 Owen Cranshaw
Owen Cranshaw Steven Haworth
Steven Haworth- Institute for Social and Economic Research (ISER), University of Essex, Colchester, United Kingdom
Objectives: This paper systematically reviews how spatial analysis has been used to measure relationships between access to the built environment and Allostatic Load (AL) or biomarkers relevant to the stress pathway. Geographic Information Systems (GIS) facilitate objective measurement of built environment access that may explain unequal health outcomes linked to living in stressful environments.
Methods: Systematic review, search date 13 July 2022 with methods published a priori. Included studies that quantitatively assessed associations between GIS measures of neighborhood attributes and biomarkers of stress.
Results: 23 studies from 14 countries were included having used GIS measures to assess relationships between access to the built environment and biomarkers relevant to AL, with 17 being cross-sectional and 6 longitudinal. Just 2 studies explicitly assessed associations between GIS measures and AL, but 21 explored biomarkers relevant to the stress pathway. GIS was used to calculate density (how much of x within y) and proximity (how far from a to b) measures.
Conclusion: GIS measures of greenspace, the food environment, area-level demographics, and land-use measures were found to influence biomarkers relevant to the stress pathway, highlighting the utility of this approach. GIS use is extremely limited when measuring the built environment and its influence on AL but has been widely used to consider effects on individual biomarkers of stress.
Systematic Review Registration: [https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=348355], identifier [CRD42022348355].
Introduction
A growing literature indicates increasing geographical inequalities in health, with the worst outcomes occurring for those born and living in the most deprived neighborhoods [1]. For example, the 2010 Marmot Review found that, on average, those living in the most deprived neighborhoods die 7 years younger than those living in the least deprived neighborhoods. Moreover, the Marmot 10 years follow up found inequalities in life expectancy had increased, particularly in the most deprived neighborhoods [2]. The effects of neighborhood characteristics on various health outcomes have been shown to persist even after adjusting for multiple individual factors such as age, gender, ethnicity and educational attainment [3–10]. As a result, where we live is increasingly being recognized as one of the most important precursors of chronic disease, and as an explanation for variations in health outcomes [11].
Yet, most neighborhood effects studies fail to define the causal mechanisms that explain how neighborhood characteristics contribute to increasing risks of poor health over and above individual risk factors [12, 13]. For instance, poorer quality housing may explain risk at an individual level, but how a neighborhood having a higher percentage of low-quality housing contributes to more widely distributed poorer health outcomes across the area (even to those not exposed directly) is less well understood. Moreover, studies often include only a limited range of neighborhood characteristics, masking complexity and hindering their ability to identify neighborhood-level determinants of health outcomes [14]. Responding to such critiques, studies have sought to identify potential causal pathways, with growing evidence pointing to the stress pathway, theoretically measured by the concept of Allostatic Load (AL), playing a mediatory role between neighborhoods and poorer health outcomes [1, 15, 16]. The stress pathway encapsulates the idea that adverse neighborhood environments, which may be characterized by social or economic disadvantage, neighborhood disorder, or fewer or poorer quality resources, can act as chronic stressors that activate and lead to dysregulation of the hypothalamic-pituitary-adrenal-axis [17]. Furthermore, AL is conceptualized as the overall wear and tear on the body, resulting from stressors in the environment and as a bridge to poorer health outcomes. As such, where environmental stressors are more pronounced or ongoing, the stress response is likely to be activated more frequently, increasing the likelihood of dysregulation across a range of markers of the stress response.
Advances in Geographic Information Systems (GIS), and recognition of the utility of the approach, make it possible to consider which attributes of neighborhoods might contribute to poorer health outcomes by objectively and accurately measuring the distribution of, and access to, specific resources within neighborhoods. GIS techniques provide the potential to capture the complexity of community environments at finer scales than existing measures of deprivation, offering the potential to identify target areas for policy interventions. As such, there is an increasing body of evidence using GIS to consider how where we live impacts health [18–20]. One complexity is that GIS measures are wide-ranging, since they can incorporate any data that has a spatial attribute. Therefore, GIS has been applied in a variety of ways, highlighting the need for this review.
This review brings together these strands of neighborhood effects research and reviews the evidence of how GIS has been used to measure relationships between access to the built environment and biomarkers associated with stress or overall AL. Given the increasing body of evidence pointing to the stress pathway linking neighborhood effects on health, and the benefits of using GIS to measure the complex structure of neighborhoods, this review seeks to elucidate how spatial analysis has and can be used and its effectiveness when exploring the relationship between place and health.
Methods
This systematic review conforms to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) Guidelines [21] and was registered with PROSPERO with protocol registration number: CRD42022348355.
Search Strategy
Search terms were clustered under three overarching themes: “Geographic Information Systems,” “Neighborhood Effects” and “Allostatic Load or Stress.” Search terms were informed by relevant systematic reviews [11, 16, 20, 22, 23]. All, included studies were required to be empirical; human; available in English; and to quantitatively assess associations between GIS measures of neighborhood attributes and biomarkers of stress or overall AL. Terms like “GPS” and “Accelerometer” measures were not included in the search terms as these were considered to capture individual level, rather than neighborhood level attributes of the built environment. Reviews and studies that did not contain explicit GIS measures or at least one stress or AL-related biomarker were excluded, as were studies focused solely on BMI. A detailed description of the search strategy and terms is available in the registered PROSPERO protocol [24]. Records were screened by both researchers independently and in duplicate, with near-perfect agreement (94%, Cohen’s k = 0.89) and discrepancies checked by an independent researcher.
Data Sources
PubMed; MEDLINE; PsychInfo; PsychArticles; CINAHL; Scopus; Web of Science, and the pre-print journal databases; ESSOAR and medRxiv were searched from database establishment to 13th July 2022. Database searching was accompanied by grey literature searches and hand searching of reference lists of included studies. Grey literature included searches through working papers from research institutes, and reports, briefs, and policy documents from relevant agencies [e.g., Office for National Statistics (ONS)].
Risk of Bias Assessment and Data Extraction
Data extraction was completed independently and in duplicate by Author-1 and Author-2. A predetermined and standardized Excel spreadsheet was used to extract: author, publication date, and title; country; population characteristics and sample size; study design; data sources for population and neighborhood data; neighborhood unit; outcome measure/s; GIS measures, results (including direction and strength); and study strengths and limitations. Extraction records were subsequently combined, with discrepancies discussed and agreed upon. Risk of bias for all included records was assessed independently and in duplicate by both researchers using the Joanna Briggs Institute (JBI) appraisal tools [25]. Records were rated as having a low, moderate or high risk of bias with discrepancies checked by an independent third researcher.
Analysis
The focus of this review is to identify how GIS methods have been used in assessing relationships between neighborhood characteristics and biomarkers relevant to AL. Therefore, methodological variations used in this field were thematically analyzed. Results were organized by the type of GIS measure used (density, proximity), and subcategorized by the aspect of the neighborhood context these measures sought to capture.
Results
Characteristics of Selected Studies
722 records were identified through database searching with 2 found through reference list searching. Of these 724 records, 172 duplicates were removed, leaving 552 unique records. Title and abstract screening further removed 414 records. The remaining 138 studies were obtained for full-text screening. During full-text screening, 63 records were excluded for only having BMI as an outcome, 32 for having no biomarkers, and 18 because they had no explicit GIS measures. The remaining 23 articles were included for review (see Figure 1).
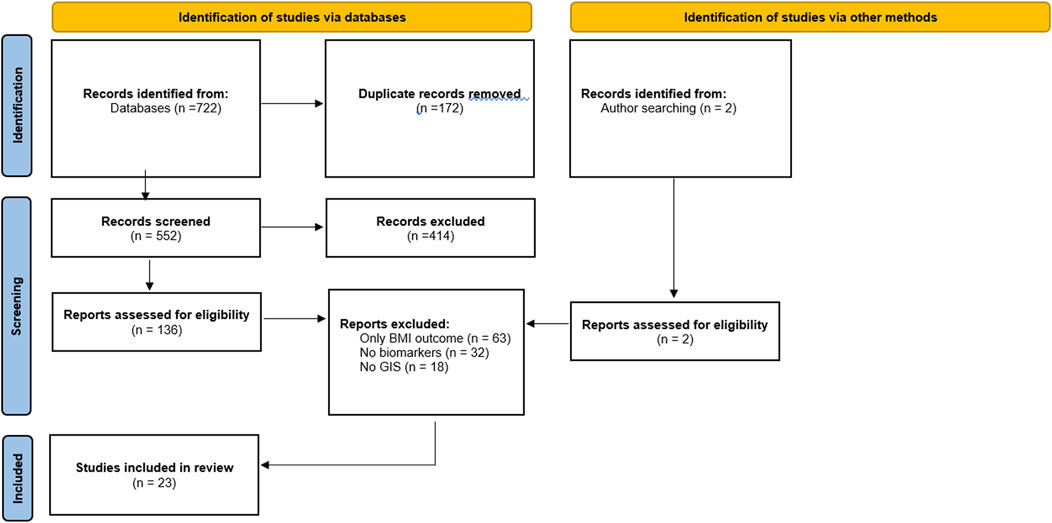
Figure 1. Flow diagram of inclusion/exclusion (systematic review, worldwide, journal start-date-2022).
The 23 included studies were conducted in 14 countries including: Australia [26], Canada [27–30], France [31], Greece [32], Japan [33], Portugal [34], South Africa [35], the United Kingdom [36], and the United States (US) [37–48]. Thirteen studies [26, 28, 29, 31, 32, 34–36, 38, 42–44, 48] were from 2017 or later. Five studies were longitudinal [36, 40, 43, 46, 47] and 18 were cross-sectional [26–35, 37–39, 41, 42, 44, 45, 48]. Twenty studies included adults only (at least 18+) [26–33, 35–40, 42–45, 47, 48], 2 included only children [34, 46], and 1 both [41]. Table 1 summarises the included studies.

Table 1. Study characteristics (systematic review, worldwide, journal start-date-2022).
Data Sources
Most studies used different sources of population data. Only the Prospective Urban Rural Epidemiology [29, 35] study and the Montreal Neighborhood Survey of Lifestyle and Health [27, 30] were used twice, making direct comparisons difficult. Ten studies [26, 28–30, 34, 35, 38, 45–47] used nationally representative data from surveys and panel studies, five [29, 32, 34, 35, 44] used cohort data, four [38, 39, 41, 43] used administrative health data, and two studies each used government [32, 47] and/or commercial [36, 37] databases. Two studies used data from an opportunity sample [33, 48]. All the included studies relied on different sources of neighborhood data in addition to population data sources. Census data was the most commonly used data source for neighborhood-level data with twelve studies using this [26–31, 37–40, 45, 46]. Transport [27, 30, 35, 40, 45], business type [26, 30, 32, 43, 47], and satellite [29, 34, 42, 46] data were also used by multiple studies to create GIS measures of neighborhood contexts.
Sample/Population
Ten studies [26, 28–30, 34, 35, 38, 45–47] used a representative design. In addition, three studies used extremely large samples ranging from 160,000 to 570,645 [36, 38, 43], with two using diabetes registry data [38, 43], although these studies did not use representative designs. Twelve studies [26, 28, 29, 31–34, 39–41, 45, 47] had large samples ranging from 931 to 7,288 and eight [27, 30, 35, 37, 42, 44, 46, 48] used small samples ranging from 80 to 377.
Areal Units
Five studies used census tract or city neighborhood boundaries as the lowest areal unit of their analysis [32, 38, 42, 45, 47]. Eighteen studies [26–31, 33–37, 39–41, 43, 44, 46, 48] used residential addresses as the lowest areal unit, which required calculating single or multiple buffer areas around point data. Buffers refer to the specific areas within boundaries drawn depending on a given criteria, with boundaries typically applied based on distance, time, or relative to administrative boundaries. Where studies considered residential address as the lowest areal unit, network distances were used to calculate buffer boundaries. For example, how many healthcare centers could be reached by paths and/or roads in 500-meter or 10-minute walking time from residential address. One study additionally constructed straight-line radial buffers, which are calculated by measuring x-meters in every direction around an address, indicating “as the crow flies” distance without accounting for potential barriers [46]. One study also compared school versus home address [34] as the lowest areal unit around which to calculate buffers, and one considered the spatial extent of all adjacent postcodes as buffer boundaries [37]. Thirteen studies calculated multiple buffer areas in order to assess the relative importance of their exposures across different scales [26, 29, 31, 33–36, 38, 40, 41, 44, 46, 48], with 10 studies using a single buffer or an administratively defined areal unit [27, 28, 30, 32, 37, 39, 42, 43, 45, 47]. Multiple buffers were used to answer questions about the relative importance of proximal access to a given feature or resource, such as a community center, within 500-meter of a residential address compared to within 1,000-meter, or the importance of having x-amount of a given resource within 500-meter compared to 1,000 m.
Where buffer analysis was used to create boundaries around residential addresses that crossed administrative areas, studies estimated weights to account for areas overlapping pre-defined boundaries, such as census tract, to create estimated population levels based on area covered across each administrative boundary [27, 29, 38]. Buffers based on distances ranged from a low of 100-meter through to a high of just under 5,000-meter, with 500-metre buffers being the most commonly considered areal unit. Where buffers were calculated based on time [26, 29], buffers were calculated based on incremental increases to estimated walking time in bands of 4 or 5 min up to a maximum buffer considered of greater than 30-minute.
GIS Measures
114 unique GIS measures were identified across included studies, of which 78 were independently tested against stress and AL-related biomarkers. Of these 78 measures, 64 were measures of density (how much of a given resource within a given boundary) and 14 were measures of proximity (how far to specific resources in distance or time). Across these measurement types, broad themes existed in terms of what aspects of the neighborhood context were being explored, with 25 measuring greenspace, 24 GIS measures capturing aspects of built environment land-use, 19 assessing area-level demographics, and 10 the food environment.
GIS measures of greenspace captured: greenspace coverage [29, 32, 36, 42, 44, 48], number of accessible greenspaces [34]; greenspace variability [29]; greenspace quality [29]; the relative importance of proximal access to greenspace from school or residential address [34]; the distance to the nearest greenspace without a pre-defined boundary [34]; distance to public open spaces, defined as publicly owned spaces larger than 700-meter squared, with or without provision for recreational activities, including nature reserves [26]; and differences between perceived and objective distances to public open spaces [26] (see Table 2). One study created a composite index of diabetes risk, where high index values corresponded to socially deprived areas with low levels of greenspace [29]. The Normalized Difference Vegetation Index (NDVI) was the most frequently used measure of greenspace exposure, used by five studies [29, 36, 42, 44, 48], although it was not uniformly constructed (in terms of resolution or area) or considered (in terms of expected effect). NDVI has scores ranging between −1 and 1 with distinct boundaries for types of land cover and measures the difference between near-infrared bandwidths (NIR) and visible red (RED) bandwidths [40]. Negative values are likely to be water, scores close to zero are likely to be urban areas or grey-space (without green), and scores close to 1 are likely to be densely green. Two studies used a similar measure of Greenspace as NDVI defined using Light Detection and Ranging (LiDAR) [42, 48]. LIDAR is a remote sensing technology that uses laser light to generate three-dimensional information about the Earth’s surface, including vegetation among others. Using LIDAR one can obtain geo-referenced data of the tree-canopy and then estimate the proportion of space covered by this canopy, as well as data on their density and height. Land covered by green urban spaces [32]; land covered by sports facilities [32]; having a garden [34]; and the number of green spaces accessible within a given radius around the household or school [34]. In each case, higher levels of greenspace were predicted to be salutogenic, regardless of the outcome considered.
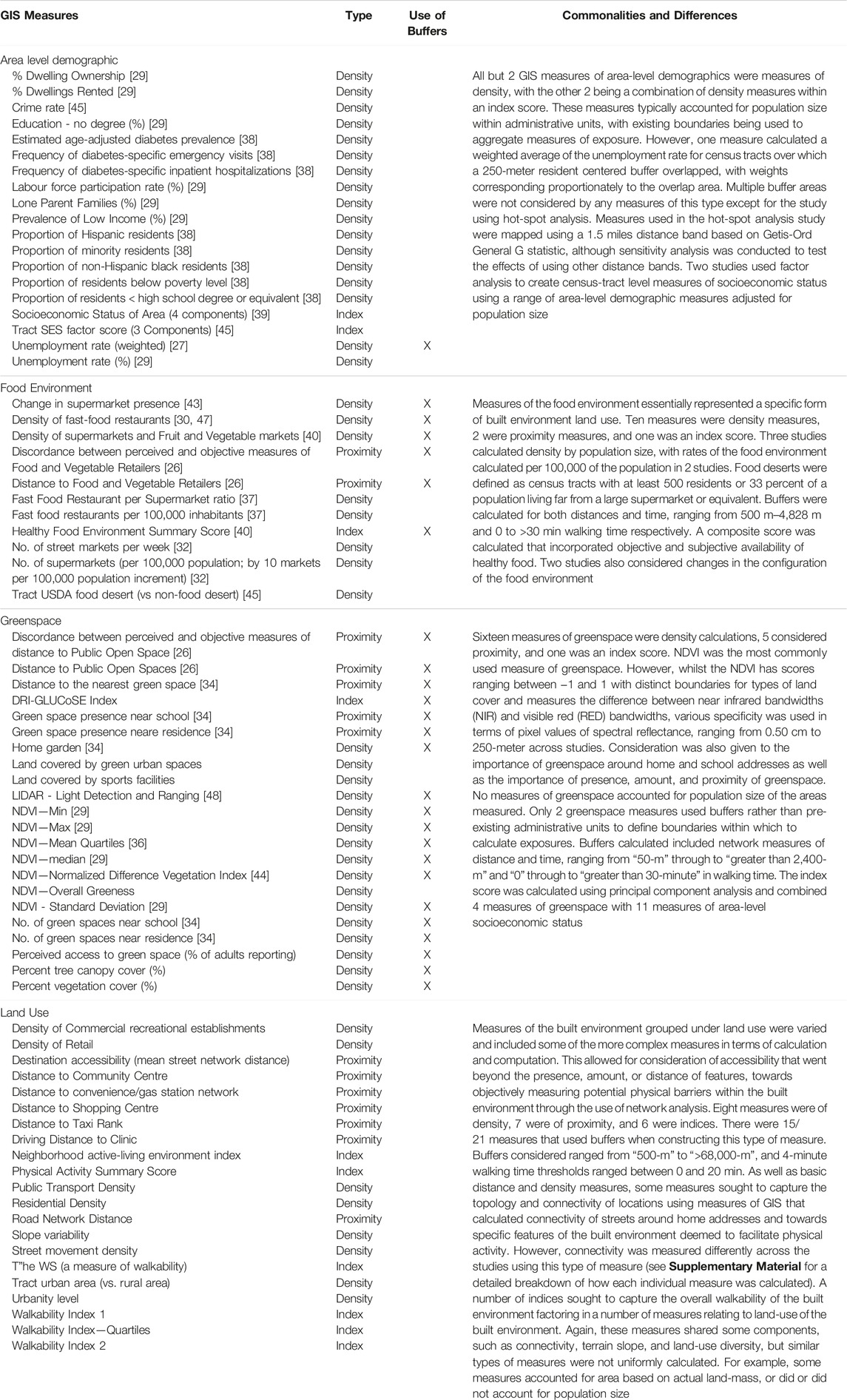
Table 2. Description of Geographic Information Systems measures (systematic review, worldwide, journal start-date-2022).
Area-level demographic density measures considered: crime [45]; education level [29, 38]; employment [27, 29]; ethnicity [38]; housing tenureship [29]; and socioeconomic status (SES) [29, 38, 39, 45]. All studies including area-level demographic density measures accounted for population levels, whereby the proportion of each measure was relative to population size across areas considered, such as county crime rate by 1,000 people. One study used hot-spot analysis (a spatial analysis technique used to assess whether high or low values cluster in a way that appears to be geographically patterned) to test the predictive ability of indirect measures against an HbA1c registry and found: diabetes-specific inpatient hospitalizations (accuracy: 89%); diabetes-specific emergency visits (90%), age-adjusted diabetes prevalence estimated from emergency department data (89%); and the proportion of minority residents (86%), as the highest-performing predictors compared to an HbA1c registry, with accuracy calculated as (true positives + true negatives)/all observations. Proportions of non-Hispanic black residents, residents below the poverty level, residents with less than a high school degree or equivalent, and Hispanic residents all had poorer (<80%) accuracy ratings using this approach [38].
Food environment measures sought to represent positive or negative exposures relating to food retailers available in an area. Supermarket presence [43], proximity to food and vegetable retailers, higher densities of street markets [32] and supermarkets [32, 37, 40, 43], and a composite index to measure the healthiness of the food environment which combined objective and perceived measures of healthy food access [40] were predicted to have beneficial effects on outcome measures, with fast food outlet density [30, 37, 47], discordance between perceived and objective distance to food and vegetable retailers [26], and food deserts [45] theorized to have negative effects on outcomes. Measures of land-use captured: public transport access [36]; access to commerce and recreation [36, 40]; urbanity-level [29, 45]; residential density [36]; area level physical accessibility [36]; distance to community centers [35]; distance to shopping centers [35]; distance to convenience stores [46]; distance to taxi ranks [35]; distance to healthcare [41]; and distance to population centers [33]. One measure assessed overall destination accessibility by calculating the average distance to schools, medical facilities, leisure, retail and places of worship within their defined buffer [36]. Six studies [28, 29, 31, 36, 40, 47] used multiple GIS measures to create an index, with included measures sometimes crossing the overarching sub-themes and measurement types. These indices sought to capture: walkable environments [28, 31, 36, 40, 47]; healthy food environments [40]; and diabetes risk [29].
Measuring Density With GIS
All but 2 [33, 41] of the 23 included studies used a GIS measure of density to assess the neighborhood context and the composition of the built environment. Density measures were calculated based on how much of a particular resource or feature there was relative to a given area [29, 30, 32, 34, 36, 40, 42–44, 47]; area and population [27, 29, 32, 37–39, 42, 45]; area, population, and time [32]; and area relative to another food environment feature [37, 45].
Measuring Proximity With GIS
Seven studies [26, 33–36, 41, 46] used a GIS proximity measure. All used road network buffers rather than radial buffers when calculating proximity measures. However, one study [46] also considered straight line (“as the crow flies”) distance. Unlike network distances, straight-line distances ignore any barriers (such as fencing/entry-points/motorways) that might exist between points. All studies using proximity measures used residential address as the start point from which to calculate distances to features of the neighborhood context, they theorised to impact their outcome. One study [34] also considered distances around the school in order to consider the impact of activity spaces around both the home and school environments of their sample of school-aged children. One study [26] first calculated distance, then estimated the walking time based on average walking speeds.
Outcome Measures: Biomarkers and Allostatic Load
Table 3 lists the 33 outcomes tested for an association with the GIS measures, indicating whether any significant (p < 0.05) associations were found or not for area-level demographic, food environment, greenspace, and land-use measures. Only two studies [34, 48] measured AL as an outcome and the biomarkers included within each measure of AL differed across the studies. Consequently, studies wishing to tease out the effects of GIS-measured neighborhood effects on AL may find this variation to be a barrier to effective interpretation of effects. Similarly, three [26, 32, 46] of the four studies [26, 30, 32, 46] that assessed the Metabolic Syndrome as an outcome conflated the included biomarkers into a composite measure obscuring individual biomarker relationships. However, these studies were included as several of the biomarkers used to measure Metabolic Syndrome, such as triglycerides, cholesterol, and hemoglobin A1c (HbA1c), are commonly used within measures of AL [49].
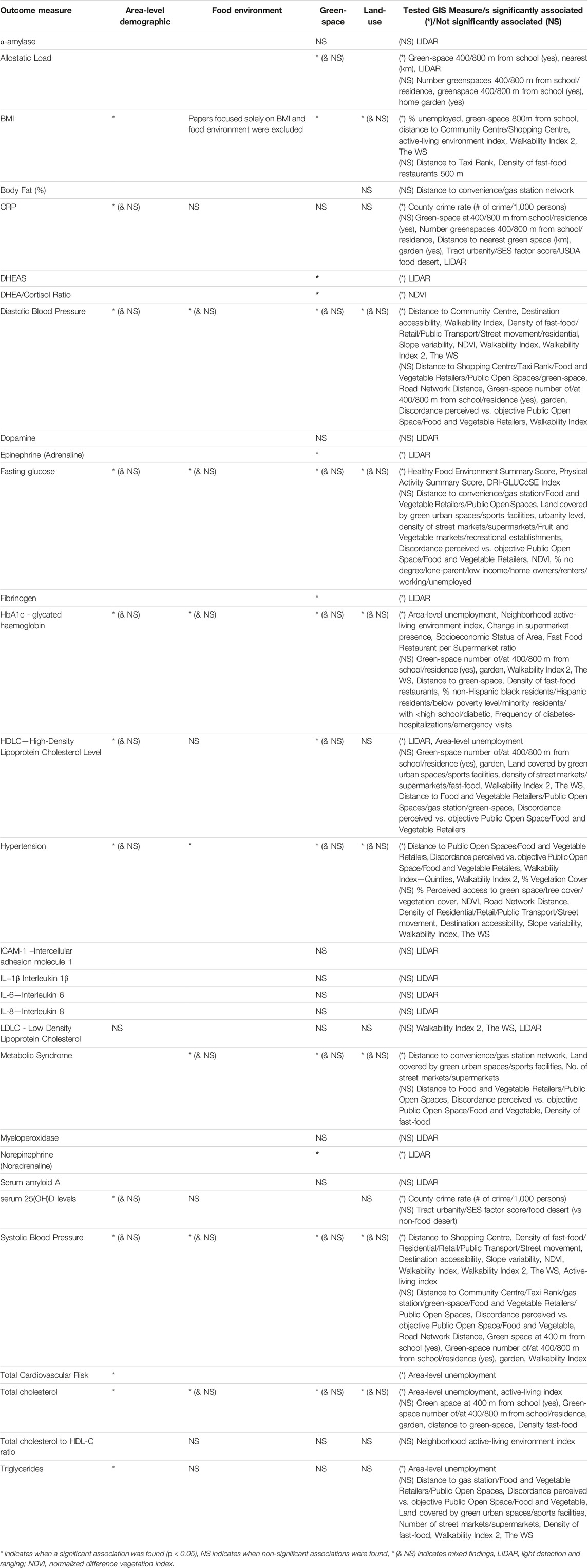
Table 3. Biomarker associations with Geographic Information Systems measures of the neighborhood context (systematic review, worldwide, journal start-date-2022).
Where associations with individual biomarkers were reported with a GIS measure: 9 studies included systolic blood pressure (SBP) [26, 28, 31, 33–36, 46, 47]; 9 HbA1c [28, 31, 33–36, 43, 46, 47]; 8 high-density-lipoprotein-cholesterol (HDL-C) [26, 27, 30–32, 34, 46, 48]; 7 diastolic blood pressure (DBP) [26, 31, 33–36, 47]; 6 triglycerides [26, 27, 30–32, 46]; 5 BMI [27, 28, 30, 31, 35]; 5 fasting glucose [26, 29, 32, 40, 46]; three waist circumference [26, 30, 32]; 3 C-Reactive Protein (CRP) [34, 45, 48]; three total cholesterol [27, 30, 34]; 2 low-density-lipoprotein-cholesterol (LDL-C) [31, 48]; 1 dehydroepiandrosterone sulfate (DHEAS) and DHEAS to cortisol ratio [44]; 1 serum 25(OH)D levels [45]; and 1 total cholesterol to HDL ratio [28]. A single study also reported associations with a GIS measure for: intercellular adhesion molecule 1 (ICAM-1); vascular cell adhesion molecule 1 (VCAM-1); interleukin-6; interleukin-8; interleukin-1β; myeloperoxidase; tumor-necrosis factor (TNF); serum amyloid A; uric acid; and α-amylase [48].
Assessment of Risk of Bias
The overall quality of evidence was found to be moderate-to-low quality for the purpose of assessing the relationships between neighborhood characteristics and AL. Six of the identified studies [26, 28, 31, 34, 36, 47] were rated as having a low risk of bias, eight demonstrated a moderate risk of bias [27, 29, 32, 35, 38, 40, 45, 46] and nine were determined to have a high risk of bias [30, 33, 37, 39, 41–44, 48]. As all study types were eligible for inclusion, a specific JBI appraisal tool was not available for all of the included studies. However, to assess each included study consistently the checklist for analytical cross-sectional studies appeared most suitable [25]. The main concerns for studies with a high risk of bias related to issues with sample size and sample selection relative to the analysis being undertaken. Other factors that led to moderate or high-risk scores included the lack of strategies being identified to deal with confounding factors, including classic issues in GIS research, such as date discrepancies between linked data, the modifiable areal unit problem (MAUP), the uncertain geographic context problem (UGCoP), and the issue of self-selection into neighborhoods.
Discussion
This systematic review was the first to consider how GIS has been used to measure relationships between access to the built environment and biomarkers of stress and AL, and to assess the quality of the existing evidence to address this question. It highlighted there is limited research in this area, with only 2 of the 23 included studies considering AL as an outcome directly. However, relationships between neighborhood attributes and relevant measures of the stress pathway were evident in this review, with findings pointing to this area being an interesting avenue for future research. For example, both studies that tested for an association between greenspace and AL, found greenspace impacted overall AL. Moreover, each tested associations at different scales using multiple buffers. This approach addresses two common issues in GIS research, described as the modifiable areal unit problem (MAUP) and the uncertain geographic context problem (UGCoP) [50]. The MAUP relates to the fact that the effects of area-based variables may be affected by the scales being used and ecological fallacy whereby group characteristics are ascribed incorrectly to individuals [50]. Whilst the UGCoP arises due to uncertainty surrounding what areas exert the most influence over individuals and uncertainty surrounding actual exposures to different contexts [50]. The UGCoP was particularly relevant in the Portuguese study, where they found a significant association between access to greenspace in the area around schools and AL, but not around the home address, for their school-aged sample. In this case, the school context appeared more important for the primary school-aged participants in terms of greenspace exposure and AL. Whilst few of the included studies explicitly addressed the MAUP and the UGCoP, the use of multiple buffers, sensitivity analysis, and studies that used longitudinal designs partially addressed these concerns. Whilst studies focused on GPS and accelerometer data were not retrieved and retained due to their individual level focus, measures calculated using this technique are argued to directly address concerns related to the UGCoP by tracking individual activity spaces. For example, this approach often centers analysis around the aspects of the built environment individuals actively engage with [51, 52]. This would be an interesting addition to the literature surrounding neighborhood access to the built environment and Allostatic Load, however, as the focus of this approach shifts from what features of the built environment are accessible at the neighbourhood level within a given space to how this space is used at a more individual level, studies of this type were not included.
The review highlights a lack of consistency in the GIS measures being used, with few studies using any of the same measures. However, broad themes were evident in terms of how measures were calculated (distance/density) and the aspects of the built environment the GIS measures sought to capture (area-level demographics, land-use, greenspace, and the food environment). Nevertheless, even where measures were ostensibly similar, such as with measures of walkability, land-use-mix, and NDVI, they were often calculated differently, whether by the collation of varied measures in indices, or by using different degrees of specificity in terms of raster imagery, buffer sizes, and/or weighting schemes, making comparisons difficult. These variations in construction may explain conflicting results across studies, but few studies have sought to directly compare NDVI with other measures of greenspace [53]. Nevertheless, differences in measures were often due to data availability, and in part reflects an advantage of using a GIS approach, in that a broader array of data sources can be brought together to deepen insight into the nature of how individuals are exposed to complex neighborhood environments. However, when different data sources are drawn together, there is the potential for a time lag between any measurement of exposure and outcome that may influence findings and interpretations, increasing the risk of bias. For example, Zhang et al. noted that the time interval between their calculation of change of supermarket presence and assessment of participant HbA1c ranged from 1 day up to 24 months. Given associations were short-lived and were not observed in long-difference regression models, this likely influenced results. As such, more work needs to be done to identify suitable techniques to manage analysis of disparate datasets collected over differing time-periods.
A noted strength of GIS measures relates to data quality and objective measurement. However, the inclusion of both objective and subjective measures in several studies also made it possible to consider the reliability of findings, and test the effectiveness of both GIS and subjective measures. For example, Baldock et al., found a subjective measure of perceived distance to healthy food environments was associated with increased hypertension risk [OR: 1.13 (CI: 1.02, 1.25), p. 0.005], but objective distance was not. However, combining this with the GIS measure made it possible to identify participants who overestimated distances, with this group having an increased risk of hypertension [OR:1.36 (CI: 1.02, 1.80) p. 0.034]. A plausible explanation for this is that people who overestimate distances may have factored in barriers to their estimation, which might be ignored by a simple objective measure of distance. As such, studies using GIS measures should consider subjective measures that might complement, expand on, and explain how access to the built environment may impact exposure to environmental stressors in greater detail (and vice versa).
Limitations
Owing to the highly varied language used surrounding GIS and the lack of consistency in how AL is conceptualized and measured [54], the broad range of search terms may still fail to pick up all of the relevant literature, particularly when combined with our exclusion criteria. For example, the decision to omit papers solely focused on BMI and not to include terms such as “GPS” and “Accelerometer” in our search terms likely impacted the types of exposures that were considered in terms of GIS measures. However, GIS measures centered on the use of Geographical Positioning System (GPS) devices tend to focus on the individual scale, rather than the effects of the neighborhood level which was the focus of this review. These types of measures have also typically been used to assess the relationship between characteristics of the built environment and activity spaces (e.g., physical exercise) [52, 55] which is the focus of a number of forthcoming systematic reviews listed on PROSPERO [56]. Nevertheless, the use of GPS tracking devices offers the opportunity to address common issues in GIS research, such as the UGCoP. Moreover, BMI is inconsistently included as a component of AL [54], the relationship between BMI and AL is not well understood [57], and the stress pathway was not expected to be central to the analysis in papers where BMI was the sole biomarker in retrieved studies. As such, we opted to continue to exclude BMI-specific papers despite the possible reduction in ability to identify some relevant literature using this type of measure. In addition, although this review is able to offer insights into how GIS measures have been used in AL research, because its focus was on the use of the methods the review is unable to speak to the effects or consequences of using different GIS measures.
Conclusion
GIS measures of neighborhood attributes have been widely used in the literature to assess relationships with biomarkers associated with stress. However, only two studies considered AL directly. As such, the quality of the evidence to assess associations between GIS measures of access to the built environment and AL suffered due to heterogeneity in both exposures and outcomes. This was largely due to the limited number of studies included which directly addressed issues relating to the stress pathway. However, measures seeking to capture access to features of the built environment such as greenspace, the food environment, area-level demographics, and land-use mix were found to influence relevant biomarkers associated with AL and the stress-pathway point to this area as an interesting avenue for future research. Moreover, several studies considered multiple areas of exposure and highlighted the complimentary influence GIS measures can offer to neighborhood effects research, particularly when used in conjunction with subjective measures.
Author Contributions
Conceptualization/protocol design: OC and SH. Literature searches/extraction/analysis: OC and SH. Initial manuscript preparation: OC and SH. Manuscript review and editing: OC and SH. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by the Soc-B Centre for Doctoral Training, which is funded by ESRC and BBSRC.
Conflict of Interest
The authors declare that they do not have any conflicts of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.ssph-journal.org/articles/10.3389/phrs.2024.1606624/full#supplementary-material
References
1. Deurzen, I, and Vanhoutte, B. A Longitudinal Study of Allostatic Load in Later Life: The Role of Sex, Birth Cohorts, and Risk Accumulation. Res Aging (2019) 41(5):419–42. doi:10.1177/0164027518813839
2. Marmot, M, Allen, J, Boyce, T, Goldblatt, P, Morrison, J, Marmot, M, et al. Health Equity in England: The Marmot Review 10 Years On. Institute of Health Equity (2020). https://www.health.org.uk/publications/reports/the-marmot-review-10-years-on
3. Diez Roux, AV, and Mair, C. Neighborhoods and Health. Ann N Y Acad Sci (2010) 1186:125–45. doi:10.1111/j.1749-6632.2009.05333.x
4. Godhwani, S, Jivraj, S, Marshall, A, and Bécares, L. Comparing Subjective and Objective Neighbourhood Deprivation and Their Association with Health over Time Among Older Adults in England. Health & place (2019) 55:51–8. doi:10.1016/j.healthplace.2018.10.006
5. Helbich, M, O’Connor, R, Nieuwenhuijsen, M, and Hagedoorn, P. Greenery Exposure and Suicide Mortality Later in Life: A Longitudinal Register-Based Case-Control Study. Environ Int (2020) 143:105982. doi:10.1016/j.envint.2020.105982
6. Deurzen, I, Rod, N, Christensen, U, Hansen, A, Lund, R, and Dich, N. Neighborhood Perceptions and Allostatic Load: Evidence from Denmark. Health & Place (2016) 40:1–8. doi:10.1016/j.healthplace.2016.04.010
7. Schulz, AJ, Mentz, G, Lachance, L, Johnson, J, Gaines, C, and Israel, BA. Associations between Socioeconomic Status and Allostatic Load: Effects of Neighborhood Poverty and Tests of Mediating Pathways. Am J Public Health (2012) 102(9):1706–14. doi:10.2105/AJPH.2011.300412
8. Fleckney, P, and Bentley, R. The Urban Public Realm and Adolescent Mental Health and Wellbeing: A Systematic Review. Soc Sci Med (2021) 284:114242. doi:10.1016/j.socscimed.2021.114242
9. Diez Roux, AV, Mujahid, MS, Hirsch, JA, Moore, K, and Moore, LV. The Impact of Neighborhoods on CV Risk. Glob Heart (2016) 11(3):353–63. doi:10.1016/j.gheart.2016.08.002
10. Murray, E, Nicholas, O, Norman, P, and Jivraj, S. Neighbourhood Deprivation Effects on Body-Mass index across the Life Course: Structural Equation Modelling of Data from Two Prospective British Longitudinal Birth Cohorts. The Lancet (2019) 394:90. doi:10.1016/s0140-6736(19)32887-9
11. Ige-Elegbede, J, Pilkington, P, Orme, J, Williams, B, Prestwood, E, Black, D, et al. Designing Healthier Neighbourhoods: A Systematic Review of the Impact of the Neighbourhood Design on Health and Wellbeing. null (2020) 6:1004–19. doi:10.1080/23748834.2020.1799173
12. Stafford, M, and Marmot, M. Neighbourhood Deprivation and Health: Does It Affect Us All Equally? Int J Epidemiol (2003) 32(3):357–66. doi:10.1093/ije/dyg084
13. Ham, M, Manley, D, Bailey, N, Simpson, L, and Maclennan, D. Neighbourhood Effects Research: New Perspectives. Berlin, Heidelberg: Springer (2012).
14. O׳Campo, P, Wheaton, B, Nisenbaum, R, Glazier, RH, Dunn, JR, and Chambers, C. The Neighbourhood Effects on Health and Well-Being (NEHW) Study. Health & Place (2015) 31:65–74. doi:10.1016/j.healthplace.2014.11.001
15. Prior, L, Manley, D, and Jones, K. Stressed Out? An Investigation of whether Allostatic Load Mediates Associations between Neighbourhood Deprivation and Health. Health Place. (2018) 52:25–33. doi:10.1016/j.healthplace.2018.05.003
16. Ribeiro, AI, Amaro, J, Lisi, C, and Fraga, S. Neighborhood Socioeconomic Deprivation and Allostatic Load: A Scoping Review. Int J Environ Res Public Health (2018) 15(6):1092. doi:10.3390/ijerph15061092
17. Sullivan, SM, Peters, ES, Trapido, EJ, Oral, E, Scribner, RA, and Rung, AL. Assessing Mediation of Behavioral and Stress Pathways in the Association between Neighborhood Environments and Obesity Outcomes. Prev Med Rep (2016) 4:248–55. doi:10.1016/j.pmedr.2016.06.012
18. Pearce, J, Witten, K, and Bartie, P. Neighbourhoods and Health: A GIS Approach to Measuring Community Resource Accessibility. J Epidemiol Community Health (2006) 60(5):389–95. doi:10.1136/jech.2005.043281
19. Huang, BX, Chiou, SC, and Li, WY. Accessibility and Street Network Characteristics of Urban Public Facility Spaces: Equity Research on parks in Fuzhou City Based on Gis and Space Syntax Model. Sustainability (Switzerland) (2020) 12(9):3618. doi:10.3390/su12093618
20. Park, YS, McMorris, BJ, Pruinelli, L, Song, Y, Kaas, MJ, and Wyman, JF. Use of Geographic Information Systems to Explore Associations between Neighborhood Attributes and Mental Health Outcomes in Adults: A Systematic Review. IJERPH (2021) 18(16):8597. doi:10.3390/ijerph18168597
21. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ (2021) 372:n71. doi:10.1136/bmj.n71
22. Guidi, J, Lucente, M, Sonino, N, and Fava, GA. Allostatic Load and its Impact on Health: A Systematic Review. Psychotherapy and psychosomatics (2021) 90(1):11–27. doi:10.1159/000510696
23. Jivraj, S, Murray, E, Norman, P, and Nicholas, O. The Impact of Life Course Exposures to Neighbourhood Deprivation on Health and Well-Being: A Review of the Long-Term Neighbourhood Effects Literature. Eur J Public Health (2020) 30(ue 5):922–8. doi:10.1093/eurpub/ckz153
24. CRD York. PROSPERO Registration (2023). Available from: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=348355 (Accessed July 14, 2023).
25. Joanna Briggs Institute. JBI. Critical Appraisal Tools (2021). Available from: https://jbi.global/critical-appraisal-tools (Accessed October 25, 2021).
26. Baldock, KL, Paquet, C, Howard, NJ, Coffee, NT, Taylor, AW, and Daniel, M. Are Perceived and Objective Distances to Fresh Food and Physical Activity Resources Associated with Cardiometabolic Risk? Int J Environ Res Public Health (2018) 15(2):224. doi:10.3390/ijerph15020224
27. Naimi, AI, Paquet, C, Gauvin, L, and Daniel, M. Associations between Area-Level Unemployment, Body Mass index, and Risk Factors for Cardiovascular Disease in an Urban Area. Int J Environ Res Public Health (2009) 6(12):3082–96. doi:10.3390/ijerph6123082
28. Hajna, S, Dasgupta, K, and Ross, NA. Laboratory-Assessed Markers of Cardiometabolic Health and Associations with GIS-Based Measures of Active-Living Environments. Int J Environ Res Public Health (2018) 15(10):2079. doi:10.3390/ijerph15102079
29. Walker, BB, Brinkmann, ST, Große, T, Kremer, D, Schuurman, N, Hystad, P, et al. Neighborhood Greenspace and Socioeconomic Risk Are Associated with Diabetes Risk at the Sub-neighborhood Scale: Results from the Prospective Urban and Rural Epidemiology (PURE) Study. J Urban Health (2022) 99(3):506–18. doi:10.1007/s11524-022-00630-w
30. Paquet, C, Dubé, L, Gauvin, L, Kestens, Y, and Daniel, M. Sense of Mastery and Metabolic Risk: Moderating Role of the Local Fast-Food Environment. Psychosomatic Med (2010) 72(3):324–31. doi:10.1097/PSY.0b013e3181cdf439
31. de Courrèges, A, Occelli, F, Muntaner, M, Amouyel, P, Meirhaeghe, A, and Dauchet, L. The Relationship between Neighbourhood Walkability and Cardiovascular Risk Factors in Northern France. Sci Total Environ (2021) 772:144877. doi:10.1016/j.scitotenv.2020.144877
32. Tsiampalis, T, Faka, A, Psaltopoulou, T, Pitsavos, C, Chalkias, C, and Panagiotakos, DB. The Relationship of the Built and Food Environments with the Metabolic Syndrome in the Athens Metropolitan Area: A Sex-Stratified Spatial Analysis in the Context of the ATTICA Epidemiological Study. Hormones (Athens) (2021) 20(4):723–34. doi:10.1007/s42000-021-00293-3
33. Hamano, T, Kimura, Y, Takeda, M, Yamasaki, M, Nabika, T, and Shiwaku, K. Is Location Associated with High Risk of Hypertension? Shimane COHRE Study. Am J Hypertens (2012) 25(7):784–8. doi:10.1038/ajh.2012.36
34. Ribeiro, AI, Tavares, C, Guttentag, A, and Barros, H. Association between Neighbourhood green Space and Biological Markers in School-Aged Children. Findings from the Generation XXI Birth Cohort. Environ Int (2019) 132:105070. doi:10.1016/j.envint.2019.105070
35. Malambo, P, De Villiers, A, Lambert, EV, Puoane, T, and Kengne, AP. The Relationship between Objectively-Measured Attributes of the Built Environment and Selected Cardiovascular Risk Factors in a South African Urban Setting. BMC Public Health (2018) 18(1):847. doi:10.1186/s12889-018-5772-3
36. Sarkar, C, Webster, C, and Gallacher, J. Neighbourhood Walkability and Incidence of Hypertension: Findings from the Study of 429,334 UK Biobank Participants. Int J Hyg Environ Health (2018) 221(3):458–68. doi:10.1016/j.ijheh.2018.01.009
37. Kahr, MK, Suter, MA, Ballas, J, Ramin, SM, Monga, M, Lee, W, et al. Geospatial Analysis of Food Environment Demonstrates Associations with Gestational Diabetes. Am J Obstet Gynecol (2016) 214(1):110.e1–9. doi:10.1016/j.ajog.2015.08.048
38. Lee, DC, Jiang, Q, Tabaei, BP, Elbel, B, Koziatek, CA, Konty, KJ, et al. Using Indirect Measures to Identify Geographic Hot Spots of Poor Glycemic Control: Cross-Sectional Comparisons with an A1C Registry. Diabetes Care (2018) 41(7):1438–47. doi:10.2337/dc18-0181
39. Geraghty, EM, Balsbaugh, T, Nuovo, J, and Tandon, S. Using Geographic Information Systems (GIS) to Assess Outcome Disparities in Patients with Type 2 Diabetes and Hyperlipidemia. J Am Board Fam Med : JABFM (2010) 23(1):88–96. doi:10.3122/jabfm.2010.01.090149
40. Christine, PJ, Auchincloss, AH, Bertoni, AG, Carnethon, MR, Sánchez, BN, Moore, K, et al. Longitudinal Associations between Neighborhood Physical and Social Environments and Incident Type 2 Diabetes Mellitus: The Multi-Ethnic Study of Atherosclerosis (MESA). JAMA Intern Med (2015) 175(8):1311–20. doi:10.1001/jamainternmed.2015.2691
41. Baumgardner, DJ, Halsmer, SE, Steber, DL, Shah, DS, and Mundt, MP. Does Proximity to Clinic Affect Immunization Rates and Blood Pressure? Int J Psychiatry Med (2006) 36(2):199–209. doi:10.2190/9N36-W446-194L-9KHW
42. Knobel, P, Kondo, M, Maneja, R, Zhao, Y, Dadvand, P, and Schinasi, LH. Associations of Objective and Perceived Greenness Measures with Cardiovascular Risk Factors in Philadelphia, PA: A Spatial Analysis. Environ Res (2021) 197:110990. doi:10.1016/j.envres.2021.110990
43. Zhang, YT, Mujahid, MS, Laraia, BA, Warton, EM, Blanchard, SD, Moffet, HH, et al. Association between Neighborhood Supermarket Presence and Glycated Hemoglobin Levels Among Patients with Type 2 Diabetes Mellitus. Am J Epidemiol (2017) 185(12):1297–303. doi:10.1093/aje/kwx017
44. Mancus, G, Cimino, AN, Hasan, MZ, Campbell, JC, Winch, PJ, Sharps, P, et al. Residential Greenness Positively Associated with the Cortisol to DHEA Ratio Among Urban-Dwelling African American Women at Risk for HIV. J Urban Health (2021) 98(4):570–8. doi:10.1007/s11524-020-00492-0
45. Chai, W, Fan, JX, and Wen, M. Association of Individual and Community Factors with C-Reactive Protein and 25-hydroxyvitamin D: Evidence from the National Health and Nutrition Examination Survey (NHANES). SSM - Popul Health (2016) 2:889–96. doi:10.1016/j.ssmph.2016.11.001
46. Dengel, DR, Hearst, MO, Harmon, JH, Forsyth, A, and Lytle, LA. Does the Built Environment Relate to the Metabolic Syndrome in Adolescents? Health Place (2009) 15(4):946–51. doi:10.1016/j.healthplace.2009.03.001
47. Li, F, Harmer, P, Cardinal, BJ, and Vongjaturapat, N. Built Environment and Changes in Blood Pressure in Middle Aged and Older Adults. Prev Med (2009) 48(3):237–41. doi:10.1016/j.ypmed.2009.01.005
48. Egorov, AI, Griffin, SM, Converse, RR, Styles, JN, Sams, EA, Wilson, A, et al. Vegetated Land Cover Near Residence Is Associated with Reduced Allostatic Load and Improved Biomarkers of Neuroendocrine, Metabolic and Immune Functions. Environ Res (2017) 158:508–21. doi:10.1016/j.envres.2017.07.009
49. Beese, S, Postma, J, and Graves, JM. Allostatic Load Measurement: A Systematic Review of Reviews, Database Inventory, and Considerations for Neighborhood Research. IJERPH (2022) 19(24):17006. doi:10.3390/ijerph192417006
50. Kwan, M. How GIS Can Help Address the Uncertain Geographic Context Problem in Social Science Research. Ann GIS (2012) 18(4):245–55. doi:10.1080/19475683.2012.727867
51. Boakye, KA, Amram, O, Schuna, JMJ, Duncan, GE, and Hystad, P. GPS-based Built Environment Measures Associated with Adult Physical Activity. Health Place (2021) 70:102602. doi:10.1016/j.healthplace.2021.102602
52. Fillekes, MP, Giannouli, E, Kim, EK, Zijlstra, W, and Weibel, R. Towards a Comprehensive Set of GPS-Based Indicators Reflecting the Multidimensional Nature of Daily Mobility for Applications in Health and Aging Research. Int J Health Geogr (2019) 18(1):17. doi:10.1186/s12942-019-0181-0
53. Rugel, EJ, Henderson, SB, Carpiano, RM, and Brauer, M. Beyond the Normalized Difference Vegetation Index (NDVI): Developing a Natural Space Index for Population-Level Health Research. Environ Res (2017) 159:474–83. doi:10.1016/j.envres.2017.08.033
54. McCrory, C, McLoughlin, S, Layte, R, NiCheallaigh, C, O’Halloran, AM, Barros, H, et al. Towards a Consensus Definition of Allostatic Load: A Multi-Cohort, Multi-System, Multi-Biomarker Individual Participant Data (IPD) Meta-Analysis. Psychoneuroendocrinology (2023) 153:106117. doi:10.1016/j.psyneuen.2023.106117
55. Katapally, TR, Bhawra, J, and Patel, P. A Systematic Review of the Evolution of GPS Use in Active Living Research: A State of the Evidence for Research, Policy, and Practice. Health & Place (2020) 66:102453. doi:10.1016/j.healthplace.2020.102453
56. PROSPERO. PROSPERO (2024). Available from: https://www.crd.york.ac.uk/prospero/#searchadvanced (Accessed January 5, 2024).
Keywords: allostatic load, geographic information systems, built environment, biomarker, GIS
Citation: Cranshaw O and Haworth S (2024) Neighborhood Access to the Built Environment and Allostatic Load: A Systematic Review of the Use of Geographic Information Systems. Public Health Rev 45:1606624. doi: 10.3389/phrs.2024.1606624
Received: 14 September 2023; Accepted: 08 May 2024;
Published: 23 May 2024.
Edited by:
Pedro Gullón, University of Alcalá, SpainReviewed by:
Two reviewers who chose to remain anonymousCopyright © 2024 Cranshaw and Haworth. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
PHR is edited by the Swiss School of Public Health (SSPH+) in a partnership with the Association of Schools of Public Health of the European Region (ASPHER)+
*Correspondence: Owen Cranshaw, bWMyMDQ5NUBlc3NleC5hYy51aw==
This Systematic Review is part of the PHR Special Issue “Neighbourhood Influences on Population Health”