 B. Heidi Ellis1*Alisa B. Miller1Georgios Sideridis1Rochelle Frounfelker2Diana Miconi2Saida Abdi3Farah Aw-Osman4Cecile Rousseau2
B. Heidi Ellis1*Alisa B. Miller1Georgios Sideridis1Rochelle Frounfelker2Diana Miconi2Saida Abdi3Farah Aw-Osman4Cecile Rousseau2- 1Department of Psychiatry and Behavioral Sciences, Boston Children’s Hospital and Harvard Medical School, Boston, MA, United States
- 2Department of Psychiatry, McGill University, Montréal, QC, Canada
- 3School of Social Work, University of Minnesota, St. Paul, MN, United States
- 4Canadian Friends of Somalia, Ottawa, ON, Canada
Objectives: We examine the association between perceived discrimination, mental health, social support, and support for violent radicalization (VR) in young adults from three locations across two countries: Montréal and Toronto, Canada, and Boston, United States. A secondary goal is to test the moderating role of location.
Methods: A total of 791 young adults between the ages of 18 and 30, drawn from the Somali Youth longitudinal study and a Canada-based study of college students, participated in the study. We used multivariate linear regression to assess the association between scores on the Radical Intentions Scale (RIS) with demographic characteristics, anxiety, depression, social support, and discrimination.
Results: In the full sample, discrimination, age, and gender were associated with RIS scores. When we examined moderation effects by location, RIS scores were associated with depression only in Montréal, and with social support (negatively) and discrimination in Toronto. None of the variables were significant in Boston.
Conclusion: These findings suggest that an understanding of risk and protective factors for support of VR may be context-dependent. Further research should take into consideration local/regional differences.
Introduction
Violent radicalization (VR) is a significant and growing threat worldwide [1, 2]. VR can be understood as “an individual or collective process whereby normal practices of dialogue, compromise, and tolerance between groups/individuals with diverging interests are abandoned and one or more groups/individuals engage in violent actions to reach a specific (political, social, religious) goal” [3]. In a context of increased social polarization, VR is affecting both majorities and minorities, targeting different forms of otherness: racial, ethnic, religious, political and gender-related (e.g., [4]). There is interest in understanding and addressing both proximal and distal risk factors that contribute to the process of VR [5]. This shift calls for a public health approach that entails distinguishing between primary, secondary, and tertiary prevention efforts [6]. Primary prevention constitutes a focus on determinants of VR opinions and attitudes in the general population, intending to prevent VR through community-based programming that emphasizes positive civic engagement, global citizenship, and constructive dialogue on polarizing issues [7].
Recent years have seen an increase in empirical work seeking to identify individual-level risk and protective factors related to VR. This research has produced inconclusive results. In a recent systematic scoping review of factors related to VR, relative deprivation of a social group—including grievances, injustices, victimization, and stigmatization—was the most common risk factor identified for radicalization to international extremism [8]. Experiences of discrimination have been linked to VR, particularly when those experiences are thought to be on the basis of language or political views [9, 10]. However, no relation between perceived discrimination and sympathy for VR was found in a sample of Muslims in England [11]. In addition, Somali youth and young adults who endorsed support for VR reported moderate, but not high, levels of exposure to discrimination in the North American context [12].
A range of psychological factors are associated with VR, some of them potentially operating as mediators between grievances and VR. Rousseau and colleagues (2019) report that depression accounts for 25% of the relationship between grievances (i.e., experiences of discrimination) and sympathy for VR [10]. Importantly, the exact association between mental health and VR is unclear; mental health symptoms—depression, in particular—are generally predictive of extremist attitudes only in conjunction with other factors [13]. These mixed findings may be partially explained by differences in study populations and local influences specific to each country.
A socio-ecological framework posits that micro, meso and macro-level risk and protective factors uniquely contribute to, and interact with one another, to produce vulnerability and resilience to radicalization [6]. As such, there is a need to move beyond a focus on individual-level risk factors and examine the relationship between larger sociopolitical contexts and support of VR. VR is a complex phenomenon that varies in expression based on the unique social, cultural, and historical contexts of diverse societies [14]. Such research entails identifying the contribution of area-level effects (such as cities, regions, and countries) on support and endorsement of radical ideology [15]. To date, empirical evidence exploring the role played by the larger social context is extremely limited, with some preliminary work indicating country and regional variations in risk factors for support of VR [16, 17].
Context of Violent Radicalization in Toronto, Montréal and Boston
Discourse and events related to VR vary widely across different locales. In Canada, VR became a heated political issue after the aborted Toronto attacks associated with religious radicalization in 2006. In this incident, a group of 18 youth (known as the “Toronto 18”) was arrested on terrorism charges. These arrests led to negative portrayal of Muslims in the media and growing suspicion and mistrust of Muslims in public opinion. Miller and Sack [18] examined over 200 newspaper columns, opinions and letters to the editor in the aftermath of this event. They conclude that a “significant portion of the published commentary raised an unreasonable public alarm, cast suspicion on the followers of a major religion and impugned Islam itself” (p. 279). As one of the biggest and most visible Muslim groups in Toronto, Somalis were impacted by this event and its aftermath, especially as some of those arrested were Somali. In the province of Quebec (Canada), an attack by a lone actor in St-Jean and the departure of Montréal youth to join DAESH in Syria in 2015, brought VR under the spotlight in 2014. Subsequently, a deadly attack against a mosque in the city of Québec in 2017 highlighted the increasing attraction exerted by different extremist discourses (extreme right and religious) in youth. These events occurred as heated public debates about immigration and cultural and religious diversity highlighted the sharp divide between the very cosmopolitan city of Montréal and the relatively more homogenous rest of Québec. Although social polarization and the associated upsurge in extremist movements has been notable both in Toronto and in Montréal, the specific local forms of intercommunity tensions are shaped by different historical and social factors in both cities: the multiculturalism ideology in Toronto and the tensions around the French language and identity in Montréal.
Similarly, the United States has experienced extremist attacks from diverse ideologies including far right, far left, and religious radicalization [19]. Within Boston, the Boston Marathon bombings of 2013, perpetrated by two brothers who espoused religious extremist ideology, drew national and international attention. In the wake of these bombings, public discourse with in Boston united around the slogan of “Boston Strong,” a call for perseverance in the face of hurt, unity across religious and ethnic lines, and rejection of hate [20, 21], although some segments of society responded to the events with bias and discrimination such as believing Islam is more likely than other religions to encourage violence [22, 23] and recommending the profiling of young Muslim men [24].
Understanding common vs. unique risk and protective factors for VR between populations and geographical settings has critical implications for cross-cultural applicability of research findings and, ultimately, how local governments or communities seek to shape programs and policies to reduce VR in their regions. In this study, we seek to further this nascent body of research by examining the association between psychosocial risk factors and support for VR across different populations (Somali and general population youth) in three different urban cosmopolitan settings spanning two countries: Montréal and Toronto, Canada, and Boston, United States. Specifically, we examine the association of discrimination, depression, anxiety (risk factors), and social support (protective factor) with support for VR. We hypothesized that after controlling for age and gender, each of the above risk and protective factors would be associated with support for VR. We further hypothesized that patterns of associations would differ by city.
Methods
Population Studied
The following analyses utilize pooled data from the multi-site Somali Youth Longitudinal Study (SYLS) and a multi-site college study in Canada.
Boston and Toronto
Current analyses draw on data from 198 Somali young adults located either in Boston or Toronto who participated in Wave 2 (data collected between 2014 and 2015) of SYLS. SYLS eligibility included having lived in the United States or Canada for at least 1 year, either born in Somalia or being of Somali descent, and being between the ages of 18 and 30 at the time of initial enrollment. Multiple strategies including snowball sampling and spreading information about SYLS through community meetings were used to recruit participants.
Montréal
Students from fourteen colleges in Québec, Canada participated in a study on sympathy for VR from 2016 to 2017. Participants were eligible to participate if they were registered as full-time students in one of the participating colleges. The response rate varied greatly between the colleges, ranging from 2 to 19%. Only respondents in the greater Montréal area were included in this analysis (n = 593 from six colleges).
Measures
Demographics Variables
Participants were asked to self-report demographic variables. Gender was self-reported as a dichotomous variable (male/female) in SYLS. Participants self-reported their gender as male, female or other in the college survey. Age was reported as a continuous variable in SYLS (how old are you?) and a categorical variable in the college survey (18, 19–21, 22–24, 25–27, 28–30, and 31+). For the purposes of these analyses, SYLS age data were coded into six categories to match the college study. The location of interview was recorded by SYLS staff and in the college study, participants identified the college they attended. All SYLS participants were of Somali ethnicity. In the college study, participants self-reported whether or not they (and their mother/father) were born in Canada and if not, asked to specify what region of the world they had been born.
Radicalism Intention Scale
The RIS is a four-item subscale of the Activism and Radicalism Intention Scales (ARIS; [25]; that measures an individual’s readiness to participate in illegal and violent behavior for one’s group or organization (support of VR). Respondents rate their agreement to statements on a seven-point Likert scale, ranging from 1 (disagree completely) to 7 (agree completely). A sample item is, “I would participate in a public protest against oppression of my group even if I thought the protest might turn violent.” Of note, an adapted version of the RIS was used for SYLS participants in order to increase acceptability within the Somali community. More specifically, items were rephrased to assess attitudes towards someone who commits legal or illegal actions, vs. personal intentions to commit these actions. A mean score was calculated with higher scores indicating more support for violent radicalization. Both the original ARIS and the adapted ARIS have demonstrated good psychometric properties [9, 25, 26]. Cronbach’s alpha for support of VR in this study were acceptable (alpha = 0.858; alpha = 0.861; alpha = 0.878) for Boston, Toronto, and Montréal respectively.
Discrimination
The Everyday Discrimination Scale (EDD [27]; is a nine-item measure of perceived discrimination, assessing day-to-day experiences of discrimination. Sample items include “being treated with less courtesy than other people” and “people act as if they think you are dishonest.” Seven options for frequency of occurrence provided ranged from “never” to “almost every day.” Responses were dichotomized into “never” and “occurred.” A mean score was calculated with higher scores indicating higher levels of discrimination. The EDD has demonstrated validity and reliability [28, 29]. Cronbach’s alpha for discrimination were good (alpha = 0.813; alpha = 0.866; alpha = 0.874) for Boston, Toronto, and Montréal respectively.
Mental Health
The depression and anxiety subscales of the Hopkins Symptoms Checklist (HSCL [30]; were used to measure mental health. The depression subscale is a 15-item subscale that measures symptoms and problems related to depression. For the current study, a 14-item depression subscale was used as one item (sexual interest) was removed in SYLS to increase acceptability; this item was dropped from the Québec data in the current analyses. The anxiety subscale consists of ten items measuring symptoms and problems related to anxiety. Respondents are asked to reflect on the past 4 weeks only and indicate how much they have had the identified symptoms or problems on a 4-point Likert scale, ranging from “not at all” to “extremely.” A mean score for each subscale was calculated with higher scores indicating more symptomology. The HSCL has demonstrated good psychometrics in immigrant groups [31]. Cronbach’s alpha for anxiety were good (alpha = 0.828; alpha = 0.808; alpha = 0.868) and for depression in this study were good to excellent (alpha = 0.872; alpha = 0.869; alpha = 0.920) for Boston, Toronto, and Montréal respectively.
Multidimensional Scale of Perceived Social Support
The MSPSS [32] is a twelve-item self-report measure of social support inclusive of three subscales (family, friends, and significant others). Two items from each of the two subscales (family and friends) were used in the current study. Respondents rate their agreement to four statements on a seven-point Likert scale, ranging from 1 (strongly disagree) to 7 (strongly agree). A sample item is, “my family really tries to help me.” A mean score for the four items was calculated with higher scores indicating more social support from family/friends. The MSPSS has demonstrated reliability and validity [10].
Procedures
Boston and Toronto
All procedures were performed in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards; the Institutional Review Board of Boston Children’s Hospital and the REB of Carlton University approved the SYLS. In SYLS, informed consent was obtained by Somali study staff and quantitative interviews were administered verbally in English by non-Somali research staff. Participants were paid $60 as a thank you for their time.
Montréal
The study protocol and procedures were approved by the Ethics Committee of the Centre Integré Universitaire de Santé et de Services Sociaux du Centre-Ouest-de-l’Ile-de-Montréal (CIUSSS-CODIM). In addition, the research ethics board of each college gave approval prior to data collection. Researchers uploaded the questionnaire on an intranet portal used by colleges to communicate with students and remained online for a month. Participants completed the survey in either French or English, depending upon their preference. The project was described as a research study on adaptation to the current social context in the province of Québec (Canada). Students were informed that their involvement was voluntary and that their responses would be confidential. Students consented to be part of the study on the first page of the survey. Participants were able to discontinue the survey at any time. Contact information of research team and ethics board members were made available to answer any questions or concerns regarding the study.
Data Analyses
First, descriptive analyses were conducted. Table 1 provides demographic information and means of variables of interest of study participants by location.
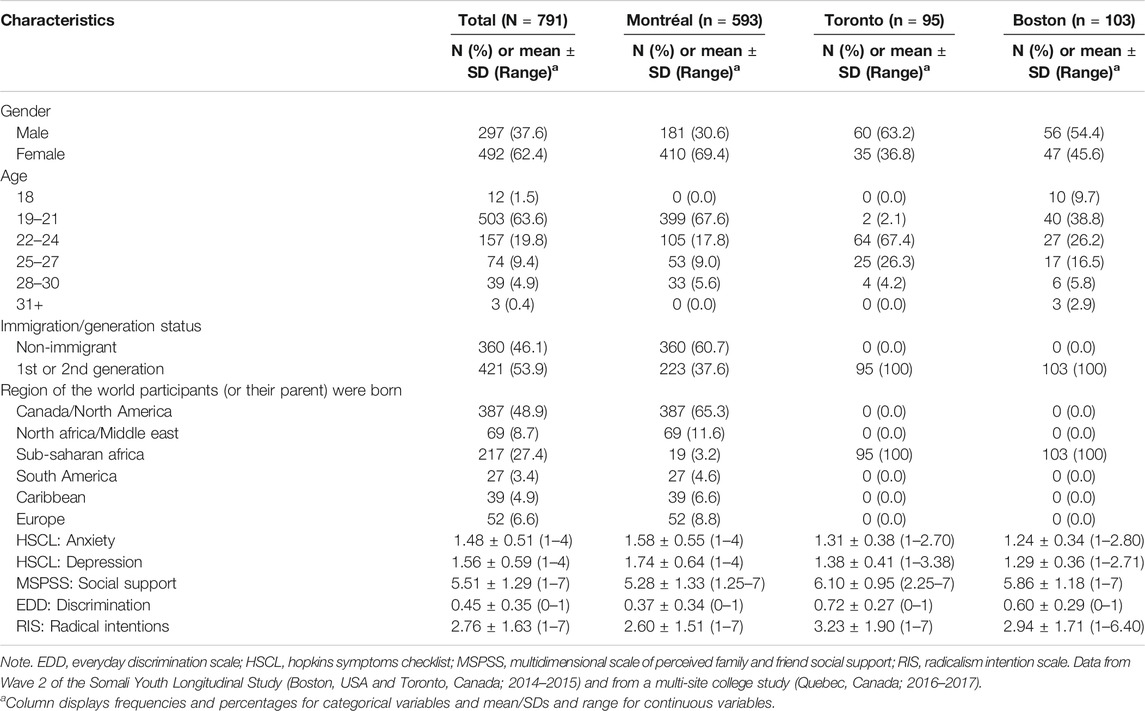
TABLE 1. Demographic information of study participants by location.
Multiple Regression Analysis
Data were analyzed by means of a multiple predictors linear regression analysis model using maximum likelihood estimation and the engagement of robust standard errors due to accounting for not meeting normality assumptions. Missing data ranged between 10.7 and 29.8%. Listwise deletion was used to engage only full cases. To ensure that listwise deletion did not result in biased point and variance estimates, means/SDs were estimated using full data and the sample involving full cases only. Results indicated minuscule differences in the estimates of the two datasets: Anxiety (Mfull = 1.4773, MListwise = 1.4753), Depression (Mfull = 1.5951, MListwise = 1.5883), Radicalism (Mfull = 2.7608, MListwise = 2.7778), social support (Mfull = 5.5086, MListwise = 5.5896), and discrimination (Mfull = 0.4510, MListwise = 0.4645). Consequently, it was concluded that listwise deletion did not result in distorted point estimates. Model fit is not evaluated using omnibus criteria as it is a saturated model; instead, each predictor is evaluated for significance using partial regression coefficients, accounting for the presence of all other predictors in the model. The level of significance was set to 5% for a two-tailed test, in light of the power estimation shown below. Further between-group comparisons were made by use of the Wald test, through specifying equivalence constraints across partial regression coefficients in two groups at a time. All analyses were conducted using Mplus 8.5.
Power Analysis
Power for a linear regression model was estimated using six independent variables for the prediction of radicalism. Using a medium effect size of a multiple correlation equal to 0.15, power levels equal to 80% and a two-tailed test using a nominal alpha level of 5%, a sample size of 97 full cases would achieve power levels equal to 80% [33]. We further explored power by estimating the required sample size to estimate as significant standardized slopes equal to 0.3, representing medium-level effects [33]. Using a Monte Carlo simulation positing standardized slopes equal to 0.30 with sample sizes of n = 94 (representing the smallest group) and 1,000 replicated samples, results indicated that power levels of the 0.3 slope coefficients were equal to 81.3% with mean coverage levels equal to 94.8% (in the 1,000 replicated samples). Consequently, the present study had ample levels of power for evaluating the predictive ability of these linear predictors.
Results
Table 2 presents intercorrelations between measured variables across locations. Notable correlations were a strong positive relationship between anxiety and depression across locations (ranging between r = 0.710 and r = 0.797), the positive correlation between discrimination and anxiety/depression across locations (ranging between r = 0.235 and r = 0.351), and a negative relationship between age and radicalism consistently across areas (ranging between −0.162 and −0.294). The remaining relationships varied across locations; for example, a negative relationship between social support and discrimination was observed for Montréal and Toronto (ranging between r = −0.178 and r = −0.187) but was non-significant in the Boston area. Similarly, social support related negatively with anxiety and depression in Montréal and Toronto (ranging between r = −0.182 and r = −0.381), but not Boston (where only depression was significant).
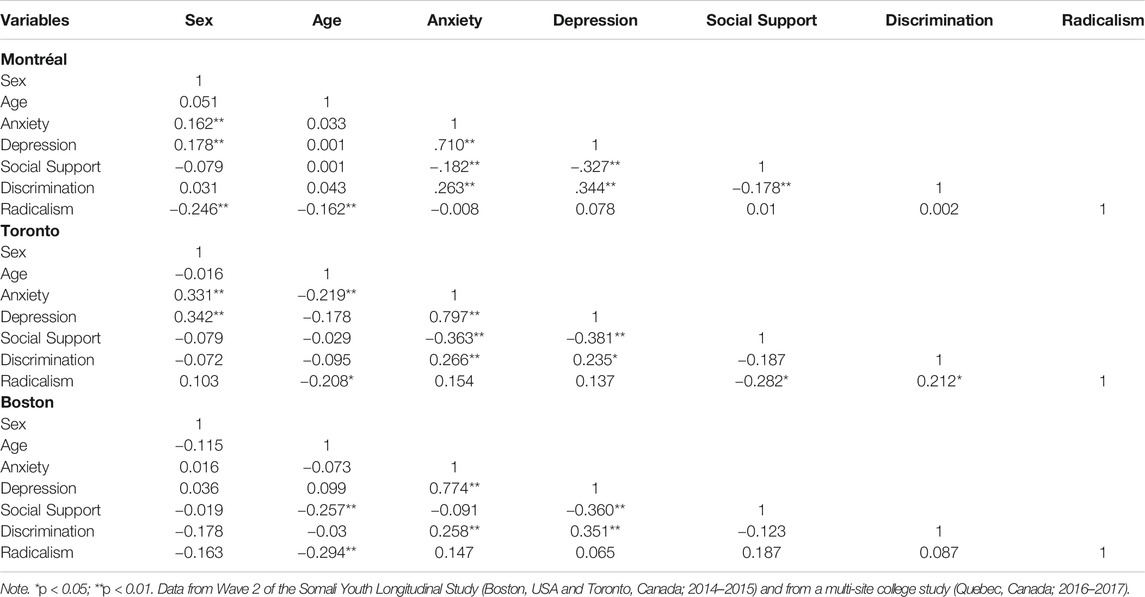
TABLE 2. Intercorrelations between measured variables by location.
Prediction of Violent Radicalization Using Radical Intention Scores From Personal Characteristics
Figure 1 displays the findings from using the full sample (i.e., aggregating data across all locations). As shown in the figure, among predictors of radical intention scores (RIS), those that exceeded conventional levels of significance were gender, age, and level of discrimination. Concerning gender, being a female was associated with significantly lower scores on the RIS compared to being a male (b = −0.195, p < 0.05) and older individuals had lower RIS scores (b = −0.204, p < 0.05). With regard to discrimination, the higher the levels of discrimination the higher the scores on the RIS (b = 0.099, p < 0.05). The total amount of variance of radicalism predicted by the linear combination of the independent variables was 6%, significantly different from zero. This effect represents a medium effect size based on [33] suggestions of medium level predictions using r-square related indices (i.e., small = 0.01, medium = 0.06, large = 0.14).
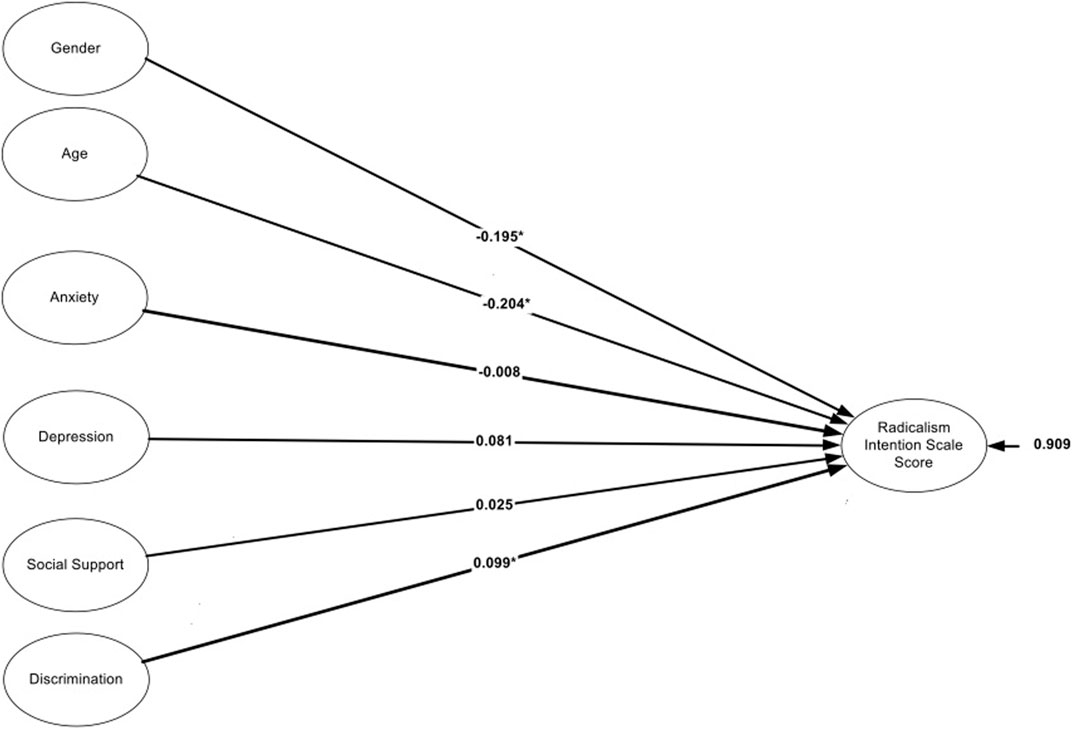
FIGURE 1. Prediction of radicalism intention scale score from demographics and psychological measures for the full data. Data from Wave 2 of the Somali Youth Longitudinal Study (Boston, USA and Toronto, Canada; 2014–2015) and from a multi-site college study (Quebec, Canada; 2016–2017).
Moderated Regression Predicting Violent Radicalization From Personal Characteristics by Area
Table 3 displays the findings from the moderated regression analysis using location as the grouping variable (see also Figure 2). Being a female was associated with lower radicalism scores in Montréal compared to Toronto (DiffSlope = −0.39, p < 0.05) and in Boston in relation to Toronto (DiffSlope = −0.35, p < 0.05). Age was not a significant moderator as its negative propensities in predicting radicalism were consistent across locations. Similarly, there were no moderated effects due to anxiety, which was consistently not predictive of levels of radicalism across all locations. The moderated effects of depression were evident as it exerted positive effects on radicalism using the Montréal only sample; the effects of depression in Toronto and Boston were null. Social support exerted negative effects on radicalism in Toronto only (b = −0.28) with the respective slopes in Montréal and Boston being non-significant. Last, discrimination was a significant moderator as its effects were significantly more pronounced in Toronto compared to Montréal and Boston. Specifically, the higher the levels of discrimination the higher the levels of radicalism in the Toronto area. All other effects were null.
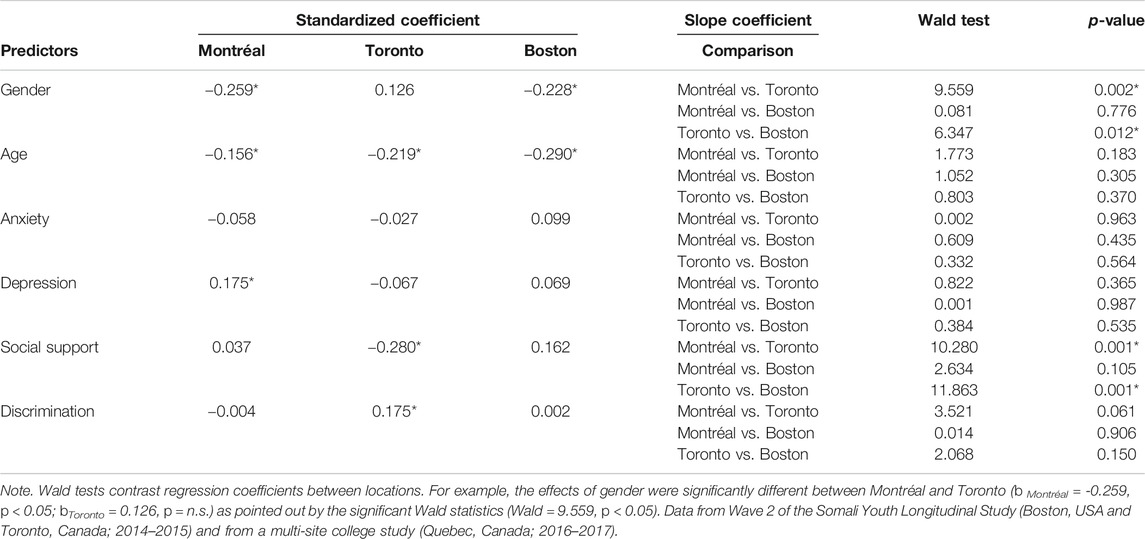
TABLE 3. Comparison between regression coefficients across locations using the wald test.
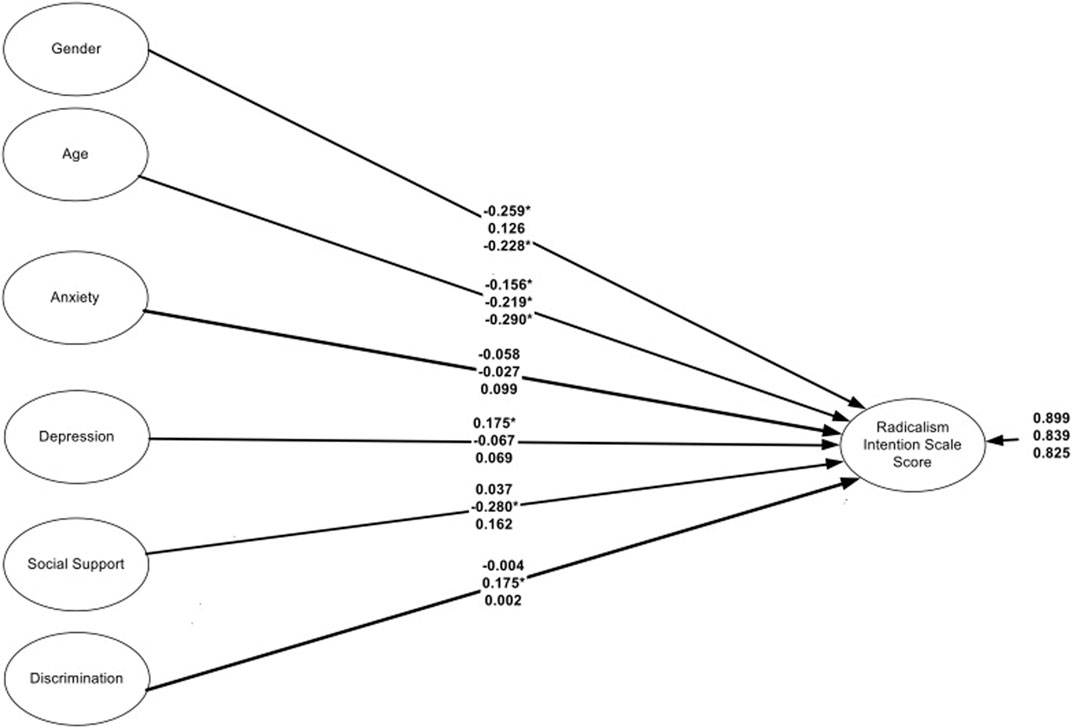
FIGURE 2. Prediction of radicalism intention scale score from linear predictors by location. Coefficients are standardized. The order of the coefficients is as follows first = Montréal, middle = Toronto, last = Boston. Data from Wave 2 of the Somali Youth Longitudinal Study (Boston, USA and Toronto, Canada; 2014–2015) and from a multi-site college study (Quebec, Canada; 2016–2017).
Discussion
Overall, our findings highlight the importance of considering contextual differences in risk and protective factors associated with support of VR. When data from the three cities were pooled, discrimination, age, and gender were associated with support of VR. However, each of the three cities provided different pictures of the relative importance of various risk and protective factors in relation to support of RV.
In Montréal the predominance of depression as a risk factor for a mixed majority-minority sample may reflect the growing feelings of helplessness and insecurity of Montréal youth, which have been documented repeatedly [34], and its association with a negative view of the future [35]. For this generation, the adoption of a dystopian view of life seems to be a strategy to confront the uncertain future and represent the existential doom associated with it (Venkatesh et al, 2019). Thus the endorsement of attitudes legitimizing violence by depressed youth can be seen as a cultural shift in idioms of distress associated with pain and despair, just as, in previous generations, self-mutilation has become a challenge to security oriented societies [36]. The relatively smaller portion of minorities in this sample may also lessen the importance of discrimination as a risk factor. Furthermore, college students may differ from the young adults included in the Boston and Toronto samples (which included both students and non-students) in other ways, such as a sense of opportunity, which may also have contributed to the diminished role of discrimination.
In Toronto discrimination and social support both significantly predicted support of VR. The potency of these particular variables in our Toronto sample, which consists of ethnic Somalis, may highlight the way in which belonging to an ethnic minority group in a multicultural society can offer both risk and protection. A greater openness to the use of violence among those who experienced high levels of discrimination may be a more externalized response to suffering, and one that on some level reflects anger and a lack of complacency in accepting marginalization as the status quo. Connection to community, in contrast, may serve to buffer a sense of marginalization and is associated with reduced support for attitudes that legitimize violence. Notably, gender did not predict support of VR, a finding that may be explained by the salience of grievances resulting from a sense of injustices perpetuated against a vulnerable community by powerful institutions such as law enforcement and the media. Such powerful grievances may be common across males and females, and supercede potential gender differences.
There are a number of reasons, both methodological and theoretical, that may explain variation in findings based on location. First, the differences are likely a reflection of the populations drawn on for this pooled dataset. While differences in method and population cannot be ignored, if differences between models were due solely to this than findings from Toronto and Boston should have been similar. The fact that the Toronto model demonstrated significant associations between support for VR and both discrimination and low social belonging, while neither of these factors was significant in the Boston sample, suggests that regional differences remain even when study methods and ethnic composition of samples is the same.
Second, findings may be a reflection of regional sociopolitics or cultural discourse related to issues such as discrimination or mental health, and cultural idioms of distress. Sociopolitical or cultural differences within the various regions may contribute to varying levels of comfort in reporting different variables. Furthermore, sociopolitical differences between different regions may lead to fundamentally distinct experiences which, in turn, leads to different forces shaping support of VR. Within Toronto, discrimination was not only highly predictive of support of VR, but was also more prevalent compared to levels experienced by the same ethnic community in Boston. An important question to further explore is whether discrimination is such a potent risk factor in Toronto in part due to the more ubiquitous nature of such experiences.
Another possibility is that the discourse within Toronto and Boston on Somalis and radicalism differs as a result of recent sociopolitical events, and this in turn shapes the risk factors for radicalism. The focus on the Somali community in Toronto related to the “Toronto 18,” vs the “Boston Strong” discourse that followed the Boston marathon bombings may have led to different contexts of perceived safety among Somalis when talking about radicalism. In a context of perceived safety, hypothesized under this framing to be more salient in Boston, endorsement of support for VR on a questionnaire may reflect an underlying comfort and stability, rather than grievance. In this case, variables reflecting distress or adversity (e.g. discrimination or depression) may be less expected to relate to higher levels of support of radicalism. In contrast, in a setting where mention of radicalism carries with it overtones of threat and stigma, support of radicalism may be a reflection of high distress as opposed to comfort and stability. Further work understanding local strains and distress, and how local media or events may create conditions of perceived safety or threat, may help to elucidate additional variables that should be included to capture regional experiences that may relate to support of VR.
Limitations
There are several limitations to this study. First, data is cross-sectional and we cannot make causal inferences about the relationship between study variables. Cross-site comparisons are also limited given differences in study populations and size, particularly when contrasting Montréal, comprised of a racially and ethnically diverse sample of college youth, and Toronto/Boston, comprised of Somali immigrant young adults. Data collection procedures also differed significantly between studies; in particular, the use of an on-line survey in Montréal resulted in low response rate and a study sample that may not be representative of the larger city population. A further methodological difference is that the SYLS used a modified version of the RIS; although this version demonstrated comparable psychometrics, it is likely that the two versions led to different rates of endorsement. An additional limitation is that the variable assessing discrimination did not include structural or systemic racism.
Public Health Implications and Conclusions
This study raises questions about the generalizability of findings related to risk and protective factors for support of VR from one geographical setting and/or population to others. In the broader field of violence prevention, it is well established that local contexts influence patterns of interpersonal violence [37]. Integrating meso and macro-level predictors of support of VR into public health practice entails developing and/or adapting existing primary prevention initiatives and policies to acknowledge and address broader contextual issues that influence support for VR. Although the need for primary prevention initiatives based on a resilience-oriented socio-ecological framework is increasingly emphasized by scholars [15], examples and empirical evaluations of such primary prevention programs are scarce and highlight that they lead to negative outcomes when they targeted specific ethnic, racial or religious groups [38, 39]. At present, most policies and interventions focus on building resilience against the influence of extremist propaganda and narratives in young and vulnerable individuals, failing to address systemic injustices, discrimination, polarized political discourses and violence in our societies [39]. Our findings suggest that primary prevention initiatives should consider that the source of adversity and violence can reside within the social order of a specific local context and thus necessitates adaptation across contexts. Bridging VR prevention policies and social policies aimed at promoting inclusion and social justice, empowering individuals and communities at a local level in a bottom-up approach is a promising way to move forward.
Data Availability Statement
The datasets presented in this article are not readily available because data analyzed in this study are pooled from multiple datasets. Requests to access the datasets should be directed to the Trauma and Community Resilience Center at Boston Children's Hospital, tcrc@childrens.harvard.edu.
Ethics Statement
The studies involving human participants were reviewed and approved by the Institutional Review Board of Boston Children’s Hospital and the Ethics Committee of the Centre Integré Universitaire de Santé et de Services Sociaux du Centre-Ouest-de-l’Ile-de-Montréal. The participants provided their written informed consent to participate in this study.
Author Contributions
BHE was responsible for study design, collaboratively developing the research questions, drafting the background and conclusion, overseeing SYLS data collection, and incorporating feedback from co-authors. AM drafted the SYLS-related methods, supported data analysis and management, collaboratively developed research questions and interpreted results, and contributed to the introduction. GS conducted all analyses and wrote the results section. RF contributed to research question development and to writing the introduction and conclusion, and worked with DM and AM on merging datasets. DM contributed to research question development and to writing the introduction and conclusion, and was the primary Montreal dataset manager. SA co-developed SYLS, ensured community input and involvement at every step, contributed to the introduction and conclusion, and reviewed community and cultural factors with the team to guide study interpretation. FA-O participated in SYLS design and implementation (including ensuring community input and involvement at every step), contributed to the introduction and conclusion, and reviewed community and cultural factors with the team to guide study interpretation. CR oversaw the study from which the Montreal data was drawn and collaboratively developed research questions, hypotheses, methods, and interpretations. All authors reviewed and edited the full manuscript.
Funding
This study was supported by a grant from the Public Safety of Canada (Sponsor; grant 8000-19455). It was also supported in part by the Department of Defense Minerva Research Initiative (grant N00014-13-1-0243) and the National Institute of Justice (grants 2012-ZA-BX-0004 and 2014-ZA-BX-0001).
All procedures performed in studies involving human participants were in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards; the Institutional Review Board of Boston Children’s Hospital and the REB of Carlton University approved the SYLS and the Ethics Committee of the Center Integré Universitaire de Santé et de Services Sociaux du Centre-Ouest-de-l’Ile-de-Montréal (CIUSSS–CODIM) approved the Québec survey study. Informed consent was obtained from all participants in the study.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank Naima Agalab of the Refugee and Immigrant Assistance Center, who has been a partner in our work with the Somali community from the beginning and has provided leadership and training in their efforts to build community leadership teams in other cities. We thank Somali community advisors Fatuma Hussein, Sharif Mohammed, and Rilwan Osman for their guidance and invaluable contribution to this project. We also thank Osob Issa for her efforts on recruitment and obtaining consent. And finally, we thank the community youth who took the time to share their stories.
References
1.National Consortium for the Study of Terrorism and Responses to Terrorism. Annex of statistical information: country reports on terrorism in 2014. College Park, MD: National Consortium for the Study of Terrorism and Responses to Terrorism (2015).
2.Institute for Economics and Peace. Global terrorism index 2018: measuring the impact of terrorism. Sydney, Australia: Institute for Economics and Peace (2018).
3. Schmid, AP. Radicalisation, De-radicalisation, counter-radicalisation: a conceptual discussion and literature review. The Hague, The Netherlands: International Centre for Counter-Terrorism (2013).
4. Stinton, C. Combining the aberrant with the ordinary: the role of white supremacy in the far-right radicalisation of women. J Appl Psychol Soc Sci (2019). 5:86–115.
5. Doosje, B, Moghaddam, FM, Kruglanski, AW, de Wolf, A, Mann, L, and Feddes, AR. Terrorism, radicalization and de-radicalization. Curr Opin Psychol (2016). 11:79–84. doi:10.1016/j.copsyc.2016.06.008
6. Eisenman, DP, and Flavahan, L. Canaries in the coal mine: interpersonal violence, gang violence, and violent extremism through a public health prevention lens. Int Rev Psychiatry (2017). 29:341–349. doi:10.1080/09540261.2017.1343527
7.UNESCO. Preventing violent extremism through education: a guide for policy-makers. Paris, France: UNESCO (2017).
8. Vergani, M, Iqbal, M, Ilbahar, G, and Barton, G. The three ps of radicalization: push, pull and personal. a systematic scoping review of the scientific evidence about radicalization into violent extremism. Stud Confl Terror (2018). 43. 854. doi:10.1080/1057610X.2018.1505686
9. Frounfelker, RL, Frissen, T, Vanorio, I, Rousseau, C, and d’Haenens, L. Exploring the discrimination-radicalization nexus: empirical evidence from youth and young adults in Belgium. Int J Public Health (2019). 64:897–908. doi:10.1007/s00038-019-01226-z
10. Rousseau, C, Hassan, G, Miconi, D, and Lecompte, D. From social adversity to sympathy for violent radicalization: the role of depression, religiosity and social support. Arch Public Heal (2019). 77:1–12. doi:10.1186/s13690-019-0372-y
11. Bhui, K, Silva, MJ, Topciu, RA, and Jones, E. Pathways to sympathies for violent protest and terrorism. Br J Psychiatry (2016). 209:483–490. doi:10.1192/bjp.bp.116.185173
12. Ellis, BH, Abdi, SM, Lazarevic, V, White, MT, Lincoln, AK, Stern, JE, et al. Relation of psychosocial factors to diverse behaviors and attitudes among Somali refugees. Am J Orthopsychiatry (2016). 86:393–408. doi:10.1037/ort0000121
13. Misiak, B, Samochowiec, J, Bhui, K, Schouler-Ocak, M, Demunter, H, Kuey, L, et al. A systematic review on the relationship between mental health, radicalization and mass violence. Eur Psychiatry (2019). 56:51–59. doi:10.1016/j.eurpsy.2018.11.005
14. Borum, R. Radicalization into violent extremism I: a review of social science theories. J Strat Sec (2011). 4:7–36. doi:10.5038/1944-0472.4.4.1
15. Stephens, W, Sieckelinck, S, and Boutellier, H. Preventing violent extremism: a review of the literature. Stud Confl Terror (2018). 44:346–361. doi:10.1080/1057610X.2018.1543144
16. Miconi, D, Calcagnì, A, Mekki-Berrada, A, and Rousseau, C. Are there local differences in support for violent radicalization? a study on college students in the province of Quebec, Canada. Polit Psychol (2020a). doi:10.1111/pops.12718
17. Fahey, S, and Lafree, G. Does country-level social disorganization increase terrorist attacks? Terrorism Polit Vio (2015). 27:81–111. doi:10.1080/09546553.2014.972156
18. Miller, J, and Sack, C. The toronto—18 terror case: trial by media? How newspaper opinion framed Canada’s biggest terrorism case. Int J Divers Organizations (2010). 10:279–296. doi:10.18848/1447-9532/cgp/v10i01/39808
19.National Academies of Sciences E and M. Exploring the use of health approaches in community-level strategies to countering violent extremism and radicalization A workshop (2017). National AcademiesAvailable From: https://www.nationalacademies.org/our-work/exploring-the-use-of-health-approaches-in-community-level-strategies-to-countering-violent-extremism-and-radicalization-a-workshop. (Accessed September 26, 2020).
20. Marcelo, P. “As trial wraps up, Boston Muslims worry about being stereotyped,” in: Northwest Arkansas democr. Nizhny Novgorod, Russia: Gaz (2015).
21. Clauss, KS. Does “Boston strong” mean anything anymore?. in: B Mag. Editor (2016). Available at: https://www.bostonmagazine.com/news/2016/04/17/boston-strong/. (Accessed Sep 26, 2020).
22. Gray, L. Muslim bashing in the wake of Boston bombing. Natl Geogr News (2013). Available From: https://www.nationalgeographic.com/news/2013/4/130426-boston-marathon-bombing-racism-hate-anti-arab-muslim-tamerlan-dzokhar-tsarnaev/#close (Accessed 22 September, 2013).
23.Pew Research Center. After Boston, little change in views of Islam and violence | pew research center (2013). Available From: https://www.pewresearch.org/politics/2013/05/07/after-boston-little-change-in-views-of-islam-and-violence/ (Accessed September 26, 2020).
24. Birnbaum, S. Anti-muslim backlash missing from marathon bombing aftermath. WGBH news (2014). Available From: https://www.wgbh.org/news/post/anti-muslim-backlash-missing-marathon-bombing-aftermath (Accessed 26 September, 2014).
25. Moskalenko, S, and McCauley, C. Measuring political mobilization: the distinction between activism and radicalism. Terrorism Polit Violence (2009). 21:239–260. doi:10.1080/09546550902765508
26. Ellis, BH, Abdi, SM, Horgan, J, Miller, AB, Saxe, GN, and Blood, E. Trauma and openness to legal and illegal activism among somali refugees. Terr Polit Vio (2015). 27:857–883. doi:10.1080/09546553.2013.867849
27. Williams, DR, Yan Yu, Y, Jackson, JS, and Anderson, NB. Racial differences in physical and mental health. J Health Psychol (1997). 2:335–351. doi:10.1177/135910539700200305
28. Taylor, TR, Kamarck, TW, and Shiffman, S. Validation of the detroit area study discrimination scale in a community sample of older African American adults: the Pittsburgh healthy heart project. Int J Behav Med (2004). 11:88–94. doi:10.1207/s15327558ijbm1102_4
29. Krieger, N, Smith, K, Naishadham, D, Hartman, C, and Barbeau, EM. Experiences of discrimination: validity and reliability of a self-report measure for population health research on racism and health. Soc Sci Med (2005). 61:1576–1596. doi:10.1016/j.socscimed.2005.03.006
30. Parloff, MB, Kelman, HC, and Frank, JD. Comfort, effectiveness, and self-awareness as criteria of improvement in psychotherapy. Am J Psychiatry (1954). 111:343–352. doi:10.1176/ajp.111.5.343
31. Mollica, R, Cardozo, BL, Osofsky, H, Raphael, B, Ager, A, and Salama, P. Mental health in complex emergencies. Lancet (2004). 364:2058–2067. doi:10.1016/s0140-6736(04)17519-3
32. Zimet, GD, Dahlem, NW, Zimet, SG, and Farley, GK. The multidimensional scale of perceived social support. J Personal Assess (1988). 52:30–41. doi:10.1207/s15327752jpa5201_2
34.Institut de la statistique Québec. Enquete québécoise sur la santé des jeunes du secondaire 2016-2017 [Québec survey on youths’ health in secondary schools in 2016-2017]. Québec City, Canada: Institut de la statistique Québec (2018).
35. Miconi, D, Oulhote, Y, Hassan, G, and Rousseau, C. Sympathy for violent radicalization among college students in Quebec (Canada): the protective role of a positive future orientation. Psychol Violence (2020b). 10:344–354. doi:10.1037/vio0000278
36. Steggals, P, Graham, R, and Lawler, S. Self-injury in social context: an emerging sociology. Soc Theor Health (2020). 18:201–210. doi:10.1057/s41285-020-00149-7
37. Azeredo, CM, Rinaldi, AEM, de Moraes, CL, Levy, RB, and Menezes, PR. School bullying: a systematic review of contextual-level risk factors in observational studies. Aggression Violent Behav (2015). 22:65–76. doi:10.1016/j.avb.2015.04.006
38. Brouillette-Alarie, S, Hassan, G, and Ousman, S. The prevention of violent radicalization: evidence-based guidelines to promote efficient interventions conference report copyright notice A conference report produced by the Canadian practitioners network for the prevention of radicalization and extremist violence (CPN-prev). Montreal, Canada: CPN-PREV Systematic Reviews (2019).
Keywords: violent radicalization, discrimination, mental health, North America, Somali
Citation: Ellis BH, Miller AB, Sideridis G, Frounfelker R, Miconi D, Abdi S, Aw-Osman F and Rousseau C (2021) Risk and Protective Factors Associated With Support of Violent Radicalization: Variations by Geographic Location. Int J Public Health 66:617053. doi: 10.3389/ijph.2021.617053
Received: 13 October 2020; Accepted: 11 February 2021;
Published: 29 March 2021.
Edited by:
Robert Wellman, University of Massachusetts Medical School, United StatesCopyright © 2021 Ellis, Miller, Sideridis, Frounfelker, Miconi, Abdi, Aw-Osman and Rousseau. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: B. Heidi Ellis, aGVpZGkuZWxsaXNAY2hpbGRyZW5zLmhhcnZhcmQuZWR1