 Maria Victoria Brunelli
Maria Victoria Brunelli Mariana Graciela Seisdedos2
Mariana Graciela Seisdedos2 Maria Maluenda Martinez
Maria Maluenda Martinez- 1Escuela de Enfermería, Facultad de Ciencias Biomedicas, Universidad Austral, Buenos Aires, Argentina
- 2Departamento de Calidad y Seguridad del Paciente, Hospital Universitario Austral, Buenos Aires, Argentina
Objectives: When adverse events (AE) occur, there are different consequences for healthcare professionals. The environment in which professionals work can influence the experience. This study aims to explore the experiences of second victims (SV) among health professionals in Argentina.
Methods: A phenomenological study was used with in-depth interviews with healthcare professionals. Audio recordings and verbatim transcriptions were analyzed independently for themes, subthemes, and codes.
Results: Three main themes emerged from the analysis: navigating the experience, the environment, and the turning point. Subthemes were identified for navigating the experience to describe the process: receiving the impact, transition, and taking action.
Conclusion: SVs undergo a process after an AE. The environment is part of this experience. It is a turning point in SVs’ professional and personal lives. Improving the psychological safety (PS) environment is essential for ensuring the safety of SVs.
Introduction
Global healthcare is threatened by a shortage of healthcare workers [1]. In 2023, the WHO warned that 55 countries have urgent needs for healthcare professionals [2] and developed the Global Health Workforce Strategy 2030. It suggests, among other actions, improving job security [3], both physically and psychologically, for healthcare personnel.
Psychological safety (PS) is defined as a work environment where team members engage in dialogue, express opinions, and request help [4]. Work relationships are perceived as supportive and trustworthy [4], and teamwork is encouraged [5, 6].
Moreover, PS is closely related to patient safety [4–6]. First, it promotes error reporting [4, 7]. Derickson et al. reported that 20% more professionals were willing to report an error in psychologically safe hospitals than in other hospitals [7]. Second, PS is an ally in the care of professionals involved in a safety incident–known as second victims (SVs) [8]. Various authors affirm that SV care programs in psychologically safe environments contribute to their recovery [8, 9].
In 2022, the European Researchers’ Network Working on Second Victims (ERNST) Consortium presented a consensus on the definition of SVs, integrating existing evidence and clarifying previous concepts proposed by Wu and Scott [10]. Thus, a SV is defined as any healthcare worker who experiences a negative impact from direct or indirect involvement in an unexpected AE, unintentional medical error, or patient injury [10]. They often feel responsible for the patient’s outcome and perceived failure [10]. The prevalence varies between 13% and 78% according to different studies [11–13]. They experience emotional, physical, and/or professional disturbances and may desire to abandon the profession [8, 11–17]. For instance, Potura et al. demonstrated that 30.4% of Austrian pediatric reports exhibited self-doubt, 26.1% experienced flashbacks in similar professional settings, and 25.6% exhibited insomnia or an excessive need for sleep [12]. Furthermore, posttraumatic stress [18–21], suicide attempts [13, 22], and substance abuse [23, 24] have also been reported.
In addition, SVs greatly benefit from supportive measures [11, 25]. This support stems from various sources, including colleagues [11], supervisors [26, 27], and organizational channels [25, 28]. Research indicates that the extent of impact is negatively correlated with the perceived level of support, highlighting an inverse relationship [26]. Similarly, the safety culture within which professionals operate is significantly linked to the distress experienced by SVs [29].
For two decades, studies have shown the relevance of the SV phenomenon, mainly in Asia [15, 28, 30–32], the United States [14, 27, 33], and Europe [8, 11–13, 18, 34–37]. In 2009, Scott described the recovery trajectory of SVs through a qualitative study conducted with healthcare professionals in the United States [38]. Several factors influence the experience, such as the relationship between the patient and caregiver, past clinical experiences, and any perceived connection [38], all of which are influenced by work and sociocultural contexts.
In the Latin American context, there is less evidence of the SV phenomenon. It has been observed some quantitative studies in Argentina [26, 39], Brazil [40], Chile [25, 41], Colombia [42], and Mexico [43]. These studies suggest that the SV phenomenon is not uncommon in Latin American countries. However, no qualitative studies have been conducted that have allowed for a deeper understanding of the experiences of SVs in this socioeconomic, labor, and cultural context. Therefore, the objective of this study was to explore the experiences of SVs among healthcare professionals in Argentina.
Methods
This phenomenological study was given access to the lived experience of healthcare professionals [44] who were involved in an AE to describe what the participants had in common regarding their SV experience [45]. The Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines [46] were used for this reporting.
Population
The participants were healthcare professionals directly involved in an AE. The inclusion criteria was they work in highly complex hospital. Professionals who were on leave of absence were excluded. The sampling was purposive, selecting typical cases related to the phenomenon and a heterogeneous sample in terms of the participants’ professions. A minimum of 5 participants [45] were enrolled until theoretical data saturation was reached.
Phenomenological studies also take into account the context or situation in which the experience is lived to find the common denominator among the participants [45]. The professionals in this study worked in a private hospital that prioritizes patient safety in its mission. The hospital has international quality and safety accreditations in healthcare practices, voluntary incident reporting, and conducts morbidity-mortality meetings. While protocols are in place for the first victim, at the time of the study, there were no formal protocols described for SVs.
Data Collection and Analysis
To access the participants, a professional who follows SVs as part of his job contacted the professionals and invited them to participate in the study. Those who agreed to participate were contacted by the principal investigator. Subsequently in-depth and semi structured face-to-face interviews were conducted using a developed question guide (Appendix). The questions were grouped into two main inquiries: “What was your experience as an SV?” and “What context or situation influenced your experience?” This approach aimed to elicit data that would lead to a description of the experience [45], thus facilitating an integrated understanding of the participants’ experiences.
The face-to-face interviews were audio recorded, and the data were transcribed verbatim, including field notes taken during the interviews.
Phenomenological studies typically involve two main movements: epoché and reduction [45]. Epoché is required to suspend personal beliefs [45]. Therefore, a written document was prepared beforehand to outline the researchers’ personal assumptions about the phenomenon being studied. The purpose of this step was to ensure the researchers were aware of their concepts and beliefs about the topic and to exclude them from the data analysis. In the second step, the researchers engaged in reflexivity with respect to the data [45] to capture the meaning of the experience. This process included delineating the quotations and units of meaning (codes) and determining the central theme for the units of meaning. Finally, in accordance with phenomenological requirements, all the themes were integrated into a particular structure [45].
ATLAS.ti version 22 software was used. Triangulation of the data analysis was performed by two researchers who independently analyzed the data. They met to discuss their initial codes and to identify commonalities in their analyses. Next, they reanalyzed the data individually and, in the subsequent joint session, agreed on the final emergent codes, organizing them into subthemes and themes. Finally, this analysis was presented to two other researchers for validation.
The study received approval from the Institutional Review Board (No. 19–017). All participants provided prior consent before participating in the interview sessions, which were conducted in person and lasted approximately 50 min each.
Results
Seven participants were interviewed, including individuals from various healthcare professions, such as nurses, physicians, and surgical technologists, with diverse specialties, including internal medicine, surgery, cardiology, and anesthesia. The time since the AE varied, ranging from 6 months to 10 years.
During the interview analysis, it was noted that despite the dynamic and personal nature of the SV experience, all participants went through a process within a specific context or environment. Subthemes and codes were identified within each of the three themes (Table 1).
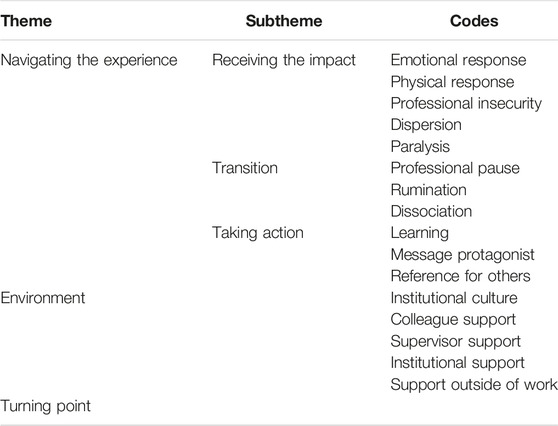
Table 1. Themes, subthemes and codes (Argentina, 2019).
Navigating the Experience
Navigating the experience encompasses the process that SVs go through. Three subthemes that make up this process delineate moments or stages: receiving the impact, transition, and taking action. Each subtheme includes various codes that define the states, actions, or characteristics of the participants. However, as noted above, the experience is dynamic and personal. Therefore, it is important to note that these moments are not rigid, and some codes are not limited to a single stage but may manifest across multiple stages or during the transition between them. Some quotes are shown in Table 2.
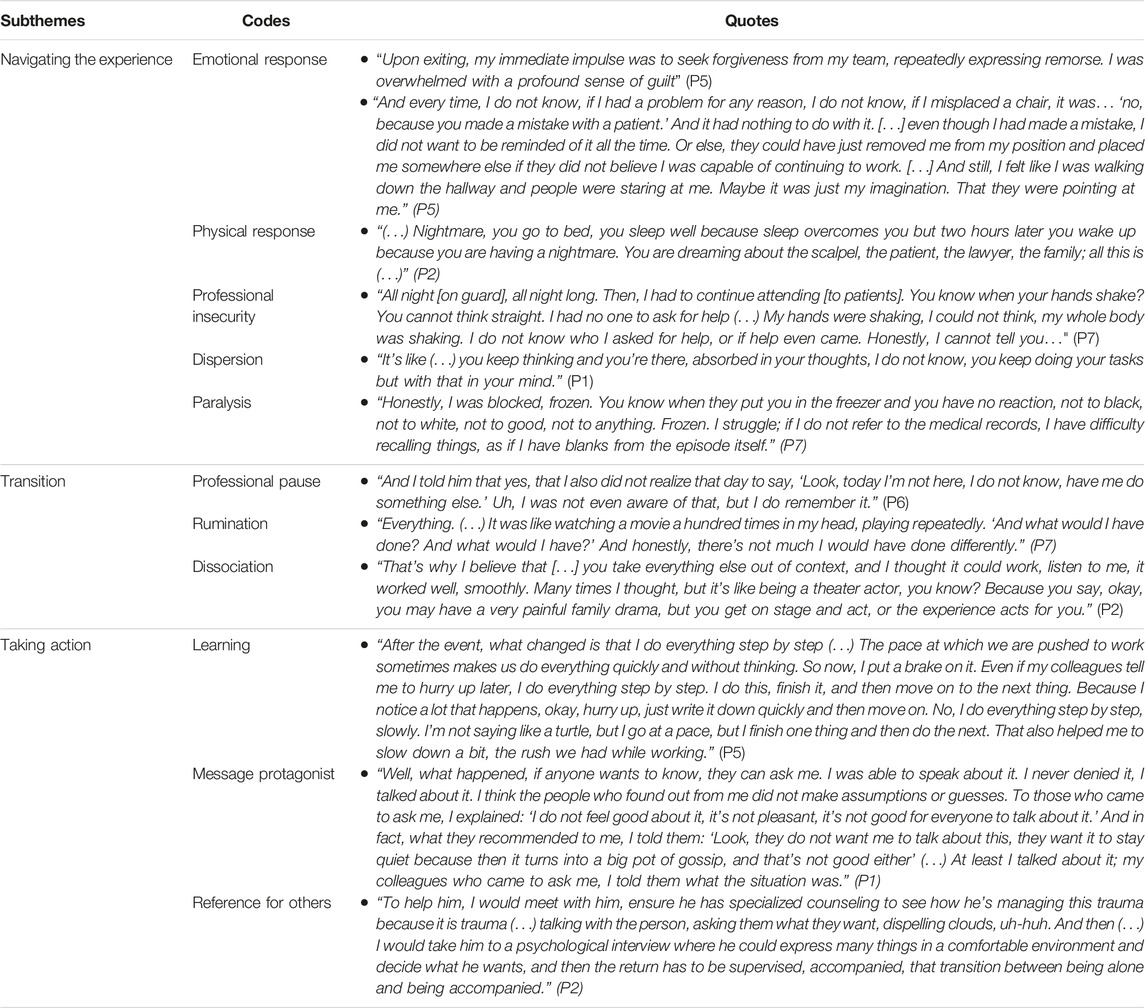
Table 2. Quotes of process (Argentina, 2019).
Receiving the Impact
The process begins when SVs express various emotions, thoughts, and experiences that indicate that they are receiving the impact. These expressions are often involuntary and intrusive.
The emotional response is a code of this initial stage. It involves the emotional state, which manifests as an emotional storm and is expressed as a manifestation of a number of simultaneous or nonsimultaneous emotions, without any one of them dominating, or when people find it difficult to name their emotions. For example, one participant expressed what he felt upon returning to work after the AE, stating, “It’s like being robbed at home and then going back in knowing the thief is not there, but it’s a feeling…" (P2). Terms such as “devastating, terrible, unforgettable, could not do anything, was stunned, or could not believe it” (P3) reflect the emotional state of the participants. In other cases, SVs are able to directly identify the emotion, using terms such as guilt, stigmatization and loneliness. Guilt emerges as a pervasive emotion among SVs. They struggle with feelings of culpability for the effects of the AE on the patient. In addition, SVs experience a sense of responsibility for their team, perceiving their inability to prevent the AE as a source of harm not only to the patient but also to the teamwork of their team. Additionally, perception of stigmatization the SVs perceive themselves as being scrutinized and judged, characterized by the label “you made a medical error” (P5). This phenomenon is particularly prevalent in the professional sphere but also extends to their family or social circles, where some professionals opt for silence out of fear of possible labeling or public exposure of their situation. Finally, feelings of loneliness are often present in SVs in response to a perceived lack of understanding of their environment.
Moreover, there are physical manifestations or consequences of receiving the impact. Participants mentioned cases of insomnia, nightmares, eating disorders, and even disease diagnoses, all of which are considered aftereffects of the traumatic event.
Furthermore, participants expressed a pervasive sense of professional insecurity. They harbor doubts about their ability to provide patient care, fear the possibility of repeating the error, and perceive themselves as inadequately equipped for their professional duties. These feelings persist not only in the immediate aftermath of the incident, when they are required to resume patient care, but also extends into the subsequent days and weeks following their return to the workplace.
Another code identified in this stage is dispersion. This code indicates that SVs demonstrated an inability to concentrate on tasks, making them more susceptible to new events.
Finally, another situation they experience when receiving the impact is paralysis, which hinders or prevents them from continuing with their tasks.
Transition
The transition state is characterized by the reactions that SVs exhibit as a means of coping with the situation. These include professional pauses, rumination, and dissociation.
A professional pause represents the desire to distance oneself from the environment in which the AE occurred.
In addition, SVs expressed that they experienced constant rumination in an intrusive and involuntary manner. This incessant rumination allowed them to replay, step-by-step, the actions they had taken before the AE. However, it also interfered with their ability to concentrate on other activities.
Finally, SVs may experience dissociation. Here, an analogy with a theater is drawn, comparing SVs with actors playing roles that are not real. In this way, the need to continue working does not allow them to acknowledge or express their feelings. Consequently, to continue their duties, they must assume a fictional persona because “the show must go on” (P7). At the same time, dissociation allows SVs to jump into action to persevere. This illustrates that some of the codes cannot be confined to a single moment in the process and that this is a dynamic process.
Taking Action
Taking action represents the final stage of the process. It encompasses the internal and/or external actions experienced by SVs that indicate movement toward exiting the situation.
This stage is characterized by actions aimed at remedying the situation, learning from the event, and contributing insights gained from their experience. The codes that comprise this stage include learning, being a messenger, and striving to be a role model for others.
Learning occurs at two levels. First, there are lessons related to the incident itself (within the work environment). Second, there are lessons related to the lives of the participants that can be translated into attitudes or values they will adopt in the future. For example, empathy, humanity, understanding, and support for colleagues are among the lessons that SVs share in their narratives.
In addition, SVs express a desire to be protagonists of the message. In doing so, they hoped to be the ones to communicate the event to those around them. They wanted to avoid the stigmatization they felt they were subjected to and the misinformation surrounding the event.
Finally, the participants want to serve as a reference for others, especially for those who may have a similar experience. SVs feel that the incident provides them with valuable experience.
Environment
The experience of SVs is significantly influenced by their surrounding environment, including both their workplace and personal domains. Various factors within the professional setting shape their experience, such as the institutional culture, support from colleagues and supervisors, and institutional backing. Meanwhile, in their personal lives, SVs may rely on support from family and friends. In both domains, the SV actively seek or passively receive support from individuals in their social circle. Table 3 shows some quotes related to the environment codes.
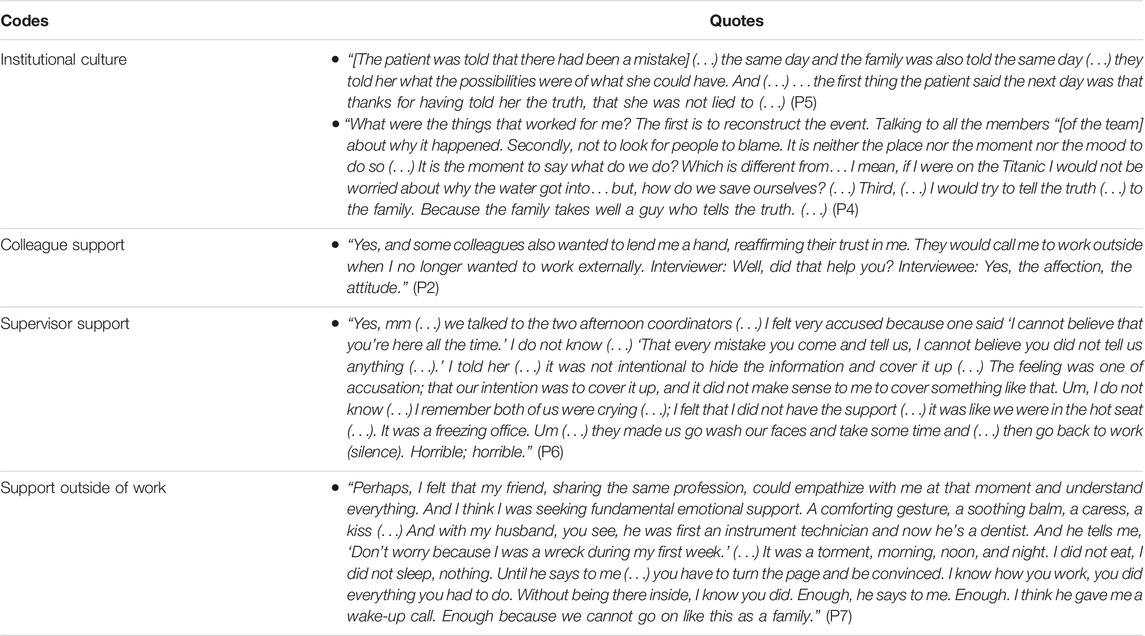
Table 3. Quotes of environment (Argentina, 2019).
The behaviors and responses of SV provide insight into the institutional culture in which they are embedded. In this regard, participants expressed an interest in prioritizing transparency in communication, not only among team members but also with patients and their families. Moreover, they sought to investigate the root causes of the AE, and in their speeches, the reporting of the event appears recurrently as a routine task they perform. In addition, the learning from the of experience that SVs expressed its a characteristics of a robust safety culture.
Colleague support played a crucial role in the SV experience. Some professionals viewed this support positively, especially when it reinforced their confidence in their professional abilities or when the team collectively assumed responsibility for the AE.
The SVs had varying perceptions of their supervisors’ responses. In some cases, support from supervisors was perceived as lacking in empathy and understanding toward them as individuals. The participants did not indicate whether supervisors sought to analyze how the AE occurred but rather emphasized how they felt they were treated. Some viewed demands to continue working or imperative instructions to avoid repeating a situation as negative support. However, others valued supervisors who show concern for their wellbeing.
In a secondary role, institutional support comes into play, expressed at times through information provided about the AE and the institutional management offered to SVs (e.g., legal support and professional support). Institutional support was seen as the backing of various individuals within the institution (fulfilling management, commercial, or legal roles) who, although not previously known to them, are felt by the SV as having supported them.
Finally, but equally significant, is the support outside of work sought by the SV. Some individuals look for support talking with their family or friends.
Turning Point
Ultimately, the study results showed that the AE marked a before and after moment in the professional lives of the participants; it was a turning point. On the one hand, terms such as ‘institutional proscription’ (P2), ‘it’s the end of my career’ (P2), and ‘it was the worst thing that happened to me in my career’ (P7) indicate that the SVs feel it is the end of their professional development. On the other hand, they use metaphors for natural disasters (such as earthquake, tsunami, upheaval). (Table 4).

Table 4. Turing Point quotes (Argentina, 2019).
Discussion
The professionals involved in an AE experience a pivotal moment in their personal and professional lives. They are going through a dynamic process influenced by their environment. PS is fundamental to the recovery of SVs.
The process consists of different stages that professionals go through. This journey is clear and distinct, yet at the same time unique and personal, as each participant may experience diverse ways of living through each stage in terms of intensity and the order in which different states occur. In a different cultural, social, and work context, Scott et al. identified stages in the recovery of SVs [38]. Although the stages found in this study are not identical to those presented by Scott, common characteristics can be identified. The environment plays a fundamental role in the recovery of SVs. When colleagues or supervisors do not provide support to professionals, coping becomes more difficult. As a result, communication and teamwork break down and PS is weakened [8].
As they experience the impact, they manifest an emotional storm that reflects not only an awareness of the gravity of the event but also a strong vocational sense. Precisely because the experience of the phenomenon and its impact are so profound, they cannot identify a single emotion but rather a mixture of them, and these emotions are sometimes contradictory. Similarly, Scott proposes emotional chaos [38] as the first stage, wherein professionals attempt to reflect on what occurred. Additionally, consistent with other studies [13, 17, 31], professionals exhibited profound guilt for the patient, expressing the professional commitment and responsibility they hold as a healthcare professional.
Negative feelings such as guilt and fear lead to the stigmatization experienced by professionals. It is important to consider that this stigma originates from the work environment (colleagues, supervisors, etc.) but also likely from the SVs themselves. That is, they feel the weight of their mistake, and it is highly possible that they will continue to reproach themselves for it, regardless of the reaction from their environment. In these cases, the attitudes of colleagues become even more important in mitigating stigmatization and fostering a psychologically safe environment for SVs [8, 47].
The loneliness experienced by professionals is closely linked to a lack of understanding or support in the work environment. Consistently, various studies have revealed a lack of empathy and understanding toward SVs [13, 19, 47]. Bass et al., in a quantitative study, argued that the majority of professionals reported not having received training in emotional strategies to support colleagues. However, these same participants had sought support from their colleagues when they were involved in an AE [19]. In this context, the experience of loneliness may be intensified by the expectation of increased empathy and support from individuals who have experienced similar adversity. Therefore, it is necessary to train professionals to provide emotional first aid. Undoubtedly, the implementation of these training programs contributes to psychologically safe work environments [4, 47, 48].
Professional pauses and rumination mark a transition stage in which professionals seem to need space for reflection to understand and analyze what happened and reflecting a significant impact of the AE on the SV. In these transitions appears that after the initial shock wears off, as SVs consciously or unconsciously seek strategies to navigate the event. In these sense, in many situations, work demands and brief times of attention to respond to economic imperatives, among others, clash with this need of SVs and consequently with patient safety. Conversely, when organizations promote PS interventions, such as debriefing spaces [11, 48], they have a significant impact on SVs [16].
Additionally, the learning process and the desire to offer recommendations (in clinical practice to prevent future AEs or for colleagues going through the same situation) indicate that SVs are taking action. Now, they can serve as a reference by making recommendations on how to handle SVs. This finding is similar to that of Scott et al. who, in their final stage [38], found that SVs had three possible final outcomes. One of them was able to give new meaning to the experience [38]. Also learning is an intervention that contributes to creating a psychologically safe environment [48] and facilitates the recovery of SVs [38].
Research into the environment is a constant concern in the recovery process of healthcare professionals encompassing both the workplace (institutional culture and support from colleagues, supervisors, and the institution) and extralaboral factors.
From the environment, the SVs expect to receive support from colleagues and supervisors. Peer support fosters teamwork, which is critical for patient safety and psychological safety [5]. They also expect their immediate superiors to demonstrate humanity, understanding, and support. If healthcare professionals are not supported by their colleagues and supervisors, they rarely perceive that they are in a psychologically safe environment. Consequently, they lack confidence, avoid dialogue, and refrain from expressing their opinions. This breakdown in communication and teamwork leads to a loss of PS [5, 6, 8].
Finally, the inclination to seek assistance from family or social circles underscores the SV’s aspiration to avoid judgment and find solace in environments characterized by stronger interpersonal bonds. This tendency may stem from the profound uncertainty engendered by the experience, prompting professionals to seek refuge in environments reminiscent of prevent normalcy. Additionally, this underscores the paramount importance of emotional support, as evidenced by the spontaneous expression of this theme by the majority of the participants, without direct questions about this aspect.
This study has several limitations. First, generalizing the findings may be limited due to the specific context in which the study was conducted. Additionally, while efforts were made to conduct comprehensive interviews, participants may have withheld or forgotten some of their experiences.
Despite these limitations, this study provides a comprehensive understanding of the experiences of SVs in a Latin American culture. These findings enables the implementation of actions aimed at strengthening the PS of the workplace. Specifically, educational interventions focused on improving teamwork through simulation and debriefing; promoting interproffessional communication, trust, and support for SVs; and designing institutional-level SV response programs involving colleagues, supervisors, patient safety committees, and legal entities are important actions for strengthening workplace PS. Furthermore, it highlights the need for further research to determine how psychologically safe environments contribute to SVs recovery.
In conclusion, SVs undergo a process following an AE that is influenced by the workplace environment. This experience represents a turning point not only in their professional lives but also in their personal lives.
Ethics Statement
The studies involving humans were approved by the Comité Institucional de Evaluación, Universidad Austral. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author Contributions
All authors contributed to the article and approved the submitted version. MB, MG conducted the interviews. MB, MG and MM did the analysis. MB, MM and MG wrote the manuscript.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The authors declare that this publication received APC funding from The Swiss School of Public Health (SSPH+). The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Conflict of Interest
The authors declare that they do not have any conflicts of interest.
References
1. The Lancet Global, H. Health-Care Workers Must Be Trained and Retained. Lancet Glob Health (2023) 11(5):e629. doi:10.1016/s2214-109x(23)00172-9
2. World Health Organization. WHO Health Workforce Support and Safeguards List (2023). Available from: https://www.who.int/publications/i/item/9789240069787 (Accessed March 24, 2024).
3. World Health Organization. Global Strategy on Human Resources for Health: Workforce 2030 (2016). Available from: https://www.who.int/publications/i/item/9789241511131 (Accessed March 24, 2024).
4. Kumar, S. Psychological Safety: What It Is, Why Teams Need It, and How to Make It Flourish. Chest (2023) 165(4):942–9. doi:10.1016/j.chest.2023.11.016
5. Arad, D, Finkelstein, A, Rozenblum, R, and Magnezi, R. Patient Safety and Staff Psychological Safety: A Mixed Methods Study on Aspects of Teamwork in the Operating Room. Front Public Health (2022) 10:1060473. doi:10.3389/fpubh.2022.1060473
6. Han, JH, and Roh, YS. Teamwork, Psychological Safety, and Patient Safety Competency Among Emergency Nurses. Int Emerg Nurs (2020) 51:100892. doi:10.1016/j.ienj.2020.100892
7. Derickson, R, Fishman, J, Osatuke, K, Teclaw, R, and Ramsel, D. Psychological Safety and Error Reporting Within Veterans Health Administration Hospitals. J Patient Saf (2024) 11(1):60–6. doi:10.1097/PTS.0000000000000082
8. Nijs, K, Seys, D, Coppens, S, Van De Velde, M, and Vanhaecht, K. Second Victim Support Structures in Anaesthesia: A Cross-Sectional Survey in Belgian Anaesthesiologists. Int J Qual Health Care (2021) 33(2):mzab058. doi:10.1093/intqhc/mzab058
9. Merandi, J, Liao, N, Lewe, D, Morvay, S, Stewart, B, Catt, C, et al. Deployment of a Second Victim Peer Support Program: A Replication Study. Pediatr Qual Saf (2017) 2(4):e031. doi:10.1097/pq9.0000000000000031
10. Vanhaecht, K, Seys, D, Russotto, S, Strametz, R, Mira, J, Sigurgeirsdóttir, S, et al. An Evidence and Consensus-Based Definition of Second Victim: A Strategic Topic in Healthcare Quality, Patient Safety, Person-Centeredness and Human Resource Management. Int J Environ Res Public Health (2022) 19(24):16869. doi:10.3390/ijerph192416869
11. Marung, H, Strametz, R, Roesner, H, Reifferscheid, F, Petzina, R, Klemm, V, et al. Second Victims Among German Emergency Medical Services Physicians (SeViD-III-Study). Int J Environ Res Public Health (2023) 20(5):4267. doi:10.3390/ijerph20054267
12. Potura, E, Klemm, V, Roesner, H, Sitter, B, Huscsava, H, Trifunovic-Koenig, M, et al. Second Victims Among Austrian Pediatricians (SeViD-A1 Study). Healthcare (2023) 11(18):2501. doi:10.3390/healthcare11182501
13. Magaldi, M, Perdomo, JM, Lopez-Baamonde, M, Chanza, M, Sanchez, D, and Gomar, C. Second Victim Phenomenon in a Surgical Area: Online Survey. Rev Esp Anestesiol Reanim Engl Ed (2021) S0034-9356:30320–0. doi:10.1016/j.redar.2020.11.009
14. Burlison, J, Scott, S, Browne, E, Thompson, S, and Hoffman, J. The Second Victim Experience and Support Tool: Validation of an Organizational Resource for Assessing Second Victim Effects and the Quality of Support Resources. J Patient Saf (2017) 13(2):93–102. doi:10.1097/PTS.0000000000000129
15. Choi, EY, Pyo, J, Lee, W, Jang, SG, Park, YK, Ock, M, et al. Nurses’ Experiences of Patient Safety Incidents in Korea: A Cross-Sectional Study. BMJ Open (2020) 10(10):e037741. doi:10.1136/bmjopen-2020-037741
16. Klemm, V, Rösner, H, Bushuven, S, and Strametz, R. The Second Victim Phenomenon-What Personnel in Anesthesiology Should Know About It. Anaesthesiologie (2023) 72(11):803–8. doi:10.1007/s00101-023-01337-6
17. Busch, IM, Moretti, F, Purgato, M, Barbui, C, Wu, AW, and Rimondini, M. Psychological and Psychosomatic Symptoms of Second Victims of Adverse Events: A Systematic Review and Meta-Analysis. J Patient Saf (2020) 16(2):e61–74. doi:10.1097/PTS.0000000000000589
18. Wahlberg, Å, Andreen Sachs, M, Johannesson, K, Hallberg, G, Jonsson, M, Skoog Svanberg, A, et al. Post-Traumatic Stress Symptoms in Swedish Obstetricians and Midwives After Severe Obstetric Events: A Cross-Sectional Retrospective Survey. BJOG: Int J Obstet Gynaecol (2017) 124(8):1264–71. doi:10.1111/1471-0528.14259
19. Baas, MAM, Scheepstra, KWF, Stramrood, CAI, Evers, R, Dijksman, LM, and Van Pampus, MG. Work-Related Adverse Events Leaving Their Mark: A Cross-Sectional Study Among Dutch Gynecologists. BMC Psychiatry (2018) 18(1):73. doi:10.1186/s12888-018-1659-1
20. Kerkman, T, Dijksman, LM, Baas, MAM, Evers, R, van Pampus, MG, and Stramrood, CAI. Traumatic Experiences and the Midwifery Profession: A Cross-Sectional Study Among Dutch Midwives. J Midwifery Womens Health (2019) 64(4):435–42. doi:10.1111/jmwh.12946
21. Kruper, A, Domeyer-Klenske, A, Treat, R, Pilarski, A, and Kaljo, K. Secondary Traumatic Stress in Ob-Gyn: A Mixed Methods Analysis Assessing Physician Impact and Needs. J Surg Educ (2021) 78(3):1024–34. doi:10.1016/j.jsurg.2020.08.038
23. Van Gerven, E, Vander Elst, T, Vandenbroeck, S, Dierickx, S, Euwema, M, Sermeus, W, et al. Increased Risk of Burnout for Physicians and Nurses Involved in a Patient Safety Incident. Med Care (2016) 54(10):937–43. doi:10.1097/mlr.0000000000000582
24. Stehman, CR, Testo, Z, Gershaw, RS, and Kellogg, AR. Burnout, Drop Out, Suicide: Physician Loss in Emergency Medicine, Part I. West J Emerg Med (2019) 20(3):485–94. doi:10.5811/westjem.2019.4.40970
25. Kappes, M, Delgado-Hito, P, Contreras, VR, and Romero-García, M. Prevalence of the Second Victim Phenomenon Among Intensive Care Unit Nurses and the Support provided by Their Organizations. Nurs Crit Care (2023) 28(6):1022–30. doi:10.1111/nicc.12967
26. Brunelli, MV, Estrada, S, Celano, C, Bandriwskyj, C, Riquelme, RJ, Ortega, A, et al. Second Victim Experience and Support From Health Professionals. Medicina (2023) 83(6):918–26.
27. Burlison, JD, Quillivan, RR, Scott, SD, Johnson, S, and Hoffman, JM. The Effects of the Second Victim Phenomenon on Work-Related Outcomes: Connecting Self-Reported Caregiver Distress to Turnover Intentions and Absenteeism. J Patient Saf (2021) 17(3):195–9. doi:10.1097/pts.0000000000000301
28. Mok, WQ, Chin, GF, Yap, SF, and Wang, W. A Cross-Sectional Survey on Nurses' Second Victim Experience and Quality of Support Resources in Singapore. J Nurs Manag (2020) 28(2):286–93. doi:10.1111/jonm.12920
29. Quillivan, RR, Burlison, JD, Browne, EK, Scott, SD, and Hoffman, JM. Patient Safety Culture and the Second Victim Phenomenon: Connecting Culture to Staff Distress in Nurses. Jt Comm J Qual Patient Saf (2016) 42(8):377–86. doi:10.1016/s1553-7250(16)42053-2
30. Luk, LA, Lee, FKI, Lam, CS, Soh, Y, Wong, YYM, and Lui, WSW. Healthcare Professional Experiences of Clinical Incident in Hong Kong: A Qualitative Study. Risk Manag Healthc Pol (2021) 14:947–57. doi:10.2147/rmhp.s292875
31. Cho, DB, Lee, W, Cha, JM, Kim, JH, Kim, J, Kang, SB, et al. Second Victim Experience and Perception Discordance of the Colonoscopic Perforation. Dig Dis Sci (2022) 67(7):2857–65. doi:10.1007/s10620-021-07107-x
32. Pyo, J, Choi, EY, Lee, W, Jang, SG, Park, YK, Ock, M, et al. Physicians' Difficulties Due to Patient Safety Incidents in Korea: A Cross-Sectional Study. J Korean Med Sci (2020) 35(17):e118. doi:10.3346/jkms.2020.35.e118
33. Finney, RE, Torbenson, VE, Riggan, KA, Weaver, AL, Long, ME, Allyse, MA, et al. Second Victim Experiences of Nurses in Obstetrics and Gynaecology: A Second Victim Experience and Support Tool Survey. J Nurs Manage (2021) 29(4):642–52. doi:10.1111/jonm.13198
34. Gómez-Durán, EL, and Arimany-Manso, J. Healthcare Professional as Second Victim in Healthcare Injuries. Med Clin (Barc) (2020) 154(3):98–100. doi:10.1016/j.medcli.2019.09.005
35. Carrillo, I, Tella, S, Strametz, R, Vanhaecht, K, Panella, M, Guerra-Paiva, S, et al. Studies on the Second Victim Phenomenon and Other Related Topics in the Pan-European Environment: The Experience of ERNST Consortium Members. J Patient Saf Risk Manage (2022) 27(2):59–65. doi:10.1177/25160435221076985
36. Vanhaecht, K, Seys, D, Schouten, L, Bruyneel, L, Coeckelberghs, E, Panella, M, et al. Duration of Second Victim Symptoms in the Aftermath of a Patient Safety Incident and Association With the Level of Patient Harm: A Cross-Sectional Study in the Netherlands. BMJ Open (2019) 9(7):e029923. doi:10.1136/bmjopen-2019-029923
37. Van Gerven, E, Deweer, D, Scott, SD, Panella, M, Euwema, M, Sermeus, W, et al. Personal, Situational and Organizational Aspects That Influence the Impact of Patient Safety Incidents: A Qualitative Study. Rev Calid Asist (2016) 31(Suppl. 2):34–46. doi:10.1016/j.cali.2016.02.003
38. Scott, SD, Hirschinger, LE, Cox, KR, McCoig, M, Brandt, J, and Hall, LW. The Natural History of Recovery for the Healthcare Provider "Second Victim" After Adverse Patient Events. Qual Saf Health Care (2009) 18(5):325–30. doi:10.1136/qshc.2009.032870
39. Brunelli, MV, Estrada, S, and Celano, C. Cross-Cultural Adaptation and Psychometric Evaluation of a Second Victim Experience and Support Tool (SVEST). J Patient Saf (2021) 17(8):e1401–e1405. doi:10.1097/pts.0000000000000497
40. Sordi, LPD, Lourenção, DCDA, Gallasch, CH, and Baptista, PCP. The Second Victim Experience: Cross-Cultural Adaptation of an Instrument for the Brazilian Context. Revista Gaúcha de Enfermagem (2022) 43:e20210010. doi:10.1590/1983-1447.2022.20210010.en
41. Mallea Salazar, F, Ibaceta Reinoso, I, and Vejar Reyes, C. Second Victims: Perceived Support Quality and Its Relationship With the Consequences of the Adverse Event. J Healthc Qual Res (2022) 37(2):117–24. doi:10.1016/j.jhqr.2021.09.002
42. Flórez, F, López, L, and Bernal, C. Prevalence of Adverse Events and Their Manifestations in Health Professionals as Second Victims. Biomedica (2022) 42(1):184–95. doi:10.7705/biomedica.6169
43. Jiménez, FEY, Alayola, SA, Mancebo, HA, and Campos, CM. Eventos adversos y burnout en profesionales de una clínica de atención primaria. Rev CONAMED (2018) 23(2):66–72.
44. Van Manen, M. Writing in the Dark: Phenomenological Studies in Interpretive Inquiry. New York: Routledge (2016).
46. Tong, A, Sainsbury, P, and Craig, J. Consolidated Criteria for Reporting Qualitative Research (COREQ): A 32-Item Checklist for Interviews and Focus Groups. Int J Qual Health Care (2007) 19(6):349–57. doi:10.1093/intqhc/mzm042
47. O'Meara, S, D'Arcy, F, Dowling, C, and Walsh, K. The Psychological Impact of Adverse Events on Urology Trainees. Ir J Med Sci (2023) 192(4):1819–24. doi:10.1007/s11845-022-03202-8
48. O'Donovan, R, and McAuliffe, E. A Systematic Review Exploring the Content and Outcomes of Interventions to Improve Psychological Safety, Speaking up and Voice Behaviour. BMC Health Serv Res (2020) 20(1):101. doi:10.1186/s12913-020-4931-2
Appendix: Second Victim Question Guide
What was your experience as an SV?
What was your participation in the event/How did you feel about your participation?
What was the outcome of the event for the patient?
Do you remember how you felt immediately after the event?
Did you have any needs (emotional, physical, professional)?
Did you express or tell anyone about these needs, and did you receive a response?
If you had a response: What response did you get, from whom, and did the response meet your need?
Did you express a need that was not met at the time? What happened to it?
Do you think the incident had an impact on your professional life? Did anything change in you? What? How?
If you perceive a change: Do you think this change is good, bad, or neutral?
On a professional level, when you returned to see patients after the incident, did you feel different (sometimes people feel fear, insecurity, embarrassment, inability to continue seeing patients, desire not to return to work)? Did this happen to you? Have you experienced any other feelings related to your professional performance that we have not discussed?
Can you identify three feelings or emotions you experienced at the time? How long did they last?
What context or situation influenced your experience?
How did you perceive your colleagues’ reactions? How did this reaction affect you (did it create positive or negative feelings?) Were you able to express it to them?
If you discussed the incident with a supervisor/coordinator or boss: How did you perceive your supervisor’s reaction to you? How did this reaction affect you (did it create positive or negative feelings?) Were you able to express it to them?
If you could go back in time, how would you have liked to have been treated by your colleagues? And by your supervisor/boss/coordinator?
Do you think the work environment would be different for you today? If so, how? Why do you think this change has occurred? How do you perceive it?
Do you highlight any behavior that was useful to you at the time?
If you are worried or stressed about a work-related problem, how do you usually handle this type of situation?
Whom do you usually turn to for advice or support in work-related situations?
Keywords: psychological safety, second victim, healthcare workers, patient safety incidents, patient safety
Citation: Brunelli MV, Seisdedos MG and Maluenda Martinez M (2024) Second Victim Experience: A Dynamic Process Conditioned by the Environment. A Qualitative Research. Int J Public Health 69:1607399. doi: 10.3389/ijph.2024.1607399
Received: 18 April 2024; Accepted: 30 May 2024;
Published: 13 June 2024.
Edited by:
Andrea Madarasova Geckova, University of Pavol Jozef Šafárik, SlovakiaReviewed by:
Two reviewers who chose to remain anonymousCopyright © 2024 Brunelli, Seisdedos and Maluenda Martinez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maria Victoria Brunelli, dmJydW5lbGxAYXVzdHJhbC5lZHUuYXI=
This Original Article is part of the IJPH Special Issue “Psychological Safety in Healthcare Settings”