 Nicolás Bronfman
Nicolás Bronfman Paula Repetto
Paula Repetto Pamela Cisternas
Pamela Cisternas Javiera Castañeda
Javiera Castañeda Paola Cordón3
Paola Cordón3- 1Engineering Sciences Department, Universidad Andres Bello, Santiago, Chile
- 2Research Center for Integrated Disaster Risk Management ANID/FONDAP/15110017, Santiago, Chile
- 3Department of Psychology, Pontificia Universidad Católica de Chile, Santiago, Chile
- 4Industrial and Systems Engineering Department, Pontificia Universidad Católica de Chile, Santiago, Chile
Objective: The purpose of this study was to determine the influence of government trust on young adults’ adoption of health behaviors to prevent infection with the SARS-CoV-2 virus.
Method: We tested the hypothesis that government trust would directly and indirectly (through worry/fear and subjective norms) influence the adoption of health-protective behaviors. A sample of 1,136 university students completed a web survey after Chile’s first wave of infections.
Results: The results indicate that low government trust only indirectly (through subjective norms) influenced health-protective behaviors. Conversely, worry/fear was the primary motivating factor for adopting health-protective behaviors in young adults, followed by subjective norms.
Conclusion: In scenarios where people perceive low government trust, emotions and social norms are the motivational factors with the most significant predictive power on the adoption of health-protective behaviors.
Introduction
Human behavior in a pandemic significantly affects the transmission of the virus that produces the disease. Therefore, it is essential to encourage people to adopt the authorities’ suggested protective measures to manage the crisis successfully [1]. Several factors determine the intention and the adoption of protective measures in a pandemic. Among these factors, the most important correspond to motivational factors such as trust in authorities, attitudes, subjective norms, fear, and worry [2–6]; as well as psychosocial conditions such as anxiety and depression [5, 7, 8]; socio-demographic factors [9–11]; among others. For the motivational factors, trust in the authorities plays an essential role in managing a pandemic [12–14] since it is crucial to building a social climate where people adopt the measures recommended by the authorities [13, 15]. Trust in the authorities will lead people to interpret information appropriately [16, 17] and foster a positive attitude and a collaborative environment that encourages the adoption of protective behaviors [3]. Suppose people do not trust the institutions in charge of protecting them. In that case, people can ignore the information provided by these institutions and also behave oppositely to the behaviors being fostered [17].
Globally, young adults have been identified as the group with the lowest rates of compliance with measures to prevent the spread of the SARS-CoV-2 virus [18, 19], possibly explained by their low risk of severe symptoms [20], the effect of confinement, and physical distancing measures on their mental health [21, 22], or the degree of their distrust in the authorities [19]. Nivette et al. [19] have concluded that non-compliance with COVID-19 protective measures by adolescents and young adults in Zurich, Switzerland, is related to their modest trust in authorities. In addition, within an environment of high distrust in authorities, people can adopt behaviors based on incorrect information about protecting themselves from the virus. For example, they may ingest bleach to prevent infection, inhale alcohol to eliminate the virus or use ultraviolet light on their skin, among other behaviors that can seriously damage their health [23, 24]. Therefore, trust in authorities plays a crucial role in promoting behaviors that protect people’s health within this pandemic.
In March 2020, the first confirmed case of COVID-19 in Chile was detected, which brought the global pandemic to this country. The pandemic arrived in Chile during a significant socio-political crisis. Protests against the government and state authorities in which many people participated, regarding income inequality, the high cost of living, among other demands. The tension increased, and severe episodes of violence and human rights violations occurred, leading the authorities to declare a state of emergency for the first time since the end of the dictatorship [25]. In addition, the government was registering its lowest public confidence indicators. The Organization for Economic Co-operation and Development (OECD) reveals that Chile has the lowest public trust among all OECD countries. Only 15.3% and 17.1% of its citizens trusted the government in 2019 and 2020, respectively [26]. Given the current scenario of a global health crisis and low government trust, the purpose of this study was to determine the influence of government trust on the adoption of health behaviors by young adults to prevent SARS-CoV-2 virus infections in a very unfavorable environment.
Government Trust and Protective Behaviors
Government trust can broaden people’s knowledge of a pandemic and increase their risk awareness [27]. Since the influenza A (H1N1) pandemic of 2009 and 2010, different studies have shown that high government trust is significantly associated with greater acceptance of protective measures [27–32]. Research by Van der Weerd et al. [30] focused on identifying the factors associated with the intention to adopt protective measures during the influenza A (H1N1) pandemic in the Netherlands. The authors concluded that the highest intent to receive the vaccine was associated with higher government trust, greater fear and worry, and greater perceived vulnerability. Researchers reported similar results in studies related to the Middle East Respiratory Syndrome (MERS) epidemic in early 2012 [33, 34].
During the pandemic caused by the SARS-CoV-2 virus, several studies have identified that trust in authorities is a significant predictor of the acceptance of health measures and the adoption of protective behaviors, such as social distancing [3, 19, 35–38], wearing face masks [4, 18, 36, 39], reducing mobility (staying at home) [35, 40], and getting vaccinated [41–44]. For example, a study in Colombia showed that when government trust is low, measures to prevent covid-19 are rejected and generate anger and disgust, and then cause the levels of distrust in authorities to increase even more [45].
Trust in the authorities is a complex variable studied by researchers from different disciplines. Trust recognizes the role of personal and cultural values and the influence of psychological, social, and political factors [46, 47]. In this study, we examined trust in government concerning its performance in a crisis, that is, the pandemic, and about two dimensions: integrity and competence. Integrity refers to values of honesty and transparency that people perceive in authorities. On the other hand, competence refers to people’s judgment regarding the authorities’ capacities and efficiency in managing a crisis [48, 49]. During a pandemic health crisis, open, honest, and transparent communication is essential to foster public government trust, which encourages the adoption of protective behaviors to mitigate or reduce the damage [27, 50]. Recent studies on the pandemic caused by the SARS-CoV-2 virus have reaffirmed the importance of open and transparent communication between government institutions and the health authorities to drive the adoption of protective behaviors [14, 51]. Thus, we expect government trust to increase health-protective behaviors in this study and propose the following hypothesis.
H1: Government trust will have a direct and positive relationship with the adoption of health-protective behaviors.
Government Trust, Worry/Fear, and Protective Behaviors
Trust in authorities plays a significant role in shaping perceptions in the face of many natural threats [49]. Government trust influences the adoption of protective measures and helps reduce stress and anxiety [5, 50]. In the context of the SARS-CoV-2 pandemic, studies conducted in the United States [3], Singapore [4], China [51], Germany [52], and Latin America [43, 52] have concluded that government trust can increase people’s perception of risk and, therefore, the adoption of protective measures. Siegrist et al. [13] conducted a study during the peak of confirmed COVID-19 cases during the first wave in Switzerland. They found that the perception of risk, measured as fear and worry about infection and the financial impact of the pandemic, was an essential driver of the acceptance and adoption of the measures recommended by the government. In addition, people with high government trust expressed more worry about contagion than people with low social trust. Similarly, Mongue-Rodriguez et al. [53], found in Peru that when people had greater trust in the information about covid-19 provided by the authorities, the population’s perception of risk and perception of treat increased.
The specialized literature indicates that people evaluate risks in cognitive terms (probability) and through emotions such as worry and fear [53–55]. Worry is a crucial determinant of behavior in the context of health-protective behaviors. For example, a study of vaccination behavior in Latin America identified fear as one of the most influential predictors of the intention to be vaccinated [43, 44]. Similar results were reported in a study associated with the A (H1N1) influenza pandemic conducted in the Netherlands [30], Italy [29], Hong Kong [31], the United States [56], and France [57]. In the SARS-CoV-2 virus pandemic context, high levels of worry and fear were associated with increased adoption of protective behaviors [6, 9]. Hence, we expect that in this study, government trust will increase the level of worry and worry, which will increase the adoption of protective behaviors. We, therefore, propose the following hypotheses:
H2: Government trust will have a direct and positive relationship with worry/fear.
H3: Worry/fear will have a significant and positive effect on adopting health-protective behaviors.
Government Trust, Subjective Norms, and Protective Behaviors
Trust can also influence protective behaviors through motivational factors that facilitate their adoption [54]. Some studies during the SARS-CoV-2 pandemic have shown that government trust and subjective social norms are significantly related, suggesting that a high degree of government trust may reflect positive values and beliefs by the public that they will be treated with fairness and integrity [3]. In this study, subjective norms refer to the importance that people give to the opinion of others about the adoption of preventive behavior [55, 56].
Lee and Li [3] found that, among the main motivational factors, subjective norms had the most significant influence on social distancing behavior to prevent the spread of the virus that causes COVID-19. The authors also found that subjective norms play a mediating role in the relationship between trust and social distancing behavior. Masser et al. [5] found that subjective norms significantly predicted the intention to donate blood during the pandemic. Trust in blood collection agencies plays a vital role in predicting subjective norms and, indirectly, behavioral intention. Also, a study in Chile identified that when people perceive that their families and friends comply with preventive behaviors against covid-19, they are more likely to wear a mask, keep their distance between people, and wash their hands for more than 20 s [57].
Similarly, Kim and Tandoc [4] found that government trust was positively and significantly related to subjective norms and with the intention to wear a face mask to prevent infection by SARS-CoV-2. Hence, in this study, we expect that government trust will increase social pressure to adopt protective measures and that these social norms will influence the adoption of health-protective behaviors. Consequently, we propose the following hypotheses:
H4: Government trust will have a direct and positive relationship with subjective norms.
H5: Subjective norms will have a direct and positive relationship with protective behaviors.
Subjective Norms and Worry/Fear
The Theory of Planned Behavior (TPB) postulates that the direct predictor of behavior is the intention to perform a behavior, which is explained by three motivational factors: attitudes, subjective norms, and perceived behavioral control [55]. Some authors, however, have criticized the TPB because it ignores the role that emotions play in human behavior [58, 59]. For example, perceived threats may cause worry about the consequences of taking or not an action, and worry may strengthen the intention to act [59]. Schmiege, Bryan and Klein [60] have identified that worry significantly affects the attitudes and subjective norms that comprise the TPB. Thus, more worry reinforces subjective norms associated with adopting behaviors, especially among those who had not previously performed that behavior. Raude et al. [6] have found that subjective norms represent the most crucial predictor of compliance with measures to prevent SARS-CoV-2 infection. Subjective norms are significantly related to worry about contracting the coronavirus. Thus, based on this line of reasoning, worry is expected to be significantly associated with subjective norms (e.g., worry will influence social pressure to adopt health-protective behaviors). We, therefore, propose the following hypothesis:
H6: Worry/fear will have a direct and positive relationship with subjective norms.
Methods
Materials
We tested the hypotheses using a web-based survey of young adults that evaluated health-protective behaviors in response to the COVID-19 pandemic in Chile. The survey contained three sections. The first section measured motivational factors (government trust, worry/fear, and subjective norms). The second section assessed health-protective behaviors (physical distancing, wearing facemasks, and handwashing), and the third one, included questions regarding socio-demographic factors.
Government trust was measured through six items grouped in two dimensions of trust, defined in previous studies [46, 48]. These dimensions comprised three items for integrity-based trust and three items for competence-based trust. Both scales were validated in Chile by previous studies [61]. Participants were asked to respond using a 5-point Likert scale: 1) strongly disagree, 2) disagree, 3) neither agree nor disagree, 4) agree, and 5) strongly agree (see Table 1). Six items characterized the worry/fear variable, adapted from previous studies focused on understanding and predicting the adoption of health-protective behaviors [62, 63]. Participants rated their level of worry and fear on a 7-point scale from (1) not at all to (7) very much. Subjective norms were evaluated using four items that asked about their motivation to comply with four groups of significant people: family, close friends, peers, and teachers (see Table 1). We adapted these items from previous studies that used the TPB in pandemics [63]. As with the item “government trust,” participants were asked to respond using a 5-point Likert scale from (1) strongly disagree to (5) strongly agree. Finally, seven items associated with health-protective behaviors were used, adapted from previous research during the A (H1N1) pandemic [29, 31]. Participants responded using a 5-point frequency scale: 1) never, 2) rarely, 3) sometimes, 4) almost always, and 5) always (see Table 1).
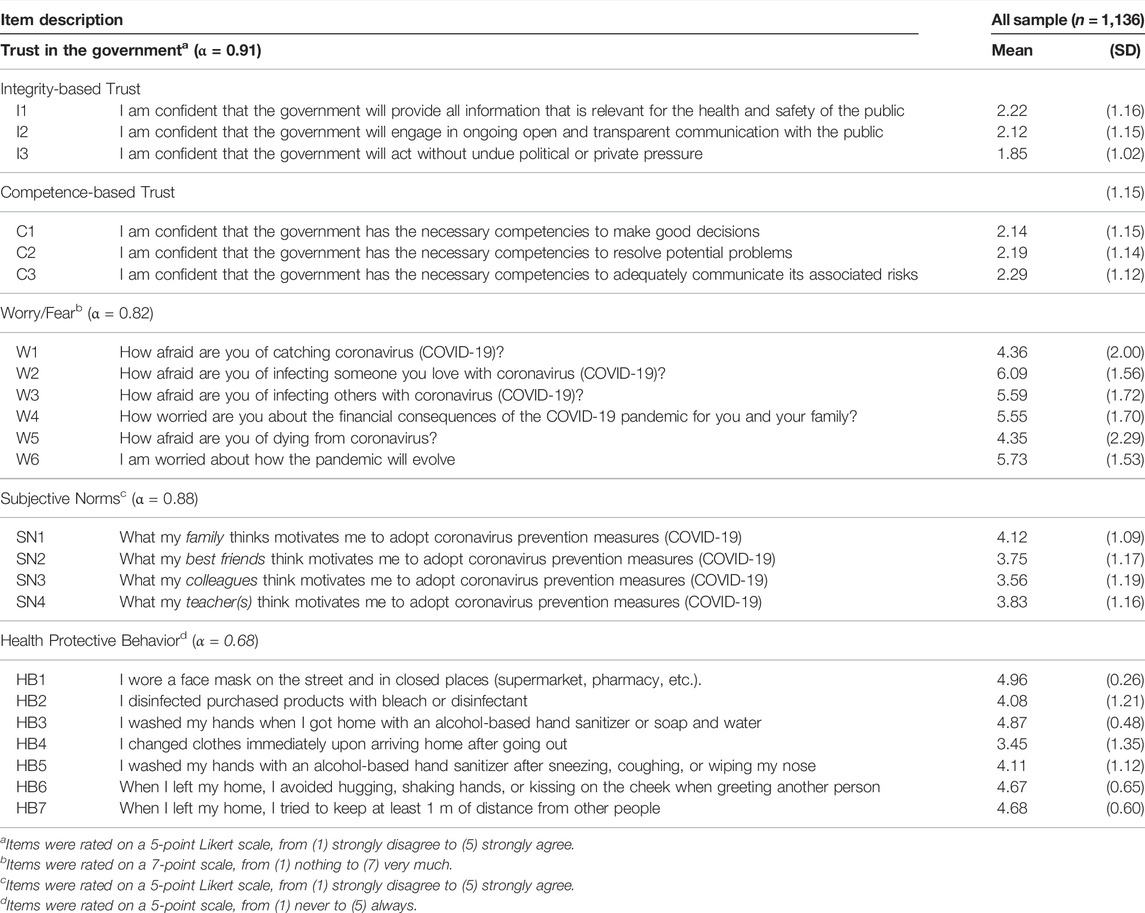
TABLE 1. Mean values and standard deviation for each item of government trust, worry/fear, subjective norms, and health protective behavior (Health-protective behaviors to prevent COVID-19, Chile, 2020).
Procedure and Participants
The survey was constructed and validated by the research team. Then, using a focus group composed of university students, we tested whether the questions were clear and comprehended. The data collection went from September to December 2020 through an online survey. The questionnaire was sent to undergraduate and graduate students of all academic programs of the Andrés Bello University and Pontificia Universidad Catolica of Chile. All respondents consented to participate voluntarily in the study to answer the survey.
One thousand one hundred thirty-six students completed the survey from the cities of Valparaíso, Concepcion, and Santiago. Participants reported an average of 23.3 years (SD = 9.3 years, between 18 and 50 years old). Of the 167 total sample, 83.5% said they were single, 30.7% were male and, 23.5% declared having a family income between 600.000 and 1 million Chilean pesos (726–1452 USD). It took participants an average of 20 min to complete the survey.
Data Analysis
To test the six hypotheses proposed for this study, an internal reliability analysis of the scales of government trust, worry/fear, subjective norms, and health-protective behaviors was conducted first. We used IBM SPSS Statistics v.27.0 software to calculate Cronbach’s Alpha Coefficient. Kline [64] suggests Alpha values higher than 0.7 for scales with high internal reliability; he also states that values lower than 0.7 can be allowed if the sample size is large enough to estimate all the model’s parameters.
IBM SPSS AMOS v.27.0 software was used to build the structural equation model to test the hypotheses of this study. Each latent variable in the model was built using the items associated with each construct as observed variables (see Figure 1). There are no missing values for the observed variables of government trust, worry/fear, and subjective norms. The number of missing values in the health-protective behavior variable was negligible, with 0.9% being the highest percentage found in the sample (item HB5). Given the low number of missing values, we used a non-stochastic imputation method, and the mean replaced the missing values. Maximum likelihood was used to estimate the model, and the following indicators were considered to determine the model fit: chi-squared (χ2), comparative fit index (CFI), normed fit index (NFI), and robustness of mean square error approximation (RMSEA). The proportion of the variance explained by the model was measured using the Squared Multiple Correlation (R2SMC).
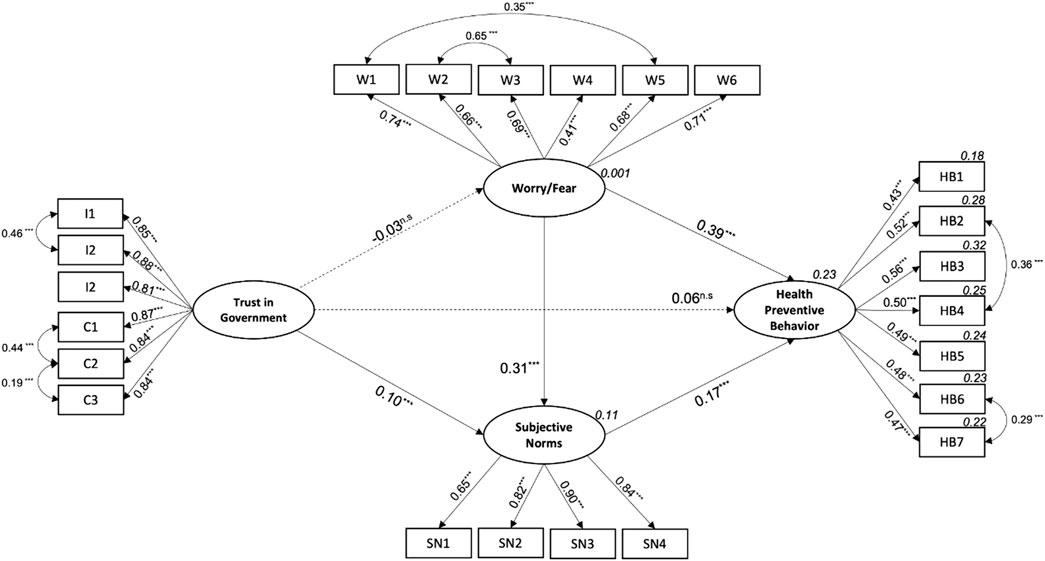
FIGURE 1. Health Protective Behavior Model (Health-protective behaviors to prevent COVID-19, Chile, 2020). Note: Arrows represent the direct relationships between the latent variables. The values above the arrows indicate the standardized regression coefficients of each relationship. Dotted lines show non-significant standardized regression coefficients. Two-headed arrows show the covariances suggested by the analysis to improve the fit of the model. The values in cursive above the latent variables represent the squared multiple correlations. The cursive values above the health protective observed variables show the proportion of explained variance for each action. Observed variables: Integrity-based Trust (I); Competence-based Trust (T) Worry/Fear (W); Subjective Norms (SN); Health Protective Behaviors (HB). The incorporation of the covariances between Trust in the government items I1-I2, C1-C2, C2-C3 is theoretically justified, since they relate the items within the dimensions of trust studied in this study. The covariances between Worry/Fear items W1–W5 and W2–W3 make theoretical sense, since in the former, both items relate to the fear of direct consequences for the participant, while in the latter, the items relate to the fear of infecting others. Finally, the inclusion of the covariance’s between items HB2-HB4 and HB6-HB7 is reasonable since they relate to health protective behaviors when leaving the home. ***p < 0.001; n.s. non-significant (p > 0.05).
Results
Table 1 contains the results of the internal reliability analysis, in addition to the mean and standard deviation for each observed variable included in the structural equation model. The Cronbach’s Alpha Coefficients for the four latent variables indicate highly consistent scales.
An analysis of the mean values for the model’s observable variables (see Table 1) indicates that government trust was substantially low, with mean values below 2.3 on a 5-point scale, for all six items. The mean values for worry/fear were moderately high, especially for items associated with fear of infecting loved ones (W2) and uncertainty about how this pandemic will evolve (W6). In terms of subjective norms, participants reported a greater motivation to adopt protective measures when recommended to do so by family members (SN1) and college professors (SN4). Finally, the analysis for the results for health-protective behaviors revealed that participants reported a high frequency in the use of face masks (HB1), hand washing (HB3), and physical distancing (HB6 and HB7).
Table 2 contains the results of the structural equation model fit. Initially, the model did not have a good fit. An analysis of modification indices suggested incorporating seven covariance’s: three for government trust, two for worry/fear, and two for health-protective behavior. The model fit significantly increased by incorporating this theoretically supported covariance (see Figure 1 for details on the covariance). The final model is represented in Figure 1. The analysis confirmed four of the six proposed hypotheses: the relationship between government trust and worry/fear or health-protective behavior was not statistically significant. Hypotheses H1 and H2 were rejected. An analysis of the standardized direct, indirect, and total effects (see Table 3) revealed that worry/fear was the variable that exerted the most significant influence on health-protective behavior (0.44), followed by subjective norms (0.17).

TABLE 2. Fit indexes for the structural model (Health-protective behaviors to prevent COVID-19, Chile, 2020).
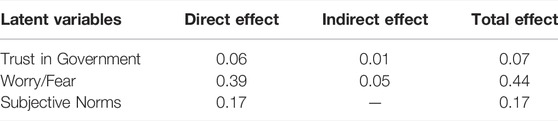
TABLE 3. Standardized direct, indirect, and total effects of the latent variables on health protective behavior (Health-protective behaviors to prevent COVID-19, Chile, 2020).
As measured by the Squared Multiple Correlation (R2SMC) for health-protective behavior, the proportion of variance explained by the model was 23%. A balanced predictive power associated with the protective behaviors included in the study was obtained, ranging between 18% and 32% of the variance explained.
Discussion
The purpose of this study was to determine the influence of government trust on the adoption of health-protective behaviors by young adults to prevent the effects of the SARS-CoV-2 virus. Based on previous studies, government trust was hypothesized to be directly and indirectly (through worry/fear and subjective norms) related to adopting protective behaviors. This research indicates that worry/fear was the main motivational factor for adopting protective behaviors by young adults, followed by subjective norms. Government trust had only an indirect effect on these behaviors.
Government Trust
Abundant research reveals that government trust is an essential predictor of accepting and adopting behaviors that prevent the effects and spread of the SARS-CoV-2 virus [19, 35, 37–39]. Government trust during a pandemic implies the belief that information provided by the government is honest and transparent and not influenced by political or private interests [13]. This belief improves communication between the government and the public, allowing for a greater flow of information to protect health [3, 53]. However, our results indicate that government trust did not directly affect preventive behaviors; it only had an indirect influence through subjective social norms on the adoption of protective behaviors by young adults. This relevant result can be explained by the low level of government trust stated by the participants, which is in line with the OECD’s 2019 and 2020 reports on Government trust, The results of this research have important implications for the persons responsible for designing communications strategies in a crisis, such as the pandemic caused by the SARS-CoV-2 virus. The low government trust reported by the participants is an alarming signal for current and future national authorities. In a context of high distrust in the authorities, people seek other reliable actors to obtain information and maintain their capacity to act in a complex environment [58]. In addition, low trust in the authorities can cause more discomfort in the population rejecting the implemented measures and may expose them to adopting erroneous and potentially harmful behaviors in terms of their health based on false or unsupported information by science [45]. Even, as Urrunaga-Pastor et al. [43] pointed out, in a study with a population in Latin America, low trust can influence people’s intention to get vaccinated against COVID, affecting one of the main strategies mitigate the impacts of the pandemic in the region. Therefore, the authorities need to design effective communication strategies that transmit information and increase public confidence, especially in countries with low trust in government.
Contrary to expectations, government trust was not related to fear and worry over the potential financial and health effects of the SARS-CoV-2 pandemic. Siegrist et al. [13] found that fear and worry (the perception of risk) concerning infection and the financial impact of the pandemic were essential drivers for the acceptance and adoption of the measures recommended by the Government in Switzerland. This discrepant result can be explained by the low government trust reported in this study. In relative terms, while the Siegrist et al. [13] study obtained a mean value of 5.74 for social trust on a 7-point scale, our study got a mean value of 2.22 on a 5-point scale.
Worry/Fear
In the context of health behaviors, worry and fear are essential determinants for people to adopt protective behaviors [9], as they motivate people to follow and implement the measures recommended by the authorities [65]. Our results indicate that worry was the primary motivating factor for adopting health behaviors that prevent the infection and spread of the SARS-CoV-2 virus. This finding is consistent with the results reported by previous research associated with the influenza A (H1N1) pandemic in Italy, Netherlands, and Hong Kong, which reveal that worry was one of the most influential predictors of the adoption of protective measures [29–31]. Therefore, we conclude that people with greater fear and worry report adopting protective behaviors and social distancing more frequently than those who report less fear and worry.
Worry was positively and significantly related to subjective norms, suggesting that fear and worry can increase the impact of social pressure on behavior, decreasing the likelihood that people will try to behave differently. However, as a significant motivational factor for adopting protective health measures, negative emotions’ role cannot be disregarded. If people become familiar with the disease and the associated risks, their levels of worry and fear may decrease. This situation could reduce the frequency with which they adopt protective behaviors, which would be an adverse scenario in controlling the pandemic.
Subjective Norms
Finally, in line with prior research [3–5], our results suggest that subjective norms were a significant predictor of health behaviors to prevent the virus that causes COVID-19 and have an essential mediating role in the weak relationship between government trust and health-protective behaviors. Similarly, Lee and Li [3] have found that subjective norms were the most influential determinants of social distancing behavior and significantly mediated the relationship between trust and this behavior. In addition, these results are similar to other studies carried out in Chile, which indicate that the opinion and behaviors of friends and relatives are relevant for young people to carry out preventive behaviors against Covid-19 [57]. Then, our results suggest aspects of the Chilean culture and how social relationships are built that can favor decision-making in uncertain and ambiguous situations.
Since subjective norms are a significant predictor of adopting health-protective behaviors, those responsible for designing and implementing risk communication strategies may consider engaging influential groups to increase social pressure on adopting protective behaviors. Our results suggest that communication through influential groups such as family and university professors could be effective for young university students. Higher education teachers usually have greater access to objective and reliable information about the risk of contracting the disease and the measures required to prevent contagion. Therefore, given the higher levels of trust by young university students that higher education professors enjoy, the latter acquires a vital role in risk communication.
Conclusion
We can conclude that, in a scenario of low government trust—as it occurs in Chile—other motivational factors, such as worry/fear and subjective norms, emerge as the most influential ones for adopting health-protective behaviors among young adults in the face of the pandemic caused by the SARS-CoV-2 virus. People with higher levels of fear and worry about potential health and financial impacts report adopting protective health and social distancing behaviors more frequently than those with less fear and worry. Similarly, young people report a greater adoption of health-protective behaviors when their families and teachers consider adopting these behaviors important.
In addition, the influence of fear and worry evidence the importance of considering emotions as relevant mechanisms for adopting preventive behaviors. Generally, the different models and theories to understand preventive behaviors, such as the TPB model, do not include the direct impact of emotions on health behaviors and only consider cognitive or social factors. However, our study suggests that emotions play an essential role in decision-making when threats are unknown to the population. Consequently, emotions should be studied as factors underlying people’s attitudes or beliefs and valid processes that influence the behavior.
Accordingly, the design and implementation of health prevention strategies need to focus on communicating information based on scientific evidence and restoring government trust. In addition, there is a need to reinforce these behaviors through young people’s significant influencers to create an environment of social cooperation to improve adherence to the current and future health-protective behaviors required to mitigate the impact of the pandemic. Interestingly, family members and university professors appear to be the most relevant among this population, contrary to the influencers commonly recruited to promote behaviors, such as singers, actors, and athletes. University students may be more influenced by their family members and as a way to protect them and their professors, from whom they may expect to learn how to protect their health.
Limitations
This study has some limitations that must be recognized. First, the cross-sectional data used do not allow inferring causality. Future research should consider longitudinal data to test causal hypotheses. Second, it can be that the global health crisis scenario, the measures implemented by the government to cope with the pandemic, and the prevailing social and political context in Chile may have had a significant influence on people’s perception, acceptance, and adoption of protective health measures. Consequently, additional studies are required to corroborate our findings. Third, the sample was composed of undergraduate and graduate university students with particular socio-demographic characteristics (age or educational level) that may influence their knowledge and behavior to prevent COVID-19.
In consequence, extending these results to the population may be done carefully. Future research should consider a more representative sample of Chile to generalize the results. Finally, the proposed model could have greater predictive power by including new motivational and psychosocial factors into future research, such as the level of trust in the scientific community, in national and international health institutions and organizations, and in the mass media, all relevant stakeholders in the global fight against the pandemic.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics Committee of the Andres Bello University, Act No. 023/2020 and the Ethics Committee of the Pontificia Universidad Católica de Chile, Act No. 200828010/2020. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Funding
This research was partially funded by the National Agency of Research and Development of Chile (ANID) of the Ministry of Science, Technology, Knowledge and Innovation of Chile through the National Fund for Scientific and Technological Research (Grant No. ID1221047/FONDECYT/ANID) and by the Research Center for Integrated Disaster Risk Management (CIGIDEN), (Grant No. ANID/FONDAP/15110017).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Siegrist, M, and Zingg, A. The Role of Public Trust during Pandemics. Eur Psychol (2014) 19:23–32. doi:10.1027/1016-9040/a000169
2. Das, AK, Abdul Kader Jilani, MM, Uddin, MS, Uddin, MA, and Ghosh, AK. Fighting Ahead: Adoption of Social Distancing in COVID-19 Outbreak through the Lens of Theory of Planned Behavior. J Hum Behav Soc Environ (2020) 1–21. doi:10.1080/10911359.2020.1833804
3. Lee, Y, and Li, JYQ. The Role of Communication Transparency and Organizational Trust in Publics' Perceptions, Attitudes and Social Distancing Behaviour: A Case Study of the COVID‐19 Outbreak. J Contingencies Crisis Management (2021) 29:368–384. doi:10.1111/1468-5973.12354
4. Kim, HK, and Tandoc, . Wear or Not to Wear a Mask? Recommendation Inconsistency, Government Trust and the Adoption of Protection Behaviors in Cross-Lagged TPB Models. Health Commun (2021) 36:1–9. doi:10.1080/10410236.2020.1871170
5. Masser, BM, Hyde, MK, and Ferguson, E. Exploring Predictors of Australian Community Members' Blood Donation Intentions and Blood Donation-Related Behavior during the COVID‐19 Pandemic. Transfusion (2020) 60:2907–17. doi:10.1111/trf.16067
6. Raude, J, Lecrique, J-M, Lasbeur, L, Leon, C, Guignard, R, Roscoät, ED, et al. Determinants of Preventive Behaviors in Response to the COVID-19 Pandemic in France: Comparing the Sociocultural, Psychosocial and Social Cognitive Explanations. Front Psychol (2020) 11:3345. doi:10.3389/fpsyg.2020.584500
7. Bäuerle, A, Teufel, M, Musche, V, Weismüller, B, Kohler, H, Hetkamp, M, et al. Increased Generalized Anxiety, Depression and Distress during the COVID-19 Pandemic: a Cross-Sectional Study in Germany. J Public Health (2020) 42:672–8. doi:10.1093/pubmed/fdaa106
8. Lee, YC, Wu, WL, and Lee, C-K. How COVID-19 Triggers Our Herding Behavior? Risk Perception, State Anxiety and Trust. Front Public Health (2021) 9:46. doi:10.3389/fpubh.2021.587439
9. Barber, SJ, and Kim, H. COVID-19 Worries and Behavior Changes in Older and Younger Men and Women. The Journals Gerontol Ser B (2021) 76:e17–e23. doi:10.1093/geronb/gbaa068
10. Rana, IA, Bhatti, SS, Aslam, AB, Jamshed, A, Ahmad, J, and Shah, AA. COVID-19 Risk Perception and Coping Mechanisms: Does Gender Make a Difference? Int J Disaster Risk Reduct (2021) 55:102096. doi:10.1016/j.ijdrr.2021.102096
11. Niño, M, Harris, C, Drawve, G, and Fitzpatrick, KM. Race and Ethnicity, Gender, and Age on Perceived Threats and Fear of COVID-19: Evidence from Two National Data Sources. SSM - Popul Health (2021) 13:100717. doi:10.1016/j.ssmph.2020.100717
12. Rieger, MO, and Wang, M. Trust in Government Actions during the COVID-19 Crisis (2020) Available at: https://www.uni-trier.de/fileadmin/fb4/prof/BWL/FIN/Files
13. Siegrist, M, Luchsinger, L, and Bearth, A. The Impact of Trust and Risk Perception on the Acceptance of Measures to Reduce COVID‐19 Cases. Risk Anal (2021) 0:1–14. doi:10.1111/risa.13675
14. Spalluto, LB, Planz, VB, Stokes, LS, Pierce, R, Aronoff, DM, McPheeters, ML, et al. Transparency and Trust during the Coronavirus Disease 2019 (COVID-19) Pandemic. J Am Coll Radiol (2020) 17:909–12. doi:10.1016/j.jacr.2020.04.026
15. Wachinger, G, Renn, O, Begg, C, and Kuhlicke, C. The Risk Perception Paradox-Implications for Governance and Communication of Natural Hazards. Risk Anal (2013) 33:1049–65. doi:10.1111/j.1539-6924.2012.01942.x
16. Paton, D. Risk Communication and Natural hazard Mitigation: How Trust Influences its Effectiveness. Ijgenvi (2008) 8:2–16. doi:10.1504/ijgenvi.2008.017256
17. Siegrist, M, and Sütterlin, B. Human and Nature-Caused Hazards: The Affect Heuristic Causes Biased Decisions. Risk Anal (2014) 34:1482–94. doi:10.1111/risa.12179
18. MacIntyre, CR, Nguyen, P-Y, Chughtai, AA, Trent, M, Gerber, B, Steinhofel, K, et al. Mask Use, Risk-Mitigation Behaviours and Pandemic Fatigue during the COVID-19 Pandemic in Five Cities in Australia, the UK and USA: A Cross-Sectional Survey. Int J Infect Dis (2021) 106:199–207. doi:10.1016/j.ijid.2021.03.056
19. Nivette, A, Ribeaud, D, Murray, A, Steinhoff, A, Bechtiger, L, Hepp, U, et al. Non-compliance with COVID-19-Related Public Health Measures Among Young Adults in Switzerland: Insights from a Longitudinal Cohort Study. Soc Sci Med (2021) 268:113370. doi:10.1016/j.socscimed.2020.113370
20. Snape, MD, and Viner, RM. COVID-19 in Children and Young People. Science (2020) 370:286–8. doi:10.1126/science.abd6165
21. Capone, V, Caso, D, Donizzetti, AR, and Procentese, F. University Student Mental Well-Being during COVID-19 Outbreak: What Are the Relationships between Information Seeking, Perceived Risk and Personal Resources Related to the Academic Context? Sustainability (2020) 12:7039. doi:10.3390/su12177039
22. O'Reilly, A, Tibbs, M, Booth, A, Doyle, E, McKeague, B, and Moore, J. A Rapid Review Investigating the Potential Impact of a Pandemic on the Mental Health of Young People Aged 12-25 Years. Ir J Psychol Med (2020) 381–16. doi:10.1017/ipm.2020.106
23. Tasnim, S, Hossain, MM, and Mazumder, H. Impact of Rumors and Misinformation on COVID-19 in Social media. J Prev Med Public Health (2020) 53:171–4. doi:10.3961/jpmph.20.094
24. Erku, DA, Belachew, SA, Abrha, S, Sinnollareddy, M, Thomas, J, Steadman, KJ, et al. When Fear and Misinformation Go Viral: Pharmacists' Role in Deterring Medication Misinformation during the 'infodemic' Surrounding COVID-19. Res Soc Administrative Pharm (2021) 17:1954–63. doi:10.1016/j.sapharm.2020.04.032
25. Gonzalez, R, and Morán, CLF. The 2019-2020 Chilean Protests: A First Look at Their Causes and Participants. Int J Sociol (2020) 50:227–35. doi:10.1080/00207659.2020.1752499
26.OECD. Trust in Government (Indicator) (2020). doi:10.1787/cc9669ed-en Retrieved from: https://www.oecd-ilibrary.org/governance/trust-in-government/indicator
27. Quinn, SC, Parmer, J, Freimuth, VS, Hilyard, KM, Musa, D, and Kim, KH. Exploring Communication, Trust in Government, and Vaccination Intention Later in the 2009 H1N1 Pandemic: Results of a National Survey. Biosecur Bioterror biodefense strategy, Pract Sci (2013) 11:96–106. doi:10.1089/bsp.2012.0048
28. Freimuth, VS, Musa, D, Hilyard, K, Quinn, SC, and Kim, K. Trust during the Early Stages of the 2009 H1N1 Pandemic. J Health Commun (2014) 19:321–39. doi:10.1080/10810730.2013.811323
29. Prati, G, Pietrantoni, L, and Zani, B. Compliance with Recommendations for Pandemic Influenza H1N1 2009: the Role of Trust and Personal Beliefs. Health Educ Res (2011) 26:761–9. doi:10.1093/her/cyr035
30. van der Weerd, W, Timmermans, DR, Beaujean, DJ, Oudhoff, J, and van Steenbergen, JE. Monitoring the Level of Government Trust, Risk Perception and Intention of the General Public to Adopt Protective Measures during the Influenza A (H1N1) Pandemic in the Netherlands. BMC public health (2011) 11:575–12. doi:10.1186/1471-2458-11-575
31. Liao, Q, Cowling, B, Lam, WT, Ng, MW, and Fielding, R. Situational Awareness and Health Protective Responses to Pandemic Influenza A (H1N1) in Hong Kong: a Cross-Sectional Study. PLoS one (2010) 5:e13350. doi:10.1371/journal.pone.0013350
32. Mesch, GS, and Schwirian, KP. Social and Political Determinants of Vaccine Hesitancy: Lessons Learned from the H1N1 Pandemic of 2009-2010. Am J Infect Control (2015) 43:1161–5. doi:10.1016/j.ajic.2015.06.031
33. Choi, D-H, Shin, D-H, Park, K, and Yoo, W. Exploring Risk Perception and Intention to Engage in Social and Economic Activities during the South Korean MERS Outbreak. Int J Commun (2018) 12:21.
34. Kim, CW, and Song, HR. Structural Relationships Among Public’s Risk Characteristics, Trust, Risk Perception and Preventive Behavioral Intention: The Case of MERS in KoreaStructural Relationships Among Public's Risk Characteristics, Trust, Risk Perception and Preventive Behavioral Intention - the Case of MERS in Korea -. Crisis Emerg Manag (2017) 13:85–95. doi:10.14251/crisisonomy.2017.13.6.85
35. Brodeur, A, Grigoryeva, I, and Kattan, L. Stay-at-home Orders, Social Distancing and Trust: Global Labor Organization (GLO). EssenGermany: Essen (2020).
36. Olivera-La Rosa, A, Chuquichambi, EG, and Ingram, GPD. Keep Your (Social) Distance: Pathogen Concerns and Social Perception in the Time of COVID-19. Personal Individual Differences (2020) 166:110200. doi:10.1016/j.paid.2020.110200
37. Storopoli, J, Braga da Silva Neto, WL, and Mesch, GS. Confidence in Social Institutions, Perceived Vulnerability and the Adoption of Recommended Protective Behaviors in Brazil during the COVID-19 Pandemic. Soc Sci Med (2020) 265:113477. doi:10.1016/j.socscimed.2020.113477
38. Uddin, S, Imam, T, Khushi, M, Khan, A, and Moni, MA. How Did Socio-Demographic Status and Personal Attributes Influence Compliance to COVID-19 Preventive Behaviours during the Early Outbreak in Japan? Lessons for Pandemic Management. Personal Individual Differences (2021) 175:110692. doi:10.1016/j.paid.2021.110692
39. Lim, VW, Lim, RL, Tan, YR, Soh, AS, Tan, MX, Othman, NB, et al. Government Trust, Perceptions of COVID-19 and Behaviour Change: Cohort Surveys, Singapore. Bull World Health Organ (2021) 99:92–101. doi:10.2471/blt.20.269142
40. Chan, HF, Brumpton, M, Macintyre, A, Arapoc, J, Savage, DA, Skali, A, et al. How Confidence in Health Care Systems Affects Mobility and Compliance during the COVID-19 Pandemic. PloS one (2020) 15:e0240644. doi:10.1371/journal.pone.0240644
41. Latkin, CA, Dayton, L, Yi, G, Konstantopoulos, A, and Boodram, B. Trust in a COVID-19 Vaccine in the US: A Social-Ecological Perspective. Soc Sci Med (1982) 2021:270113684. doi:10.1016/j.socscimed.2021.113684
42. Lazarus, JV, Ratzan, SC, Palayew, A, Gostin, LO, Larson, HJ, Rabin, K, et al. A Global Survey of Potential Acceptance of a COVID-19 Vaccine. Nat Med (2021) 27:225–8. doi:10.1038/s41591-020-1124-9
43. Urrunaga-Pastor, D, Bendezu-Quispe, G, Herrera-Añazco, P, Uyen-Cateriano, A, Toro-Huamanchumo, CJ, Rodriguez-Morales, AJ, et al. Cross-sectional Analysis of COVID-19 Vaccine Intention, Perceptions and Hesitancy across Latin America and the Caribbean. Trav Med Infect Dis (2021) 41:102059. doi:10.1016/j.tmaid.2021.102059
44. Skjefte, M, Ngirbabul, M, Akeju, O, Escudero, D, Hernandez-Diaz, S, Wyszynski, DF, et al. COVID-19 Vaccine Acceptance Among Pregnant Women and Mothers of Young Children: Results of a Survey in 16 Countries. Eur J Epidemiol (2021) 36:197–211. doi:10.1007/s10654-021-00728-6
45. Sandoval, AV, Calixto, MBG, and Salazar, M. Colombia: Innovation, Trust and Emotions during the COVID-19 Pandemic. Management Res J Iberoamerican Acad Management (2020) 19. 1–21. doi:10.1108/mrjiam-05-2020-1040
46. Slovic, P. Perceived Risk, Trust, and Democracy. In: Cvetkovich G,, and Löfstedt R, editors. Social Trust and the Management of Risk. London: Earthscan Publications Ltd (2000). p. 42–52.
47. Bouckaert, G, and Van de Walle, S. Government Performance and Trust in Government. In: Proceedings of Ponencia presentada en la annual conference of the European group on public administration. vaasa (Finlandia). p. 19–42.
48. Johnson, BB. Exploring Dimensionality in the Origins of hazard-related Trust. J Risk Res (1999) 2:325–54. doi:10.1080/136698799376763
49. Metlay, D. Institutional Trust and Confidence: A Journey into a Conceptual Quagmire. In: Cvetkovich G,, and Löfstedt R, editors. Social Trust and the Management of Risk. London: Earthscan Publications Ltd. (1999). p. 100–16.
50. Paek, H-J, Hilyard, K, Freimuth, VS, Barge, JK, and Mindlin, M. Public Support for Government Actions during a Flu Pandemic: Lessons Learned from a Statewide Survey. Health Promot Pract (2008) 9:60S–72S. doi:10.1177/1524839908322114
51. Enria, L, Waterlow, N, Rogers, NT, Brindle, H, Lal, S, Eggo, RM, et al. Trust and Transparency in Times of Crisis: Results from an Online Survey during the First Wave (April 2020) of the COVID-19 Epidemic in the UK. PloS one (2021) 16:e0239247. doi:10.1371/journal.pone.0239247
52. Jovančević, A, and Milićević, N. Optimism-pessimism, Conspiracy Theories and General Trust as Factors Contributing to COVID-19 Related Behavior - A Cross-Cultural Study. Pers Individ Dif (2020) 167:110216. doi:10.1016/j.paid.2020.110216
53. Monge-Rodríguez, FS, Jiang, H, Zhang, L, Alvarado-Yepez, A, Cardona-Rivero, A, Huaman-Chulluncuy, E, et al. Psychological Factors Affecting Risk Perception of COVID-19: Evidence from Peru and China. Ijerph (2021) 18:6513. doi:10.3390/ijerph18126513
54. Siegrist, M, and Cvetkovich, G. Perception of Hazards: The Role of Social Trust and Knowledge. Risk Anal (2000) 20:713–20. doi:10.1111/0272-4332.205064
55. Ajzen, I. The Theory of Planned Behavior. Organizational Behav Hum Decis Process (1991) 50:179–211. doi:10.1016/0749-5978(91)90020-t
56. Ajzen, I. The Theory of Planned Behavior: Frequently Asked Questions. Hum Behav Emerg Tech (2020) 2:314–24. doi:10.1002/hbe2.195
57. Gerber, MM, Cuadrado, C, Figueiredo, A, Crispi, F, Jiménez‐Moya, G, and Andrade, V. Taking Care of Each Other: How Can We Increase Compliance with Personal Protective Measures during the COVID‐19 Pandemic in Chile? Polit Psychol (2021) 42:863–80. doi:10.1111/pops.12770
58. Miller, ZD. The Enduring Use of the Theory of Planned Behavior. Hum Dimensions Wildl (2017) 22:583–90. doi:10.1080/10871209.2017.1347967
59. Conner, M, and Abraham, C. Conscientiousness and the Theory of Planned Behavior: Toward a More Complete Model of the Antecedents of Intentions and Behavior. Pers Soc Psychol Bull (2001) 27:1547–61. doi:10.1177/01461672012711014
60. Schmiege, SJ, Bryan, A, and Klein, WMP. Distinctions between Worry and Perceived Risk in the Context of the Theory of Planned Behavior. J Appl Soc Psychol (2009) 39:95–119. doi:10.1111/j.1559-1816.2008.00431.x
61. Bronfman, NC, Cisternas, PC, López-Vázquez, E, and Cifuentes, LA. Trust and Risk Perception of Natural Hazards: Implications for Risk Preparedness in Chile. Nat Hazards (2016) 81:307–27. doi:10.1007/s11069-015-2080-4
62. Chapman, GB, and Coups, EJ. Emotions and Preventive Health Behavior: Worry, Regret, and Influenza Vaccination. Health Psychol (2006) 25:82–90. doi:10.1037/0278-6133.25.1.82
63. Cheng, C, and Ng, A-K. Psychosocial Factors Predicting SARS-Preventive Behaviors in Four Major SARS-Affected Regions. J Appl Soc Psychol (2006) 36:222–47. doi:10.1111/j.0021-9029.2006.00059.x
64. Kline, RB. Principles and Practice of Structural Equation Modeling. New York, NY: Guilford (2015).
65. Ro, J-S, Lee, J-S, Kang, S-C, and Jung, H-M. Worry Experienced during the 2015 Middle East Respiratory Syndrome (MERS) Pandemic in Korea. PloS one (2017) 12:e0173234. doi:10.1371/journal.pone.0173234
Keywords: COVID–19, protective behaviors, worry, subjective norms, government trust
Citation: Bronfman N, Repetto P, Cisternas P, Castañeda J and Cordón P (2022) Government Trust and Motivational Factors on Health Protective Behaviors to Prevent COVID-19 Among Young Adults. Int J Public Health 67:1604290. doi: 10.3389/ijph.2022.1604290
Received: 11 June 2021; Accepted: 22 March 2022;
Published: 13 April 2022.
Edited by:
Lyda Osorio, University of Valle, ColombiaReviewed by:
Katarzyna Krot, Bialystok University of Technology, Bialystok, PolandCopyright © 2022 Bronfman, Repetto, Cisternas, Castañeda and Cordón. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nicolás Bronfman, bmJyb25mbWFuQHVuYWIuY2w=