 Nadia Sourial1,2*
Nadia Sourial1,2* Jean-Baptiste Beuscart3Łukasz Posłuszny4Matthieu Calafiore5Sónia S. Sousa6Esther Sansone7Marcelina Zuber8Isabelle Vedel9,10 COVERAGE Collaborative Group
Jean-Baptiste Beuscart3Łukasz Posłuszny4Matthieu Calafiore5Sónia S. Sousa6Esther Sansone7Marcelina Zuber8Isabelle Vedel9,10 COVERAGE Collaborative Group- 1Department of Health Management, Evaluation and Policy, School of Public Health, University of Montreal, Montreal, QC, Canada
- 2The University of Montreal Hospital Research Centre (CRCHUM), Montreal, QC, Canada
- 3Faculty of Medicine, Centre Hospitalier Universitaire Lille, University of Lille, Lille, France
- 4Department of Sociology, University of Wroclaw, Wroclaw, Poland
- 5Department of Family Medicine, University of Lille, Lille, France
- 6Psychological Neuroscience Laboratory, CIPsi, School of Psychology, University of Minho, Braga, Portugal
- 7Espace de Réflexion Éthique Régional des Hauts-de-France, University of Lille, Lille, France
- 8Department of Sociology, University of Wrocław, Wroclaw, Poland
- 9Department of Family Medicine, McGill University, Montreal, QC, Canada
- 10Lady Davis Institute, Jewish General Hospital, Montreal, QC, Canada
Introduction
Older vulnerable adults (OVA) are among the populations that interact the most with the healthcare system. Vulnerability in older adults has been broadly defined as the combination of frailty, “a clinically recognizable state in which older people’s ability to cope with daily or acute stressors,” and precarity, which “refers to insecurities and risks in the context of economic and social change, the hazards of contemporary life” [1].
Recruiting OVA can present particular challenges given their physical, cognitive, social (cultural, socioeconomic, language barriers) and political vulnerabilities [2] and are often excluded from research [3–5]. While general recommendations exist in addressing recruitment challenges in older adults [2, 6] and in hard-to-reach populations [7], there is a lack of methodological guidance specific to the recruitment of OVA whether it be in the context of quantitative or qualitative research. We collaborated with 26 international experts and researchers in aging from five countries (France, Italy, Poland, Lithuania, Portugal, Canada), part of an international research consortium on the care experiences of OVA [1], to highlight evidence-based solutions to meet these challenges. Consultations with experts were conducted through 27 workshops, including three 2-day in-person meetings organized Vulnerâge chair at the University of Lille and 24 virtual meetings between 2021 and 2023. A range of research projects involving the recruitment of OVA was discussed including a mix of quantitative (e.g., observational, quasi-experimental) and qualitative studies (e.g., descriptive, analytical). We chose to focus and highlight common challenges across these designs and across countries. A core group from the consortium, who are main authors of this article, synthesized the common challenges and proposed evidence-based solutions. This preliminary set of recommendations was then sent to the broader consortium for revision and validation. This manuscript includes an overview of three specific challenges and proposed solutions for the recruitment of OVA in research: finding the right recruitment process to foster representativeness, facilitating informed consent and promoting retention. A table of recommandations is also provided for easy use (Table 1).
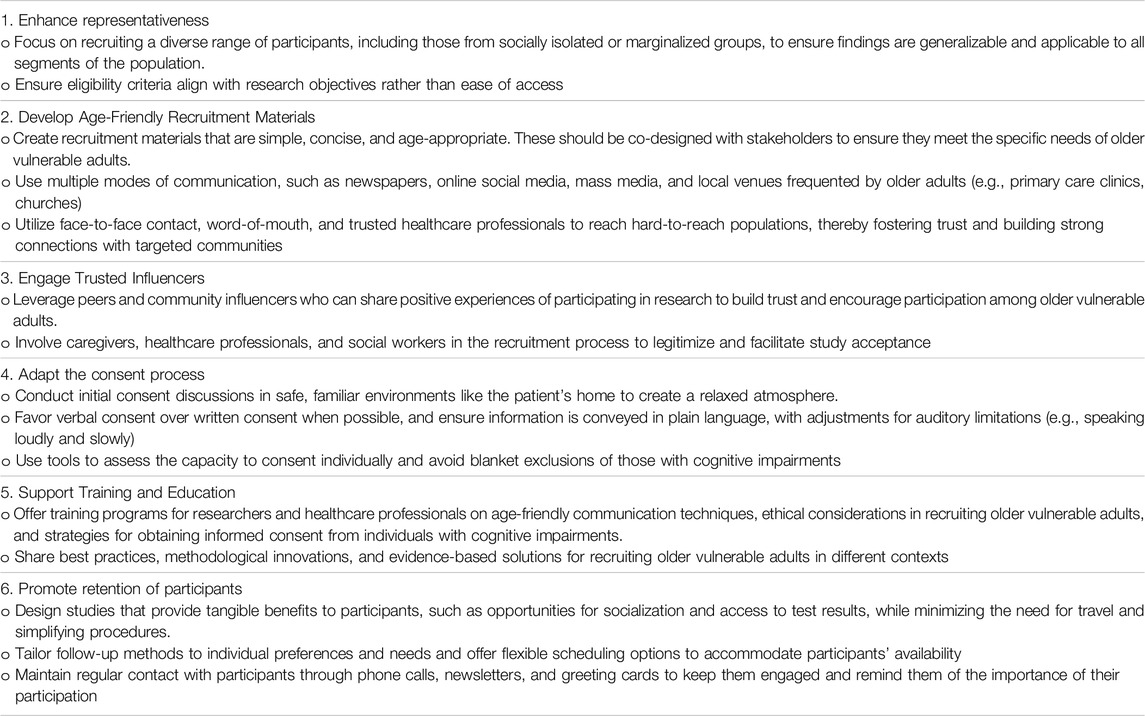
Table 1. Recommendations to facilitate the recruitment of older vulnerable adults in research based on best practices and COVERAGE Collaborative Group discussion meetings in Lille, France, year 2023–2024.
Finding the Right Recruitment Process to Foster Representativeness
It is usually of interest to take into account OVA’s diversity (e.g., very old age, socially isolated, rural, ethnicity, languages, education), type of care (e.g., home care) in order to explore a wide range of experiences or needs [5, 8] It may be tempting to exclude hard-to-reach populations such as highly vulnerable and marginalized OVA (e.g., homeless, cognitively impaired). However, to foster representativeness, it is crucial that recruitment focus on the target population, eligibility criteria and research objectives [6] rather than easiness to reach.
Providing clear and understandable information about the study which is accessible to all OVA is another critical issue during the recruitment phase given their health and social vulnerabilities [6]. Recruitment requires an “age friendly” approach by recruiters, in which communication should be appropriately adapted to the needs of OVA [9] including the content, style, and approach [6]. In addition, caregivers and healthcare professionals, staff (e.g., nursing homes) might resist recruiting more vulnerable older patients [2].
Several solutions have been proposed in the literature [9–11]. For instance, messages should be age-appropriate and drafted with stakeholders [11], and need to be in short and explicit paper format [2, 10]. Multiple modes of communication should also be considered, such as newspapers, online social media, and mass media that have their own benefits and risks. For example, recruiting OVA through mass email lists will be insufficient to capture the segment of OVA that are less likely to participate or who do not have access to technology [10]. The recruitment strategy should also focus on local venues where older people usually go (e.g., primary care clinics, church) [5]. Peers may also be leveraged as influencers and can share their positive perceptions in participating in research [9]. Finally, recruitment of hard-to-reach populations is most efficient if done by face-to-face contact, word-of-mouth, families or by known and trusted healthcare professional [5, 10] in order to convey reassurance, trustworthiness and develop strong connections with targeted communities. It is thus key to involve and educate resource people (healthcare professionals, social workers, relatives, etc.) in the field in order to help facilitate and legitimize acceptance of the study [9, 11].
Facilitating Informed Consent
Informed consent is particularly difficult for OVA as it strongly influences social relationships and can feel threatening for individuals who may fear losing health services if they refuse to participate [12]. In addition, ensuring informed consent for very vulnerable OVA such as those with cognitive disorders is particularly challenging [13]. Blanket exclusion of those with cognitive impairment is to be avoided [6]. Instead, decisions regarding the capacity to consent should be based on an individual basis [6].
The literature proposes several potential solutions to address challenges which are specific to OVA [13]. First and foremost, first encounters by researchers should ideally happen in a safe place and relaxed atmosphere such as the patient’s home [11]. When possible, verbal consent should be favored over signed consent which tends to generate more concerns among OVA [12]. In addition to ensuring information is conveyed in an appropriate and plain language, care should be taken to speak loudly and slowly where patients have auditory limitations [2]. Time should be taken to explain and repeat the purpose of the study, how the study will be conducted and how results will be kept safe and confidential [2]. Informed consent for OVA with cognitive impairment is particularly challenging [14, 15]. It is important to note that informed consent can often still be obtained for persons at mild and moderate stages of dementia while, consent by a legal representative may be considered for more advanced stages to ensure that the decision to participate or not is based on the person’s wishes and preferences. Using tools to assess the capacity to consent is therefore an essential component in recruiting OVA for research [14, 15].
Promoting Retention
Retention is usually an important challenge for longitudinal studies with OVA who are prone to fatigue, cognitive impairment, disabilities, illness or sensory limitations [2, 16]. Research teams should plan a variety of strategies to facilitate recruitment and retention. Designing studies that maximises the benefit/burden ratio can help with recruitment and retention [16] such as providing opportunity for socialization, access to test results [2, 16] and minimizing travel [16, 17]. Finally, regular “keep in touch” calls and mailings (i.e., newsletters and greeting cards) have been shown to increase retention [17].
Conclusion
In conclusion, recruitment methods need to be adapted to consider the particular physical, mental and social aspects of OVA. In this context, it is key to reflect on these challenges inherent to the recruitment and consenting process to promote representativeness and retention. Table 1 proposes a summary of the recommendations to address these challenges. These recommendations demonstrate the need to consider and incorporate a variety of methods to help ensure that recruitment is adapted to OVA’s needs and reality, leading to richer and more meaningful research results. While this study focused on recruitment challenges common across designs and jurisdictions, future research could consider a more in-depth analysis of design-specific challenges and contextual differences between countries given the different legal frameworks, healthcare systems, and research infrastructure.
Author Contributions
NS, IV, JB-B, ŁP, MC, SS, ES, and MZ contributed to the design of the manuscript, literature review, and writing of the manuscript. The COVERAGE collaborative group contributed to the identification of methodological challenges and the development of solutions. All authors contributed to the article and approved the submitted version.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. Fonds de recherche du Québec-Santé, Canadian Institutes of Health Research, Grant from the European Union (H2020). Sponsors had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Conflict of Interest
The authors declare that they do not have any conflicts of interest.
Acknowledgments
Acknowledgement of collaborative authorship: The members of the COVERAGE Collaborative Group are: Raminta Bardauskienė, Paweł Czajkowski, Paula Cristina Soares Encarnação, Olivieri Fabio, Anabela Silva Fernandes, Diego Pinal Fernandez, Agata Katkonien, Maria Manuela Pereira Machado, Carla Di Martino, Christine Moroni, Barbara Pabjan, Anna Aluffi Pentini, Fernando Alberto Soares Petronilho, Jolanta Pivoriene, Philippe Sabot, Adriana Teodorescu, and Irena Zemaitaityte. We would like to thank Audrey Plante for her assistance in editing and formatting the manuscript.
References
1. Sabot, P, Di Martino, C, Moroni, C, Pentini, AA, Pabjan, B, Machado, MMP, et al. Reconsidering Frailty From a Human and Social Sciences Standpoint: Towards an Interdisciplinary Approach to Vulnerability. Age and Ageing (2023) 52(5):afad064. doi:10.1093/ageing/afad064
2. Strotmeyer, ES, Arnold, AM, Boudreau, RM, Ives, DG, Cushman, M, Robbins, JA, et al. Long-Term Retention of Older Adults in the Cardiovascular Health Study: Implications for Studies of the Oldest Old. J Am Geriatr Soc (2010) 58(4):696–701. doi:10.1111/j.1532-5415.2010.02770.x
3. Van Spall, HG, Toren, A, Kiss, A, and Fowler, RA. Eligibility Criteria of Randomized Controlled Trials Published in High-Impact General Medical Journals: A Systematic Sampling Review. JAMA (2007) 297(11):1233–40. doi:10.1001/jama.297.11.1233
4. Helfand, BK, Webb, M, Gartaganis, SL, Fuller, L, Kwon, C-S, and Inouye, SK. The Exclusion of Older Persons From Vaccine and Treatment Trials for Coronavirus Disease 2019—Missing the Target. JAMA Intern Med (2020) 180(11):1546–9. doi:10.1001/jamainternmed.2020.5084
5. Liljas, AE, Walters, K, Jovicic, A, Iliffe, S, Manthorpe, J, Goodman, C, et al. Strategies to Improve Engagement of ‘Hard to Reach’Older People in Research on Health Promotion: A Systematic Review. BMC Public Health (2017) 17(1):349–12. doi:10.1186/s12889-017-4241-8
6. Goodwin, VA, Low, MSA, Quinn, TJ, Cockcroft, EJ, Shepherd, V, Evans, PH, et al. Including Older People in Health and Social Care Research: Best Practice Recommendations Based on the INCLUDE Framework. Age and Ageing (2023) 52(6):afad082. doi:10.1093/ageing/afad082
7. Aliyas, Z, Collins, PA, Chrun-Tremblay, S, Bayram, T, and Frohlich, KL. “Hard-To-Reach” or Hardly Reaching? Critical Reflections on Engaging Diverse Residents From Low Socio-Economic Status Neighborhoods in Public Health Research. Int J Public Health (2023) 67:1605296. doi:10.3389/ijph.2022.1605296
8. Levy, C, Zimmerman, S, Mor, V, Gifford, D, Greenberg, SA, Klinger, JH, et al. Pragmatic Trials in Long-Term Care: Implementation and Dissemination Challenges and Opportunities. J Am Geriatr Soc (2022) 70(3):709–17. doi:10.1111/jgs.17698
9. Meekes, WMA, Ford, C, and Stanmore, EK. Recruitment and Retention of Older Adults in Assisted Living Facilities to a Clinical Trial Using Technology for Falls Prevention: A Qualitative Case Study of Barriers and Facilitators. Health Soc Care Community (2021) 29(5):1296–307. doi:10.1111/hsc.13170
10. Chatters, R, Newbould, L, Sprange, K, Hind, D, Mountain, G, Shortland, K, et al. Recruitment of Older Adults to Three Preventative Lifestyle Improvement Studies. Trials (2018) 19(1):121. doi:10.1186/s13063-018-2482-1
11. O'Regan, A, García Bengoechea, E, Clifford, AM, Casey, M, Gallagher, S, Glynn, L, et al. How to Improve Recruitment, Sustainability and Scalability in Physical Activity Programmes for Adults Aged 50 Years and Older: A Qualitative Study of Key Stakeholder Perspectives. PLoS One (2020) 15(10):e0240974. doi:10.1371/journal.pone.0240974
12. Balard, F, Corre, SPL, Trouvé, H, Saint-Jean, O, and Somme, D. Exploring Representations and Experiences of Case-Management Users: Towards Difficulties and Solutions to Leading Qualitative Interviews With Older People With Complex Living Conditions. Qual Prim Care (2013) 21(4):229–35.
13. Shepherd, V. Advances and Challenges in Conducting Ethical Trials Involving Populations Lacking Capacity to Consent: A Decade in Review. Contemp Clin Trials (2020) 95(106054):106054. doi:10.1016/j.cct.2020.106054
14. Pennington, C, Davey, K, Ter Meulen, R, Coulthard, E, and Kehoe, PG. Tools for Testing Decision-Making Capacity in Dementia. Age and ageing (2018) 47(6):778–84. doi:10.1093/ageing/afy096
15. Grenier, A, O’Connor, D, James, K, Imahori, D, Minchopoulos, D, Velev, N, et al. Consent and Inclusion of People Living With Dementia (PLWD) in Research: Establishing a Canadian Agenda for Inclusive Rights-Based Practices. Can J Aging/La Revue canadienne du vieillissement. (2024) 1–8. doi:10.1017/S0714980824000217
16. Mody, L, Miller, DK, McGloin, JM, Freeman, M, Marcantonio, ER, Magaziner, J, et al. Recruitment and Retention of Older Adults in Aging Research. J Am Geriatr Soc (2008) 56(12):2340–8. doi:10.1111/j.1532-5415.2008.02015.x
Keywords: recruitment, challenges, older adults, vulnerability, equity
Citation: Sourial N, Beuscart J-B, Posłuszny Ł, Calafiore M, Sousa SS, Sansone E, Zuber M, Vedel I and COVERAGE Collaborative Group (2024) Challenges and Solutions in Recruiting Older Vulnerable Adults in Research. Int J Public Health 69:1607247. doi: 10.3389/ijph.2024.1607247
Received: 05 March 2024; Accepted: 08 July 2024;
Published: 30 July 2024.
Edited by:
Nino Kuenzli, Swiss Tropical and Public Health Institute (Swiss TPH), SwitzerlandReviewed by:
Victoria Shepherd, Cardiff University, United KingdomRebecca Amati, University of Italian Switzerland, Switzerland
Copyright © 2024 Sourial, Beuscart, Posłuszny, Calafiore, Sousa, Sansone, Zuber, Vedel and COVERAGE Collaborative Group. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nadia Sourial, bmFkaWEuc291cmlhbEB1bW9udHJlYWwuY2E=