literature [40]. In contrast, during the second wave, the percentage of compliant adolescents was lower than in the pre-pandemic period. This reduction may be explained by the increase in ST. Previous research reported that adolescents who spent more time on screens slept fewer hours, primarily due to time spent on portable devices such as phones, which proved to delay sleep onset [41]. During the lockdown period, the irregular timetable and the absence of travel to school, may have allowed the delay in sleep time to be compensated by a later waking time, resulting in an overall increase in sleep duration. However, it is likely that this compensation may not have been possible during the second wave due to the return to a more stable schedule while schools were kept open.
In our population, lifestyle was associated with two indicators of well-being, self-rated health and life satisfaction, which is consistent with previous research conducted before [1, 12, 23] and during the pandemic [8–10]. In contrast to previous studies, we accounted for the combined associations of PA, ST, and sleep duration with well-being, and demonstrated that meeting recommendations for all three behaviours as well as for combinations of two of them is more relevant for achieving optimal well-being than meeting recommendations for just a single behaviour. Evidence for an association with number of recommendations met and adherence patterns was stronger for life satisfaction than for self-reported health. Our findings support previous literature showing a dose-response relationship between lifestyle behaviours and physical health or global cognition [19, 20]. Importantly, lifestyle behaviours during the second wave were associated with well-being in early 2021, even after accounting for lifestyle before the pandemic and during the lockdown of the first wave. This suggests that well-being in children and adolescents is associated with recent lifestyle behaviours and thus likely fluctuating as these behaviours change. To note, well-being was assessed in a separate follow-up questionnaire two to 3 months after the assessment of lifestyle behaviours during the second wave, thus ruling out potential bias attributable to cross-sectional designs. The fact that schools were open during the second wave of the pandemic as well as at the time when well-being was assessed (i.e., early 2021) may have played an important role in the observed associations. Schools, as well as leisure facilities, not only have an important role in promoting healthy lifestyle behaviours but are also essential to promote children’s and adolescents’ mental health and well-being [42].
Future Directions for Practice and Research
Given the already high prevalence of children and adolescents not meeting lifestyle recommendations in the pre-pandemic period and the worsening during the pandemic in 2020, public health policies aiming to avoid permanent changes in lifestyle and negative long-term consequences associated with adverse changes during the pandemic are needed. Our findings suggest that the drastic changes in lifestyle behaviour during the early pandemic may have been partially recovered with the lifting of pandemic related restrictions. However, variability in recovery may be large and put those not meeting lifestyle recommendations before the pandemic at even higher risk for health problems. Future research should test intervention strategies to revert lifestyle changes using specific approaches for different age groups, especially for adolescents and children with high-risk behaviours (i.e., insufficient PA and/or sleep, and high media use). In addition, it is important that future studies make a special effort to include families from low socioeconomic status and collect information on socioeconomic factors that may influence the association between lifestyle behaviours and well-being such as parental working conditions or availability of green spaces nearby. Children and adolescents with a low socioeconomic status are likely to have a more sedentary lifestyle and more mental health problems than those from affluent families [43, 44]. Therefore, it is possible that these children and adolescents are more affected by restrictions in their daily life activities. Finally, future research should assess the long-term consequences of the pandemic on lifestyle behaviours and extend the assessment to the period when all restrictions are lifted and, eventually, after the pandemic.
Strengths and Limitations
The strengths of this study are the large sample size and the broad age range of the study sample, which allowed us to assess changes in lifestyle behaviours separately for different age groups. The inclusion of children and adolescents from four geographically and culturally different cantons of Switzerland support the external validity of our results, although we recognise that this is not a truly population-based study. In addition, the availability of measurements of lifestyle behaviours with reference to three time-points (i.e., pre-pandemic, lockdown, and second wave) allowed us to characterize changes over time and the partial recovery with the relief of pandemic related restrictions. Finally, as we had data for PA, ST and sleep, we were able to assess the associations between these lifestyle behaviours alone and in combination with well-being measured in early 2021.
However, we also need to acknowledge some limitations. Lifestyle behaviours were self-reported or based on parental-report. Also, these factors were assessed retrospectively for the period before the pandemic and during the lockdown of the first wave and the length of recall was different for each canton. Therefore, there is a potential bias in the estimation of PA, ST, and sleep. The slight differences in the formulation of the questions to assess lifestyle behaviours is another limitation. In ZH, questions for PA referred to hours per day (instead of hours per week), which could have led to an overestimation of PA for this subgroup. In addition, we did not collect data on frequency of PA or type of ST, although it has been suggested that both of these factors play a role on children’s and adolescents’ mental health [45, 46]. Furthermore, well-being indicators were also reported by parents for younger children and therefore some bias is possible for these measures, though we adjusted models for parent report. The fact that participants included in the study were more often from families with Swiss nationality and a high education level than those excluded due to missing data may not allow the generalizability of our results to populations with more ethnic variability and lower socio-economic status. Finally, although we accounted for a wide range of potential confounders when assessing the associations between lifestyle and well-being, residual confounding may still be a concern as we did not consider other factors such as COVID-19 infections, existing psychological problems, social isolation, parental working conditions, mental health or family cohesion, some of which were likely to change over the course of the pandemic Future studies should repeatedly assess and model covariates that are subject to change to evaluate their influence on the association between lifestyle and well-being in children and adolescents.
Conclusion
In conclusion, our findings demonstrate that the COVID-19 pandemic has had a negative effect on children’s and adolescents’ lifestyle behaviours, but some recovery has taken place within the first year since the outbreak. Policymakers and school managers should tease out the balance of disease prevention and promotion of a healthy lifestyle when (re-)activating restrictive measures. In addition, our study indicates that lifestyle is an important predictor of children’s and adolescents’ well-being, and it further suggests that future public health strategies aiming to promote well-being should target sufficient time for PA and sleep as well as reduce ST.
Ethics Statement
The studies involving human participants were reviewed and approved by the Ethics Committee of the cantons of Ticino (2020-01514), St. Gallen/Graubünden (2020-01247) and Zurich (2020-01336), Switzerland. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Author Contributions
SK, MP, A-LC, and CK conceived the study. A-LC, CK, AN, TR, AU, and SK recruited study participants, collected and managed the data. SH analysed the data. A-LC, AN, GP accessed and verified the data. GP wrote the first draft. All authors contributed to the design of the study, the interpretation of results and revised and approved the manuscript for intellectual content. All authors confirm that they had full access to all the data in the study and accept responsibility to submit for publication.
Funding
This study is part of the Corona Immunitas research network, coordinated by the Swiss School of Public Health (SSPH+), and funded by fundraising of SSPH+ that includes funds of the Swiss Federal Office of Public Health and private funders (ethical guidelines for funding stated by SSPH+ were respected), by funds of the cantons of Switzerland (Vaud, Zurich, and Basel), and by institutional funds of the Universities. The Ciao Corona study (ZH) received additional funding from the University of Zurich Foundation. The funders were not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank the Swiss Federal Statistical Office for providing the randomized list of participants. We thank SSPH+ for their help with coordination of all study sites. We also thank the ‘‘Volkschulamt” of the canton of Zurich for providing us with the comprehensive list of all schools and classes of the canton for the Ciao Corona study, and the supportive collaboration of school principals and teachers. In addition, we would like to thank all nurses, medical students, researchers, clinicians, and staff that contributed to the implementation of Corona Immunitas. Finally, we truly thank all children, adolescents, and their parents for their willingness to participate in this study. The present study was published as a preprint in MedRxiv before submission to the International Journal of Public Health (GP, A-LC, SH, CK, EL, LM, et al. Lifestyle behaviours of children and adolescents during the first two waves of the COVID-19 pandemic in Switzerland and their relation to well-being: a population-based study [47].
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.ssph-journal.org/articles/10.3389/ijph.2022.1604978/full#supplementary-material
References
1. Rodriguez-Ayllon, M, Cadenas-Sánchez, C, Estévez-López, F, Muñoz, NE, Mora-Gonzalez, J, Migueles, JH, et al. Role of Physical Activity and Sedentary Behavior in the Mental Health of Preschoolers, Children and Adolescents: A Systematic Review and Meta-Analysis. Sports Med (2019) 49:1383–410. doi:10.1007/s40279-019-01099-5
2. Hoare, E, Milton, K, Foster, C, and Allender, S. The Associations between Sedentary Behaviour and Mental Health Among Adolescents: A Systematic Review. Int J Behav Nutr Phys Act (2016) 13:108. doi:10.1186/s12966-016-0432-4
3. Chaput, J-P, Gray, CE, Poitras, VJ, Carson, V, Gruber, R, Olds, T, et al. Systematic Review of the Relationships between Sleep Duration and Health Indicators in School-Aged Children and Youth. Appl Physiol Nutr Metab (2016) 41:S266–82. doi:10.1139/apnm-2015-0627
4.Swiss Federal Office of Public Health. Coronavirus: Federal Council Declares ‘extraordinary Situation’ and Introduces More Stringent Measures (2020). Available at: https://www.bag.admin.ch/bag/en/home/das-bag/aktuell/medienmitteilungen.msg-id-78454.html (Accessed Sep 30, 2021).
5. Ritchie, H, Mathieu, E, Rodés-Guirao, L, Appel, C, Giattino, C, Ortiz-Ospina, E, et al. Coronavirus Pandemic (COVID-19) (2020). Available at: https://ourworldindata.org/coronavirus (Accessed Nov 16, 2021).
6.Swiss Federal Office of Public Health. Coronavirus: Measures and Ordinances (2021). Available at: https://www.bag.admin.ch/bag/en/home/krankheiten/ausbrueche-epidemien-pandemien/aktuelle-ausbrueche-epidemien/novel-cov/massnahmen-des-bundes.html#757183649 (Accessed Sep 30, 2021).
7. Paterson, DC, Ramage, K, Moore, SA, Riazi, N, Tremblay, MS, and Faulkner, G. Exploring the Impact of COVID-19 on the Movement Behaviors of Children and Youth: A Scoping Review of Evidence after the First Year. J Sport Health Sci (2021) 10:675–89. doi:10.1016/j.jshs.2021.07.001
8. Szwarcwald, CL, Malta, DC, Barros, MBA, Júnior, PRB, Romero, D, de Almeida, WDS, et al. Associations of Sociodemographic Factors and Health Behaviors with the Emotional Well-Being of Adolescents during the Covid-19 Pandemic in Brazil. Int J Environ Res Public Health (2021) 18:6160. doi:10.3390/ijerph18116160
9. Breidokienė, R, Jusienė, R, Urbonas, V, Praninskienė, R, and Girdzijauskienė, S. Sedentary Behavior Among 6–14-Year-Old Children during the COVID-19 Lockdown and its Relation to Physical and Mental Health. Healthcare (2021) 9:756. doi:10.3390/healthcare9060756
10. Morres, ID, Galanis, E, Hatzigeorgiadis, A, Androutsos, O, and Theodorakis, Y. Physical Activity, Sedentariness, Eating Behaviour and Well-Being during a COVID-19 Lockdown Period in Greek Adolescents. Nutrients (2021) 13:1449. doi:10.3390/nu13051449
11. Nagata, JM, Cortez, CA, Cattle, CJ, Ganson, KT, Iyer, P, Bibbins-Domingo, K, et al. Screen Time Use Among US Adolescents during the COVID-19 Pandemic. JAMA Pediatr (2021) 176:94. doi:10.1001/jamapediatrics.2021.4334
12. Kalak, N, Lemola, S, Brand, S, Holsboer-Trachsler, E, and Grob, A. Sleep Duration and Subjective Psychological Well-Being in Adolescence: a Longitudinal Study in Switzerland and Norway. Neuropsychiatr Dis Treat (2014) 10:1199–207. doi:10.2147/NDT.S62533
13. Chaffee, BW, Cheng, J, Couch, ET, Hoeft, KS, and Halpern-Felsher, B. Adolescents’ Substance Use and Physical Activity before and during the COVID-19 Pandemic. JAMA Pediatr (2021) 175:715–22. doi:10.1001/jamapediatrics.2021.0541
14. Reece, LJ, Owen, K, Foley, B, Rose, C, Bellew, B, and Bauman, A. Understanding the Impact of COVID-19 on Children’s Physical Activity Levels in NSW, Australia. Health Promot J Austr (2021) 32:365–6. doi:10.1002/HPJA.436
15. Shneor, E, Doron, R, Levine, J, Zimmerman, DR, Benoit, JS, Ostrin, LA, et al. Objective Behavioral Measures in Children before, during, and after the Covid-19 Lockdown in israel. Int J Environ Res Public Health (2021) 18:8732. doi:10.3390/ijerph18168732
16. Hirshkowitz, M, Whiton, K, Albert, SM, Alessi, C, Bruni, O, DonCarlos, L, et al. National Sleep Foundation’s Updated Sleep Duration Recommendations: Final Report. Sleep Health (2015) 1:233–43. doi:10.1016/j.sleh.2015.10.004
17. Bull, FC, Al-Ansari, SS, Biddle, S, Borodulin, K, Buman, MP, Cardon, G, et al. World Health Organization 2020 Guidelines on Physical Activity and Sedentary Behaviour. Br J Sports Med (2020) 54:1451–62. doi:10.1136/BJSPORTS-2020-102955
19. Walsh, JJ, Barnes, JD, Cameron, JD, Goldfield, GS, Chaput, J-P, Gunnell, KE, et al. Associations between 24 Hour Movement Behaviours and Global Cognition in US Children: a Cross-Sectional Observational Study. Lancet Child Adolesc Health (2018) 2:783–91. doi:10.1016/S2352-4642(18)30278-5
20. Carson, V, Chaput, J-P, Janssen, I, and Tremblay, MS. Health Associations with Meeting New 24-hour Movement Guidelines for Canadian Children and Youth. Prev Med (Baltim) (2017) 95:7–13. doi:10.1016/j.ypmed.2016.12.005
21. Marciano, L, and Camerini, AL. Recommendations on Screen Time, Sleep and Physical Activity: Associations with Academic Achievement in Swiss Adolescents. Public Health (2021) 198:211–7. doi:10.1016/j.puhe.2021.07.027
22. Guerrero, MD, Barnes, JD, Walsh, JJ, Chaput, JP, Tremblay, MS, and Goldfield, GS. 24-hour Movement Behaviors and Impulsivity. Pediatrics (2019) 144:e20190187. doi:10.1542/peds.2019-0187
23. Khan, A, Lee, E-Y, Rosenbaum, S, Khan, SR, and Tremblay, MS. Dose-dependent and Joint Associations between Screen Time, Physical Activity, and Mental Wellbeing in Adolescents: an International Observational Study. Lancet Child Adolesc Health (2021) 5:729–38. doi:10.1016/S2352-4642(21)00200-5
24. West, EA, Anker, D, Amati, R, Richard, A, Wisniak, A, Butty, A, et al. Corona Immunitas: Study Protocol of a Nationwide Program of SARS-CoV-2 Seroprevalence and Seroepidemiologic Studies in Switzerland. Int J Public Health (2020) 65:1529–48. doi:10.1007/s00038-020-01494-0
25.Swiss Federal Statistical Office. Demographic Balance of the Permanent Resident Population, by canton and Commune, 2010-2020 (2021). Available at: https://www.bfs.admin.ch/bfs/en/home/statistics/population/effectif-change/regional-distribution.assetdetail.18344222.html (Accessed Oct 1, 2021).
26. Ulyte, A, Radtke, T, Abela, IA, Haile, SR, Braun, J, Jung, R, et al. Seroprevalence and Immunity of SARS-CoV-2 Infection in Children and Adolescents in Schools in Switzerland: Design for a Longitudinal, School-Based Prospective Cohort Study. Int J Public Health (2020) 65:1549–57. doi:10.1007/s00038-020-01495-z
27. Szkultecka-Dębek, M, Dzielska, A, Drozd, M, Małkowska-Szkutnik, A, and Mazur, J. What Does the Cantril Ladder Measure in Adolescence? Arch Med Sci (2018) 14:182–9. doi:10.5114/aoms.2016.60718
28. Idler, EL, and Benyamini, Y. Self-rated Health and Mortality: A Review of Twenty-Seven Community Studies. J Health Soc Behav (1997) 38:21–37. doi:10.2307/2955359
29. Levin, KA, and Currie, C. Reliability and Validity of an Adapted Version of the Cantril Ladder for Use with Adolescent Samples. Soc Indic Res (2014) 119:1047–63. doi:10.1007/s11205-013-0507-4
30. De Onis, M. 4.1 The WHO Child Growth Standards. World Rev Nutr Diet (2015) 113:278–94. doi:10.1159/000360352
31. Sawyer, SM, Azzopardi, PS, Wickremarathne, D, and Patton, GC. The Age of Adolescence. Lancet Child Adolesc Health (2018) 2:223–8. doi:10.1016/S2352-4642(18)30022-1
32. Agresti, A, and Coull, BA. Approximate Is Better Than “Exact” for Interval Estimation of Binomial Proportions. Am Stat (1998) 52:119. doi:10.2307/2685469
33. Muff, S, Nilsen, EB, O’Hara, RB, and Nater, CR. Rewriting Results Sections in the Language of Evidence. Trends Ecol Evol (2022) 37:203–10. doi:10.1016/j.tree.2021.10.009
34.R Core Team. A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing (2020). Available at: https://www.r-project.org/ (Accessed Sep 7, 2021).
35. Wickham, H. ggplot2: Elegant Graphics for Data Analysis. Cham: Springer International Publishing (2016). doi:10.1007/978-3-319-24277-4
36. Pedersen, TL. Patchwork: The Composer of Plots. R Package Version 1.1.1 (2020). Available at: https://cran.r-project.org/package=patchwork (Accessed Sep 7, 2021).
37. Serrano-Sanchez, JA, Martí-Trujillo, S, Lera-Navarro, A, Dorado-García, C, González-Henríquez, JJ, and Sanchís-Moysi, J. Associations between Screen Time and Physical Activity Among Spanish Adolescents. PLoS One (2011) 6:e24453. doi:10.1371/journal.pone.0024453
38. Jarnig, G, Jaunig, J, and van Poppel, MNM. Association of COVID-19 Mitigation Measures with Changes in Cardiorespiratory Fitness and Body Mass Index Among Children Aged 7 to 10 Years in Austria. JAMA Netw Open (2021) 4:e2121675. doi:10.1001/jamanetworkopen.2021.21675
39. Wang, J, Li, Y, Musch, DC, Wei, N, Qi, X, Ding, G, et al. Progression of Myopia in School-Aged Children after COVID-19 home Confinement. JAMA Ophthalmol (2021) 139:293–300. doi:10.1001/jamaophthalmol.2020.6239
40. López-Gil, JF, Tremblay, MS, and Brazo-Sayavera, J. Changes in Healthy Behaviors and Meeting 24-h Movement Guidelines in Spanish and Brazilian Preschoolers, Children and Adolescents during the Covid-19 Lockdown. Children (2021) 8:83. doi:10.3390/children8020083
41. Twenge, JM, Hisler, GC, and Krizan, Z. Associations between Screen Time and Sleep Duration Are Primarily Driven by Portable Electronic Devices: Evidence from a Population-Based Study of U.S. Children Ages 0–17. Sleep Med (2019) 56:211–8. doi:10.1016/j.sleep.2018.11.009
42. Viner, R, Russell, S, Saulle, R, Croker, H, Stansfield, C, Packer, J, et al. School Closures during Social Lockdown and Mental Health, Health Behaviors, and Well-Being Among Children and Adolescents during the First COVID-19 Wave: A Systematic Review. JAMA Pediatr (2022) 176:400–9. doi:10.1001/jamapediatrics.2021.5840
43. Puolakka, E, Pahkala, K, Laitinen, TT, Magnussen, CG, Hutri-Kähönen, N, Männistö, S, et al. Childhood Socioeconomic Status and Lifetime Health Behaviors: The Young Finns Study. Int J Cardiol (2018) 258:289–94. doi:10.1016/j.ijcard.2018.01.088
44. Reiss, F. Socioeconomic Inequalities and Mental Health Problems in Children and Adolescents: A Systematic Review. Soc Sci Med (2013) 90:24–31. doi:10.1016/j.socscimed.2013.04.026
45. Marciano, L, Ostroumova, M, Schulz, PJ, and Camerini, A-L. Digital Media Use and Adolescents’ Mental Health during the Covid-19 Pandemic: A Systematic Review and Meta-Analysis. Front Public Health (2022) 9:793868. doi:10.3389/fpubh.2021.793868
46. Moeijes, J, van Busschbach, JT, Bosscher, RJ, Twisk, JWR, Loth, E, and Camerini, A-L. Sports Participation and Health-Related Quality of Life: a Longitudinal Observational Study in Children. Qual Life Res (2019) 28:2453–69. doi:10.1007/s11136-019-02219-4
47. Peralta, GP, Camerini, AL, Haile, SR, Kahlet, CR, Radtke, T, Ulyte, A, et al. Lifestyle behaviours of children and adolescents during the first two waves of the COVID-19 pandemic in Switzerland and their relation to well-being: a population-based study. MedRxiv [Preprint] (2019). Available from: https://www.medrxiv.org/content/10.1101/2021.11.29.21267019v1 (Accessed December 1, 2021).
Keywords: COVID-19, physical activity, well-being, children and adolescents, lifestyle, screen time, sleep
Citation: Peralta GP, Camerini A-L, Haile SR, Kahlert CR, Lorthe E, Marciano L, Nussbaumer A, Radtke T, Ulyte A, Puhan MA and Kriemler S (2022) Lifestyle Behaviours of Children and Adolescents During the First Two Waves of the COVID-19 Pandemic in Switzerland and Their Relation to Well-Being: An Observational Study. Int J Public Health 67:1604978. doi: 10.3389/ijph.2022.1604978
Received: 01 April 2022; Accepted: 26 August 2022;
Published: 08 September 2022.
Edited by:
Olaf Von Dem Knesebeck, University Medical Center Hamburg-Eppendorf, GermanyReviewed by:
Rebeca Mozun, University Children’s Hospital Zurich, SwitzerlandCopyright © 2022 Peralta, Camerini, Haile, Kahlert, Lorthe, Marciano, Nussbaumer, Radtke, Ulyte, Puhan and Kriemler. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Susi Kriemler, c3VzaS5rcmllbWxlcndpZ2V0QHV6aC5jaA==
†These authors have contributed equally to this work and share first authorship
‡These authors have contributed equally to this work and share last authorship