 Perla Boutros1
Perla Boutros1 Nour Kassem1Valentin Boudo1,2Ali Sié1,2Stephen Munga1,3Martina A. Maggioni4,5,6Marcin Golec1Robin Simion1Till Bärnighausen1,7,8Volker Winkler1Sandra Barteit1*
Nour Kassem1Valentin Boudo1,2Ali Sié1,2Stephen Munga1,3Martina A. Maggioni4,5,6Marcin Golec1Robin Simion1Till Bärnighausen1,7,8Volker Winkler1Sandra Barteit1*- 1Heidelberg Institute of Global Health, Heidelberg University Hospital, Heidelberg, Germany
- 2Centre de Recherche en Santé de Nouna, Nouna, Burkina Faso
- 3Kenya Medical Research Institute (KEMRI), Nairobi, Kenya
- 4Institute of Physiology, Center for Space Medicine and Extreme Environment, Charité Universitätsmedizin Berlin, Berlin, Germany
- 5Department of Biomedical Sciences for Health, Faculty of Medicine and Surgery, University of Milan, Milan, Italy
- 6Charité Center for Global Health, Charité Universitätsmedizin Berlin, Berlin, Germany
- 7Africa Health Research Institute (AHRI), Durban, South Africa
- 8Department of Global Health and Population, School of Public Health, Harvard University, Boston, MA, United States
Objective: This scoping review aims to identify risk factors for COPD and asthma, examine the burden and intervention measures, and clarify the findings in the context of climate change, with a particular focus on LMICs.
Methods: Following the PRISMA-ScR guidelines, we conducted a scoping review using PubMed, Embase, and Scopus, focusing on studies published from 2011 to 2024.
Results: Our review included 52 studies that encompassed 244,004 participants. Predominantly conducted in SSA (n = 43, 83%) and Asia (n = 16, 31%), they address indoor and ambient air pollution, occupational hazards, and environmental conditions. Climate change exacerbates risks, varying regionally. SSA faces severe household and occupational exposures, while other LMICs deal with industrial and urban pollution. Stigma, social exclusion and economic burden underscore the necessity for intervention strategies (e.g., educational programs, pulmonary rehabilitation, low-emission cookstoves).
Conclusion: Our research shows a strong link between air pollution, occupational and environmental exposures, and the prevalence of COPD and asthma in LMICs. It suggests that targeted interventions are effective ways to mitigate these diseases and also highlights the significant impact of climate change on respiratory health.
Introduction
Chronic respiratory diseases like chronic obstructive pulmonary disease (COPD) and asthma have a significant impact on low- and middle-income countries (LMICs) due to environmental and socio-economic factors. Globally, COPD affects 4.1% of the population, while asthma affects 3.7% [1]. Asthma is characterized by chronic lower respiratory inflammation triggered by various factors like smoke, pollutants, and allergens [2], while COPD involves irreversible airway obstruction from chronic inflammation [3]. In 2019, out of the 391.9 million individuals aged 30–79 years affected by COPD worldwide, 315.5 million resided in LMICs [4]. Furthermore, LMICs account for over 80% of asthma-related deaths [3] and 90% of COPD-related deaths [5].
In LMICs, COPD accounts for approximately 1,000 disability-adjusted life years (DALYs) per 100,000 individuals [6]. In Sub-Saharan Africa (SSA), the rate is slightly lower at 715 DALYs per 100,000 individuals [7]. Furthermore, both COPD and asthma are often underserved diseases, exacerbated by the limited availability and cost-effectiveness of asthma medications and diagnostic procedures [3]. Limited access to healthcare, exposure to pollutants, and inadequate public health policies exacerbate these conditions in LMICs [3]. Asthma medications like long-acting muscarinic antagonists (LAMAs) are often scarce and costly in LMICs, impacting treatment availability [8–10]. Prioritizing preventive interventions, early diagnosis, and improving access to essential medications is crucial in reducing the burden of these diseases in LMICs [11].
In addition to the high prevalence, climate change, characterized by rising temperatures, increased heat exposure, and varying humidity levels, is emerging as a potentially under-explored risk factor that exacerbates respiratory diseases [12]. Elevated temperatures and weather variability, linked to climate change, may increase the frequency and concentration of airborne pollutants, allergens, and ozone, potentially worsening respiratory conditions [13]. Additionally, climate change-induced weather extremes may increase dust exposure [14], whereby inhaling dust particles may cause or worsen inflammation and irritation in the airways, leading to acute respiratory reactions such as bronchoconstriction, excess mucus production, and increased inflammation. Dust often contains allergens and microbes, introducing further respiratory irritants [15]. High humidity can increase airway resistance because of its high water content and raise the physiological demand for oxygen, resulting in heightened breathlessness [16]. Additionally, high humidity may promote mold growth, posing an additional risk to both healthy individuals and those with asthma and COPD who already have sensitive airways [17]. The World Meteorological Organization (WMO) predicts a 66% chance of global temperatures rising by at least 1.5° above pre-industrial levels between 2023 and 2027, potentially leading to a significant increase in the exacerbation of respiratory diseases [18]. SSA is already established as a highly vulnerable region to the impacts of climate change and extreme weather events [19, 20], experiencing the sharpest increases in temperature and changes in rainfall patterns [21].
However, research on obstructive lung diseases, notably COPD and asthma, is both limited and unevenly distributed worldwide [22]. In the literature, we identified five systematic reviews focusing on COPD in SSA [23–27], primarily examining the prevalence of the disease [23, 25–27], inadequate supply and quality of spirometry tests and equipment [23, 24, 27], risk factors [26], and the lack of non-communicable disease (NCD) healthcare plans [23, 24]. These studies primarily focused on countries such as South Africa, Nigeria, Tanzania, Malawi, Uganda, and Ethiopia, leaving many other low- and middle-income countries (LMICs) unexplored. Asthma research in SSA is scant and primarily centered on South Africa, while studies from high-income countries often lack relevance for SSA and other LMICs due to distinct population and environmental factors [26, 28, 29]. Key knowledge gaps regarding the impact of various risk factors and climate change on the health of individuals with COPD and asthma, as well as the evaluation of the effectiveness of current interventions, remain unexplored in LMICs.
To address these knowledge gaps, we conducted a scoping review and interpreted the findings in the context of climate change. This review was guided by the following research objectives:
1. To identify major risk factors of obstructive lung diseases, specifically COPD and asthma,
2. To elucidate the burden of disease of living with COPD and asthma and,
3. To determine intervention approaches and their effectiveness in managing and preventing COPD and asthma
Methods
The scoping review adhered to the methodological framework by Arksey and O’Malley [30], refined by Levac et al. [31], following defined steps like defining research questions, selecting studies, charting data, and reporting findings in line with Preferred Reporting Items for Systematic Reviews and Meta Analyses for Scoping Reviews (PRISMA-ScR) guidelines [32].
Inclusion and Exclusion Criteria
The study employed the Population-Exposure-Outcome (PEO) framework (see Supplementary Table S1), refining screening criteria and focusing on English primary research articles post-1st January 2011. This aligns with van Gemert et al.’s seminal work in 2011, evaluating asthma and COPD risk factors, impacts in SSA, and suggesting intervention strategies [26].
Our review encompassed studies from LMICs [33] exploring COPD and asthma as exposures, assessing risk factors, interventions for prevention and management, and challenges faced by affected individuals. Excluded were studies solely focusing on disease prevalence.
Search Strategy
We searched electronic databases, including PubMed, Embase, and Scopus. Additionally, we examined grey literature via Google Scholar, focusing on the first 200 search results. Reference lists of relevant articles were hand-searched to manually identify and include relevant studies. Our search strategy incorporated index terms (e.g., MeSH, Emtree) and relevant keywords specific to the topic and context (see Supplementary Table S2).
Study Selection
Articles identified from the databases were imported into Rayyan software [34], which removed duplicates. Two independent reviewers (PB, NK) evaluated the studies in a two-step process, using the predefined inclusion and exclusion criteria. Initially, titles and abstracts were screened. If either reviewer deemed a study potentially relevant, a full-text review was undertaken. A study was excluded only if both reviewers agreed on its irrelevance.
Data Charting
Relevant data were extracted and organized in a Microsoft Excel spreadsheet. The charting process included parameters of title, author, publication year, country of origin, study objectives, target population, sample size (if provided), research design, analytical methods, gender distribution, age range, and primary findings.
Reporting the Results
A narrative synthesis was conducted to provide an overview of the primary emerging themes from the included studies.
Results
Overview
The initial database search was conducted on August 9th, 2022, and updated on 4th January 2024. The results of the latter search are presented in the PRISMA-ScR flowchart (refer to Figure 1). After deduplication and incorporating 13 manually searched references from relevant studies, a total of 2,103 studies were considered. After screening titles, abstracts and full texts, n = 130 full-text articles were reviewed, of which n = 52 studies met the inclusion criteria and were subsequently included into the scoping review.
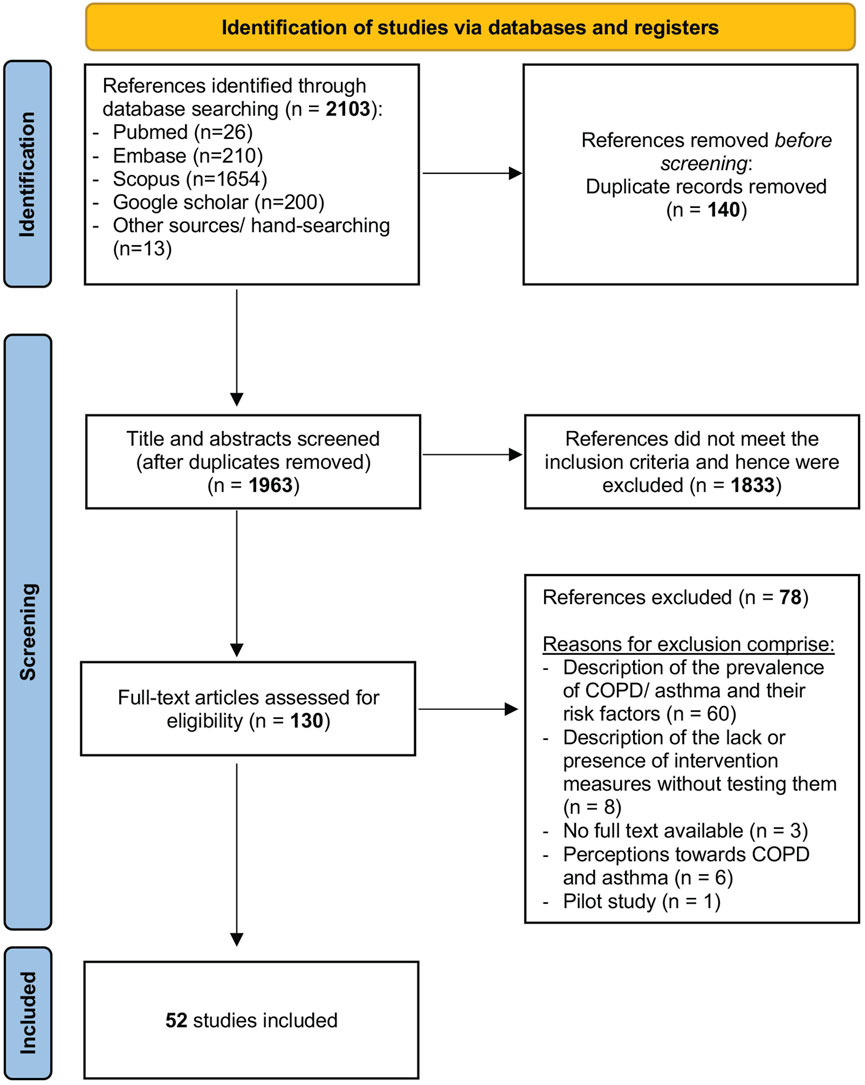
Figure 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews flowchart (scoping review, low- and middle-income countries, 2022–2024).
Study Characteristics
In this review, we analyzed data from a total study population of n = 244,004 participants covered in n = 52 studies (see Supplementary Table S3). The largest study, conducted in India in 2012, included n = 156,316 (64%) participants. From 2011 to 2022, publications on interventions for obstructive lung diseases in LMICs (see Figure 2) increased. Six studies (12%) were multinational in scope [35–40]. Specifically, n = 43 studies (83%) were conducted in SSA, representing n = 76,481 participants (31%), with Nigeria and Uganda contributing twelve (23%) and ten (19%) studies, respectively. The distribution of studies per country is depicted in Figure 3. The methodologies varied, with n = 38 (73%) being cross-sectional, n = 7 (13%) experimental longitudinal, n = 4 (8%) observational longitudinal, n = 2 (4%) randomized controlled trials, and n = 1 (2%) non-randomized controlled trials. Of the 52 studies, n = 7 (13%) exclusively involved women, n = 9 (17%) focused on children, n = 1 (2%) included both women and children, and n = 2 (4%) was focusing on men. Fourteen studies (27%) included participants diagnosed with asthma or COPD, whereas n = 38 studies (73%) focused on participants exposed to risk factors for obstructive lung diseases (Table 1).
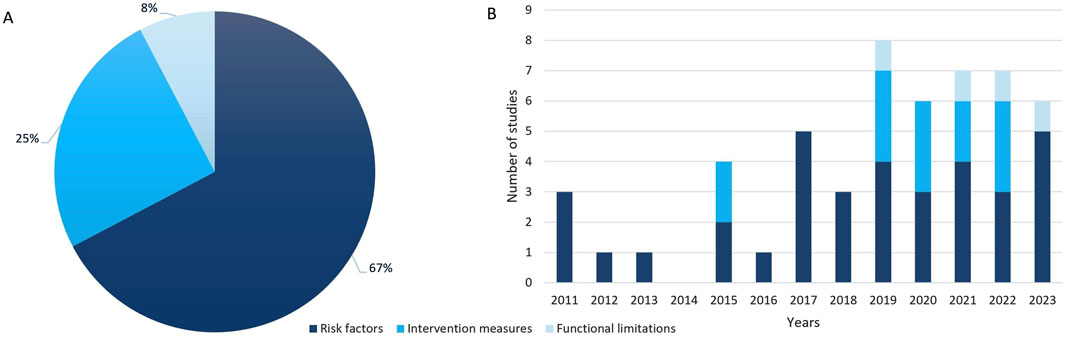
Figure 2. Distribution (A) and trend (B) of publications in low- and middle-income countries from 2011 to 2023 highlighting key areas: risk factors, intervention measures and functional limitations (scoping review, low- and middle-income countries, 2022–2024).
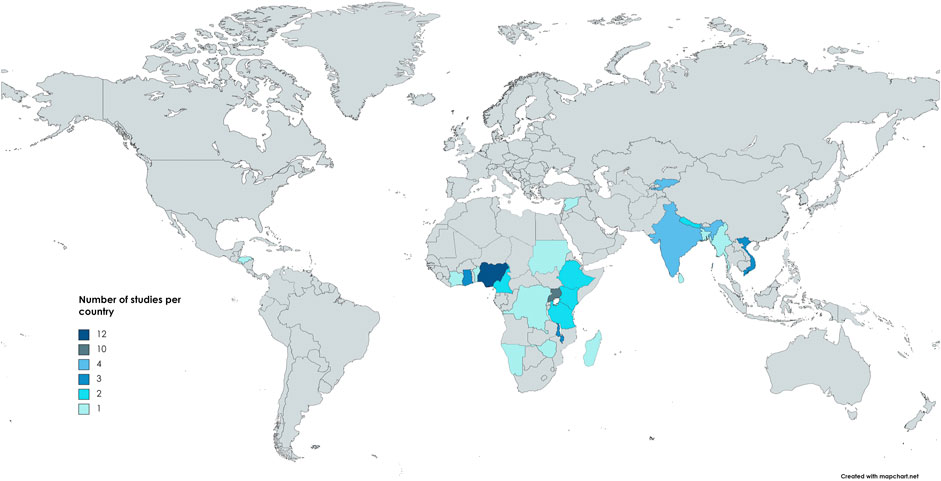
Figure 3. Distribution of included studies per country (scoping review, low- and middle-income countries, 2022–2024).
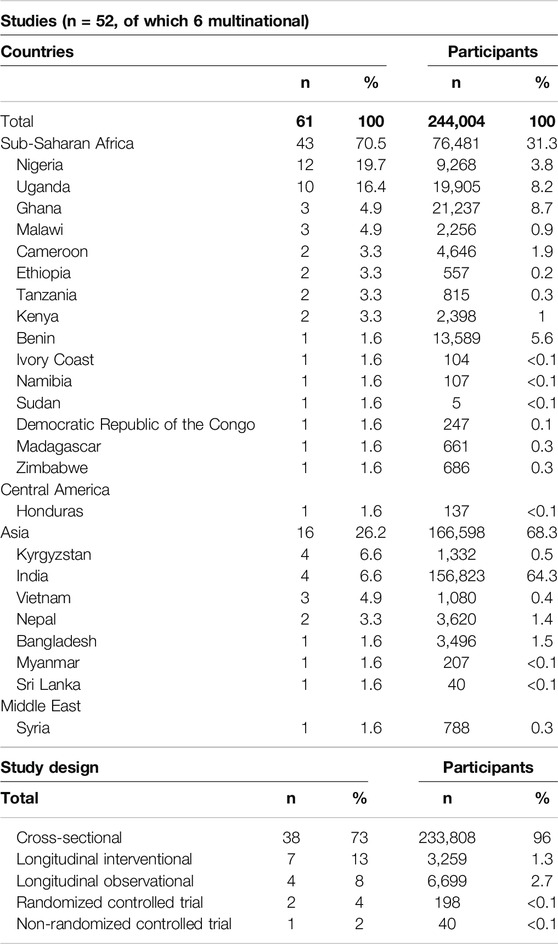
Table 1. Overview of study characteristics of included studies (scoping review, low- and middle-income countries, 2022–2024).
Risk Factors for COPD and Asthma
Thirty-five studies (67%) [39, 41–74] reviewed the association between various risk factors and the incidence or severity of obstructive lung diseases, respiratory symptoms, and spirometry outcomes (see Figure 4). Disease status was determined using self-reports, hospital records, or spirometry results. Questionnaires were utilized to collect data on respiratory symptoms, and spirometry tests (see Supplementary Table S4) were used to measure lung function.
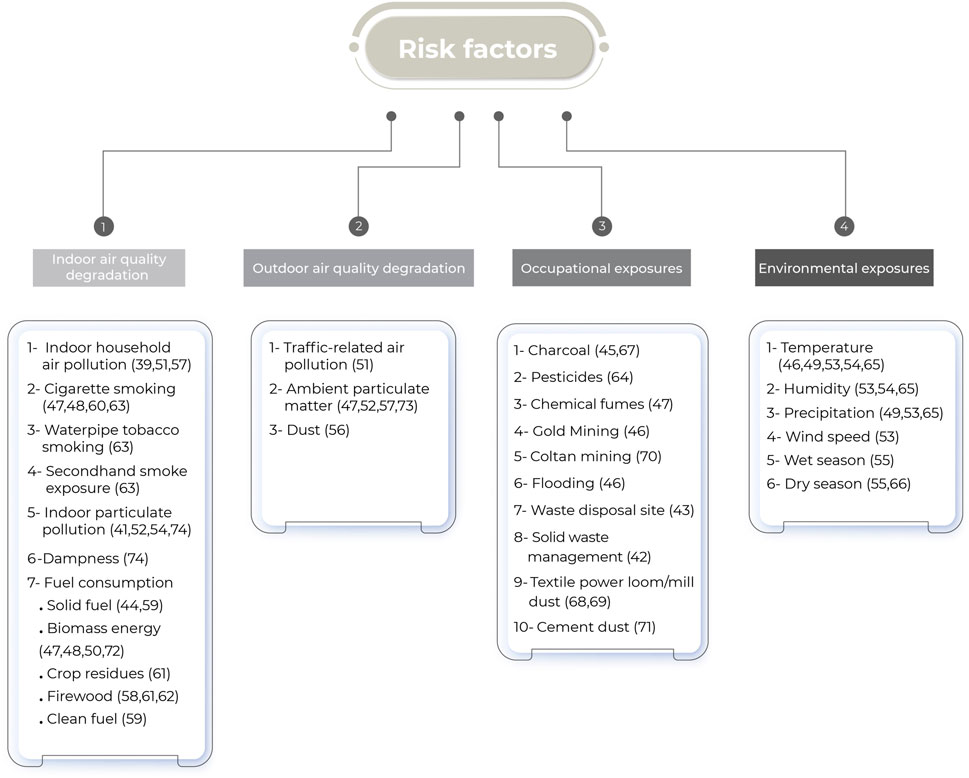
Figure 4. Categorization of risk factors identified in reviewed studies, grouped into four main domains: indoor air quality degradation, outdoor air quality degradation, occupational exposures, and environmental exposures (scoping review, low- and middle-income countries, 2022–2024).
The questionnaires, designed to capture respiratory symptoms such as cough, sputum production, wheezing, and shortness of breath, were either developed by the researchers or adapted from established, validated instruments. These instruments include The Bold Core questionnaire, the Medical Research Council (MRC) questionnaire on respiratory symptoms, the Global Alliance Against Chronic Respiratory Diseases (GARD) World Health Organization (WHO) survey, the International Study of Asthma and Allergies in Childhood (ISAAC) questionnaire, and the European Community Respiratory Health Survey (ECRHS) questionnaire.
Indoor Air Quality Degradation
Eighteen (35%) studies [39, 41, 44, 47, 48, 50, 51, 52, 54, 57, 58, 59, 60, 61, 62, 63, 72, 74] explored the link between Indoor Air Quality degradation and lung diseases, respiratory symptoms, lung function tests, and disease severity (see Supplementary Table S5).
Outdoor Air Quality Degradation
Six (12%) studies [47, 51, 52, 56, 57, 73] assessed the relationship between outdoor air quality degradation and respiratory symptoms, as well as lung function outcomes (see Supplementary Table S6).
Occupational Exposures
Eleven (21%) studies [42, 43, 45, 46, 47, 64, 67, 68, 69, 70, 71] investigated the connection between occupational exposure and respiratory health outcomes (see Supplementary Table S7).
Environmental Exposures
Weather data was obtained through direct measurement, sourced from meteorological agencies, or inferred based on seasonal patterns (see Supplementary Table S8). Seven (13%) studies [46, 49, 53–55, 65, 66] investigated the relationship between environmental exposures and respiratory diseases (see Supplementary Table S9).
Burden of Living With an Obstructive Lung Disease in Low-Resource Countries
Four (8%) studies [35, 40, 75, 76] estimated the personal and socioeconomic burden of living with an obstructive lung disease in low-resource settings. In a cross-sectional study conducted by Zoller et al. in Tanzania from 2015 to 2016, it was found that non-smokers refrained from taking a job due to shortness of breath. This condition was linked to high carboxyhemoglobin (SpCO) levels, living in rural areas, and the use of wood for cooking on open fires [75]. Brakema et al. found that asthma and COPD patients across Uganda, Vietnam, and Kyrgyzstan experienced low work absenteeism but significant activity impairment at work due to breathlessness, smoking, and solid fuel use [35]. In a qualitative study conducted by Tamire et al. in Addis Ababa, Ethiopia, it was found that COPD patients suffered from work impairment, decreased productivity, and limitations in physical activities due to their respiratory symptoms [35, 76]. These symptoms extended to financial, psychological, and social challenges, such as medication affordability issues, stress, helplessness, and reduced participation in social and religious events [76]. Similarly, Egere et al. explored challenges faced by chronic respiratory disease (CRD) patients - including asthma, COPD, occupational lung diseases, pulmonary hypertension, and cystic fibrosis - in Sudan and Tanzania. CRD resulted in reduced work capacity, economic hardship, and additional social and psychological burdens, including challenges in education expenses and caregiving for older relatives [40]. Healthcare-related costs, such as diagnostic tests and transportation, further burdened participants. Routine personal and community activities were severely impacted, leading to feelings of exclusion. Additionally, CRD patients faced stigmatization, often being wrongly associated with human immunodeficiency virus (HIV) or tuberculosis due to chronic cough, resulting in community isolation, limitations in sexual activities, and challenges in marital pursuits [40].
Intervention Measures
Thirteen (25%) studies [36–38, 77–86] assessed various COPD and asthma intervention measures in low-resource settings, focusing on knowledge of the diseases and their risk factors, disease screening and control, treatment adherence, behavioral changes, and the use of improved indoor cookstoves (see Table 2).
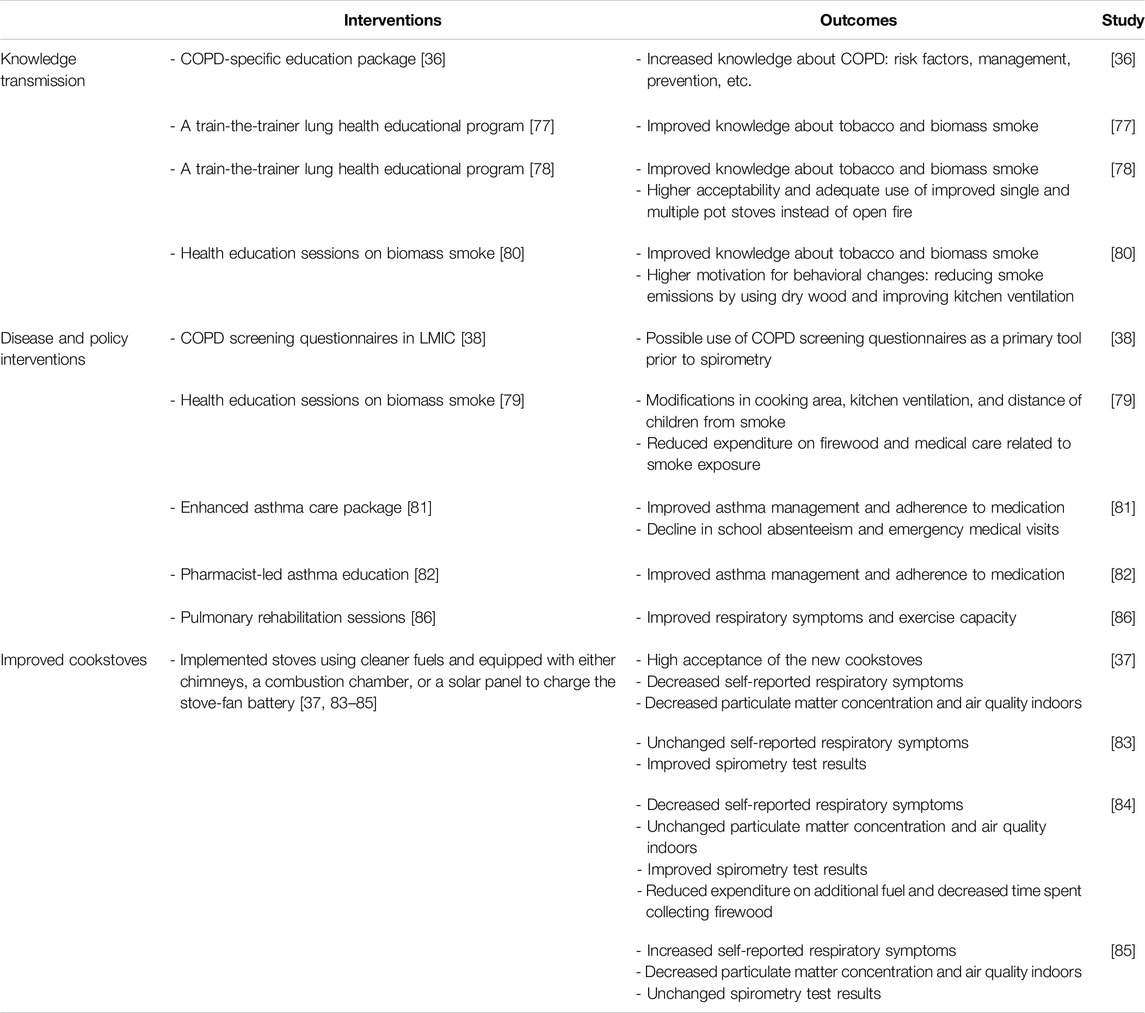
Table 2. Intervention measures for chronic obstructive pulmonary disease and asthma in low-resource contexts based on included studies (scoping review, low- and middle-income countries, 2022–2024).
Knowledge Transmission
Four (8%) studies [36, 77, 78, 80] investigated educational interventions to enhance awareness of obstructive lung diseases and risk factors using tools like posters, flip charts, brochures, and local radio broadcasts (see Supplementary Table S10). In Uganda, a successful train-the-trainer program improved healthcare and community health workers’ understanding of tobacco and biomass smoke’s impact on lung health, resulting in increased questionnaire scores. This knowledge was effectively communicated to villagers, particularly regarding the dangers of tobacco smoke [77]. The program, adapted for Kyrgyzstan and Vietnam, led to a significant increase in correct responses on knowledge questionnaires, indicating sustained behavioral changes such as greater acceptance and proper use of lower-emission cookstoves [78]. Robertson et al. observed improved COPD knowledge in Nepal, Peru, and Uganda after distributing a COPD-specific educational package by community health workers [36]. Furthermore, educational sessions conducted by midwives in Uganda not only increased pregnant women’s knowledge about biomass smoke as an asthma risk factor by 45% but also motivated them to switch to safer fuel types and enhance kitchen ventilation [80].
Approaches to disease Management and Policy Interventions
Five (10%) studies [38, 79, 81, 82, 86] focused on interventions that improved COPD screening, asthma management, new respiratory health policy implementation and, rehabilitation and treatment of COPD in LMICs (see Supplementary Table S11).
COPD Screening
In these settings, three screening questionnaires - the COPD Assessment in Primary Care to Identify Undiagnosed Respiratory Disease and Exacerbation Risk (CAPTURE), the Lung Function Questionnaire (LFQ), and the COPD in LMICs Assessment (COLA-6) - were evaluated for their efficacy in identifying individuals diagnosed with COPD who would benefit from further spirometry testing [38]. The study found that participants diagnosed with COPD often had severe obstruction and were mostly unaware of their condition, despite experiencing a low quality of life. Those with false-positive results typically had a history of asthma or chronic bronchitis and were currently exposed to biomass smoke [38].
Asthma Management
In a randomized control trial (RCT), non-physicians delivered an enhanced asthma care package, including clinical assessment, optimized inhaled treatments, and customized asthma education, while the control group received standard physician care [81]. The intervention group showed fewer school absences, reduced emergency visits, and improved asthma control and medication adherence [81]. Another RCT assessed a pharmacist-led asthma education intervention [82], delivering information on triggers, control methods, and inhalers through clinic visits, mobile phone calls, and texts, compared to standard hospital care for the control group. The intervention resulted in improved asthma control and medication adherence [82].
Educational and Policy Interventions on Respiratory Health
Cartwright et al. evaluated the long-term effects of educational sessions on biomass smoke, initially investigated by Nantanda et al. [80], which were conducted by midwives for pregnant women and mothers [79]. The study observed that participants made modifications in their cooking areas, enhanced kitchen ventilation, and reduced children’s proximity to smoke while cooking [79]. Furthermore, a reduction in expenses for wood and medical care associated with smoke exposure was also noted [79].
Rehabilitation and Treatments in Low-Resource Settings
In Sri Lanka, a non-randomized controlled trial adapted the University Hospital of Leicester’s pulmonary rehabilitation protocol for COPD individuals in low-resource settings. The 6-week program included supervised and home-based exercises such as walking, stretching and strength training using simple equipment like water-filled bottles. Significant improvements were noted in respiratory symptoms, dyspnea, and exercise performance, with the intervention group surpassing the Minimum Clinically Important Difference (MCID) [86].
Low Emission Cookstoves
Four (8%) studies [37, 83–85] investigated the impact of introducing low-emission cookstoves indoors (see Supplementary Table S12). These stoves, utilizing cleaner fuels or enhancements like chimneys, combustion chambers and solar-powered stove-fan batteries led to reduced indoor particulate matter (PM2.5) [37, 85] and decreased self-reported respiratory symptoms [37, 84]. However, one study observed no change in cough or clinic visits after adoption [83]. Another study reported an increase in respiratory symptoms, attributed to altered reporting methods rather than a true increase [85]. Spirometry tests demonstrated improved lung function in Honduras and Kenya [83, 84], but no significant changes were noted in Malawi [85]. Improved cookstoves were well-received in rural communities across Uganda, Vietnam, and Kyrgyzstan [37], providing additional benefits such as reduced fuel costs and less time spent gathering firewood [84].
Discussion
This review examines COPD and asthma in SSA and other LMICs, with a particular focus on the impact of climate change. It highlights key risk factors such as indoor and ambient air pollution, occupational hazards, and environmental allergens, impacting disease severity and exacerbations. Individuals with these conditions face multifaceted challenges including reduced work capacity, limited access to healthcare, social stigma, financial strain and psychological stress [87, 88]. Biomass fuel use for cooking exacerbates COPD in LMICs [87], particularly affecting women and children in rural areas [89]. Additionally, cultural practices such as burning incense, using kerosene lamps, and lighting mosquito coils contribute to higher levels of indoor pollution [89]. Interventions such as educational programs, non-physician-led treatments, and improved cookstove initiatives aim to mitigate indoor air pollution and improve respiratory outcomes. Aging also appears to significantly contribute to the prevalence of COPD in SSA. Between 1990 and 2019, the overall prevalence of COPD cases in SSA increased by 117%. However, during the same period, the age-standardized COPD prevalence rate declined by 3.3% [7]. The decline in the age-standardized COPD prevalence rate in SSA, amidst an overall case increase, might result from improved healthcare, public health policies, and a younger population.
Greenhouse gas concentrations have increased rapidly since 1850, in parallel with a 1.1°C increase in global surface temperature by 2011–2020 compared to 1850–1900 [90]. The regions that have generally contributed the least to CO2 emissions and climate change are considered to be the most vulnerable [91] and are mainly located in East, Central and West Africa, with some other regions in South Asia and Central and South America [90]. Climate change can have direct and indirect effects on health; for example, exposure to extreme heat can have indirect effects through increased transmission of food- and waterborne diseases, and direct effects through dehydration, heat stroke, and increased hospitalization and mortality from respiratory and cardiovascular diseases [92].
Although no study in the literature has explicitly examined the relationship between climate change and chronic respiratory diseases in SSA and other LMICs, it can be argued that some of the risk factors exacerbating COPD and asthma developed in this review may serve as mediators between climate change and chronic respiratory diseases. Thus, a hypothesized link between both entities in SSA and other LMICs can be deduced.
Weather variables like temperature, humidity, and precipitation play a significant role in obstructive lung diseases. Studies exhibit inconsistent outcomes, potentially attributable to climate variations or differing methodologies and settings; for example, a study conducted in Sudan’s dry Savanna region revealed an inverse correlation between temperature and asthma severity [53]. This contrasts with the common understanding that high temperatures worsen respiratory conditions [93]. The wet season with low temperatures and high humidity has been associated with increased asthma cases owing to a greater prevalence of viral infections and indoor triggers [54], which is consistent with previous research, highlighting the role of humidity and the presence of allergens and pollutants in indoor environments [94]. The combination of low temperature and humidity can cause bronchoconstriction, underscoring the importance of maintaining suitable indoor climates [95]. High humidity can exacerbate asthma by releasing allergens, highlighting the importance of indoor air quality management [95]. Although wind can increase long-range transport of pollen and pollutants [96], increased outdoor wind speed can help disperse pollutants, potentially providing protective benefits that require further investigation [95]. Human-induced climate change associated with increased greenhouse gas emissions affects weather variables, leading to heat waves, heavy precipitation and droughts in some regions [90]. Climate change may therefore have direct and indirect effects on respiratory health [97]. The included studies in this review however focused on variations of climate factors rather than extreme weather events caused by climate change. Further investigation should therefore be implemented, particularly in highly affected areas such as SSA, to study the complex relationship between climate change and chronic respiratory diseases.
In this review, other risk factors listed in Figure 4 have been shown to be associated with reduced lung function.
Ambient air pollution, divided into gaseous and particulate matter (PM) pollutants, affects both indoor and outdoor air quality. Gaseous pollutants include nitrogen dioxide (NO2), sulfur dioxide (SO2), ozone (O3), carbon monoxide (CO), carbon dioxide (CO2), and volatile organic compounds (VOCs). PM pollutants, on the other hand, are classified by size and are formed from gases such as nitrogen oxides, ammonia, SO2, and VOCs [97]. In this review, studies have shown that indoor biomass and coal burning for cooking and heating in SSA and other LMICs has led to an increase in indoor gaseous and PM pollutants, and therefore to a degradation of indoor air quality. Exposure to dust and traffic-related air pollution has led to an increase in outdoor PM pollutants, resulting in poor outdoor air quality. PM pollutants have been shown to vary seasonally, with higher levels in winter due to increased dust particles and biomass burning [97]. Specifically, in SSA, excessive heat and heavy rainfall during the rainy season make outdoor cooking impractical, leading people to burn biomass indoors more frequently, resulting in poorer indoor air quality. In addition, future intense heat waves caused by climate change will lead to more wildfires, which will increase particulate matter and harmful greenhouse gases and lead to deterioration of outdoor air quality [98]. Dry and hot conditions and reduced precipitation can also lead to increased air pollution, especially ozone [97, 98], due to increased photochemical production [98]. Climate change and air pollution have also been shown to be interrelated, as PM pollutants and greenhouse gases are often co-emitted [99]; burning fossil fuels not only increases air pollution but also produces greenhouse gases, which in turn lead to extreme weather events such as droughts, heat waves and floods, which can further affect respiratory health [97]. Charcoal production and climate change are also linked through a feedback loop rather than a direct cause and effect relationship. The process of charcoal production involves deforestation and the release of greenhouse gases such as CO2 and methane, which in turn contribute to global warming [100]. In some regions affected by climate change, particularly drought, farmers may be more likely to engage in charcoal production during the dry season. In Tanzania, farmers rely on charcoal production as an alternative source of income after crop failure during the dry season [101]. This cyclical relationship will lead to poorer respiratory health. Pesticide use and climate change have also been shown to be interconnected. Rising temperatures allow for severe pest outbreaks because such conditions allow pests to survive in regions where they were previously unable to thrive [102]. In addition, the lengthening of the growing season due to higher temperatures exposes plants to pests for longer periods of time [103]. This leads to increased use of pesticides to control pest infestations. Pesticides, in turn, contribute to CO2 emissions and can disrupt soil health by killing microorganisms that play a beneficial role in carbon sequestration [104], resulting in the release of more CO2 into the atmosphere and exacerbating climate change.
Implementing cookstoves that use cleaner fuels and are equipped with a solar panel to charge the stove-fan battery [85] is an effective way that allows individuals to cook indoors during extreme heat and heavy rainfall while maintaining a good indoor air quality and generating less CO2 emissions. On the other hand, cookstoves with chimneys or a combustion chamber may reduce indoor air pollution but will still contribute to greenhouse gas emissions [83, 84]. In addition, the introduction of educational programs to increase knowledge about biomass smoke [77, 78, 80] can play a key role in reducing the burning of indoor biomass fuel but does not offer an established long-term alternative that can be afforded by the general population. These solutions can then be considered as important intermediate steps in LMICs, where resources are scarce and the use of clean energy and electric stoves is not always feasible.
Sustainable agricultural practices and predominantly plant-based diets decrease emission of greenhouse gases [98]. Adopting diets rich in antioxidants and vitamins, characteristic of Mediterranean or “prudent” diets, can significantly improve pulmonary function and reduce asthma and COPD risks [105–108]. However, over two million people suffer micronutrient deficiencies [109], especially in SSA [110]. Educational initiatives in LMICs promoting healthy diets typically utilize printed and digital materials, often based on behavior change models, and aim to engage both women and men, reflecting their distinct roles in food preparation and decision-making [111–113]. Climate change is likely to exacerbate nutrient deficiency in LMICs by affecting food security, namely accessibility, availability and food stability [114, 115]. However, other key factors contribute to food insecurity in LMICs, including limited access to modern agricultural technologies, reliance on subsistence farming, and political and economic instability in conflict zones, which disrupt agricultural production and reduce access to food [116].
It is evident that climate change plays a pivotal role in the prevalence of chronic respiratory diseases in SSA and other LMICs. This impact can be achieved directly or indirectly through various mediators, including indoor and outdoor air pollution, charcoal production, pesticide use, and nutrient deficiency. However, additional factors unique to SSA contribute to the heightened burden of chronic respiratory diseases and impede their prevention.
In certain regions in SSA where targeted asthma management protocols are lacking, managing risk factors and promoting lifestyle changes are prioritized [117]. The shortage of trained medical professionals, particularly in remote areas, poses a challenge for diagnosing and managing obstructive lung diseases. Community-based screening, technology utilization, and awareness initiatives are crucial for enhancing primary healthcare [89]. Spirometry plays a vital role in diagnosing obstructive lung diseases, but inconsistencies in diagnosis can arise from varying cutoff measures [7]. In countries like South Africa and Nigeria, spirometry use is largely confined to specialized hospitals and research settings, despite being recommended for asthma diagnosis. In Tanzania, asthma diagnosis relies mainly on clinical history and findings, while Zimbabwe lacks specific asthma diagnostic guidelines [117]. Challenges in asthma diagnosis encompass not only spirometry availability and clinician training but also equipment maintenance, electricity access, technical support, and the use of outdated equipment, necessitating comprehensive training and guidelines for healthcare workers [89, 118]. Implementing tailored pulmonary rehabilitation programs and national strategies can alleviate the burden of lung diseases in low-resource settings [89, 118, 119], although challenges like infrastructure limitations, budget constraints, political instability and healthcare workforce shortages persist in implementing WHO’s NCD management framework [11, 120].
Enhanced research, screening, and interventions are crucial for obstructive respiratory diseases in LMICs, especially in SSA, where the need is intensified by the disproportionate impact of climate change-induced global warming [119].
Limitations
In our review, we focused exclusively on studies from LMIC contexts, a deliberate choice that, while limiting comparative insights from high-resource settings, was aimed at a specific analysis. The included studies varied in their definitions of certain risk factors and were influenced by multiple confounders, necessitating cautious interpretation of direct comparisons. Additionally, we omitted studies that described but did not empirically test intervention measures, which could have offered a wider view on potential intervention strategies despite their lack of practical outcome data.
Conclusion
This review examines the impact of different risk factors on the health of individuals with COPD and asthma in LMICs. Climate change plays an indirect but pivotal role in the exacerbation of the burden of chronic respiratory diseases by impacting some risk factors specific to SSA and other LMICs.
This research highlights the need for comprehensive strategies that encompass educational programs, low-emission cookstoves and the implementation of targeted healthcare policy to mitigate the effects of climate change on respiratory health. Furthermore, it emphasizes the urgent necessity for further interventions that are tailored to the specific environmental and socio-economic context. In order to address these challenges, it is essential that there is urgent global collaboration and investment in research and infrastructure with the aim of improving public health resilience against climate-related exacerbations of respiratory conditions in LMICs.
Author Contributions
The research question was formulated by PB and SB; title, abstract, full-text screening, and data extraction were performed by PB and NK; PB wrote the manuscript draft with significant contributions from all authors in editing and revisions. All authors contributed to the article and approved the submitted version.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. The authors express their gratitude to the German Research Foundation (Deutsche Forschungsgemeinschaft) for the support provided in the context of a research unit funded by the Deutsche Forschungsgemeinschaft (project number: 409670289).
Conflict of Interest
The authors declare that they do not have any conflicts of interest.
Acknowledgments
We are grateful to all authors for their collaboration and input throughout the review process. We acknowledge the assistance of ChatGPT version 3.5, an AI language model developed by OpenAI, for providing help with sentence structure and grammar.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.ssph-journal.org/articles/10.3389/phrs.2024.1607339/full#supplementary-material
Abbreviations
CAPTURE, COPD Assessment in Primary Care to Identify Undiagnosed Respiratory Disease and Exacerbation Risk; COLA-6, COPD in LMICs Assessment; COPD, Chronic obstructive pulmonary disease; CRD, Chronic Respiratory Disease; ECRHS, European Community Respiratory Health Survey; FEV1, Forced Expiratory Volume in 1 s; FVC, Forced Vital Capacity; GARD, Global Alliance Against Chronic Respiratory Diseases; HIV, Human Immunodeficiency Virus; ISAAC, International Study of Asthma and Allergies in Childhood; LAMAs, Long-acting muscarinic antagonists; LFQ, Lung Function Questionnaire; LMICs, Low-and middle-income countries; MCID, Minimum Clinically Important Difference; MRC, Medical Research Council; NCD, Non-communicable disease; PEFR, Peak Expiratory Flow Rate; PEO, Population-Exposure-Outcome; PM, Particulate Matter; PRISMA-ScR, Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews; RCT, Randomized Control Trial; SpCO, Carboxyhemoglobin saturation; SSA, Sub-Saharan Africa; WHO, World Health Organization; WMO, World Meteorological Organization.
References
1. Labaki, WW, and Han, MK. Chronic Respiratory Diseases: A Global View. The Lancet Respir Med (2020) 8(6):531–3. doi:10.1016/S2213-2600(20)30157-0
2. Mims, JW. Asthma: Definitions and Pathophysiology. Int Forum Allergy Rhinol (2015) 5(Suppl. 1):S2–6. doi:10.1002/alr.21609
3. Grace Marie, VK, Valeria Campos da, S, Guy, K, Patrick, D, Benoit, N, Bruno, M, et al. Chronic Respiratory Diseases in Africa: Identifying Social Determinants and Formulating Appropriate, strategic responses. (2021). KU Leuven: Enabel-Institute for Tropical Medicine Available from: https://www.researchgate.net/publication/353571587_Chronic_Respiratory_Diseases_in_Africa_Identifying_social_determinants_and_formulating_appropriate_strategic_responses (Accessed: September 6, 2023)
4. Adeloye, D, Song, P, Zhu, Y, Campbell, H, Sheikh, A, Rudan, I, et al. Global, Regional, and National Prevalence of, and Risk Factors for, Chronic Obstructive Pulmonary Disease (COPD) in 2019: A Systematic Review and Modelling Analysis. The Lancet Respir Med (2022) 10(5):447–58. doi:10.1016/S2213-2600(21)00511-7
5. World Health Organization. Chronic Obstructive Pulmonary Disease (COPD) (2023). Available from: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd) (Accessed: September 6, 2023)
6. Institute for Health Metrics and Evaluation. GBD Results (2024). Available from: https://vizhub.healthdata.org/gbd-results (Accessed March 12, 2024).
7. Mulubirhan, AA, Maria, EZ, Lucia, C, Peter, N, and Vanessa, GL, GBD 2019 Sub-Saharan COPD. Burden and Risk Factors of Chronic Obstructive Pulmonary Disease in Sub-Saharan African Countries, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. eClinicalMedicine (2023) 64:102215. Available from: https://www.thelancet.com/journals/eclinm/article/PIIS2589-5370(23)00392-9/fulltext (Accessed: December 22, 2023)
8. Stolbrink, M, Thomson, H, Hadfield, RM, Ozoh, OB, Nantanda, R, Jayasooriya, S, et al. The Availability, Cost, and Affordability of Essential Medicines for Asthma and COPD in Low-Income and Middle-Income Countries: A Systematic Review. The Lancet Glob Health (2022) 10(10):e1423–42. doi:10.1016/S2214-109X(22)00330-8
9. Muiser, S, Gosens, R, Berge, M van den, and Kerstjens, HAM. Understanding the Role of Long-Acting Muscarinic Antagonists in Asthma Treatment. Ann Allergy Asthma & Immunol (2022) 128(4):352–60. doi:10.1016/j.anai.2021.12.020
10. Miravitlles, M, Kawayama, T, and Dreher, M. LABA/LAMA as First-Line Therapy for COPD: A Summary of the Evidence and Guideline Recommendations. J Clin Med (2022) 11(22):6623. doi:10.3390/jcm11226623
11. van Gemert, FA, Kirenga, BJ, Gebremariam, TH, Nyale, G, de Jong, C, and van der Molen, T. The Complications of Treating Chronic Obstructive Pulmonary Disease in Low Income Countries of Sub-saharan Africa. Expert Rev Respir Med (2018) 12(3):227–37. doi:10.1080/17476348.2018.1423964
12. Scovronick, N, Sera, F, Acquaotta, F, Garzena, D, Fratianni, S, Wright, CY, et al. The Association between Ambient Temperature and Mortality in South Africa: A Time-Series Analysis. Environ Res (2018) 161:229–35. doi:10.1016/j.envres.2017.11.001
13. Ayres, JG, Forsberg, B, Annesi-Maesano, I, Dey, R, Ebi, KL, Helms, PJ, et al. Climate Change and Respiratory Disease: European Respiratory Society Position Statement. Eur Respir J (2009) 34(2):295–302. doi:10.1183/09031936.00003409
14. D’Amato, G, Cecchi, L, D’Amato, M, and Annesi-Maesano, I. Climate Change and Respiratory Diseases. Eur Respir Rev (2014) 23(132):161–9. doi:10.1183/09059180.00001714
15. Philippova, A, Aringazina, R, Kurmanalina, G, and Beketov, V. Epidemiology, Clinical and Physiological Manifestations of Dust Lung Disease in Major Industrial Centers. Emerg Themes Epidemiol (2022) 19:3. doi:10.1186/s12982-022-00111-0
16. Lepeule, J, Litonjua, AA, Gasparrini, A, Koutrakis, P, Sparrow, D, Vokonas, PS, et al. Lung Function Association with Outdoor Temperature and Relative Humidity and its Interaction with Air Pollution in the Elderly. Environ Res (2018) 165:110–7. doi:10.1016/j.envres.2018.03.039
17. Lohi, J, Tuomela, T, and Tuuminen, T. Exposure to Mould and Moisture Damage Is a Potential Risk Factor for the Development of Respiratory Diseases Opinion. Int J Immunol (2020) 8:38. doi:10.11648/j.iji.20200803.11
18. World Meteorological Organization. World Meteorological Organization Declares Onset of El Niño Conditions (2023) Available from: https://public.wmo.int/en/media/press-release/world-meteorological-organization-declares-onset-of-el-ni%C3%B1o-conditions (Accessed: September 6, 2023)
19. Kotir, JH. Climate Change and Variability in Sub-saharan Africa: A Review of Current and Future Trends and Impacts on Agriculture and Food Security. Environ Dev Sustain (2011) 13(3):587–605. doi:10.1007/s10668-010-9278-0
20. Omotoso, AB, and Omotayo, AO. The Interplay between Agriculture, Greenhouse Gases, and Climate Change in Sub-saharan Africa. Reg Environ Change (2023) 24(1):1. doi:10.1007/s10113-023-02159-3
21. UNFCCC. Climate Change Is an Increasing Threat to Africa (2024). Available from: https://unfccc.int/news/climate-change-is-an-increasing-threat-to-africa (Accessed October 9, 2024)
22. Williams, S, Sheikh, A, Campbell, H, Fitch, N, Griffiths, C, Heyderman, RS, et al. Respiratory Research Funding Is Inadequate, Inequitable, and a Missed Opportunity. Lancet Respir Med (2020) 8(8):e67–8. doi:10.1016/S2213-2600(20)30329-5
23. Adeloye, D, Basquill, C, Papana, A, Chan, KY, Rudan, I, and Campbell, H. An Estimate of the Prevalence of COPD in Africa: A Systematic Analysis. COPD: J Chronic Obstructive Pulm Dis (2015) 12(1):71–81. doi:10.3109/15412555.2014.908834
24. Finney, LJ, Feary, JR, Leonardi-Bee, J, Gordon, SB, and Mortimer, K. Chronic Obstructive Pulmonary Disease in Sub-saharan Africa: A Systematic Review. Int J Tuberc Lung Dis (2013) 17(5):583–9. doi:10.5588/ijtld.12.0619
25. Awokola, BI, Amusa, GA, Jewell, CP, Okello, G, Stobrink, M, Finney, LJ, et al. Chronic Obstructive Pulmonary Disease in Sub-saharan Africa. Int J Tuberc Lung Dis (2022) 26(3):232–42. doi:10.5588/ijtld.21.0394
26. van Gemert, F, van der Molen, T, Jones, R, and Chavannes, N. The Impact of Asthma and COPD in Sub-saharan Africa. Prim Care Respir J (2011) 20(3):240–8. doi:10.4104/pcrj.2011.00027
27. Mehrotra, A, Oluwole, AM, and Gordon, SB. The Burden of COPD in Africa: A Literature Review and Prospective Survey of the Availability of Spirometry for COPD Diagnosis in Africa. Trop Med & Int Health (2009) 14(8):840–8. doi:10.1111/j.1365-3156.2009.02308.x
28. Ndlovu, V, Chimbari, MJ, and Sibanda, E. Assessing the Nature of Asthma in African Epidemiological Studies: A Scoping Review Protocol. Syst Rev (2020) 9(1):230. doi:10.1186/s13643-020-01491-7
29. Adeloye, D, Chan, KY, Rudan, I, and Campbell, H. An Estimate of Asthma Prevalence in Africa: A Systematic Analysis. Croat Med J (2013) 54(6):519–31. doi:10.3325/cmj.2013.54.519
30. Arksey, H, and O’Malley, L. Scoping Studies: Towards a Methodological Framework. Int J Social Res Methodol (2005) 8(1):19–32. doi:10.1080/1364557032000119616
31. Levac, D, Colquhoun, H, and O’Brien, K. Scoping Studies: Advancing the Methodology. Implement Sci (2010) 5:69. doi:10.1186/1748-5908-5-69
32. Tricco, AC, Lillie, E, Zarin, W, O’Brien, KK, Colquhoun, H, Levac, D, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med (2018) 169(7):467–73. doi:10.7326/M18-0850
33. World Bank Country and Lending Groups. World Bank Data Help Desk (2023). Available from: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (Accessed November 16, 2023).
34. Ouzzani, M, Hammady, H, Fedorowicz, Z, and Elmagarmid, A. Rayyan—a Web and Mobile App for Systematic Reviews. Syst Rev (2016) 5(1):210. doi:10.1186/s13643-016-0384-4
35. Brakema, EA, Tabyshova, A, Van Der Kleij, RMJJ, Sooronbaev, T, Lionis, C, Anastasaki, M, et al. The Socioeconomic Burden of Chronic Lung Disease in Low-Resource Settings across the Globe - an Observational FRESH AIR Study. Respir Res (2019) 20(1):291. doi:10.1186/s12931-019-1255-z
36. Robertson, NM, Siddharthan, T, Pollard, SL, Alupo, P, Flores-Flores, O, Rykiel, NA, et al. Development and Validity Assessment of a Chronic Obstructive Pulmonary Disease Knowledge Questionnaire in Low- and Middle-Income Countries. Ann Am Thorac Soc (2021) 18(8):1298–305. doi:10.1513/AnnalsATS.202007-884OC
37. van Gemert, F, de Jong, C, Kirenga, B, Musinguzi, P, Buteme, S, Sooronbaev, T, et al. Effects and Acceptability of Implementing Improved Cookstoves and Heaters to Reduce Household Air Pollution: A FRESH AIR Study. npj Prim Care Respir Med (2019) 29(1):32. doi:10.1038/s41533-019-0144-8
38. Siddharthan, T, Pollard, SL, Quaderi, SA, Rykiel, NA, Wosu, AC, Alupo, P, et al. Discriminative Accuracy of Chronic Obstructive Pulmonary Disease Screening Instruments in 3 Low- and Middle-Income Country Settings. JAMA (2022) 327(2):151–60. doi:10.1001/jama.2021.23065
39. Siddharthan, T, Grigsby, MR, Goodman, D, Chowdhury, M, Rubinstein, A, Irazola, V, et al. Association between Household Air Pollution Exposure and Chronic Obstructive Pulmonary Disease Outcomes in 13 Low- and Middle-Income Country Settings. Am J Respir Crit Care Med (2018) 197(5):611–20. doi:10.1164/rccm.201709-1861OC
40. Egere, U, Shayo, EH, Chinouya, M, Taegtmeyer, M, Ardrey, J, Mpagama, S, et al. “Honestly, This Problem Has Affected Me a Lot”: A Qualitative Exploration of the Lived Experiences of People with Chronic Respiratory Disease in Sudan and Tanzania. BMC Public Health (2023) 23(1):485. doi:10.1186/s12889-023-15368-6
41. Eghomwanre, AF, and Oguntoke, O. Concentrations of Indoor Gaseous Air Pollutants and Risk Factors Associated with Childhood Asthma in Benin City, Nigeria. Environ Monit Assess (2022) 194(5):391. doi:10.1007/s10661-022-10026-7
42. Munyai, O, and Nunu, WN. Health Effects Associated with Proximity to Waste Collection Points in Beitbridge Municipality. Zimbabwe Waste Management (2020) 105:501–10. doi:10.1016/j.wasman.2020.02.041
43. Akpeimeh, GF, Fletcher, LA, and Evans, BE. Exposure to Bioaerosols at Open Dumpsites: A Case Study of Bioaerosols Exposure from Activities at Olusosun Open Dumpsite, Lagos Nigeria. Waste Management (2019) 89:37–47. doi:10.1016/j.wasman.2019.03.058
44. Obaseki, DO, Awopeju, OF, Awokola, BI, Adeniyi, BO, Adefuye, BO, Ozoh, OB, et al. Domestic Solid Fuel Combustion in an Adult Population in Nigeria: A Cross Sectional Analysis of Association with Respiratory Symptoms, Quality of Life and Lung Function. Respir Med (2017) 130:61–8. doi:10.1016/j.rmed.2017.07.014
45. Obiebi, IP, Ibekwe, RU, and Eze, GU. Lung Function Impairment Among Charcoal Workers in an Informal Occupational Setting in Southern Nigeria. Afr J Respir Med (2017) 13(1):8–13.
46. Ayaaba, E, Li, Y, Yuan, J, and Ni, C. Occupational Respiratory Diseases of Miners from Two Gold Mines in Ghana. Int J Environ Res Public Health (2017) 14(3):337. doi:10.3390/ijerph14030337
47. Hamatui, N, and Beynon, C. Particulate Matter and Respiratory Symptoms Among Adults Living in Windhoek, Namibia: A Cross Sectional Descriptive Study. Int J Environ Res Public Health (2017) 14(2):110. doi:10.3390/ijerph14020110
48. Agrawal, S. Effect of Indoor Air Pollution from Biomass and Solid Fuel Combustion on Prevalence of Self-Reported Asthma Among Adult Men and Women in India: Findings from a Nationwide Large-Scale Cross-Sectional Survey. J Asthma (2012) 49(4):355–65. doi:10.3109/02770903.2012.663030
49. Landry, MMJ, and Soleil, BRA. The Influence of Climate Change/variability on the Prevalence of Respiratory Diseases: The Case of Asthma in Bamenda (2024).
50. Pathak, U, Gupta, N, Suri, J, and Tyagi, C. Effects of Biomass Fuel Generated Indoor Air Pollution on Prevalence of Self-Reported Asthma Among Adult Women in North Indian Rural Villages. JoARMST (2018) 5:10–3. doi:10.24321/2394.6539.201805
51. Mustapha, BA, Blangiardo, M, Briggs, DJ, and Hansell, AL. Traffic Air Pollution and Other Risk Factors for Respiratory Illness in Schoolchildren in the niger-delta Region of Nigeria. Environ Health Perspect (2011) 119(10):1478–82. doi:10.1289/ehp.1003099
52. René, KAK, Kouadio, K, Siele, S, Harvey, AT, M’begnan, C, Leandre, K, et al. Prevalence of Asthma in Children under 5 Years Old Exposed to Air Pollution in Abidjan,(Côte D’ivoire). Int J Recent Scientific Res (2019) 10(07):33353–8. doi:10.24327/ijrsr.2019.1007.3655
53. Abbas, A, Okpapi, JU, Njoku, CH, Abba, AA, Isezuo, SA, and Danasabe, IM. Influence of Seasonal Changes on Asthma Exacerbation in a sudan Savanna Region: An Analysis of 87 Cases. Ann Afr Med (2021) 20(4):302–6. doi:10.4103/aam.aam_66_20
54. Eghomwanre, AF, Oguntoke, O, and Taiwo, AM. Levels of Indoor Particulate Matter and Association with Asthma in Children in Benin City, Nigeria. Environ Monit Assess (2022) 194(7):467. doi:10.1007/s10661-022-10135-3
55. Desalu, OO. Seasonal Variation in Hospitalisation for Respiratory Diseases in the Tropical Rain Forest of South Western Nigeria. The Niger Postgrad Med J (2011) 18(1):39–43. doi:10.4103/1117-1936.170300
56. McElroy, S, Dimitrova, A, Evan, A, and Benmarhnia, T. Saharan Dust and Childhood Respiratory Symptoms in Benin. Int J Environ Res Public Health (2022) 19(8):4743. doi:10.3390/ijerph19084743
57. Oyebanji, FF, Ana, GREE, Mijinyawa, Y, and Ogunseye, OO. Predicting Exposure to Dust Particles Using Spirometric Index and Perception Studies Among Farmers in Selected Farm Settlements in Ogun State, nigeria. Aerosol Air Qual Res (2021) 21(7):200509. doi:10.4209/aaqr.200509
58. Woolley, KE, Bagambe, T, Singh, A, Avis, WR, Kabera, T, Weldetinsae, A, et al. Investigating the Association between Wood and Charcoal Domestic Cooking, Respiratory Symptoms and Acute Respiratory Infections Among Children Aged under 5 Years in uganda: A Cross-Sectional Analysis of the 2016 Demographic and Health Survey. Int J Environ Res Public Health (2020) 17(11):3974–14. doi:10.3390/ijerph17113974
59. Tamire, M, Addissie, A, Kumie, A, Husmark, E, Skovbjerg, S, Andersson, R, et al. Respiratory Symptoms and Lung Function Among Ethiopian Women in Relation to Household Fuel Use. Int J Environ Res Public Health (2020) 17(1):41. doi:10.3390/ijerph17010041
60. Brakema, EA, Tabyshova, A, Kasteleyn, MJ, Molendijk, E, Van Der Kleij, RMJJ, Van Boven, JFM, et al. High COPD Prevalence at High Altitude: Does Household Air Pollution Play a Role? Eur Respir J (2019) 53(2):1801193. doi:10.1183/13993003.01193-2018
61. Das, I, Jagger, P, and Yeatts, K. Biomass Cooking Fuels and Health Outcomes for Women in Malawi. EcoHealth (2017) 14(1):7–19. doi:10.1007/s10393-016-1190-0
62. Ngahane, BHM, Ze, EA, Chebu, C, Mapoure, NY, Temfack, E, Nganda, M, et al. Effects of Cooking Fuel Smoke on Respiratory Symptoms and Lung Function in Semi-rural Women in Cameroon. Int J Occup Environ Health (2015) 21(1):61–5. doi:10.1179/2049396714Y.0000000090
63. Mohammad, Y, Shaaban, R, Al-Zahab, BA, Khaltaev, N, Bousquet, J, and Dubaybo, B. Impact of Active and Passive Smoking as Risk Factors for Asthma and COPD in Women Presenting to Primary Care in Syria: First Report by the WHO-GARD Survey Group. Int J COPD (2013) 8:473–82. doi:10.2147/COPD.S50551
64. Quansah, R, Bend, JR, Armah, FA, Bonney, F, Aseidu, J, Yawson, DO, et al. Respiratory and Non-respiratory Symptoms Associated with Pesticide Management Practices Among Farmers in Ghana’s Most Important Vegetable Hub. Environ Monit Assess (2019) 191(12):716. doi:10.1007/s10661-019-7898-x
65. Omonijo, AG, Oguntoke, O, Matzarakis, A, and C, OA. A Study of Weather Related Respiratory Diseases in Eco-Climatic Zones. Afr Phys Rev (2011) 5:41–56.
66. Narh, CT, Der, JB, Afetor, M, Ofosu, A, Blettner, M, and Wollschlaeger, D. Sociodemographic Factors Associated with Time to Discharge for Hospitalised Patients with Asthma and Asthma Exacerbation Using the Ghana Health Service District Information Management System 2 (DHIMS-2) Database, 2012-2017. BMJ Open Respir Res (2021) 8(1):e001034. doi:10.1136/bmjresp-2021-001034
67. Olujimi, OO, Ana, GREE, Ogunseye, OO, and Fabunmi, VT. Air Quality Index from Charcoal Production Sites, Carboxyheamoglobin and Lung Function Among Occupationally Exposed Charcoal Workers in South Western Nigeria. SpringerPlus (2016) 5(1):1546. doi:10.1186/s40064-016-3227-9
68. Subramaniam, S, Ganesan, A, Raju, N, and Prakash, C. Investigation of Indoor Air Quality and Pulmonary Function Status Among Power Loom Industry Workers in Tamil Nadu, South India. Air Qual Atmos Health (2023) 17:215–30. doi:10.1007/s11869-023-01439-5
69. Oo, TW, Thandar, M, Htun, YM, Soe, PP, Lwin, TZ, Tun, KM, et al. Assessment of Respiratory Dust Exposure and Lung Functions Among Workers in Textile Mill (Thamine), Myanmar: A Cross-Sectional Study. BMC Public Health (2021) 21(1):673. doi:10.1186/s12889-021-10712-0
70. Leon-Kabamba, N, Ngatu, NR, Kakoma, SJB, Nyembo, C, Mbelambela, EP, Moribe, RJ, et al. Respiratory Health of Dust-Exposed Congolese Coltan Miners. Int Arch Occup Environ Health (2018) 91(7):859–64. doi:10.1007/s00420-018-1329-0
71. Dushyant, K, Walia, GK, and Devasenapathy, N. Lung Function and Respiratory Morbidity Among Informal Workers Exposed to Cement Dust: A Comparative Cross-Sectional Study. Study (2023) 89(1):47. doi:10.5334/aogh.4089
72. Jestin-Guyon, N, Ouaalaya, EH, Harison, MT, Ravahatra, K, Rakotomizao, J, Raharimanana, RN, et al. Impact of Biomass Fuel Smoke on Respiratory Health of Children under 15 Years Old in Madagascar. Respir Med Res (2023) 83:100989. doi:10.1016/j.resmer.2023.100989
73. Meme, H, Amukoye, E, Bowyer, C, Chakaya, J, Das, D, Dobson, R, et al. Asthma Symptoms, Spirometry and Air Pollution Exposure in Schoolchildren in an Informal Settlement and an Affluent Area of Nairobi, Kenya. Thorax (2023) 78(11):1118–25. doi:10.1136/thorax-2023-220057
74. Wafula, ST, Nalugya, A, Mendoza, H, Kansiime, WK, Ssekamatte, T, Walekhwa, AW, et al. Indoor Air Pollutants and Respiratory Symptoms Among Residents of an Informal Urban Settlement in Uganda: A Cross-Sectional Study. PLOS ONE (2023) 18(8):e0290170. doi:10.1371/journal.pone.0290170
75. Zoller, T, Mfinanga, EH, Zumba, TB, Asilia, PJ, Mutabazi, EM, Wimmersberger, D, et al. Symptoms and Functional Limitations Related to Respiratory Health and Carbon Monoxide Poisoning in Tanzania: A Cross Sectional Study. Environ Health A Glob Access Sci Source (2022) 21(1):38. doi:10.1186/s12940-022-00847-x
76. Tamire, M, Worku, A, Addissie, A, Ayele, S, Haile, T, and Bekele, A. Blinded to Their Own Daily Sufferings: The Lived Experience of Patients with Chronic Obstructive Pulmonary Disease in Addis Ababa. Ethiopian J Health Development (2021) 35(4). doi:10.21203/rs.3.rs-105773/v1
77. Jones, R, Kirenga, B, Buteme, S, Williams, S, and Van Gemert, F. A Novel Lung Health Programme Addressing Awareness and Behaviour-Change Aiming to Prevent Chronic Lung Diseases in Rural Uganda. Afr J Respir Med (2020) 14(2):2–9.
78. Brakema, EA, van Gemert, FA, Williams, S, Sooronbaev, T, Emilov, B, Mademilov, M, et al. Implementing a Context-Driven Awareness Programme Addressing Household Air Pollution and Tobacco: A FRESH AIR Study. NPJ Prim Care Respir Med (2020) 30(1):42. doi:10.1038/s41533-020-00201-z
79. Cartwright, LL, Callaghan, LE, Jones, RC, Nantanda, R, and Fullam, J. Perceptions of Long Term Impact and Change Following a Midwife Led Biomass Smoke Education Program for Mothers in Rural Uganda: A Qualitative Study. Rural and Remote Health (2022) 22(1):6893. doi:10.22605/RRH6893
80. Nantanda, R, Buteme, S, van Kampen, S, Cartwright, L, Pooler, J, Barton, A, et al. Feasibility and Acceptability of a Midwife-Led Health Education Strategy to Reduce Exposure to Biomass Smoke Among Pregnant Women in Uganda, A FRESH AIR Project. Glob Public Health (2019) 14(12):1770–83. doi:10.1080/17441692.2019.1642931
81. Rylance, S, Chinoko, B, Mnesa, B, Jewell, C, Grigg, J, and Mortimer, K. An Enhanced Care Package to Improve Asthma Management in Malawian Children: A Randomised Controlled Trial. Thorax (2021) 76(5):434–40. doi:10.1136/thoraxjnl-2020-216065
82. Amorha, KC, Okonta, MJ, and Ukwe, CV. Impact of Pharmacist-Led Educational Interventions on Asthma Control and Adherence: Single-Blind, Randomised Clinical Trial. Int J Clin Pharm (2021) 43(3):689–97. doi:10.1007/s11096-020-01187-x
83. Rennert, WP, Porras Blanco, RM, and Muniz, GB. The Effects of Smokeless Cookstoves on Peak Expiratory Flow Rates in Rural Honduras. J Public Health (UK) (2015) 37(3):455–60. doi:10.1093/pubmed/fdu087
84. Critchley, K, Teather, K, Hughes, H, Macdonald, A, Gibson, M, J, B, et al. Air Quality, Respiratory Health and Wood Use for Women Converting from Low-to High-Efficiency Stoves in Rural Kenya. 23rd International Conference on Modelling, Monitoring and Management of Air Pollution, AIR 2015 (2015) 198:205–16.
85. Rylance, S, Jewell, C, Naunje, A, Mbalume, F, Chetwood, JD, Nightingale, R, et al. Non-communicable Respiratory Disease and Air Pollution Exposure in Malawi: A Prospective Cohort Study. Thorax (2020) 75(3):220–6. doi:10.1136/thoraxjnl-2019-213941
86. Sooriyakanthan, M, Orme, MW, Sivapalan, K, Selvaratnam, G, Singh, SJ, and Wimalasekera, S. A Feasibility Trial of Pulmonary Rehabilitation for Patients with COPD in a Low Resource Setting: Jaffna, Sri Lanka. BMC Pulm Med (2022) 22(1):302. doi:10.1186/s12890-022-02092-x
87. Leng, MEF, Daniel, S, and Munday, D. Respiratory Problems in Low-Resource Settings. Curr Opin Support Palliat Care (2017) 11(3):174–8. doi:10.1097/SPC.0000000000000287
88. Uzaslan, E, Mahboub, B, Beji, M, Nejjari, C, Tageldin, MA, Khan, JA, et al. The Burden of Chronic Obstructive Pulmonary Disease in the Middle East and North Africa: Results of the BREATHE Study. Respir Med (2012) 106:S45–59. doi:10.1016/S0954-6111(12)70014-8
89. Rossaki, FM, Hurst, JR, van Gemert, F, Kirenga, BJ, Williams, S, Khoo, EM, et al. Strategies for the Prevention, Diagnosis and Treatment of COPD in Low- and Middle-Income Countries: The Importance of Primary Care. Expert Rev Respir Med (2021) 15(12):1563–77. doi:10.1080/17476348.2021.1985762
90. AR6 Synthesis Report. Clim Change (2023). Available from: https://www.ipcc.ch/report/ar6/syr/ (Accessed October 7, 2024).
91. Romanello, M, Napoli, Cdi, Green, C, Kennard, H, Lampard, P, Scamman, D, et al. The 2023 Report of the Lancet Countdown on Health and Climate Change: The Imperative for a Health-Centred Response in a World Facing Irreversible Harms. The Lancet (2023) 402(10419):2346–94. doi:10.1016/S0140-6736(23)01859-7
92. Jones, A. The Health Impacts of Climate Change: Why Climate Action Is Essential to Protect Health. Orthopaedics and Trauma (2022) 36(5):248–55. doi:10.1016/j.mporth.2022.07.001
93. Anderson, GB, Dominici, F, Wang, Y, McCormack, MC, Bell, ML, and Peng, RD. Heat-related Emergency Hospitalizations for Respiratory Diseases in the Medicare Population. Am J Respir Crit Care Med (2013) 187(10):1098–103. doi:10.1164/rccm.201211-1969OC
94. Chen, M, Zhang, K, Zhang, X, Gao, J, Zhang, R, Wei, X, et al. Association between Living Habits, Indoor Humidity, Ventilation and Asthma Among Residents in the Tropical Regions of China. Front Public Health (2023) 11:1294115. doi:10.3389/fpubh.2023.1294115
95. Lam, HCyu, Li, AM, Chan, EYyang, and Goggins, WB. The Short-Term Association Between Asthma Hospitalisations, Ambient Temperature, Other Meteorological Factors and Air Pollutants in Hong Kong: A Time-Series Study. Thorax (2016) 71(12):1097–109. doi:10.1136/thoraxjnl-2015-208054
96. D’Amato, G, Chong-Neto, HJ, Monge Ortega, OP, Vitale, C, Ansotegui, I, Rosario, N, et al. The Effects of Climate Change on Respiratory Allergy and Asthma Induced by Pollen and Mold Allergens. Allergy (2020) 75(9):2219–28. doi:10.1111/all.14476
97. Syed, M, Folz, RJ, and Ali, U. Environmental Factors and Their Impact on Airway Diseases: Exploring Air Pollution, Indoor and Outdoor Allergens, and Climate Change. Curr Pulmonol Rep (2023) 12(3):162–70. doi:10.1007/s13665-023-00319-8
98. Pinho-Gomes, AC, Roaf, E, Fuller, G, Fowler, D, Lewis, A, ApSimon, H, et al. Air Pollution and Climate Change. Lancet Planet Health (2023) 7(9):e727–8. doi:10.1016/S2542-5196(23)00189-4
99. Orru, H, Ebi, KL, and Forsberg, B. The Interplay of Climate Change and Air Pollution on Health. Curr Environ Health Rep (2017) 4(4):504–13. doi:10.1007/s40572-017-0168-6
100. Chidumayo, EN, and Gumbo, DJ. The Environmental Impacts of Charcoal Production in Tropical Ecosystems of the World: A Synthesis. Energy Sustainable Development (2013) 17(2):86–94. doi:10.1016/j.esd.2012.07.004
101. Nike, D, and Charles, M. The Marginalization of Sustainable Charcoal Production in the Policies of a Modernizing African Nation. Front. Environ. Sci. (2024) 5. doi:10.3389/fenvs.2017.00027
102. Teodoro-Paulo, J, Deere, JA, Valeriano-Santos, J, Charlesworth, S, Duncan, AB, Kant, MR, et al. Rising Temperatures Favour Defence-Suppressing Herbivores. J Pest Sci (2024). doi:10.1007/s10340-024-01781-2
103. Srinivasa Rao, M, Mani, M, Prasad, YG, Prabhakar, M, Sridhar, V, Vennila, S, et al. Climate Change and Pest Management Strategies in Horticultural and Agricultural Ecosystems. In: M Mani, editor. Trends in Horticultural Entomology. Singapore: Springer Nature (2022). 81–122. doi:10.1007/978-981-19-0343-4_3
104. Hesam, K, Morteza, S, Haslenda, H, and Mohammad, Y. Carbon Dynamics in Agricultural Greenhouse Gas Emissions and Removals: A Comprehensive Review. Carbon Lett (2024) 34:265–289. doi:10.1007/s42823-023-00647-4
105. Shaheen, SO, Jameson, KA, Syddall, HE, Sayer, AA, Dennison, EM, Cooper, C, et al. The Relationship of Dietary Patterns with Adult Lung Function and COPD. Eur Respir J (2010) 36(2):277–84. doi:10.1183/09031936.00114709
106. Keranis, E, Makris, D, Rodopoulou, P, Martinou, H, Papamakarios, G, Daniil, Z, et al. Impact of Dietary Shift to Higher-Antioxidant Foods in COPD: A Randomised Trial. Eur Respir J (2010) 36(4):774–80. doi:10.1183/09031936.00113809
107. Scoditti, E, Massaro, M, Garbarino, S, and Toraldo, DM. Role of Diet in Chronic Obstructive Pulmonary Disease Prevention and Treatment. Nutrients (2019) 11(6):1357. doi:10.3390/nu11061357
108. Berthon, BS, and Wood, LG. Nutrition and Respiratory Health—Feature Review. Nutrients (2015) 7(3):1618–43. doi:10.3390/nu7031618
109. World Health Organization. WHO Global Strategy for Food Safety 2022-2030: Towards Stronger Food Safety Systems and Global Cooperation (2023). Available from: https://www.who.int/publications-detail-redirect/9789240057685 (Accessed December 28, 2023)
110. Kogan, F, Guo, W, and Yang, W. Drought and Food Security Prediction from NOAA New Generation of Operational Satellites. Geomatics, Nat Hazards Risk (2019) 10(1):651–66. doi:10.1080/19475705.2018.1541257
111. Mayén, AL, de Mestral, C, Zamora, G, Paccaud, F, Marques-Vidal, P, Bovet, P, et al. Interventions Promoting Healthy Eating as a Tool for Reducing Social Inequalities in Diet in Low- and Middle-Income Countries: A Systematic Review. Int J Equity Health (2016) 15(1):205. doi:10.1186/s12939-016-0489-3
112. White, SC, Agurto, I, and Araguas, N. Promoting Healthy Behaviors to Prevent Chronic Disease in Panama and Trinidad & Tobago: Results of the Women as Agents of Change Project. J Community Health (2006) 31(5):413–29. doi:10.1007/s10900-006-9022-8
113. Vio, F, Lera, L, and Zacaría, I. Evaluation of a Nutrition Education and Physical Activity Intervention in Chilean Low Socioeconomic Women. Arch Latinoam Nutr (2011) 61(4):406–13.
114. Simatele, MD, Tantoh, HB, and Donkor, FK. Editorial: Climate Change, Land, Energy and Food Security: Perspectives from Sub-saharan Africa. Front Sustainable Food Syst (2023) 7. doi:10.3389/fsufs.2023.1164917
115. Müller, C, Ouédraogo, WA, Schwarz, M, Barteit, S, and Sauerborn, R. The Effects of Climate Change-Induced Flooding on Harvest Failure in Burkina Faso: Case Study. Front Public Health (2023) 11:1166913. doi:10.3389/fpubh.2023.1166913
116. Al Daccache, M, Abi Zeid, B, Hojeij, L, Baliki, G, Brück, T, and Ghattas, H. Systematic Review on the Impacts of Agricultural Interventions on Food Security and Nutrition in Complex Humanitarian Emergency Settings. BMC Nutr (2024) 10(1):60. doi:10.1186/s40795-024-00864-8
117. Kevaki, S, Ngocho, JS, Amour, C, Schmid-Grendelmeier, P, Mmbaga, Bt, and Renz, H. Epidemiology and Management of Asthma and Atopic Dermatitis in Sub-saharan Africa. The J Allergy Clin Immunol (2021) 148(6):1378–86. doi:10.1016/j.jaci.2021.10.019
118. Adeloye, D, Agarwal, D, Barnes, PJ, Bonay, M, van Boven, JF, Bryant, J, et al. Research Priorities to Address the Global Burden of Chronic Obstructive Pulmonary Disease (COPD) in the Next Decade. J Glob Health (2021) 11:15003. doi:10.7189/jogh.11.15003
119. Hurst, JR, Buist, AS, Gaga, M, Gianella, GE, Kirenga, B, Khoo, EM, et al. Challenges in the Implementation of Chronic Obstructive Pulmonary Disease Guidelines in Low- and Middle-Income Countries: An Official American Thoracic Society Workshop Report. Ann Am Thorac Soc. (2021) 18(8):1269–1277. doi:10.1513/AnnalsATS.202103-284ST
120. Organization, WH. WHO Package of Essential Noncommunicable (PEN) Disease Interventions for Primary Health Care. Geneve, Switzerland: World Health Organization (2020). Available from: https://iris.who.int/handle/10665/334186 (Accessed October 24, 2024).
Keywords: COPD, asthma, low-and middle-income countries, sub-Saharan Africa, climate change
Citation: Boutros P, Kassem N, Boudo V, Sié A, Munga S, Maggioni MA, Golec M, Simion R, Bärnighausen T, Winkler V and Barteit S (2024) Understanding the Risk Factors, Burden, and Interventions for Chronic Respiratory Diseases in Low- and Middle-Income Countries: A Scoping Review. Public Health Rev 45:1607339. doi: 10.3389/phrs.2024.1607339
Received: 29 March 2024; Accepted: 22 October 2024;
Published: 31 October 2024.
Edited by:
Nino Kuenzli, Swiss Tropical and Public Health Institute (Swiss TPH), SwitzerlandReviewed by:
Rafaella Moreira, University of International Integration of Afro-Brazilian Lusophony, BrazilNino Kuenzli, Swiss Tropical and Public Health Institute (Swiss TPH), Switzerland
Copyright © 2024 Boutros, Kassem, Boudo, Sié, Munga, Maggioni, Golec, Simion, Bärnighausen, Winkler and Barteit. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
PHR is edited by the Swiss School of Public Health (SSPH+) in a partnership with the Association of Schools of Public Health of the European Region (ASPHER)+
*Correspondence: Sandra Barteit, YmFydGVpdEB1bmktaGVpZGVsYmVyZy5kZQ==