 Vivian Hui
Vivian Hui Bohan Zhang1
Bohan Zhang1- 1School of Nursing, The Hong Kong Polytechnic University, Kowloon, Hong Kong SAR, China
- 2Health and Community Systems, School of Nursing, University of Pittsburgh, Pittsburgh, PA, United States
- 3School of Nursing, University of Lowa, Iowa City, IA, United States
- 4Health Sciences Library System, University of Pittsburgh, Pittsburgh, PA, United States
Objectives: The following scoping review aims to identify and map the existing evidence for HIT interventions among women with DV experiences in the United States. And provide guidance for future research, and facilitate clinical and technical applications for healthcare professionals.
Methods: Five databases, PubMed, EBSCOhost CINAHL, Ovid APA PsycINFO, Scopus and Google Scholar, were searched from date of inception to May 2023. Reviewers extracted classification of the intervention, descriptive details, and intervention outcomes, including physical safety, psychological, and technical outcomes, based on representations in the included studies.
Results: A total of 24 studies were included, identifying seven web-based interventions and four types of abuse. A total of five studies reported safety outcomes related to physical health. Three studies reported depression, anxiety, and post-traumatic stress disorder as psychological health outcomes. The effectiveness of technology interventions was assessed in eight studies.
Conclusion: Domestic violence is a major public health issue, and research has demonstrated the tremendous potential of health information technology, the use of which can support individuals, families, and communities of domestic violence survivors.
Introduction
Domestic violence (DV) is a significant yet frequently underreported public health concern that menaces individuals’ physical and mental wellbeing globally [1]. As defined by the United States (U.S.) Office on Violence against Women, DV encompasses a pattern of abusive behavior within any intimate relationship that one partner uses to sustain or maintain control over another partner [2]. An array of abuse that could happen within a household includes physical, psychological, sexual, and financial towards the children, elderly, or intimate partner [2]. One in three women encounters physical violence from an intimate partner every minute, resulting in approximately 10 million abuse survivors annually in the U.S. [3]. Moreover, DV exerts a significant financial burden with an estimated cost of $103,767 per female affected by intimate partner violence (IPV) [4].
Compared to men, women exhibit a significantly elevated vulnerability to experiencing DV in a lifetime [5]. Persistent experience of DV is associated with an array of detrimental effects on physical and mental health, including hypertension, diabetes [6], depression, anxiety, and post-traumatic stress disorder (PTSD) [7–9], AIDS/HIV infection [10], sleep disturbances [11], and suicide attempts [12]. Nevertheless, the profound impact of DV on women is often underestimated due to its intricate nature, the prevalence of revictimization, and intergenerational victimization [13].
Intervention studies are pivotal in empowering survivors to overcome their challenges and enhancing their physical and mental wellbeing. However, conducting studies involving women with DV experiences often encountered substantial challenges. Previous research highlighted the difficulties faced when approaching DV survivors in person due to societal stigma, shame, guilt, alienation, and judgment [14–16]. Traditional intervention methods such as focus group, one-to-one in-person interviews, and individual/group therapy require substantial time for participants’ recruitment and are susceptible to confidentiality issues among participants. Recently, health information technology (HIT) has been gaining traction in DV research, such as developing more precise and effective screening tools and improving the overall wellbeing for DV survivors. HIT refers to the utilization and application of information processing that includes both computer hardware and software, across the spectrum of data storing, retrieving, sharing, and using healthcare information, health-related data from both patients or healthcare providers, and knowledge for effective healthcare communication and decision-making in certain disease journey [17]. HIT interventions (e.g., guided online support) offer an anonymous environment that allows survivors to access information and seek help without the time and location constraints [18]. Women with DV experiences face additional vulnerabilities due to limited access to resources and the societal-asserted feminine duties on childcare and housework tasks. The use of HIT intervention allows these women to reach resources and seek help from the virtual space without restrictions. Also, studies indicated that women survivors tend to be more emotional and prefer text-based communication with healthcare providers as it provides them with a sense of anonymity and security [19].
With HIT accessible through mobile devices, women may easily acquire a wealth of health information and increase their likelihood of disclosing their abusive experience [20]. Studies also show the use of HIT interventions can improve health outcomes among the DV population. However, to the best of our knowledge, current reviews have only examined HIT interventions for mental health [21], child maltreatment [22], and peer aggression [23]. Although the application of HIT in the DV population has surged unprecedentedly, no evidence summarized the current state of the science of HIT interventions particularly in women with DV experiences.
As such, this scoping review aims to identify and map the available evidence for HIT interventions among women with DV experiences in the United States. This review can guide future research and advance the clinical and technological applications available to healthcare professionals.
Methods
Search Strategy
Four bibliographic databases were searched from date of inception to May 2023 (PubMed, EBSCOhost CINAHL, Ovid APA PsycINFO, Scopus). Initial searches were run in Oct 2018 and search updates were run in May 2023. Searches were also run in Google Scholar. To ensure comprehensive coverage, a health sciences librarian (blinded) designed the PubMed search strategy and then adapted that search strategy for use in other databases. The search strings utilized a combination of natural language and, where applicable, controlled vocabulary to cover the concepts of “technology” and “family or domestic violence.” In instances where possible, the search results were limited to articles published in the English language. The full list of search strings from different databases is shown in Table 1.
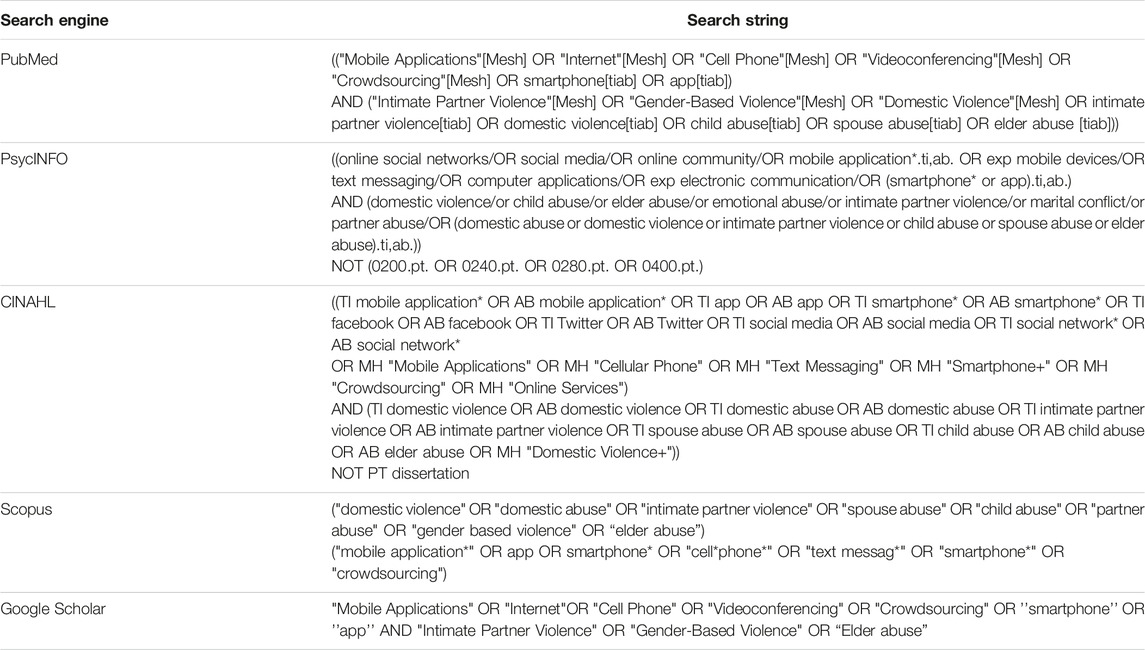
Table 1. Search string from different search engines (Worldwide publications, from date of inception to May 2023).
Definition of DV
In this article, abuse that could happen in a household setting in the United States, including child abuse, IPV and elder abuse, regardless of the relationship between survivors and perpetrators will be considered as DV. Specifically, DV can occur between a parent and child, or siblings, while IPV can only occur between romantic partners who may or may not be living together in the same household.
Eligibility Criteria
The inclusion criteria include 1) health information technology interventions applied 2) women with DV experiences (including IPV, child abuse and elder abuse) 3) published between January 2008 and May 2023. Studies related to dating violence and social media were excluded because the settings could be out of the household in the United States. Editorials, commentaries, non-peer reviewed articles, study protocols, conference abstracts, and non-English articles were also excluded.
Review Process
In the initial phase (Figure 1), articles were assessed based on their titles and abstracts, specifically examining their relevance to technology interventions for DV. Articles did not include women, or not conducted in the United States were not retrieved. Subsequently, in the second stage, full-text documents were obtained and subjected to qualitative review, guided by inclusion criteria. Prior to screening, a training session was conducted where reviewers evaluated a set of sample records together. A 75% inter-rater agreement was achieved among reviewers on this initial set before proceeding to the formal screening. During the formal screening, two independent reviewers examined the titles and abstracts of the records and categorized them as “included,” “excluded” or “uncertain” based on the relevancy to HIT interventions for DV. The reasons for exclusions include not related to HIT intervention, review articles, or any commentary articles. For any uncertain records, a senior researcher (BLINDED) resolved the status of the record.
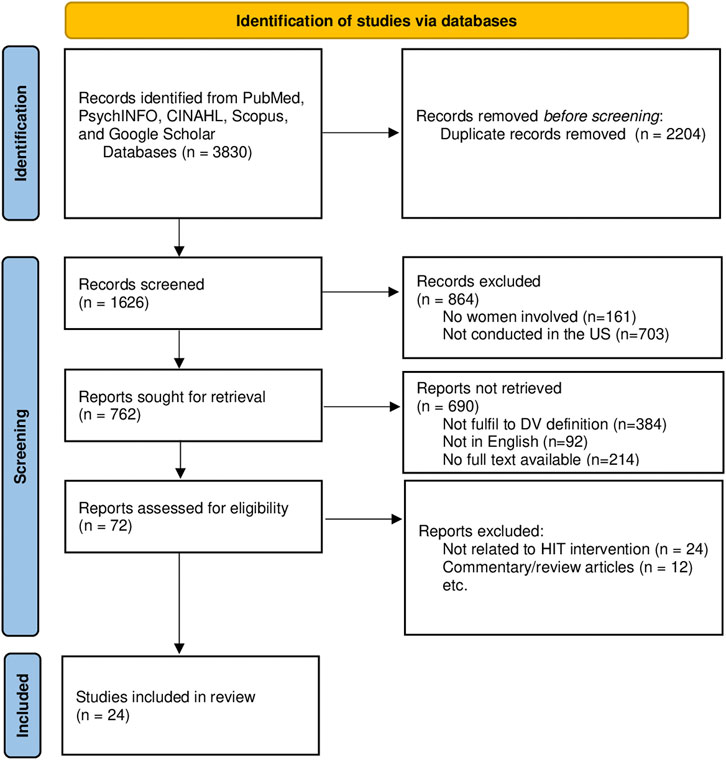
Figure 1. Preferred reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram (Worldwide publications, from date of inception to May 2023).
Data Abstraction
Two reviewers independently charted data from each eligible articles. Any disagreements were resolved through group discussions or adjudication by a third author. The variables in the spreadsheet were organized into three categories: 1) classification of the intervention (including study purpose, technology, type of intervention, and abuse), 2) descriptive details (such as sample size, location, and settings), and 3) intervention outcomes (including physical safety, psychological, and technological outcomes). This scoping review followed the guidelines from Arksey and O’Malley [24].
Results
A total of 3,830 articles were identified from four academic databases, as well as from Google Scholar. 2,204 duplicates and irrelevant articles were removed, and 72 articles underwent a more detailed screening based on the abstract and titles. 48 articles were subsequently removed due to irrelevance to the research questions or ineligibility to the predefined criteria (e.g., non-intervention studies, exploratory studies conducted in non-U.S. territory). Finally, twenty-four articles (N = 24) met all of the inclusion criteria and were included in this review (Figure 1). Table 2 listed the participant characteristics, purpose of study, purpose of intervention and types of technology, while Table 3 described the outcomes of interventions measured across studies.
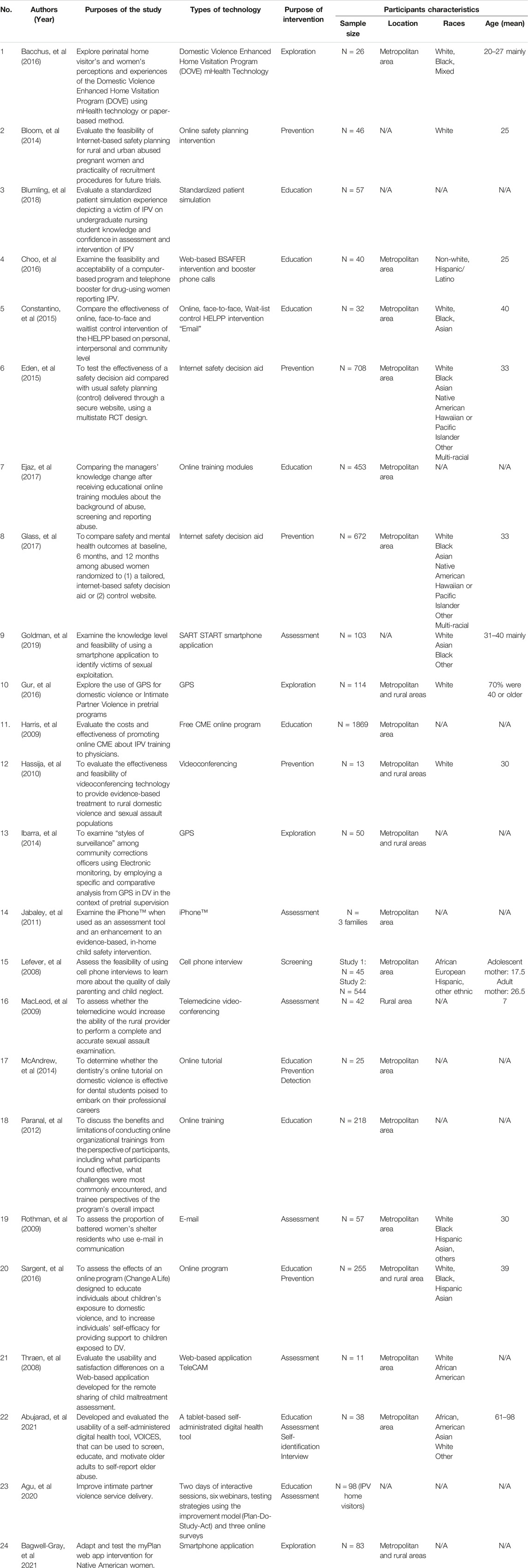
Table 2. Literature summary of critical findings among 24 studies from 2008 to 2023 (Worldwide publications, from date of inception to May 2023).
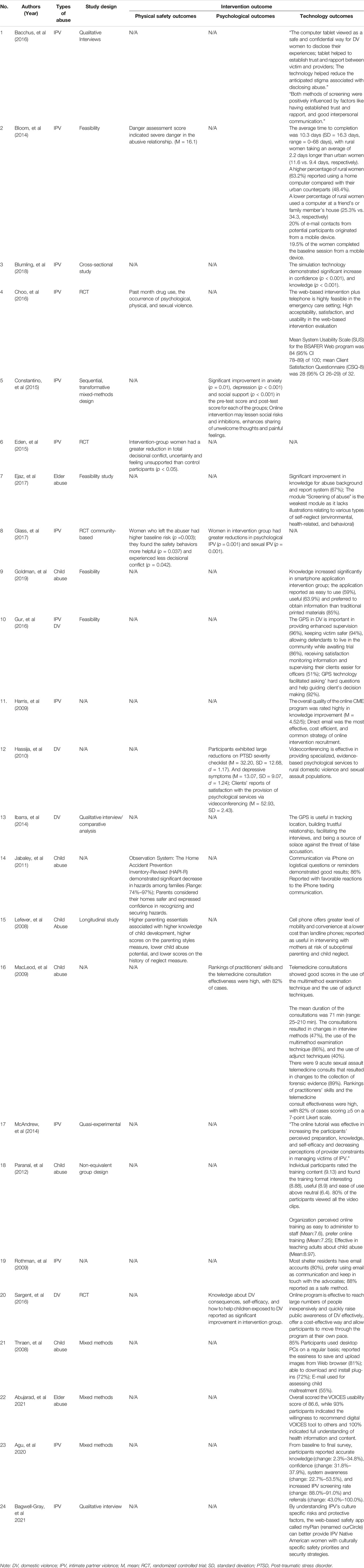
Table 3. Literature summary of critical findings among 24 studies from 2008 to 2023 (Worldwide publications, from date of inception to May 2023).
Types of Technology
Seven web-based interventions were identified; five of them collected data from a stand-alone website [25–29]. Four online trainings were designed for multidisciplinary healthcare professionals [30–33]. Five studies leveraged mobile devices to provide intervention [34–38]. Two studies used email as an intervention tool [31, 39]. Another two studies used Global Positioning System (GPS) as interventions [40, 41]. One article used videoconferencing as intervention [42], and another study utilized simulation technology to tackle domestic violence [30].
Types of Intervention
Four studies focused on prevention [25–27, 42], and ten focused on education [28, 30–33, 37, 39, 43–45]. Five studies delineated the effectiveness of HIT intervention [34, 40, 41, 46, 47] and three focused on various types of DV assessment [29, 35, 48]. Only one study emphasized screening for patients [36].
Participant Characteristics
Different types of DV survivors or potential survivors were captured in this review, such as adolescent mothers [36], abused women [27, 42], pregnant women [25, 46], and battered women [47]. Simultaneously, participants were extended to various professions like nurses [30], physicians [31], dental students [32], and law enforcement officers [34]. Among twenty-four studies, the sample sizes were ranged from 11 to 1,869. The sample characteristics and demographics were diversified. The majority of studies recruited participants from designated clinical settings (e.g., hospitals, clinics), community centers (e.g., non-governmental organizations, shelters), schools, and criminal justice services departments. A mean age of 7–40 was found across studies.
The review studies include people of diverse ethnic backgrounds, including Whites, African Americans, Hispanic Latinos, Asians, and others; however, the samples were predominantly White (N = 13). Only one article was conducted in rural areas [48] compared to fourteen articles in metropolitan areas [26, 27, 29, 31, 32, 35–37, 39, 43–47]. Another five articles have been discussed domestic violence in both metropolitan and rural areas [28, 38, 40–42].
Types of Abuse
Four types of abuse were included. Twelve studies focused on intimate partner violence (IPV) [25–27, 30–33, 38, 39, 43, 46, 47], six highlighted child abuse [29, 34–36, 45, 48], four illustrated DV [28, 40–42], and two studies targeted on elder abuse [37, 44].
Study Designs
Various research methods are used, including randomized controlled trials (N = 5) [26–28, 43, 46], and longitudinal (N = 1) [36], mixed methods (N = 5) [29, 33, 37–39], feasibility tests (N = 5) [25, 30, 34, 40, 44], non-equivalent group design (N = 1) [45], quasi-experimental design (N = 1) [32], as well as qualitative studies (N = 1) [41].
Intervention Outcomes
Physical Safety Outcomes
Physical safety outcomes were reported in five studies [25–27, 36, 43]. Only one study assessed the abuse score for physical sexual violence [43], while the other one evaluated the neglect score among children at a home setting [36]. Both studies indicated a decrease in scores for both neglect and abuse. Moreover, three other studies showed improvement in danger assessment, safety strategies, and safety behaviors using different types of measurements [25–27].
Psychological Outcomes
Depression, anxiety, and PTSD were reported as psychological health outcomes in three articles [25, 39, 42]. Bloom et al. (2014), Constantino et al. (2015), and Hassija et al. (2010) showed improvement in depression [25, 39, 42], Constantino et al. (2015) and Bloom et al. (2014) also reported improvement in PTSD and anxiety outcomes in their studies [25, 39]. Choo et al. (2016) and Lefever et al. (2008) illustrated the abuse reduction as an outcome measure [36, 43]. Only one article reported improved social support [39].
Technological Outcomes
Technological interventions effectiveness was evaluated in eight studies, which demonstrated strong feasibility, usability, and acceptability [25, 29, 34, 36, 37, 42–44]. Bloom et al. (2004), Choo et al. (2016), Thraen et al. (2008), and Abujarad et al. (2021) measured the usability [25, 29, 37, 43], while Bloom et al. (2014), Choo et al. (2016), Ejaz et al. (2017), Goldman et al. (2019), Hassija et al. (2010), and Lefever et al. (2008) measured feasibility [25, 34, 36, 42–44], and Choo et al. (2016) measured the acceptability of the technological intervention [43].
Discussion
Our study synthesized research articles on the technology interventions, research designs, and reports on the overall state of DV technology over the past decade. The results demonstrated the diverse application of technological interventions among women with DV experiences. Seven types of technology interventions were identified for DV (e.g., mobile applications, online training, web-based intervention, Global Positioning System (GPS), emails, videoconferencing, and simulation), and the majority of studies assessed usability, acceptability, and participants’ satisfaction. Several studies assessed psychological wellbeing outcomes, including stress levels, quality of life, sleep quality, and emotional needs.
HIT Interventions Dominant in IPV
Our results highlight that HIT interventions focused on different types of abuse within families, with Intimate Partner Violence (IPV) being the most common and elder abuse being the least. Research has demonstrated that young and educated people were the population group more willing to accept and adopt HIT interventions in clinical and community settings, while older adults staying at home were unwilling to use these health interventions due to perceived barriers, such as inertia, cognitive impairment, and physical disabilities [49, 50]. However, this situation might decline because of aging and the rise of computer literacy among the elderly. According to Internet World Statistics, over 89 percent of the U.S. population were internet users in 2019 [51]. The web-literate population has been growing and constantly surging with the increasing reliance on technology, machine learning, and artificial intelligence in our daily lives. Fleming (2015) delineated that over 60% of people older than 50 used technologies to browse social networking sites, take photos, and communicate in text messages [52]. Although those older than 65 may have more perceived barriers to using health technology, such as hearing deficit and cognitive impairment, they will accept new technologies when the benefits outweigh the drawbacks. There has been a proliferation of research concerning the utilization of technology in addressing elder abuse, highlighting its significant feasibility, accessibility, and effectiveness in monitoring neglect or physiological changes among elder abuse survivors, both at home and in clinical settings [53]. Therefore, it is anticipated that computer literacy and the implementation of HIT interventions among the elderly will continue to grow, leading to the expansion of interventions targeting aging in the forthcoming decades.
HIT Interventions Thrives in Urban and Rural Areas
The findings of our study also revealed that the use of HIT had been employed to assist DV survivors residing in both urban and rural settings. Due to limited access to healthcare services, women residing in rural areas experiencing DV face difficulties in effectively addressing their DV situation [54]. Previously, individuals from rural areas who were DV survivors may not have benefitted from technological advancements and treatments due to the inadequate support available to them [54]. However, our review demonstrates that digital devices in rural areas hold promise for telemedicine, providing an interactive means of delivering care, making referrals, and offering diagnosis and screening for DV survivors who may be able to meet healthcare professionals physically in a clinic or hospital. As the digital literacy rate has consistently improved over the past decade, it is expected that the limitations of technical support (such as limited wireless devices, unstable Internet, and restricted access to technical assistance) are no longer hindrances to implementing HIT interventions in rural areas. The current body of research has explored the utilization of videoconferencing, interventions pertaining to medical appointments, counseling services, and danger assessments, all of which should be expanded to rural areas through digital platforms or means. It is anticipated that the utilization of teleconferencing and online counseling services will become even more prominent, as indicated by the expanding coverage of health insurance plans for online services and consultations that aimed at addressing the mental health needs of women with DV experiences.
Web-Based Interventions Provide Better Platform for Self-Disclosure
The utilization of web-based interventions has emerged as a growing trend in DV prevention and education. HIT offers several advantages, including convenience, interactive design, and the creation of an anonymous environment facilitated by the Internet. Given that DV survivors may be reluctant to engage in face-to-face social interactions due to fear of stigmatization, shame, guilt, and judgment [16], web-based interventions provide an anonymous platform that encourages survivors to disclose their traumatic experiences more vividly and seek help proactively. It is well-documented that the sense of anonymity and social distance feeling created by the online platform fosters candid, sensitive and traumatic conversations [55, 56]. It is noteworthy that effective patient-provider communication remains the linchpin of positive intervention outcomes, particularly when addressing sensitive topics such as DV. Technological advancements promise to promote truthful or effective communication between DV survivors and healthcare professionals.
While utilizing technology for DV was predominantly applied at the patient level, the application also extends to healthcare professionals’ training. Previous literature highlighted the lack of training provided for healthcare providers to screen DV cases, thereby weakening their ability to probe DV questions and the lack of empathic listening skills during consultations. As such, DV survivors easily suffer from delayed treatment or referral from physicians [57]. For future endeavors, DV training development can extend the targeted participants to more healthcare professionals who might be poorly equipped, such as new nursing staff, social workers, or counselors during the orientation program.
HIT Intervention Improved Physical Safety and Psychological Outcomes
HIT interventions have evaluated physical safety and psychological outcomes of women with DV experience. For instance, technology-based interventionshave heightened the awareness of safety strategies among women with DV experience, strengthening their sense of security and capacity to defend themselves from perpetrators within their households [27]. Mobile applications and online training programs have evaluated the current danger level for women, thereby increasing their prompt recognition and engagement in modifying their safety strategies [25]. By leveraging the use of technology, women can actively participate in reassessing their danger level and adapting their contingency plans [27]. They feel safer and find it easier to evaluate their situation on their smartphone [35]. Moreover, online platforms, emails, and messaging systems could reduce the risk of anxiety, depression, and post-traumatic stress disorder (PTSD) among women experiencing DV [25, 39]. Technology provides a valuable platform for women to share and discuss their experiences with other survivors, aligning with previous research indicating that computer-based interventions can significantly improve social support, self-efficacy, and alleviate feelings of loneliness among rural women [58]. Consequently, HIT interventions can contribute to developing a stronger social support network for women facing DV.
There is a wealth of evidence showing the importance of emotional health towards women with DV experiences. However, our review indicated limited HIT intervention studies on assessing the emotional aspects of survivors’ experiences. For example, World Health Organization (WHO) demonstrated that women with IPV experience could have a higher demand for mental health services and an increased likelihood of psychological distress [59]. Women could experience emotional breakdown easier or the need to express themselves after traumatic experiences like DV. The anonymity and instant communication facilitated by mobile devices and the Internet, have provided opportunities for women to seek emotional support through texting through online platforms [60, 61]. This avenue enables better adaptations and enhances the quality of life following traumatic experiences caused by abusive relationships. Future HIT research endeavors could focus on improving the emotional status of survivors, thus promoting more favorable mental health outcomes.
Despite the positive outcomes reported in the literature, adopting HIT interventions for DV population is not without demerits. Several articles have delineated the limitations of using a technical device across community, clinical, and household settings [62, 63]. With reference to the power and control theory of DV, Baddam (2017) believes that the use of technology may exacerbate DV conditions as perpetrators can install tracker applications with GPS and blame the survivors for concealing the DV-related on their smartphones [64]. Perpetrators can turn out to be digital stalkers and constitute a significant threat to the victim, thereby permanently menacing psychological harm to the victim’s life [65].
HIT interventions have predominantly focused on raising awareness and building a digital platform for women to communicate. However, the evaluation of most interventions has typically been limited to pre-and post-test assessments, without consistently tracking long-term performance across multiple time points, such as 3, 6, and 9 months follow-up. Besides, existing research weights physical wellbeing higher than emotional wellbeing. There is currently no standardized measurement for assessing emotions via technology. It is suggested that incorporating advanced machine learning data analytics could be beneficial in extracting emotional needs and delivering emotional support through virtual messaging, such as natural language processing. Further research can capitalize on data analytics to develop an emotional terminology dictionary (e.g., terms related to resilience or distress) that provides a measurable benchmark for extracting and systematically quantifying emotional text data (Table 4).
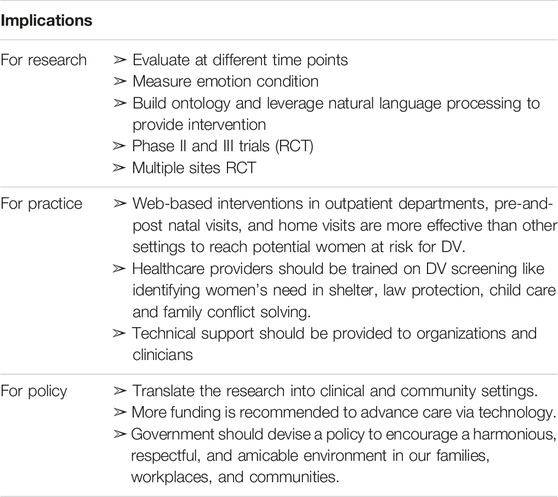
Table 4. Literature summary on implications for practice, policy and research among 24 studies From 2008 to 2023 (Worldwide publications, from date of inception to May 2023).
Furthermore, it is important to direct future research avenues towards conducting phase II and III randomized controlled clinical trials to evaluate the preliminary effect size, side effects, and efficacy of the technology within a specific context. The majority of studies reviewed primarily focused on intervention design, feasibility, and prototype intervention. The subsequent step should involve an initial test of intervention in comparison with an appropriate alternative option. To identify outcomes and determine whether the measurement tools can detect the anticipated changes, a small sample size of 40–60 randomized controlled trials should be conducted, enabling the calculation of effect sizes for the intervention [66]. Future research can assess technological interventions by RCT in multiple settings or within a targeted setting to evaluate the efficacy.
This review also provides clinical insights into the context and environment of DV technology interventions. There are abundant web-based interventions, supported by theoretical and empirical evidence of their efficacy and feasibility, to raise awareness, enhance knowledge, and evaluate the specific needs of survivors. The utilization of web-based interventions in outpatient departments, prenatal or postnatal clinics, and home visits yield greater effectiveness compared to other settings. Moreover, existing literature highlights the importance of prioritizing victim’s needs during family conflict. Healthcare providers should be well-informed and trained in addressing the common application procedures and criteria for DV shelter, safety planning, law protection, and childcare through technology (i.e., online training, and case study from online).
The resolution of this public health concern necessitates the implementation of policy modifications or reforms. From a policy standpoint, it is crucial to facilitate the translation of research findings into practical applications in clinical and community settings. In accordance with the socioecological model, the prevention of DV should involve interventions targeting individuals, interpersonal relationships, societal structures, and community dynamics. The government and other relevant stakeholders should join forces and support to violence prevention research endeavors. Additionally, it is recommended to allocate increased funding towards research and innovative technologies to enhance the provision of nursing care and social services through technological interventions. Furthermore, the government should formulate policies to foster an atmosphere of harmony, respect, and amicability within families, workplaces, and communities.
Limitations
Studies included in this review have methodological considerations regarding the sample size, demographic characteristics, and design that should be noted with caution. Our included studies generally with small sample size, with several studies even being characterized as pilot or exploratory studies. Although the geographical settings from our studies include rural, suburban, urban, clinical, and community areas, the demographic characteristics still predominantly comprise a white population, which affected the overall generalizability of this study. Given the inconsistent reporting of study location among studies, we categorized them as either metropolitan or rural areas based on the current metrics from the U.S. Census Bureau (2016) [67]. Notably, only four studies took place in rural areas; future research should strive to clarify the definition or characteristics of locations where the interventions were conducted. Also, this review did not capture which forms of abuse were experienced by the DV survivors, which could influence the adherence to HIT intervention. We accept this trade-off for this scoping review as the adherence data was not provided in most of the studies. To maintain consistency and precise comparison in the analysis, this review specifically excluded dating violence, and articles using social media to collect data for DV. Therefore, it is possible that certain HIT interventions in DV populations were missed from this review.
Conclusion
By and large, DV remains a significant public health issue characterized by repetitive trauma within a vicious cycle, especially in the United States. This review highlights the current scope of HIT interventions in addressing DV. Our synthesized literature demonstrates substantial heterogeneity in intervention modalities, target populations, as well as study designs. HIT interventions offer an opportunity to reach potential survivors from underserved rural and suburban areas where access to healthcare services and DV support may be limited. Moreover, the range of HIT interventions for DV encompasses interventions at the patient and provider levels. Implementing online training modules for multidisciplinary healthcare practitioners shows promise in improving outcomes, as demonstrated by pre- and post-intervention assessments. While not all physical health outcomes were measured, the findings emphasize technology’s immense potential in reaching a broader and more heterogeneous sample base. Leveraging HIT can support DV survivors across individuals, families, and communities.
Author Contributions
VH conceptualized the idea for the scoping review. BZ and BJ undertook the search strategy and ran the database searches. MK provided guidance on methodology. VH, BZ, and BJ screened abstracts and titles for inclusion/exclusion and full text articles for inclusion/exclusion. Data was extracted by VH, BZ, and BJ. VH, BZ, and BJ contributed to interpretation of results. Writing was completed by VH and BZ. KW and YL reviewed the manuscript and provided overall direction and edited the manuscript. All authors contributed to the article and approved the submitted version.
Funding
The author(s) declare(s) that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of Interest
The authors declare that they do not have any conflicts of interest.
Acknowledgments
The main results of this study have been published as a PhD dissertation thesis and the approval to republish the data has been obtained.
References
1. Sugg, N. Intimate Partner Violence: Prevalence, Health Consequences, and Intervention. Med Clin North Am (2015) 99:629–49. doi:10.1016/j.mcna.2015.01.012
2. Department of Justice. Office on Violence Against Women (OVW) (2019). Available from: https://www.justice.gov/ovw (Accessed April 1, 2023).
3. Black, MC, Basile, KC, Breiding, MJ, Smith, SG, Walters, ML, Merrick, MT, et al. The National Intimate Partner and Sexual Violence Survey: 2010 Summary Report (2011) (2011). Available from: http://www.cdc.gov/violenceprevention/pdf/nisvs_report2010-a.pdf (Accessed April 1, 2023).
4. Peterson, C, Kearns, MC, McIntosh, WL, Estefan, LF, Nicolaidis, C, McCollister, KE, et al. Lifetime Economic Burden of Intimate Partner Violence Among U.S. Adults. Am J Prev Med (2018) 55:433–44. doi:10.1016/j.amepre.2018.04.049
5. National Center for Injury Prevention and Control, Centers for Disease Control and Prevention. Infographic Based on Data from the National Intimate Partner and Sexual Violence Survey (Nisvs): 2010-2012 State Report (2017). Available from: https://www.cdc.gov/violenceprevention/pdf/NISVS-infographic-2016.pdf (Accessed April 1, 2023).
6. Dolezal, TA, McCollum, DL, and Callahan, MJ. Hidden Costs in Health Care: The Economic Impact of Violence and Abuse. MN: Academy on Violence and Abuse (2009).
7. Carlson, BE, McNutt, LA, and Choi, DY. Childhood and Adult Abuse Among Women in Primary Health Care: Effects on Mental Health. J interpersonal violence (2003) 18:924–41. doi:10.1177/0886260503253882
8. Golding, JM. Intimate Partner Violence as a Risk Factor for Mental Disorders: A Meta-Analysis. J Fam violence (1999) 14:99–132. doi:10.1023/a:1022079418229
9. Hathaway, JE, Mucci, LA, Silverman, JG, Brooks, DR, Mathews, R, and Pavlos, CA. Health Status and Health Care Use of Massachusetts Women Reporting Partner Abuse. Am J Prev Med (2000) 19(4):302–7. doi:10.1016/s0749-3797(00)00236-1
10. Li, Y, Marshall, CM, Rees, HC, Nunez, A, Ezeanolue, E, and Ehiri, J. Intimate Partner Violence and HIV Infection Among Women: A Systematic Review and Meta-Analysis. J Int AIDS Soc (2014) 17(1):18845. doi:10.7448/IAS.17.1.18845
11. Breiding, MJ, Chen, J, and Black, MC. Intimate Partner Violence in the United States—2010. Atlanta, GA: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention (2014). Available from: https://stacks.cdc.gov/view/cdc/21961 (Accessed April 1, 2023).
12. Devries, K, Watts, C, Yoshihama, M, Kiss, L, Schraiber, LB, Deyessan, N, et al. Violence Against Women Is Strongly Associated With Suicide Attempts: Evidence From the WHO Multi-Country Study on Women’s Health and Domestic Violence Against Women. Soc Sci Med (2011) 73(1):79–86. doi:10.1016/j.socscimed.2011.05.006
13. Desai, S, Arias, I, Thompson, MP, and Basile, KC. Childhood Victimization and Subsequent Adult Revictimization Assessed in a Nationally Representative Sample of Women and Men. Violence and victims (2002) 17(6):639–53. doi:10.1891/vivi.17.6.639.33725
14. Choo, E, Ranney, M, Wetle, T, Morrow, K, Mello, M, Squires, D, et al. Attitudes Toward Computer Interventions for Partner Abuse and Drug Use Among Women in the Emergency Department. Addict Disord their Treat (2015) 14:95–104. doi:10.1097/ADT.0000000000000057
15. Suler, J. The Online Disinhibition Effect. Cyberpsychol Behav (2004) 7:321–6. doi:10.1089/1094931041291295
16. Tarzia, L, Iyer, D, Thrower, E, and Hegarty, K. “Technology Doesn’t Judge You”: Young Australian Women’s Views on Using the Internet and Smartphones to Address Intimate Partner Violence. J Technol Hum Serv (2017) 35:199–218. doi:10.1080/15228835.2017.1350616
17. Thompson, TG, and Brailer, DJ. The Decade of Health Information Technology: Delivering Consumer-Centric and Information-Rich Health Car. Med Benefits (2004) 21:12.
18. Ranney, ML, Choo, EK, Cunningham, RM, Spirito, A, Thorsen, M, Mello, MJ, et al. Acceptability, Language, and Structure of Text Message-Based Behavioral Interventions for High-Risk Adolescent Females: A Qualitative Study. J Adolesc Health (2014) 55:33–40. doi:10.1016/j.jadohealth.2013.12.017
19. Gilroy, H, McFarlane, J, Nava, A, and Maddoux, J. Preferred Communication Methods of Abused Women. Public Health Nurs (2013) 30:402–8. doi:10.1111/phn.12030
20. Al-Alosi, H. Fighting Fire With Fire: Exploring the Potential of Technology to Help Victims Combat Intimate Partner Violence. Aggression Violent Behav (2020) 52:101376. doi:10.1016/j.avb.2020.101376
21. Boydell, KM, Hodgins, M, Pignatiello, A, Teshima, J, Edwards, H, and Willis, D. Using Technology to Deliver Mental Health Services to Children and Youth: A Scoping Review. J Can Acad Child Adolesc Psychiatry (2014) 23(2):87–99. doi:10.1016/j.avb.2020.101376
22. Tiwari, A, Recinos, M, Garner, J, Self-Brown, S, Momin, R, Durbha, S, et al. Use of Technology in Evidence-Based Programs for Child Maltreatment and its Impact on Parent and Child Outcomes. Front digital Health (2023) 5:1224582. doi:10.3389/fdgth.2023.1224582
23. Vandebosch, H, Botezat, A, Amodeo, AL, Pabian, S, Plichta, P, Puharić, Z, et al. A Scoping Review of Technological Interventions to Address Ethnicity-Related Peer Aggression. Aggression violent Behav (2022) 67:101794. doi:10.1016/j.avb.2022.101794
24. Arksey, H, and O'Malley, L. Scoping Studies: Towards a Methodological Framework. Int J Soc Res Methodol (2005) 8(1):19–32. doi:10.1080/1364557032000119616
25. Bloom, TL, Glass, NE, Case, J, Wright, C, Nolte, K, and Parsons, L. Feasibility of an Online Safety Planning Intervention for Rural and Urban Pregnant Abused Women. Nurs Res (2014) 63:243–51. doi:10.1097/NNR.0000000000000036
26. Eden, KB, Perrin, NA, Hanson, GC, Messing, JT, Bloom, TL, Campbell, JC, et al. Use of Online Safety Decision Aid by Abused Women: Effect on Decisional Conflict in a Randomized Controlled Trial. Am J Prev Med (2015) 48:372–83. doi:10.1016/j.amepre.2014.09.027
27. Glass, NE, Perrin, NA, Hanson, GC, Bloom, TL, Messing, JT, Clough, AS, et al. The Longitudinal Impact of an Internet Safety Decision Aid for Abused Women. Am J Prev Med (2017) 52:606–15. doi:10.1016/j.amepre.2016.12.014
28. Sargent, KS, McDonald Rvu, NL, and Jouriles, EN. Evaluating an Online Program to Help Children Exposed to Domestic Violence: Results of Two Randomized Controlled Trials. J Fam Violence (2016) 31:647–54. doi:10.1007/s10896-016-9800-8
29. Thraen, IM, Frasier, L, Cochella, C, Yaffe, J, and Goede, P. The Use of TeleCAM as a Remote Web-Based Application for Child Maltreatment Assessment, Peer Review, and Case Documentation. Child Maltreat (2008) 13(4):368–76. doi:10.1177/1077559508318068
30. Blumling, A, Kameg, K, Cline, T, Szpak, J, and Koller, C. Evaluation of a Standardized Patient Simulation on Undergraduate Nursing Students’ Knowledge and Confidence Pertaining to Intimate Partner Violence. J forensic Nurs (2018) 14:174–9. doi:10.1097/JFN.0000000000000212
31. Harris, JJM, Novalis-Marine, C, Amend, RW, and Surprenant, ZJ. Promoting Free Online CME for Intimate Partner Violence: What Works at what Cost? J Contin Educ Health Professions (2009) 29:135–41. doi:10.1002/chp.20025
32. McAndrew, M, Pierre, GC, and Kojanis, LC. Effectiveness of an Online Tutorial on Intimate Partner Violence for Dental Students: A Pilot Study. J Dent Educ (2014) 78:1176–81. doi:10.1002/j.0022-0337.2014.78.8.tb05789.x
33. Agu, N, Michael-Asalu, A, Ramakrishnan, R, Birriel, PC, Balogun, O, Parish, A, et al. Improving Intimate Partner Violence Services in home Visiting: A Multisite Learning Collaborative Approach. J Soc Serv Res (2019) 46:439–51. doi:10.1080/01488376.2019.1582452
34. Goldman, S, and Goyal, D. Knowledge Regarding Child Victims of Commercial Sexual Exploitation and the Feasibility of Using a Smartphone Application: A Pilot Study. J forensic Nurs (2019) 15:103–9. doi:10.1097/JFN.0000000000000240
35. Jabaley, JJ, Lutzker, JR, Whitaker, DJ, and Self-Brown, S. Using iPhones™ to Enhance and Reduce Face-To-Face home Safety Sessions Within SafeCare®: An Evidence-Based Child Maltreatment Prevention Program. J Fam Violence (2011) 26:377–85. doi:10.1007/s10896-011-9372-6
36. Lefever, JB, Howard, KS, Lanzi, RG, Borkowski, JG, Atwater, J, Guest, KC, et al. Cell Phones and the Measurement of Child Neglect: The Validity of the Parent-Child Activities Interview. Child Maltreat (2008) 13:320–33. doi:10.1177/1077559508320680
37. Abujarad, F, Ulrich, D, Edwards, C, Choo, E, Pantalon, MV, Jubanyik, K, et al. Development and Usability Evaluation of VOICES: A Digital Health Tool to Identify Elder Mistreatment. J Am Geriatr Soc (2021) 69:1469–78. doi:10.1111/jgs.17068
38. Bagwell-Gray, ME, Loerzel, E, Dana Sacco, G, Messing, J, Glass, N, Sabri, B, et al. From Myplan to Ourcircle: Adapting a Web-Based Safety Planning Intervention for Native American Women Exposed to Intimate Partner Violence. J Ethnic Cult Divers Soc Work (2021) 30:163–80. doi:10.1080/15313204.2020.1770651
39. Constantino, RE, Braxter, B, Ren, D, Burroughs, JD, Doswell, WM, Wu, L, et al. Comparing Online With Face-To-Face HELPP Intervention in Women Experiencing Intimate Partner Violence. Issues Ment Health Nurs (2015) 36:430–8. doi:10.3109/01612840.2014.991049
40. Gur, OM, Ibarra, PR, and Erez, E. Specialization and the Use of GPS for Domestic Violence by Pretrial Programs: Findings From a National Survey of US Practitioners. J Technol Hum Serv (2016) 34:32–62. doi:10.1080/15228835.2016.1139418
41. Ibarra, PR, Gur, OM, and Erez, E. Surveillance as Casework: Supervising Domestic Violence Defendants With GPS Technology. Crime, L Soc Change (2014) 62:417–44. doi:10.1007/s10611-014-9536-4
42. Hassija, C, and Gray, MJ. The Effectiveness and Feasibility of Videoconferencing Technology to Provide Evidence-Based Treatment to Rural Domestic Violence and Sexual Assault Populations. Telemed e-Health (2011) 17:309–15. doi:10.1089/tmj.2010.0147
43. Choo, EK, Zlotnick, C, Strong, DR, Squires, DD, Tapé, C, and Mello, MJ. BSAFER: A Web-Based Intervention for Drug Use and Intimate Partner Violence Demonstrates Feasibility and Acceptability Among Women in the Emergency Department. Substance abuse (2016) 37:441–9. doi:10.1080/08897077.2015.1134755
44. Ejaz, FK, Rose, M, and Anetzberger, G. Development and Implementation of Online Training Modules on Abuse, Neglect, and Exploitation. J elder abuse neglect (2017) 29:73–101. doi:10.1080/08946566.2017.1307153
45. Paranal, RK, Washington, T, and Derrick, C. Utilizing Online Training for Child Sexual Abuse Prevention: Benefits and Limitations. J Child Sex Abus (2012) 21:507–20. doi:10.1080/10538712.2012.697106
46. Bacchus, LJ, Bullock, L, Sharps, P, Burnett, C, Schminkey, DL, Buller, AM, et al. Infusing Technology Into Perinatal Home Visitation in the United States for Women Experiencing Intimate Partner Violence: Exploring the Interpretive Flexibility of an mHealth Intervention. J Med Internet Res (2016) 18:e302. doi:10.2196/jmir.6251
47. Rothman, EF, Meade, J, and Decker, MR. E-Mail Use Among a Sample of Intimate Partner Violence Shelter Residents. Violence Against Women (2009) 15:736–44. doi:10.1177/1077801209332188
48. MacLeod, KJ, Marcin, JP, Boyle, C, Miyamoto, S, Dimand, RJ, and Rogers, KK. Using Telemedicine to Improve the Care Delivered to Sexually Abused Children in Rural, Underserved Hospitals. Pediatrics (2009) 123:223–8. doi:10.1542/peds.2007-1921
49. Jimison, H, Gorman, P, Woods, S, Nygren, P, Walker, M, Norris, S, et al. Barriers and Drivers of Health Information Technology Use for the Elderly, Chronically Ill, and Underserved. Evid Rep Technol Assess (Full Rep) (2008) 175:1–1422.
50. Lober, WB, Zierler, B, Herbaugh, A, Shinstrom, SE, Stolyar, A, Kim, EH, et al. Barriers to the Use of a Personal Health Record by an Elderly Population. AMIA Annu Symp Proc (2006) 2006:514–8.
51. Internet World Stats © Copyright. Miniwatts Marketing Group (2019). Available from: http://internetworldstats.com/ (Accessed April 8, 2019).
52. Fleming, G, Reitsma, R, Pappafotopoulos, T, Duan, X, and Birrel, R. The State of Consumers and Technology Benchmark 2015. US. Cambridge, MA: Forrester (2015).
53. Beach, SR. The Role of Technology in Elder Abuse Research. In: X Dong, editor. Elder Abuse: Research, Practice and Policy. Cham: Springer (2017). p. 201–14.
54. Peek-Asa, C, Wallis, A, Harland, K, Beyer, K, Dickey, P, and Saftlas, A. Rural Disparity in Domestic Violence Prevalence and Access to Resources. J Womens Health (Larchmt) (2011) 20:1743–9. doi:10.1089/jwh.2011.2891
55. Cantrell, MA, and Lupinacci, P. Methodological Issues in Online Data Collection. J Adv Nurs (2007) 60:544–9. doi:10.1111/j.1365-2648.2007.04448.x
56. Wharton, CM, Hampl, JS, Hall, R, and Winham, DM. PCs or Paper-And Pencil:online Surveys for Data Collection. J Am Diet Assoc (2003) 103:1458–60. doi:10.1016/j.jada.2003.09.004
57. Gillespie, K, Branjerdporn, G, Tighe, K, Carrasco, A, and Baird, K. Domestic Violence Screening in a Public Mental Health Service: A Qualitative Examination of Mental Health Clinician Responses to DFV. J Psychiatr Ment Health Nurs (2023) 30:472–80. doi:10.1111/jpm.12875
58. Weinert, C, Cudney, S, and Hill, WG. Rural Women, Technology, and Self-Management of Chronic Illness. Can J Nurs Res (2008) 40:114–34.
59. Ellsberg, M, Jansen, HA, Heise, L, Watts, CH, and Garcia-Moreno, C, WHO Multi-country Study on Women's Health and Domestic Violence against Women Study Team. Intimate Partner Violence and Women's Physical and Mental Health in the WHO Multi-Country Study on Women's Health and Domestic Violence: An Observational Study. The lancet (2008) 371:1165–72. doi:10.1016/S0140-6736(08)60522-X
60. Kivran-Swaine, F, Brody, S, Diakopoulos, N, and Naaman, M. Of joy and Gender: Emotional Expression in Online Social Networks. In: S Poltrock, editor. Proceedings of the ACM 2012 Conference on Computer Supported Cooperative Work Companion. New York, NY, United States: Association for Computing Machinery (2012). p. 139–142.
61. Hui, V, Constantino, RE, and Lee, YJ. Harnessing Machine Learning in Tackling Domestic Violence—An Integrative Review. Int J Environ Res Public Health (2023) 20(6):4984. doi:10.3390/ijerph20064984
62. Murray, CE, Pow, AM, Chow, A, Nemati, H, and White, J. Domestic Violence Service Providers’ Needs and Perceptions of Technology: A Qualitative Study. J Technol Hum Serv (2015) 33:133–55. doi:10.1080/15228835.2014.1000558
63. Southworth, C, Finn, J, Dawson, S, Fraser, C, and Tucker, S. Intimate Partner Violence, Technology, and Stalking. Violence Against Women (2007) 13:842–56. doi:10.1177/1077801207302045
64. Baddam, B. Technology and its Danger to Domestic Violence Victims: How Did He Find Me? Alb LJ Sci Tech (2017) 28:73.
65. Melander, LA. College Students' Perceptions of Intimate Partner Cyber Harassment. Cyberpsychol Behav Soc Netw (2010) 13:263–8. doi:10.1089/cyber.2009.0221
66. Gitlin, LN. Introducing a New Intervention: An Overview of Research Phases and Common Challenges. Am J Occup Ther (2013) 67:177–84. doi:10.5014/ajot.2013.006742
67. U.S. Census Bureau. Defining Rural at the U.S. Census Bureau American Community Survey and Geography Brief (2016). Available from: https://www2.census.gov/geo/pdfs/reference/ua/Defining_Rural.pdf (Accessed April 1, 2023).
Keywords: health information technology, domestic violence, scoping review, women’s health, domestic abuse
Citation: Hui V, Zhang B, Jeon B, Wong KCA, Klem ML and Lee YJ (2024) Harnessing Health Information Technology in Domestic Violence in the United States: A Scoping Review. Public Health Rev 45:1606654. doi: 10.3389/phrs.2024.1606654
Received: 21 September 2023; Accepted: 20 May 2024;
Published: 21 June 2024.
Edited by:
Raquel Lucas, University Porto, PortugalReviewed by:
Shirin Shahbazi Sighaldeh, Tehran University of Medical Sciences, IranSara Soares, University Porto, Portugal
Copyright © 2024 Hui, Zhang, Jeon, Wong, Klem and Lee. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
PHR is edited by the Swiss School of Public Health (SSPH+) in a partnership with the Association of Schools of Public Health of the European Region (ASPHER)+
*Correspondence: Vivian Hui, dml2aWFuYy5odWlAcG9seXUuZWR1Lmhr
†Present address: Mary Lou Klem, Health Sciences Library System, University of Pittsburgh, Pittsburgh, PA, United States