 Rafaella Pessoa Moreira1*
Rafaella Pessoa Moreira1* Clara Beatriz Costa da Silva1Tainara Chagas de Sousa1Flávia Lavinnya Betsaida Félix Leitão1Huana Carolina Cândido Morais1Andressa Suelly Saturtino de Oliveira1
Clara Beatriz Costa da Silva1Tainara Chagas de Sousa1Flávia Lavinnya Betsaida Félix Leitão1Huana Carolina Cândido Morais1Andressa Suelly Saturtino de Oliveira1 Gonzalo Duarte-Clíments2,3María Begoña Sánchez Gómez2,4
Gonzalo Duarte-Clíments2,3María Begoña Sánchez Gómez2,4 Tahissa Frota Cavalcante1Alexandre Cunha Costa5
Tahissa Frota Cavalcante1Alexandre Cunha Costa5- 1Institute of Health Sciences, University of International Integration of Afro-Brazilian Lusophony, Redenção, Brazil
- 2School of Nursing, University of La Laguna, San Cristóbal de La Laguna, Spain
- 3School of Nursing, Valencian International University, Castelló de la Plana, Spain
- 4Department of Nursing, UCAM Catholic University of Murcia, Guadalupe, Spain
- 5Institute of Engineering and Sustainable Development, University of International Integration of Afro-Brazilian Lusophony, Redenção, Brazil
Objectives: In the face of escalating global aridification, this study examines the complex relationship between climate variability, air pollution, natural disasters, and the prevalence of cardiovascular disease (CVD) and diabetes mellitus (DM) in arid regions.
Methods: The study conducted a scoping review of multiple databases using JBI guidelines and included 74 studies.
Results: The results show that acute myocardial infarction (n = 20) and stroke (n = 13) are the primary CVDs affected by these factors, particularly affecting older adults (n = 34) and persons with hypertension (n = 3). Elevated air temperature and heat waves emerge as critical risk factors for CVD, exacerbating various cardiovascular mechanisms. Atmospheric pollutants and natural disasters increase this risk. Indirect effects of disasters amplify risk factors such as socioeconomic vulnerability (n = 4), inadequate medical care (n = 3), stress (n = 3), and poor diet (n = 2), increasing CVD and DM risk.
Conclusion: The study underscores the need for nations to adhere to the Paris Agreement, advocating for reduced air pollutants, resilient environments, and collaborative, multidisciplinary research to develop targeted health interventions to mitigate the adverse effects of climate, pollution, and natural disasters.
Introduction
Climate change is characterized by long-term increase in temperature, changes in the geographical distribution of precipitation, and an increase in the magnitude and frequency of extreme weather events such as floods, droughts, and heatwaves [1, 2]. These changes in weather patterns can influence people’s health and lead to the development of Climate-Sensitive Diseases (CSD) [3, 4]. Climate change represents one of the most significant threats to human wellbeing [5], making the global population more vulnerable to CSDs such as cardiovascular diseases (CVD) and diabetes mellitus (DM) [6–9].
In the face of climate change, climate projections indicate an increase of drylands worldwide over the coming decades [10–12]. Drylands (arid, semi-arid, and dry sub-humid lands) are characterized by natural water scarcity, where the annual ratio between precipitation and evapotranspiration, or aridity index, is greater than 0.05 and less than 0.65. Drylands cover 41% of the land surface, produce 44% of the crops, and contain over 2 billion people and half of the world’s livestock [13].
In dry regions, extreme weather events such as droughts [14], dust or sandstorms [15], heatwaves [16], and/or fires are frequent [12, 17, 18]. These weather events can occur in combination [19]. Additionally, other natural disasters such as earthquakes and hurricanes may also be recurrent and affected by climate change [20]. Populations in drylands, constantly affected by natural disasters, are more vulnerable to subsistence crises [21], poverty, economic and political marginalization [22], and health problems [23].
Recent studies highlight the effects of climate on cardiovascular diseases [24] and diabetes mellitus [25], where extreme temperatures, changes in relative humidity, and wind intensity were determining factors. Furthermore, the role of global climate phenomena such as El Niño in the development and/or exacerbation of CVD is emphasized [24–26].
Air pollution, combined with climatic effects, poses an additional risk factor for mortality from cardiovascular diseases and influences the increase in hospitalizations due to diabetes mellitus [27, 28]. Furthermore, the contribution of increased air pollution to the retention of greenhouse gases, responsible for warming the Earth’s surface and raising temperatures globally [1], highlights its role in the long-term effects of climate change on CVD.
Thus, in addition to established risk factors for CVD and DM, known as non-modifiable (ethnicity, age, family history) and modifiable (sedentary lifestyle, poor diet, alcoholism, smoking, dyslipidemia, obesity) [29, 30], it is necessary to map the risk factors for CVD and DM related to climate variability, air pollution, and natural disasters. In this context, it is also relevant to identify populations living in dry regions that are most vulnerable to developing cardiovascular diseases and diabetes mellitus.
The general objective of this scoping review was to map the influence of climate variability, air pollution, and natural disasters on cardiovascular diseases and diabetes mellitus in drylands, aiming to identify the main cardiovascular diseases, the most vulnerable populations, the socio-environmental factors related to physiological mechanisms for the development and/or exacerbation of these diseases, and the main risk factors intensified by natural disasters.
It is expected that the results of this research will be useful for the development of public health protocols that can guide the implementation of effective multidisciplinary interventions for the prevention of CVD and DM and their complications resulting from climate variability, air pollution, and natural disasters in dry regions, especially in populations identified as most vulnerable in a context of climate change.
Methods
A scoping review was conducted following the Joanna Briggs Institute (JBI) approach for scoping reviews, the PRISMA Extension for Scoping Reviews (PRISMA-ScR) guidelines, and the JBI Evidence Synthesis Manual. The protocol was registered in the Open Science Framework (OSF). Registration DOI.
Review Question
The Population, Concept, and Context (PCC) framework was adopted to formulate the research questions:
Population
Individuals with cardiovascular diseases: Group of heart and blood vessel diseases, including: coronary artery disease, acute myocardial infarction; cerebrovascular disease: peripheral artery disease; rheumatic heart disease; congenital heart disease; deep vein thrombosis and pulmonary embolism [31]; diabetes: Chronic metabolic disease characterized by high blood glucose levels, leading over time to serious damage to the heart, blood vessels, eyes, kidneys, and nerves [31].
Concept
Climate variability: Variations in climate compared to its average, resulting in changes in air pressure, temperature, precipitation, humidity, and other climate variables [32]. The climate variables included in this study are: air temperature, precipitation, air humidity, wind speed, and phenomena such as El Niño; Air pollution: Refers to contamination of the indoor or outdoor environment resulting in the modification of the atmosphere’s natural characteristics. This contamination can occur due to chemical, physical, or biological agents [20]; Natural disasters: Severe weather conditions, including floods, tornadoes, hurricanes, wildfires, droughts, earthquakes, or a combination of these extreme events. They represent a major threat to infrastructure, health, property, and human security [33].
Context
Drylands characterized by water scarcity (a ratio between average annual precipitation and potential evapotranspiration, also known as aridity index, greater than 0.05 and less than 0.65). They can be classified as arid, semi-arid, and dry sub-humid lands [34].
Based on the aforementioned strategy, the following research question was formulated: 1) What is the influence of climate variability, air pollution, and natural disasters on cardiovascular diseases and diabetes mellitus in drylands? In this context, the following auxiliary questions were identified: 1) What are the most prevalent cardiovascular diseases and which populations are most vulnerable? 2) What are the effects of exposure to climate variability, air pollution, and natural disasters on hospitalizations and deaths from cardiovascular diseases? 3) What are the socio-environmental factors related to physiological mechanisms for the development and/or exacerbation of cardiovascular diseases? 4) What are the main risk factors for cardiovascular diseases and diabetes mellitus intensified by natural disasters?
Eligibility Criteria
Inclusion: Studies that addressed the research questions, formulated based on the PCC framework, were included. Multinational studies that included any dry climate region were also included in this review.
Exclusion: Descriptive studies without identification of influencing factors, duplicate studies (only one of the studies was considered for analysis), and studies not available in full text.
Study Designs
We included studies using various designs: experimental and quasi-experimental studies (randomized and non-randomized controlled trials), before-after and interrupted time series studies, and analytical observational studies (prospective and retrospective cohort studies, case-control studies, and cross-sectional analytical studies), as well as descriptive observational studies including case series and reports of individual cases, qualitative studies, and systematic reviews. No language or time restrictions were applied.
Search Strategy
The search strategies were developed by the research team in collaboration with a librarian, utilizing the PCC components. Search terms were identified from controlled vocabularies such as Health Sciences Descriptors (DeCS), Medical Subject Headings (MeSH), and Embase Subject Headings (Emtree).
The search involved three steps. Firstly, a preliminary search in PubMed, Cochrane Library, OSF, and JBI Synthesis identified keywords and terms for the search strategy. Secondly, this strategy was applied to all chosen databases. A third search checked reference lists for additional sources. The detailed search strategies are in Supplementary Appendix Table S1. Searches were conducted on 04 September 2023, across various databases and gray literature sources, including Agris, Virtual Health Library, Academic Search Premier, CINAHL, GreenFILE, SocINDEX, CAB Direct, Cochrane Library, Embase, Engineering Village, Epistemonikos, PubMed Central, PubMed, Scielo, Scopus, and Web of Science.
Descriptors
Cardiovascular diseases; Cardiopathies; Diabetes Mellitus; Stroke; Coronary Disease; Coronary Artery Disease; Droughts; Dryland; Arid Season; Arid Zone; Semi-Arid Zone; “atmosphere pollution”; Natural Disasters.
Study Selection
After completing the bibliographic search, all results obtained from the databases were grouped and then exported to Rayyan CRI from Qatar, specifically for blinded document selection. Duplicates were removed, and titles and abstracts were independently assessed by two pairs of blinded reviewers based on predefined inclusion criteria. Potentially relevant sources were retrieved in full, and citation details were imported into the JBI System for unified management, assessment, and information review. The full text of selected citations was evaluated according to the inclusion criteria by two pairs of independent reviewers. Reasons for excluding full-text articles were recorded and reported. Any discrepancies among reviewers at each stage of the selection process were resolved through discussion or involvement of a third reviewer—the responsible researcher. Screening was only completed when the agreement proportion among reviewers reached or exceeded 75% [35].
Methodological Quality Assessment
As this study is a scoping review aiming to map available evidence, no bias risk assessment or quality assessment of included studies was conducted. However, we emphasize that the study remains consistent with the methodology proposed for scoping reviews [35].
Graphs, Data Extraction, and Synthesis of Results
Data extraction included the following elements: database, title, year, country, authorship, objective, study design, cardiovascular diseases/diabetes mellitus, risk factors, gender, age, and climatic variable. Results were mapped, organized into tables/diagrams/figures, and subjected to thematic analysis and narrative synthesis based on full-text article reading. Labels reflecting content were created for passages that addressed research questions, and similar passages were subsequently grouped [36], resulting in the construction of three thematic categories: climate variability, air pollution, and natural disasters. Figures were created to present thematic categories and associated risk factors influencing the development of CVD or exacerbation of DM, aiming to synthesize the findings of this review. Tables are provided in Supplementary Appendix S1.
Role of Funding Source
The funding sources had no involvement in study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the paper for publication.
Results
The search process is summarized in a PRISMA flow diagram in Figure 1. Initially, a total of 5,660 studies were identified. Following title and abstract screening, 2,180 studies were selected for further consideration. Subsequently, after full-text screening, 228 studies remained. After a second full-text screening, 74 studies were ultimately selected for data extraction as they met the inclusion criteria. A synthesis of the selected studies can be found in Supplementary Appendix S2.
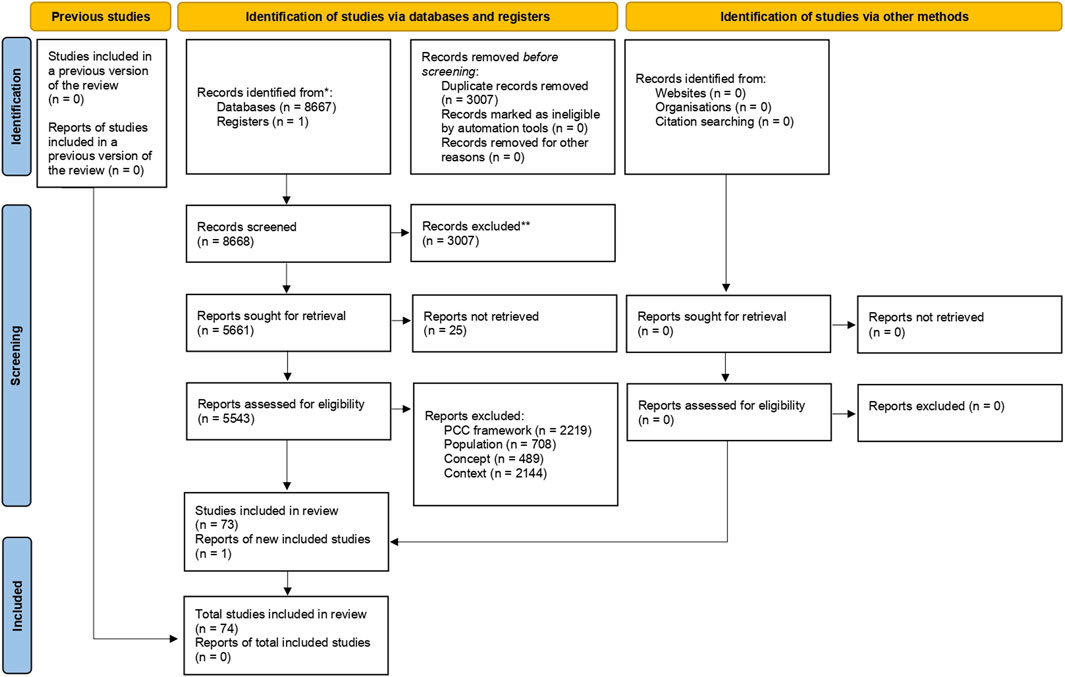
Figure 1. Flowchart of study selection based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (2023, Brazil).
The articles identified in the review are notably recent, with 43 having been published within the last 5 years (2018–2023). The studies were conducted in 12 countries, predominantly high-income (n = 17) and upper-middle-income (n = 16) countries. Only 2 studies were conducted in low-income countries. The income levels of countries were based on the World Bank classification (World Bank Group, 2024). The four countries with the highest number of studies were the United States (n = 12), Iran (n = 12), and China (n = 11). The geographical distribution of the number of publications for each country is depicted in Figure 2 and detailed in Supplementary Appendix Table S2.
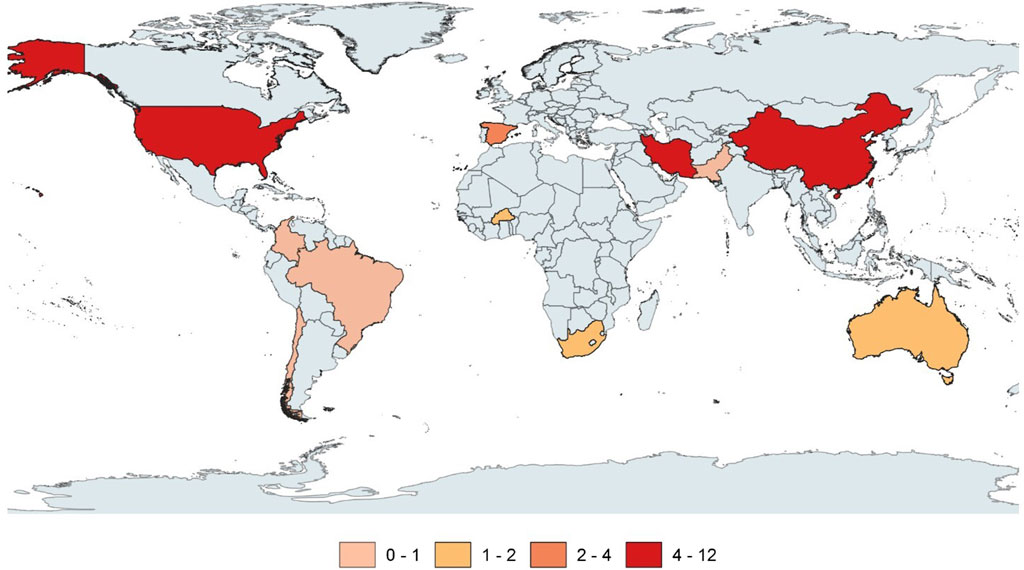
Figure 2. Geographical distribution of publications by country (2023, Brazil). (A) Thematic categories. (B) Climate variability. (C) Atmospheric pollution. (D) Natural disasters.
A variety of study designs were identified, including time series (n = 14), retrospective (n = 7), systematic reviews (n = 7), narrative reviews (n = 6), ecological (n = 5), literature reviews (n = 4), clinical studies (n = 3), cross-sectional (n = 2), longitudinal (n = 2), cohort (n = 1), cross-sectional case-control (n = 1), regression analysis (n = 1), and report (n = 1). Some studies were categorized by researchers as quantitative (n = 19) and qualitative (n = 4) without specification of study design (Supplementary Appendix Table S3). The studies were retrieved from databases and portals including PubMed/Medline (n = 28), Scopus (n = 24), EBSCO (n = 17), Scielo (n = 2), BVS (n = 1), Embase (n = 1), and Institute of Electric and Electronic Engineers (n = 1) (Supplementary Appendix Table S4; Supplementary Appendix Figure S1).
The cardiovascular diseases identified included acute myocardial infarction (AMI) (n = 20), stroke (n = 13), systemic arterial hypertension (SAH) (n = 8), and heart failure (HF) (n = 3). In addition, diabetes mellitus was identified (n = 12) (Supplementary Appendix Table S5). The most vulnerable populations for CVD and diabetes mellitus in the dry regions were the older adults (n = 34), women (n = 9), and children aged 0–5 years (n = 5). Among the most affected were older adults aged 65–94 years with arterial hypertension (n = 3) (Supplementary Appendix Tables S6, S7; Supplementary Appendix Figure S2).
In this research, three central thematic categories were developed from data analysis: climate variability, atmospheric pollution, and natural disasters (Figure 3 and Supplementary Appendix Tables S8–S11). These categories are interconnected in influencing the development of cardiovascular diseases and the exacerbation of diabetes mellitus in dry regions, as we will discuss below.
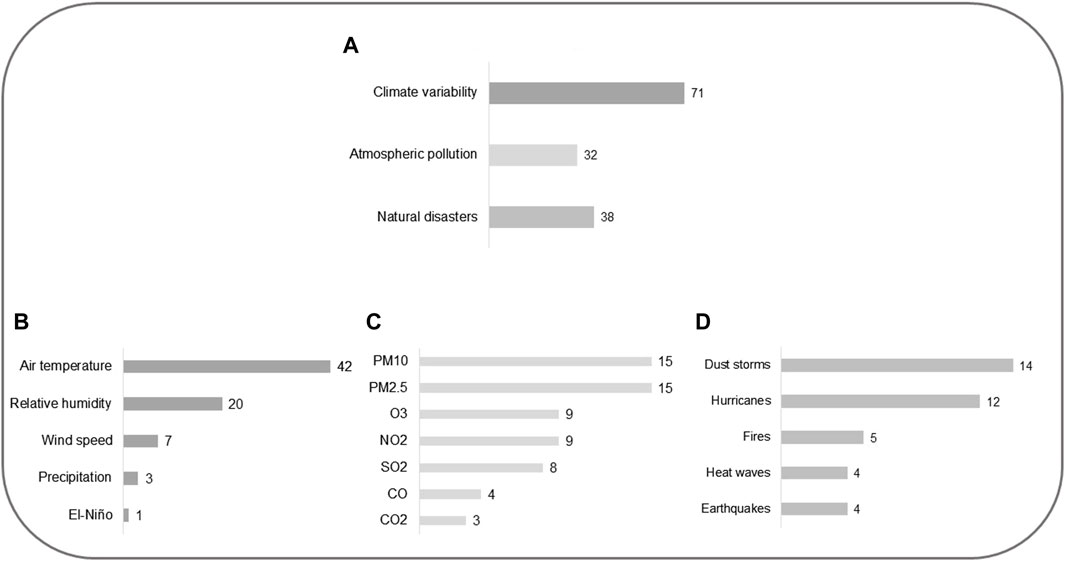
Figure 3. Central thematic categories emerging from data analysis: climate variability, atmospheric pollution, and natural disasters (2023, Brazil).
The variation of climate variables (precipitation, air temperature, air humidity, and wind speed) and El Niño were understood as part of the climate variability category (n = 71). Within this category, studies were distributed as follows: air temperature (n = 42), relative air humidity (n = 20), wind speed (n = 7), precipitation (n = 3), and El Niño (n = 1). Additionally, 22 studies mentioned climate variability, but did not specify the variable or phenomenon itself. In the atmospheric pollution category (n = 32), pollution by particulate matter (PM10, PM2.5), O3, NO2, SO2, CO, and CO2 were included. Studies focused on each pollutant were distributed as follows: PM10 (n = 15), PM2.5 (n = 15), O3 (n = 9), NO2 (n = 9), SO2 (n = 8), CO (n = 4), and CO2 (n = 3). Extreme natural events, whether climatic or not, were categorized as natural disasters (earthquake, hurricane, fire, heatwaves, and dust storms). Studies in the natural disasters category (n = 38) were distributed as follows: earthquake (n = 4), hurricane (n = 12), dust storms (n = 14), fire (n = 5), and heatwaves (n = 4). Some studies mentioned more than one climate variable, pollutant, and/or natural disaster, as detailed in Supplementary Appendix Tables S9–S11.
In studies focusing on the influence of climatic components, it was observed that high precipitation was associated with more cases of CVD [37]. Air temperature significantly above or below historical averages is linked to increased CVD mortality [38]. The extreme heat characteristic of drought episodes is considered an important risk factor related to CVD [39]. Heatwaves are a causative factor of stress and exhaustion, posing risks to individuals with CVD [40]. Conversely, extreme decreases in temperature compared to historical averages can also lead to cardiovascular problems such as AMI and stroke [41].
The rise in air temperature, decrease in relative air humidity, and increase in wind speed can exacerbate the harmful effects of air pollutants on cardiovascular health. Increased temperature influences the concentration of air pollutants such as SO2, O3, NO2, PM10, and PM2.5 [42].
Dust storms, characterized by strong winds, elevate the concentration of air pollutants of natural or anthropogenic origin, such as SO2, O3, NO2, PM10, and PM2.5 [41–43]. These pollutants, along with CO2, have been associated with the formation of atherosclerotic plaques, leading to blood vessel obstruction [44].
Studies indicate that days with low relative air humidity have higher levels of air pollutants [45]. Additionally, dust storms also occur during periods of low relative air humidity, leading to increased hospital admissions for CVD [46].
The influence of the El Niño phenomenon on cardiovascular diseases is noteworthy. Meteorological droughts caused by El Niño in certain regions of the planet can intensify the risk of forest fires. These fires, in turn, emit gases and increase the concentration of air pollutants. Thus, a higher number of deaths and hospital admissions due to stroke are associated with El Niño occurrences [47].
The main effects mentioned in studies relating climatic variables, atmospheric pollution, and natural disasters to the development of CVD are summarized in Figures 4, 5.
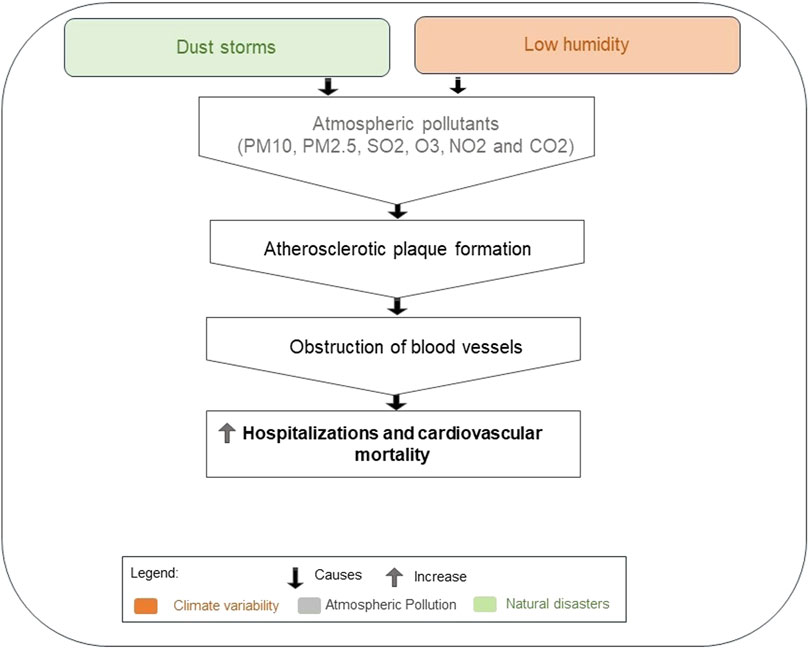
Figure 4. Effect of climate variables, atmospheric pollution, and natural disasters on increased hospitalizations and cardiovascular mortality (2023, Brazil).
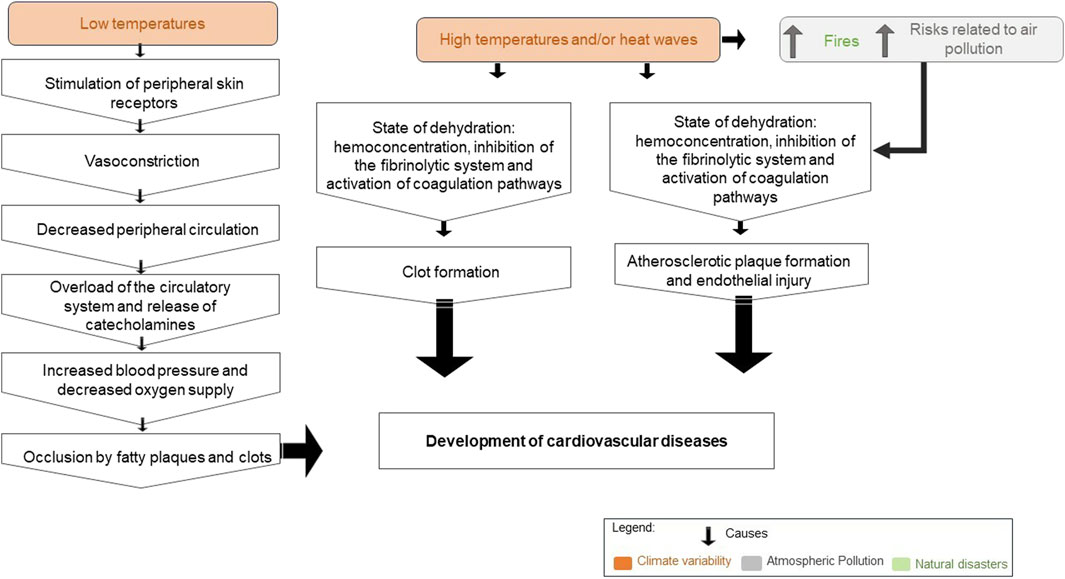
Figure 5. Effect of climate variables, atmospheric pollution, and natural disasters on the development of cardiovascular diseases (2023, Brazil).
Natural disasters such as heatwaves, dust storms, and wildfires are risk factors and have a direct impact on the development of cardiovascular diseases, as discussed above. However, there are disasters like earthquakes and hurricanes that have an indirect impact (Supplementary Appendix Table S11). Exposure to these disasters (earthquakes and hurricanes) contributes to exacerbating the effect of other risk factors in people with CVD and DM, such as: stress (n = 3), inadequate diet (n = 2), socioeconomic vulnerability (n = 4); medication unavailability, non-adherence, and treatment interruption (n = 3); increased smoking (n = 3); unstable blood sugar levels (n = 2); increased alcohol consumption (n = 2); and difficulty accessing healthcare services (n = 2), as shown in Supplementary Appendix Figure S3. These risk factors are further explored in Supplementary Appendix Table S12 and Supplementary Appendix S2.
Due to disasters such as earthquakes or hurricanes, individuals residing in affected areas need to relocate to refuge locations. In this process, many people are unable to bring the necessary medications for the treatment of chronic diseases such as diabetes mellitus and hypertension, discontinuing treatment [48], which can lead to alterations in blood glucose and/or blood pressure levels. Additionally, the food offered in shelters is often restricted and inadequate for people with CVD and DM, posing another risk factor for individuals to experience episodes of hyperglycemia, severe hypoglycemia, or hypertensive crises [49].
Discussion
This scoping review allowed us to map the influence of variations in climatic variables (precipitation, air temperature, air humidity, and wind speed), El Niño, atmospheric pollution (PM10, PM2.5, CO2, O3, SO2, and NO2), and natural disasters (earthquake, hurricane, fire, heatwaves, and dust storms) on cardiovascular diseases and diabetes mellitus in dry regions. The most frequent diseases addressed in the studies were AMI and stroke. Exposure to extreme temperatures and atmospheric pollutants were the main risk factors with direct impacts on CVD, while exposure to natural disasters was an important risk factor for amplifying other known risk factors (inadequate diet, alcohol consumption, smoking, and stress), thus considered a risk factor with indirect impact on CVD and DM.
When analyzing the category of climatic variability, one of the studies included in this review related increased precipitation to increased CVD [37]. Similarly, an ecological study conducted in China identified an increase in hospitalizations due to ischemic stroke associated with increased precipitation, especially in men and older adults (>65 years) [50]. Other researchers observed in a cohort study a higher risk of incidence of stroke (ischemic and hemorrhagic) when rainfall was higher [51].
Additionally, the risk of stroke may increase when precipitation is associated with other climatic variables such as air humidity, as in environments with very high precipitation and higher humidity, the body’s decreased ability to sweat and the blockage of chloride and sodium discharge can lead to stroke [52]. On the other hand, low precipitation is observed in dry periods [53] and has been considered a risk factor for CVD, such as stroke [39]. In summary, it is known that extremes of high or low precipitation can increase the risk of stroke, even though there is no consensus in the literature on the type of stroke.
Regarding temperature variations, it was observed that, isolated or associated with other climatic variables, it was the one that most influenced the development or worsening of CVD. In the studies, we observed that the increase or decrease in temperature reference values was associated with CVD in the region where each study was conducted, with the association between increased temperature and heatwave being more frequent with the worsening or development of any cardiovascular disease [40].
In China, on days when heatwaves were present, there was an increased risk of various CVDs: chronic ischemic heart disease (32.2%), acute (27.3%), cerebrovascular disease (26.7%), and myocardial infarction (25.2%) [54]. According to the literature, the main pathophysiological mechanisms that can explain the relationship between increased temperature and CVD are dehydration, hemoconcentration, hypercoagulable state, and electrolyte disturbances [55]. Moreover, the formation of clots from hypercoagulation can result in acute coronary events or stroke [26]. We found in this research that heat stress and exhaustion resulting from heatwaves generated by the rise in temperature can pose risks for people with CVD [40]. According to Coates et al. [56], heatwaves already cause more deaths than all other natural disasters combined.
Similar to our research, other studies have also linked decreases in temperature to an increased incidence of myocardial infarction [57] and stroke [58]. The impact of low temperatures on these cardiovascular events may be connected to vasoconstriction—a natural response of the human body to cold. Vasoconstriction aims to reduce heat loss by narrowing blood vessels. However, this narrowing can raise the risk of myocardial infarction by reducing peripheral blood circulation. Additionally, it may promote the occlusion of arteries due to fat plaques and blood clots. Furthermore, cold temperatures can lead to elevated blood pressure and decreased oxygen supply [59, 60], further contributing to cardiovascular risks.
In addition to the isolated influence of climate variability on CVD, some of the studies included in this review also highlighted the effects of these climatic variables on the concentration of air pollutants in the development of CVD. A higher concentration of air pollutants was observed during periods of low air humidity in dry seasons, contributing to increased cardiovascular hospitalizations and mortality [46]. Also, low humidity, combined with the high temperatures typical of dry seasons, provides favorable conditions for dust storms [61] and fires [62]. During dust storms, hot air masses can intensively concentrate local pollutants [63], besides favoring the transport and condensation of gaseous pollutants such as SO2 [64].
Just like dust storms, temperature variation, and heatwaves influence the increase in concentration of air pollutants harmful to cardiovascular health, such as greenhouse gases [42], which can accentuate CVD mortality. Particulate matter along with CO2 has been associated with the formation of atherosclerotic plaques, stemming from blood hypercoagulability due to endothelial dysfunction [44], exposing individuals to the risk of myocardial infarction and heart failure [39, 41].
The pathophysiological mechanisms by which exposure to air pollution negatively affects cardiovascular diseases are not yet fully understood; however, studies have highlighted possible explanations such as systemic inflammatory response [28], oxidative stress [65], genetic and epigenetic factors, impact on the central nervous system and autonomic dysfunction, as well as prothrombotic response, vascular dysfunction, and remodeling [66].
The last category presented in this study was that of natural disasters, being the only one where studies directed at people with DM were identified. Natural disasters, such as hurricanes [49] and earthquakes [48, 67], can be risk factors that cause indirect impacts, as they lead to the development or intensification of other risk factors, such as behavioral factors (tobacco and alcohol use, sedentary lifestyle, among others) and/or hypertension, which can trigger and/or exacerbate cardiovascular problems and diabetes mellitus.
After a disaster situation, a person may experience a hypertensive crisis due to sudden stress. Also, a gradual increase in blood pressure values is common due to the immediate and unplanned need for lifestyle changes, such as inadequate meals leading to weight gain, and the possibility of increased alcohol consumption. This finding is supported by a study conducted in the city of Fukushima, Japan, on the evacuation experience of individuals after a hurricane, which found an increase in blood pressure among these individuals [68]. After a disaster, in addition to changes in blood pressure values, alterations in HbA1c levels in people with DM are common, increasing the risk of hospitalizations [69].
Dietary habits may change after a natural disaster, for example, individuals in temporary shelters are restricted to the meals provided there [49, 67, 70]. Another influencing factor may be the distance from supermarkets and fast-food outlets when individuals are relocated to areas farther away from these establishments [71], reducing their opportunities to obtain the foods that were part of their diet.
Changes in dietary patterns can also occur due to mental illness, such as symptoms of post-traumatic stress disorder (PTSD) and depression [72], thereby increasing the risk of CVD and DM. The occurrence of late-onset post-traumatic stress disorder among survivors of natural disasters may be associated with impaired self-control [73]. A study conducted in Japan after the major earthquake and tsunami in 2011 suggested that the increased risks of cardiometabolic diseases may result from changes in diet associated with PTSD and depression. There was an association between reduced healthy eating patterns and depressive and/or PTSD symptoms, leading to increased unhealthy eating habits such as higher consumption of processed foods rich in carbohydrates and proteins, reduced intake of fruits and vegetables, and increased alcohol consumption, especially among males [74].
The likelihood of using toxic substances among survivors of natural disasters was also identified in our study. The main concerns of survivors were directed towards potential family or material losses, which can lead individuals to high levels of physical and emotional stress [49, 67, 75], favoring increased cigarette smoking [38, 70, 75] or alcohol consumption [38]. This finding may be associated with psychological distress resulting from decreased self-efficacy perception in coping, leading to increased substance use post-natural disaster [76]. Alcohol use as a temporary relief for stress is also common [77].
Other conditions reported in studies and related to increased hospitalization or mortality from CVD or DM in individuals affected by natural disasters include interruption of routine healthcare services [78] and lack of access to medications and treatments [48, 49, 67, 79] due to increased difficulty in accessing services [70]. All of this may be related to difficulty in self-managing some chronic diseases post-natural disaster [80].
The destruction of facilities, infrastructure, and significant changes in living conditions caused by natural disasters can increase difficulty, especially in older people, in maintaining healthy practices [77]. In addition to causing the destruction of health facilities, natural disasters can also reduce the number of professionals and interfere with the quality and effectiveness of health services provided [81, 82]. Furthermore, in circumstances of natural disaster, health actions often focus on patients with acute conditions such as trauma or infectious diseases, even though inadequate control of chronic diseases is considered a major threat to people’s health [82].
The most vulnerable groups identified in this review are similar to other research, with a focus on older adults, women, and children, who are most affected by climate influence [83]. This association may occur due to the greater susceptibility of older adults to retain more heat when exposed to hot and dry conditions than younger individuals [84]. The presence of comorbidities, such as hypertension, may further increase this vulnerability of older adults to heat exposure [85].
Women were also indicated in the studies as one of the vulnerable groups. This result may be associated with the progression of atherosclerotic disease. In women, the progression of atheroma plaques is slower but more severe [86] and may be exacerbated by climate change. Children were also considered vulnerable in the analyzed studies. This relationship may be related to the physiological development of children being different from adults. Furthermore, it is worth noting that children are exposed to long-term extreme weather events [87], as recent studies indicate that children born in 2020 will be more exposed to heatwaves (7 times more) and wildfires (2 times more) than previous generations in recent decades [88].
Exposure to climatic variability, pollution, and natural disasters in drylands is linked to cardiovascular diseases. Natural disasters also indirectly worsen diabetes mellitus. Vulnerability is particularly pronounced among older adults, women, and children. These factors often interact rather than act independently, highlighting the importance of nations adhering to Paris Agreement targets to decrease air pollutants and enhance resilience against disasters. Further research is imperative for tailored health interventions, necessitating interdisciplinary teams to alleviate the health impacts of climate, pollution, and disasters on these conditions.
Study Limitations
The study has limitations due to variability in population size and composition across the studies analyzed. Moreover, factors like public policies (such as early warning systems or green spaces) and socioeconomic status (income) could influence the results but were not addressed in this study.
Author Contributions
RM and AC contributed with conceptualization, formal analysis, funding acquisition, investigation, supervision, and writing. CdS contributed with conceptualization, formal analysis, investigation, and writing. TdS and FL contributed with formal analysis, investigation, and writing. HM and AdO contributed with formal analysis, visualization, and writing. GD-C, MG, and TC contributed with conceptualization, formal analysis, visualization, and writing. All authors contributed to the article and approved the submitted version.
Funding
The authors declare that financial support was received for the research, authorship, and/or publication of this article. This work was funded by the Brazilian National Council for Scientific and Technological Development (Universal Grant 18/2021—Band A—Emerging groups—process no. 402514/2021-1), by the Brazilian National Council for Scientific and Technological Development (Universal Grant 10/2023, process no. 403732/2023-9), by the Cearense Foundation for Support to Scientific and Technological Development (Funcap/Brazil, 18/2020—Strategic Partnerships in the States), and by the CAPES Foundation/Brazilian Ministry of Education (Grant no. 216/2018).
Conflict of Interest
The authors declare that they do not have any conflicts of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.ssph-journal.org/articles/10.3389/phrs.2024.1607300/full#supplementary-material
References
1. Intergovernmental Panel on Climate Change (IPCC). Climate Change 2021: The Physical Science Basis - Contribution of Working Group I to the Sixth Assessment Report of the Intergovernmental Panel on Climate Change. Cambridge: Cambridge University Press (2021).
2. United Nations. What Are Climate Changes? Brazil: United Nations (2022). Available from: https://brasil.un.org/pt-br/175180-o-que-s%C3%A3o-mudan%C3%A7as-clim%C3%A1ticas (Accessed December 15, 2023).
3. Souza, A, Abreu, MC, and Oliveira-Júnior, JF. Impact of Climate Change on Human Infectious Diseases: Dengue. Braz Arch Biol Technol (2021) 64:e21190502. doi:10.1590/1678-4324-2021190502
4. Bonomo, S, Marchetti, P, Fasola, S, Vesentini, R, Marcon, A, Ferrante, G, et al. Asthma Incidence Can Be Influenced by Climate Change in Italy: Findings From the GEIRD Study—A Climatological and Epidemiological Assessment. Sci Rep (2023) 13:19047. doi:10.1038/s41598-023-46423-2
5. United Nations. Climate Change: Key Facts (2023). Available from: https://bit.ly/49zDwNs (Accessed December 15, 2023).
6. Zilbermint, M. Diabetes and Climate Change. J Community Hosp Intern Med Perspect (2020) 10:10409–412. doi:10.1080/20009666.2020.1791027
7. Moreira, RP, Costa, AC, Gomes, TF, and Ferreira, GO. Climate and Climate-Sensitive Diseases in Semi-Arid Regions: A Systematic Review. Int J Public Health (2020) 65:1749–61. doi:10.1007/s00038-020-01464-6
8. Al-Shihabi, F, Moore, A, and Chowdhury, TA. Diabetes and Climate Change. Diabet Med (2023) 40:e14971. doi:10.1111/dme.14971
9. Breitner-Busch, S, Mücke, HG, Schneider, A, and Hertig, E. Impact of Climate Change on Non-Communicable Diseases Due to Increased Ambient Air Pollution. J Health Monit (2023) 8:103–21. doi:10.25646/11655
10. Scholes, RJ. The Future of Semi-Arid Regions: A Weak Fabric Unravels. Climate (2020) 8:43. doi:10.3390/cli8030043
11. Yao, J, Liu, H, Huang, J, Gao, Z, Wang, G, Li, D, et al. Accelerated Dryland Expansion Regulates Future Variability in Dryland Gross Primary Production. Nat Commun (2020) 11(1):1665. doi:10.1038/s41467-020-15515-2
12. Spinoni, J, Barbosa, P, Cherlet, M, Forzieri, G, McCormick, N, Naumann, G, et al. How Will the Progressive Global Increase of Arid Areas Affect Population and Land-Use in the 21st Century? Glob Planet Change (2021) 205:103597. doi:10.1016/j.gloplacha.2021.103597
13. Naciones Unidas Convención de Lucha contra la Desertificación (UNCCD). Perspectiva Global de la tierra. Bonn: UNCCD (2017).
14. Furtak, K, and Wolinska, A. The Impact of Extreme Weather Events as a Consequence of Climate Change on the Soil Moisture and on the Quality of the Soil Environment and Agriculture – A Review. Catena (2023) 231:107378. doi:10.1016/j.catena.2023.107378
15. World Meteorological Organization (WMO). Sand and Dust Storms (2022). Available from: https://public-old.wmo.int/en/our-mandate/focus-areas/environment/sand-and-dust-storms (Accessed December 15, 2023).
16. Guo, Y, Gasparrini, A, Armstrong, BG, Tawasupa, B, Tobias, A, Lavigne, E, et al. Heat Wave and Mortality: A Multicountry, Multicommunity Study. Environ Health Perspect (2017) 125(8):087006. doi:10.1289/EHP1026
17. Middleton, NJ, and Sternberg, T. Climate Hazards in Drylands: A Review. Earth Sci Rev (2013) 126:48–57. doi:10.1016/j.earscirev.2013.07.008
18. Greve, P, Orlowsky, B, Mueller, B, Sheffield, J, Reichstein, M, and Seneviratne, SI. Global Assessment of Trends in Wetting and Drying Over Land. Nat Geosci (2014) 7:716–21. doi:10.1038/ngeo2247
19. Raymond, C, Horton, RM, Zscheischler, J, Martius, O, AghaKouchak, A, Balch, J, et al. Understanding and Managing Connected Extreme Events. Nat Clim Chang (2020) 10:611–21. doi:10.1038/s41558-020-0790-4
20. World Health Organization (WHO). Environment, Climate Change and Health (2024). Available from: https://www.who.int/teams/environment-climate-change-and-health/emergencies (Accessed December 15, 2023).
21. Mirzabaev, A, Wu, J, Evans, J, García-Oliva, F, Hussein, IAG, Iqbal, MM, et al. Desertification. In: M Delmotte, P Zhai, HO Pörtner, D Roberts, J Skea, and EC Buendia, editors Climate Change and Land: An IPCC Special Report on Climate Change, Desertification, Land Degradation, Sustainable Land Management, Food Security, and Greenhouse Gas Fluxes in Terrestrial Ecosystems. Cambridge: Intergovernmental Panel on Climate Change (2019).
22. Mbow, C, Rosenzweig, C, Barioni, LG, Benton, TG, Herrero, M, Krishnapillai, M, et al. Food Security. In: M Delmotte, P Zhai, HO Pörtner, D Roberts, J Skea, and EC Buendia, editors. Climate Change and Land: An IPCC Special Report on Climate Change, Desertification, Land Degradation, Sustainable Land Management, Food Security, and Greenhouse Gas Fluxes in Terrestrial Ecosystems. Cambridge: Intergovernmental Panel on Climate Change (2019).
23. Frumkin, H, Das, MB, Negev, M, Rogers, BC, Bertollini, R, Dora, C, et al. Protecting Health in Dry Cities: Considerations for Policy Makers. BMJ (2020) 371:m2936. doi:10.1136/bmj.m2936
24. Vaičiulis, V, Venclovienė, J, Kačienė, G, Tamošiūnas, A, Kiznys, D, Lukšienė, D, et al. Association Between El Niño-Southern Oscillation Events and Stroke: A Case-Crossover Study in Kaunas City, Lithuania, 2000–2015. Int J Biometeorol (2022) 66:769–79. doi:10.1007/s00484-021-02235-5
25. Vallianou, NG, Geladari, EV, Kounatidis, D, Geladari, CV, Stratigou, T, Durakis, SP, et al. Diabetes Mellitus in the Era of Climate Change. Diabetes Metab (2021) 47(4):101205. doi:10.1016/j.diabet.2020.10.003
26. Desai, Y, Khraishah, H, and Alahmad, B. Heat and the Heart. Yale J Biol Med (2023) 96(2):197–203. doi:10.59249/HGAL4894
27. Li, Y, Xu, L, Shan, Z, Teng, W, and Han, C. Association Between Air Pollution and Type 2 Diabetes: An Updated Review of the Literature. Ther Adv Endocrinol Metab (2019) 10:2042018819897046. doi:10.1177/2042018819897046
28. Rajagopalan, S, Al-Kindi, SG, and Brook, RD. Air Pollution and Cardiovascular Disease: JACC State-Of-The-Art Review. J Am Coll Cardiol (2018) 72(17):2054–70. doi:10.1016/j.jacc.2018.07.099
29. World Health Organization (WHO). Cardiovascular Diseases (2021). Available from: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds (Accessed December 15, 2023).
30. American Heart Association. Diabetes Risks Factors (2021). Available from: https://www.heart.org/en/health-topics/diabetes/understand-your-risk-for-diabetes (Accessed December 15, 2023).
31. Pan American Health Organization (PAHO). WHO Reveals Main Causes of Death and Disability Worldwide Between 2000 and 2019 (2020). Available from: https://bit.ly/49m25he (Accessed February 18, 2024).
32. International Research Institute for Climate and Society. Climate Variability (2023). Available from: https://iri.columbia.edu/our-expertise/climate/climate-variability/ (Accessed December 15, 2023).
33. U.S. Department of Homeland Security. Natural Disasters (2023). Available from: https://www.dhs.gov/natural-disasters (Accessed December 15, 2023).
34. Andela, N, Liu, YY, van Dijk, AIJM, de Jeu, RAM, and McVicar, TR. Global Changes in Dryland Vegetation Dynamics (1988–2008) Assessed by Satellite Remote Sensing: Comparing a New Passive Microwave Vegetation Density Record With Reflective Greenness Data. Biogeosciences (2023) 10:6657–76. doi:10.5194/bg-10-6657-2013
35. Peters, MDJ, Marnie, C, Tricco, AC, Pollock, D, Munn, Z, Alexander, L, et al. Updated Methodological Guidance for the Conduct of Scoping Reviews. JBI Evid Synth (2020) 18(10):2119–26. doi:10.11124/JBIES-20-00167
36. Braun, V, and Clarke, V. Using Thematic Analysis in Psychology. Qual Res Psychol (2006) 3(2):77–101. doi:10.1191/1478088706qp063oa
37. Malik, SM, Awan, H, and Khan, N. Mapping Vulnerability to Climate Change and Its Repercussions on Human Health in Pakistan. Glob Health (2012) 8:31. doi:10.1186/1744-8603-8-31
38. Huang, KS, He, DX, Huang, DJ, Tao, QL, Deng, XJ, Zhang, B, et al. Changes in Ischemic Heart Disease Mortality at the Global Level and Their Associations With Natural Disasters: A 28-Year Ecological Trend Study in 193 Countries. PLoS One (2021) 16(7):e0254459. doi:10.1371/journal.pone.0254459
39. Weilnhammer, V, Schmid, J, Mittermeier, I, Schreiber, F, Jiang, L, Pastuhovic, V, et al. Extreme Weather Events in Europe and Their Health Consequences - A Systematic Review. Int J Hyg Environ Health (2021) 233:113688. doi:10.1016/j.ijheh.2021.113688
40. Rocque, RJ, Beaudoin, C, Ndjaboue, R, Cameron, L, Poirier-Bergeron, L, Poulin-Rheault, RA, et al. Health Effects of Climate Change: An Overview of Systematic Reviews. BMJ Open (2021) 11(6):e046333. doi:10.1136/bmjopen-2020-046333
41. Khraishah, H, Alahmad, B, Ostergard, RL, AlAshqar, A, Albaghdadi, M, Vellanki, N, et al. Climate Change and Cardiovascular Disease: Implications for Global Health. Nat Rev Cardiol (2022) 19(12):798–812. doi:10.1038/s41569-022-00720-x
42. Aghababaeian, H, Ostadtaghizadeh, A, Ardalan, A, Asgary, A, Akbary, M, Yekaninejad, MS, et al. Global Health Impacts of Dust Storms: A Systematic Review. Environ Health Insights (2021) 15:11786302211018390. doi:10.1177/11786302211018390
43. Kinay, P, Morse, AP, Villanueva, EV, Morrissey, K, and Staddon, PL. Direct and Indirect Health Impacts of Climate Change on the Vulnerable Elderly Population in East China. Environ Rev (2019) 27:295–303. doi:10.1139/er-2017-0095
44. Sandoval, DB, Rettig, MD, Reyes, RT, and Oyarzún, GM. Impacto de la contaminación aérea por incendios forestales en la morbimortalidad de la población expuesta. Neumología Pediátrica (2021) 16(4):167–71.
45. Crooks, JL, Cascio, WE, Percy, MS, Reyes, J, Neas, LM, and Hilborn, ED. The Association Between Dust Storms and Daily Non-Accidental Mortality in the United States, 1993-2005. Environ Health Perspect (2016) 124(11):1735–43. doi:10.1289/EHP216
46. Yang, CY, Chen, YS, Chiu, HF, and Goggins, WB. Effects of Asian Dust Storm Events on Daily Stroke Admissions in Taipei, Taiwan. Environ Res (2005) 99(1):79–84. doi:10.1016/j.envres.2004.12.009
47. Marlier, ME, DeFries, RS, Voulgarakis, A, Kinney, PL, Randerson, JT, Shindell, DT, et al. El Niño and Health Risks From Landscape Fire Emissions in Southeast Asia. Nat Clim Chang (2013) 3:131–6. doi:10.1038/nclimate1658
48. Gohardehi, F, Seyedin, H, and Moslehi, S. Prevalence Rate of Diabetes and Hypertension in Disaster-Exposed Populations: A Systematic Review and Meta-Analysis. Ethiop J Health Sci (2020) 30(3):439–48. doi:10.4314/ejhs.v30i3.15
49. Cefalu, WT, Smith, SR, Blonde, L, and Fonseca, V. The Hurricane Katrina Aftermath and Its Impact on Diabetes Care: Observations From “Ground Zero”: Lessons in Disaster Preparedness of People With Diabetes. Diabetes Care (2006) 29(1):158–60. doi:10.2337/diacare.29.1.158
50. Tang, C, Liu, X, He, Y, Gao, J, Xu, Z, Duan, J, et al. Association Between Extreme Precipitation and Ischemic Stroke in Hefei, China: Hospitalization Risk and Disease Burden. Sci Total Environ (2020) 732:139272. doi:10.1016/j.scitotenv.2020.139272
51. Matsumoto, M, Ishikawa, S, and Kajii, E. Cumulative Effects of Weather on Stroke Incidence: A Multi-Community Cohort Study in Japan. J Epidemiol (2010) 20(2):136–42. doi:10.2188/jea.je20090103
52. Cho, GJ, Ahn, KH, Kim, LY, Hwang, SY, Hong, SC, Oh, MJ, et al. Effect of Relative Humidity on Preeclampsia. Clin Exp Obstet Gynecol (2017) 44(2):264–7. doi:10.12891/ceog3462.2017
53. World Health Organization. Drought (2023). Available from: https://bit.ly/3I3aObZ (Accessed December 15, 2023).
54. Yan, M, Xie, Y, Zhu, H, Ban, J, Gong, J, and Li, T. Cardiovascular Mortality Risks During the 2017 Exceptional Heatwaves in China. Environ Int (2023) 172:107767. doi:10.1016/j.envint.2023.107767
55. Stewart, S, Keates, AK, Redfern, A, and McMurray, JJ. Seasonal Variations in Cardiovascular Disease. Nat Rev Cardiol (2017) 14(11):654–64. doi:10.1038/nrcardio.2017.76
56. Coates, L, Haynes, K, O’brien, J, McAneney, J, and Oliveira, FD. Exploring 167 Years of Vulnerability: An Examination of Extreme Heat Events in Australia 1844–2010. Environ Sci Pol (2014) 42:33–44. doi:10.1016/j.envsci.2014.05.003
57. Silva, GAP, and Kock, KS. Effect of Seasonality in Hospitalizations and Deaths From Acute Myocardial Infarction in Southern Brazil From 2009 to 2018. Am J Cardiovasc Dis (2021) 11(1):148–54.
58. Bai, L, Li, Q, Wang, J, Lavigne, E, Gasparrini, A, Copes, R, et al. Increased Coronary Heart Disease and Stroke Hospitalisations From Ambient Temperatures in Ontario. Heart (2018) 104(8):673–9. doi:10.1136/heartjnl-2017-311821
59. Honda, T, Fujimoto, K, and Miyao, Y. Influence of Weather Conditions on the Frequent Onset of Acute Myocardial Infarction. J Cardiol (2016) 67(1):42–50. doi:10.1016/j.jjcc.2015.02.013
60. Fares, A. Winter Cardiovascular Diseases Phenomenon. N Am J Med Sci (2013) 5(4):266–79. doi:10.4103/1947-2714.110430
61. Wehner, MF, Arnold, JR, Knutson, T, Kunkel, KE, and LeGrande, NA. Droughts, Floods, and Wildfires. In: DJ Wuebbles, DW Fahey, KA Hibbard, DJ Dokken, BC Stewart, and TK Maycock, editors Climate Science Special Report: Fourth National Climate Assessment. Washington: U.S. Global Change Research Program (2017). p. 231–56.
62. Smith, LT, Aragão, LEOC, Sabel, CE, and Nakaya, T. Drought Impacts on Children’s Respiratory Health in the Brazilian Amazon. Sci Rep (2014) 4:3726. doi:10.1038/srep03726
63. Pandolfi, M, Tobias, A, Alastuey, A, Sunyer, J, Schwartz, J, Lorente, J, et al. Effect of Atmospheric Mixing Layer Depth Variations on Urban Air Quality and Daily Mortality During Saharan Dust Outbreaks. Sci Total Environ (2014) 494-495:283–9. doi:10.1016/j.scitotenv.2014.07.004
64. Bertheau, AMR, Varona, MM, Rodríguez, IM, Hernández, HF, and Armenteros, TG. Desarrollo tecnológico, impacto sobre el medio ambiente y la salud. Rev Cubana Hig Epidemiol (2011) 49:308–19.
65. Haberzettl, P, Conklin, DJ, Abplanalp, WT, Bhatnagar, A, and O’Toole, TE. Inhalation of Fine Particulate Matter Impairs Endothelial Progenitor Cell Function via Pulmonary Oxidative Stress. Arterioscler Thromb Vasc Biol (2018) 38(1):131–42. doi:10.1161/ATVBAHA.117.309971
66. Combes, A, and Franchineau, G. Fine Particle Environmental Pollution and Cardiovascular Diseases. Metabolism (2019) 100S:153944. doi:10.1016/j.metabol.2019.07.008
67. Miller, AC, and Arquilla, B. Chronic Diseases and Natural Hazards: Impact of Disasters on Diabetic, Renal, and Cardiac Patients. Prehosp Disaster Med (2008) 23(2):185–94. doi:10.1017/s1049023x00005835
68. Kobari, E, Tanaka, K, Nagao, M, Okazaki, K, Hayashi, F, Kazama, S, et al. Impact of Lifestyle and Psychosocial Factors on the Onset of Hypertension After the Great East Japan Earthquake: A 7-Year Follow-Up of the Fukushima Health Management Survey. Hypertens Res (2022) 45(10):1609–21. doi:10.1038/s41440-022-00968-3
69. Lee, DC, Gupta, VK, Carr, BG, Malik, S, Ferguson, B, Wall, SP, et al. Acute Post-Disaster Medical Needs of Patients With Diabetes: Emergency Department Use in New York City by Diabetic Adults After Hurricane Sandy. BMJ Open Diabetes Res Care (2016) 4(1):e000248. doi:10.1136/bmjdrc-2016-000248
70. Huang, KS, He, DX, Tao, Q, Wang, YY, Yang, YQ, Zhang, B, et al. Changes in the Incidence and Prevalence of Ischemic Stroke and Associations With Natural Disasters: An Ecological Study in 193 Countries. Sci Rep (2022) 12(1):1808. doi:10.1038/s41598-022-05288-7
71. Hikichi, H, Aida, J, Kondo, K, Tsuboya, T, and Kawashi, I. Residential Relocation and Obesity After a Natural Disaster: A Natural experiment From the 2011 Japan Earthquake and Tsunami. Sci Rep (2019) 9(1):374. doi:10.1038/s41598-018-36906-y
72. Hall, KS, Hoerster, KD, and Yancy, JWS. Post-Traumatic Stress Disorder, Physical Activity, and Eating Behaviors. Epidemiol Rev (2015) 37:103–15. doi:10.1093/epirev/mxu011
73. Walter, KH, Gunstad, J, and Hobfoll, SE. Self-Control Predicts Later Symptoms of Posttraumatic Stress Disorder. Psychol Trauma (2010) 2(2):97–101. doi:10.1037/a0018958
74. Yazawa, A, Shiba, K, Hikichi, H, Okuzono, SS, Aida, J, Kondo, K, et al. Post-Disaster Mental Health and Dietary Patterns Among Older Survivors of an Earthquake and Tsunami. J Nutr Health Aging (2023) 27(2):124–33. doi:10.1007/s12603-023-1887-z
75. Peters, MN, Moscona, JC, Katz, MJ, Deandrade, KB, Quevedo, HC, Tiwari, S, et al. Natural Disasters and Myocardial Infarction: The Six Years After Hurricane Katrina. Mayo Clin Proc (2014) 89(4):472–7. doi:10.1016/j.mayocp.2013.12.013
76. Alexander, AC, and Ward, KD. Understanding Postdisaster Substance Use and Psychological Distress Using Concepts From the Self-Medication Hypothesis and Social Cognitive Theory. J Psychoactive Drugs (2018) 50(2):177–86. doi:10.1080/02791072.2017.1397304
77. Shin, SH, and Ji, H. Health Risks of Natural Hazards and Resilience Resources: Evidence From a U. S. Nationwide Longitudinal Study. Soc Sci Med (2021) 281:114110. doi:10.1016/j.socscimed.2021.114110
78. Hua, CL, Thomas, KS, Peterson, LJ, Hyer, K, and Dosa, DM. Emergency Department Use Among Assisted Living Residents After Hurricane Irma. J Am Med Dir Assoc (2021) 22(4):918–22.e1. doi:10.1016/j.jamda.2020.10.010
79. Quast, T, Andel, R, and Sadhu, AR. Long-Term Effects of Disasters on Seniors With Diabetes: Evidence From Hurricanes Katrina and Rita. Diabetes Care (2019) 42(11):2090–7. doi:10.2337/dc19-0567
80. Ryan, B, Franklin, RC, Burkle, JFM, Aitken, P, Smith, E, Watt, K, et al. Identifying and Describing the Impact of Cyclone, Storm and Flood Related Disasters on Treatment Management, Care and Exacerbations of Non-Communicable Diseases and the Implications for Public Health. Plos Curr (2015)) 7:ecurrents.dis.62e9286d152de04799644dcca47d9288. doi:10.1371/currents.dis.62e9286d152de04799644dcca47d9288
81. Aoki, T, Takahashi, J, Fukumoto, Y, Yasuda, S, Ito, K, Miyata, S, et al. Effect of the Great East Japan Earthquake on Cardiovascular Diseases–Report From the 10 Hospitals in the Disaster Area. Circ J (2013) 77(2):490–3. doi:10.1253/circj.cj-12-1594
82. Moslehi, S, and Shirazi, FB. Challenges of Providing Health Services to Patients With Cardiovascular Diseases During Disasters in Iran: A Qualitative Study. J Educ Health Promot (2023) 12:25. doi:10.4103/jehp.jehp_548_22
83. Cianconi, P, Betrò, S, and Janiri, L. The Impact of Climate Change on Mental Health: A Systematic Descriptive Review. Front Psychiatry (2020) 11:74. doi:10.3389/fpsyt.2020.00074
84. Meade, RD, Notley, SR, Akerman, AP, McGarr, GW, Richards, BJ, McCourt, ER, et al. Physiological Responses to 9 Hours of Heat Exposure in Young and Older Adults: Part I - Body Temperature and Hemodynamic Regulation. J Appl Physiol (2023) 135(3):673–87. doi:10.1152/japplphysiol.00227.2023
85. Schlader, ZJ, Coleman, GL, Sackett, JR, Sarker, S, Chapman, CL, Hostler, D, et al. Behavioral Thermoregulation in Older Adults With Cardiovascular Co-Morbidities. Temperature (Austin) (2018) 5(1):70–85. doi:10.1080/23328940.2017.1379585
86. Maas, AH, and Appelman, YE. Gender Differences in Coronary Heart Disease. Neth Heart J (2010) 18(12):598–602. doi:10.1007/s12471-010-0841-y
87. Bunyavanich, S, Landrigan, CP, McMichael, AJ, and Epstein, PR. The Impact of Climate Change on Child Health. Ambul Pediatr (2003) 3(1):44–52. doi:10.1367/1539-4409(2003)003<0044:tiocco>2.0.co;2
88. Dunning, H. Children Will Face Huge Increases in Extreme Climate Events in Their Lifetimes. London, United Kingdom: Imperial College (2021). Available from: https://www.imperial.ac.uk/news/230618/children-will-face-huge-increases-extreme/ (Accessed December 15, 2023).
Keywords: climate change, atmospheric pollution, environmental resilience, cardiovascular diseases, diabetes mellitus
Citation: Moreira RP, da Silva CBC, de Sousa TC, Leitão FLBF, Morais HCC, de Oliveira ASS, Duarte-Clíments G, Gómez MBS, Cavalcante TF and Costa AC (2024) The Influence of Climate, Atmospheric Pollution, and Natural Disasters on Cardiovascular Diseases and Diabetes Mellitus in Drylands: A Scoping Review. Public Health Rev 45:1607300. doi: 10.3389/phrs.2024.1607300
Received: 20 March 2024; Accepted: 26 July 2024;
Published: 08 August 2024.
Edited by:
Katarzyna Czabanowska, Maastricht University, NetherlandsReviewed by:
Pratik Shingru, Independent Researcher, Boston, United StatesMahdiyeh Mohammadzadeh, Tehran University of Medical Sciences, Iran
Copyright © 2024 Moreira, da Silva, de Sousa, Leitão, Morais, de Oliveira, Duarte-Clíments, Gómez, Cavalcante and Costa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
PHR is edited by the Swiss School of Public Health (SSPH+) in a partnership with the Association of Schools of Public Health of the European Region (ASPHER)+
*Correspondence: Rafaella Pessoa Moreira, cmFmYWVsbGFwZXNzb2FAdW5pbGFiLmVkdS5icg==
This Review Article is part of the PHR Special Issue “Mitigating and Adapting to Climate Change: Evidence for Public Health”