 Stefan Kohler1,2*†
Stefan Kohler1,2*† Till Bärnighausen1†
Till Bärnighausen1† Patrick Kazonda3†Germana H. Leyna4†Julia Lohmann1,5†
Patrick Kazonda3†Germana H. Leyna4†Julia Lohmann1,5† Japhet Killewo4†
Japhet Killewo4† Julia K. Rohr6†Laura-Marie Stieglitz1†
Julia K. Rohr6†Laura-Marie Stieglitz1† Nicolas Paul1†
Nicolas Paul1†- 1Heidelberg Institute of Global Health, Faculty of Medicine and University Hospital, Heidelberg University, Heidelberg, Germany
- 2Institute of Social Medicine, Epidemiology and Health Economics, Charité – Universitatsmedizin Berlin, Corporate Member of Freie Universitat Berlin and Humboldt-Universitat zu Berlin, Berlin, Germany
- 3Dar es Salaam Urban Cohort Study, Dar es Salaam, Tanzania
- 4Department of Epidemiology and Biostatistics, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania
- 5Department of Global Health and Development, London School of Hygiene and Tropical Medicine, London, United Kingdom
- 6Harvard Center for Population and Development Studies, Harvard University, Cambridge, MA, United States
Objectives: Chronic conditions and multimorbidity affect care needs and prevention opportunities.
Methods: We studied 2,246 men and women aged ≥40 years within the Dar es Salaam Urban Cohort Study from June 2017 to July 2018. Seventeen chronic conditions were assessed based on self-report, body and blood pressure measurement, blood tests, and screening instruments.
Results: Hypertension (51.3%), anemia (34.1%), obesity (32.2%), diabetes (31.6%), depressive symptoms (31.5%), low grip strength (21.2%), and ischemic heart disease (11.9%) were widespread. Multimorbidity was common (73.7%). Women had higher odds of obesity, ischemic heart disease, and high cholesterol (adjusted OR: 2.08–4.16) and lower odds of underweight, low grip strength, alcohol problems, and smoking (adjusted OR: 0.04–0.45). Ten years of age were associated with higher odds of low grip strength, cognitive problems, hypertension, kidney disease, chronic cough, diabetes, high cholesterol, ischemic heart disease, and multimorbidity (adjusted OR: 1.21–1.81) and lower odds of HIV infection (adjusted OR: 0.51).
Conclusion: We found a higher prevalence of multimorbidity than previously estimated for middle-aged and elderly people in sub-Saharan Africa. The chronic conditions underlying multimorbidity differed by sex.
Introduction
Sub-Saharan Africa has been experiencing an epidemiological transition with a shift in the disease burden from infectious diseases to non-communicable diseases [1–3]. Health systems in this region face the challenge to care for rising levels of non-communicable diseases, still high levels of infectious diseases, and combinations thereof [1, 2]. Aggravating this health system challenge, the population aged ≥65 years in Africa has been predicted to grow from 48 million in 2021 to 569 million in 2100 [4, 5].
In a meta-analysis of 39 studies on low-income and middle-income countries, including 15 studies of five different datasets from sub-Saharan African countries, the estimated pooled prevalence of multimorbidity of non-communicable diseases was 36.4% (95% CI: 32.2–40.6) with a large variation from 0.7% to 81.3% between studies. The prevalence of multimorbidity of non-communicable diseases tended to be higher for the aged, women, people who were well-off, and urban dwellers [6]. Another meta-analysis of multimorbidity of communicable and non-communicable conditions estimated a pooled prevalence of 37.2% (95% CI: 34.9–39.4) globally based on 126 studies from 54 countries and 28.2% (95% CI: 15.6–40.8) for sub-Saharan Africa based on 10 studies [7]. The study conjectured that the low pooled prevalence estimated for sub-Saharan Africa could result from high levels of undiagnosed chronic illness [7].
Previous studies assessing the prevalence of multimorbidity in sub-Saharan Africa were often conducted in South Africa [6–10]. South Africa is one of the few upper middle income countries in the region and maintained an average upper middle income level since 2004 [11]. Studies in Tanzania reported a prevalence of multimorbidity of 25.3% [12], 61.1% [13], and 73.8% (95% CI: 71.2–76.3) for women only [14] among ≥40-year-olds assessing eight, 13, and 15 chronic conditions, respectively, in the same population as this study. A study among ≥60-year-olds in rural Tanzania found a multimorbidity prevalence of 26.1% (95% CI: 16.7–35.4) based on self-report of chronic conditions and 67.3% (95% CI: 57.0–77.5) based on clinical assessment, screening tools, and blood pressure measurement [15]. Another study in Tanzania and Uganda reported a multimorbidity prevalence of 25.6% among people living with HIV, diabetes, and/or hypertension [16]. None of these previous studies of multimorbidity in sub-Sahara Africa reported the prevalence of multimorbidity and underlying conditions by sex and age.
In this study, we evaluated 17 communicable and non-communicable health conditions among ≥40-year-old men and women living in two peri-urban wards of Dar es Salaam, Tanzania. First, we estimated the prevalence of chronic conditions and multimorbidity. Second, we assessed the relationships of chronic conditions and multimorbidity with sex and age.
Methods
Study Design and Setting
Tanzania transitioned from a low-income country to a lower middle-income country in 2019 based on the estimated gross national income per capita [11]. Dar es Salaam is Tanzania’s largest city and among its wealthier regions. We conducted a cross-sectional study between June 2017 and July 2018 among the peri-urban dwellers living in the Ukonga and Gongolamboto wards of Dar es Salaam. The neighboring Ukonga and Gongolamboto wards are located about 20 km from the city center, were densely populated, and had a mixture of well-built houses and mud houses. Most households had a toilet and about half had electricity [17]. The study was part of the “Health and Aging in Africa: Longitudinal Studies in Three INDEPTH Communities” (HAALSI) project [18].
Study Population
We randomly selected a sex-stratified sample of 4,850 individuals (2,450 men and 2,400 women) aged ≥40 years from the 2016 Dar es Salaam Health and Demographic Surveillance System, which is also known as the Dar es Salaam Urban Cohort Study (DUCS) [17]. Half of the study sample was randomly selected for additional point-of-care blood tests. Of the individuals selected for the study, 2,299 (744 men and 1,555 women) agreed to participate in a survey and non-invasive health measurement; 1,024 (318 men and 706 women) agreed to undergo additional blood testing. Reasons for non-participation in the survey and non-invasive measurements included unsuccessful attempts to reach a selected participant at home and lack of time to participate. Reasons for not agreeing to blood testing included concerns about confidentiality, the invasiveness of the requested procedures, and religious reasons.
After removing records with missing socioeconomic characteristics, the final study sample comprised up to 2,246 participants for the survey and non-invasive measurements and up to 1,014 participants for blood testing. The analyzed study sample underrepresented men (718 of 2,246; 32.0%) in comparison to the 2016 DUCS population aged ≥40 years (9,067 of 16,898, 54.7%; p < 0.001). In the sex-stratified study sample, the share of men aged 40–54 years was lower and the share of men aged ≥55 years was higher than in the 2016 DUCS population (p < 0.001). The shares of women aged 40–44 years, 50–54 years, or 70–74 years were lower and the shares of women aged 45–49 years or 55–70 years were higher in the study sample than in the 2016 DUCS population (p = 0.002) (Supplementary Table S1; Supplementary Figures S1, S2).
Data Collection
Field researchers visited study participants at home to conduct a computer-assisted personal interview, take body measurements, and measure blood pressure. The personal interviews included adapted versions of pre-existing screening instruments for chronic conditions. Body measurements included height, weight, and grip strength of the dominant hand. A finger-prick blood sample was taken from a subgroup of the study participants and point-of-care blood tests were performed. The CareSens Blood Glucose Monitoring System and the HemoCue Hemoglobin 201+ Analyser were used for point-of-care blood testing.
Assessment of Chronic Conditions
Self-Report of Chronic Conditions
Ischemic heart disease, hypercholesterolemia, stroke, smoking status, chronic cough (no tuberculosis [TB]), kidney disease, HIV, and tuberculosis were identified by self-reporting either a diagnosis or ever receiving treatment for the respective condition. Diabetes and hypertension were identified either by a self-report of current treatment or by measurement (Supplementary Table S2).
Measurement of Chronic Conditions
Anemia, diabetes, hypertension, obesity, and underweight were defined based on thresholds for hemoglobin (<12 mg/dL for women and <13 mg/dL for men), blood glucose (≥200 mg/dL at any time, fasting blood glucose ≥126 mg/dL, or on diabetes treatment), blood pressure (systolic pressure ≥140 mmHg, diastolic pressure ≥90 mmHg, or on antihypertensive treatment), and the body mass index (>30 kg/m2 and <18.5 kg/m2), respectively. The hemoglobin threshold was adjusted for smoking (+0.3 mg/dL) and African origin (−1 mg/dL) [19, 20]. Hand grip strength <27 kg for men and <16 kg for women was categorized as low and indicative of sarcopenia [21] (Supplementary Table S2).
Screening of Chronic Conditions
Ischemic heart disease included a self-reported past diagnosis or screening positive for symptoms of angina pectoris, which were assessed using a modified Rose Angina Questionnaire [22, 23]. Depressive symptoms were assessed using the 10-item Center of Epidemiologic Studies Depression Scale (cut-off score ≥10) [24, 25]. Signs of alcoholism were assessed using the Cut, Annoyed, Guilty, and Eye (CAGE) questionnaire (cut-off score ≥2) [26]. Signs of cognitive problems were assessed using recall tests (cut-off score ≤1.5 SD of sample mean), which we adapted from the United States Health and Retirement Study [27, 28], or self-rated memory (rated as fair or poor) if recall tests were incomplete (Supplementary Table S2).
Multimorbidity
Multimorbidity was defined as being affected by ≥2 chronic conditions. As anemia and diabetes were only assessed in a subsample of study participants, we assessed multimorbidity based on either 17 or 15 chronic conditions. The multimorbidity measure based on 17 chronic conditions was the primary multimorbidity outcome assessed. It was only available in the subsample of study participants selected for blood testing. The multimorbidity measure based on 15 chronic conditions excluded anemia and diabetes and was thus available for the full study sample. Both multimorbidity measures were treated as missing data when data on one or more chronic conditions was missing.
Data Analysis
Characteristics of the study participants were summarized using descriptive statistics. We report the median and interquartile range (IQR) for continuous variables and the number and percentage of observations in a category for categorical variables. Statistical differences between male and female study participants were assessed using the Wilcoxon rank-sum test for continuous variables and the Pearson’s χ2 test for categorical variables. The sample prevalence for each chronic condition and multimorbidity was estimated as a proportion with logit-transformed confidence intervals. Tests on the equality of proportions used large-sample statistics. Tetrachoric correlation was used to analyze pairwise correlations between chronic conditions and multimorbidity. For each sex, the relationships of chronic conditions and multimorbidity with age were assessed using point biserial correlation and Epanechnikov kernel-weighted local polynomial regression graphs. The relationships of chronic conditions and multimorbidity with sex and age were further assessed using univariable and multivariable logistic regressions. The multivariable regressions included sex and age together and adjusted for religion, marital status, number of children, literacy, formal education, work status, availability of food, and the location of the dwelling. We rescaled age to 10-year increments to better reflect longer term developments in the regression results. Odds ratios of age (ORs) therefore express changes per 10 years. Standard errors were estimated using the Huber-White sandwich estimator. Statistical significance was assumed for p < 0.05. All analyses were conducted in Stata/SE 18.5.
Ethical Considerations
The institutional review boards of the Muhimbili University of Health and Allied Sciences in Tanzania (2015-04-22/AEC/Vol.IX/82) and the Harvard T.H. Chan School of Public Health in the United States (14-4282) approved the study. Participants gave written informed consent to participate in the study before interviews and, where applicable, again before blood collection and testing.
Results
Sample Characteristics
Our study sample of 2,246 participants aged ≥40 years included 32.0% men and 68.0% women. About half of the study participants (48.3%) were 40–49 years old and about one-quarter (27.0%) were 50–59 years old. About one-quarter (24.7%) had reached or surpassed the retirement age of 60 years. Almost all study participants (98.9%) were of Tanzanian origin. About half (54.4%) stated to be Muslim and about half (45.6%) to be Christian. Being married or cohabitant (70.8%) and having children (97.1%) was common. Most study participants could read and/or write (83.8%) and attended less than 7 years or no formal education (77.6%). Almost half (48.8%) of the study participants experienced food insecurity at home due to a lack of money at least once in the past year (Table 1).
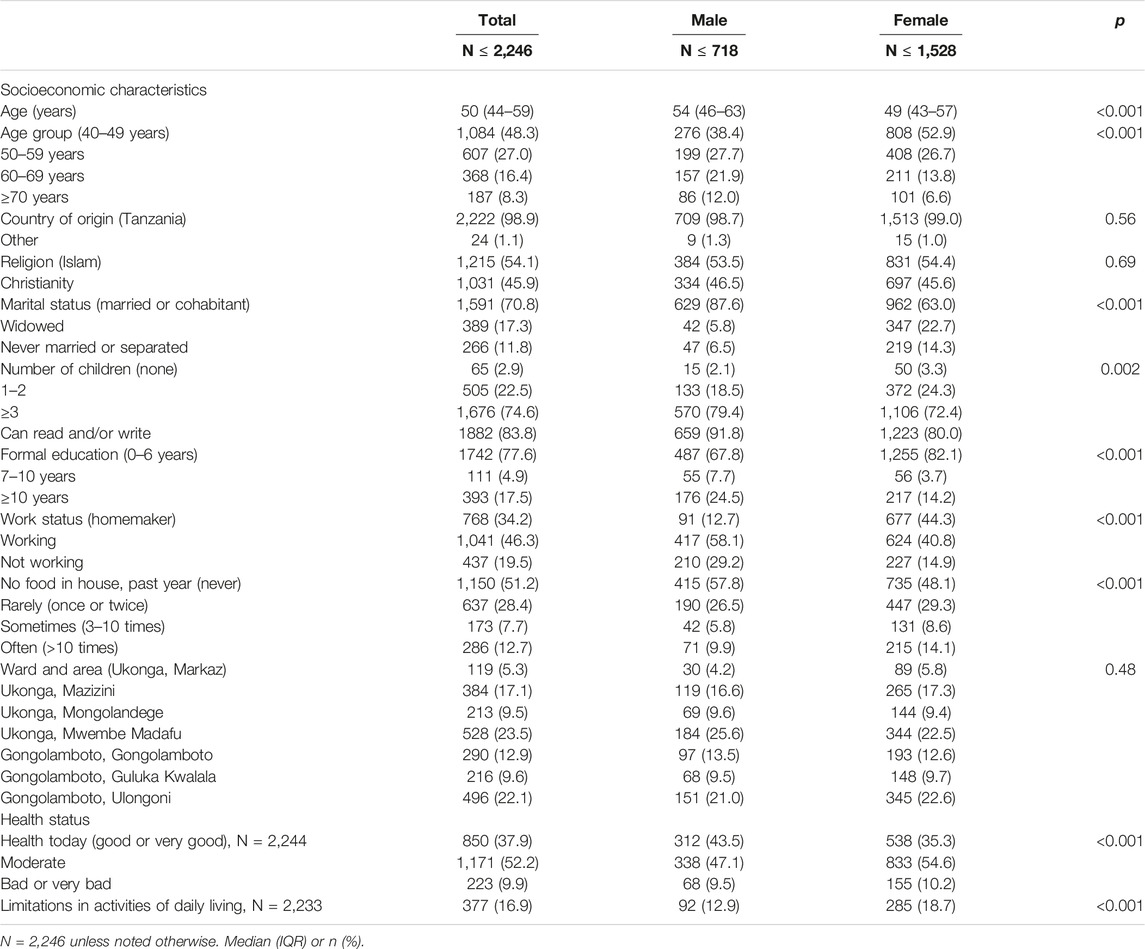
Table 1. Sociodemographic characteristics and health status of ≥40-year-old study participants (Dar es Salaam, Tanzania, 2024).
Women had a median age of 49 years (IQR: 43–57) and were younger than men who had a median age of 54 years (IQR: 46–63; p < 0.001). Men were more often than women married or cohabitant, had ≥3 children, any literacy, or attended formal education (all p ≤ 0.002). Women were more often than men working as homemaker or otherwise and were affected by food insecurity in the past year (both p < 0.001). Similar portions of men (9.5%) and women (10.2%) reported a bad or very bad health status on the study day, but good or very good health was more frequently reported by men (43.5%) than women (35.3%; p < 0.001). Fewer men than women reported one or more limitations in activities of daily living (12.9% versus 18.7%; p < 0.001).
Prevalence of Chronic Conditions and Multimorbidity Across Sexes and Age Groups
Among the ≥40-year-old study participants, 93.9% (95% CI: 92.1–95.3) had one or more chronic conditions. The prevalence of multimorbidity was 73.7% (95% CI: 70.7–76.4) when anemia and diabetes were considered. The prevalence of multimorbidity without anemia and diabetes was 58.5% (95% CI: 56.3–60.6). Between half and every 10th study participant screened positive for one or more of the seven most common chronic conditions. These were hypertension (51.3%, 95% CI: 49.2–53.4), anemia (34.1%, 95% CI: 31.2–37.2), obesity (32.2%, 95% CI: 30.3–34.2), diabetes (31.6%, 95% CI: 28.7–34.5), depressive symptoms (31.5%, 95% CI: 29.6–33.5), low grip strength (21.2%, 95% CI: 19.5–23.0), and ischemic heart disease (11.9%, 95% CI: 10.6–13.3). Signs of alcohol problems were found in 7.7% (95% CI: 6.7–8.9), signs of cognitive problems in 6.6% (95% CI: 5.6–7.7), and HIV infection in 5.1% (95% CI: 4.2–6.1) of the study participants. The seven least prevalent chronic conditions, which affected every 20th or fewer study participants, were high cholesterol (5.0%, 95% CI: 4.2–6.0), tuberculosis (4.8%, 95% CI: 4.0–5.8), stroke (4.8%, 95% CI: 4.0–5.8), current smoking (4.5%, 95% CI: 3.7–5.4), underweight (4.3%, 95% CI: 3.5–5.2), chronic cough (3.3%, 95% CI: 2.6–4.1), and kidney disease (2.9%, 95% CI: 2.3–3.6) (Table 2; Supplementary Table S3).
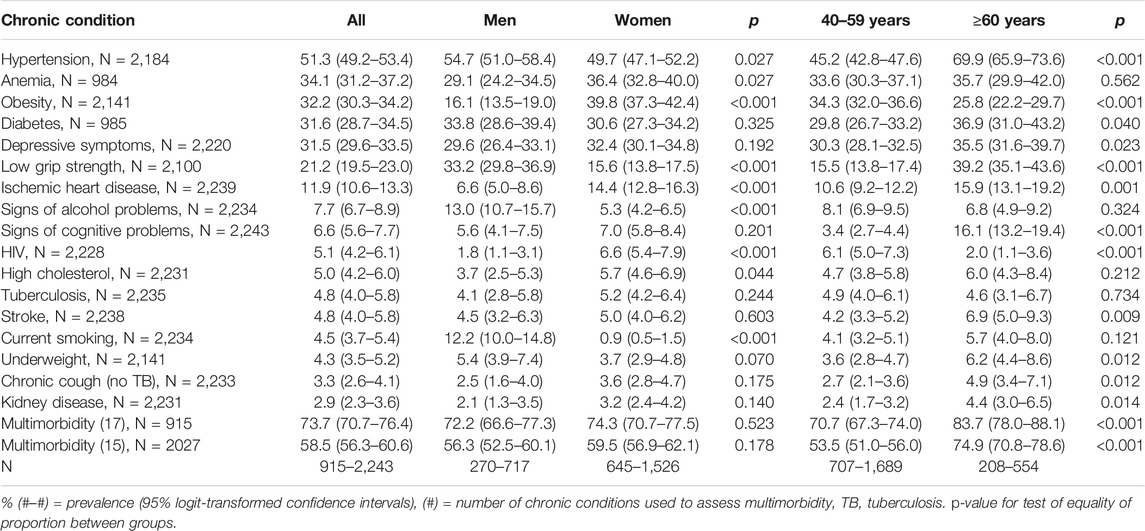
Table 2. Prevalence of chronic conditions and multimorbidity among ≥40-year-old study participants (Dar es Salaam, Tanzania, 2024).
Prevalence of Chronic Conditions and Multimorbidity by Sex and Age
The prevalence of multimorbidity was similar among men and women irrespectively of whether multimorbidity was assessed based on 17 or 15 chronic conditions. However, the prevalence of the underlying chronic conditions differed between men and women. Hypertension, low grip strength, signs of alcohol problems, and current smoking were more prevalent among men. More prevalent among women were anemia, obesity, signs of ischemic heart disease, HIV, and high cholesterol (all p ≤ 0.044). The prevalence of multimorbidity was higher among the study participants of or over the retirement age of 60 years (70.7%, 95% CI: 67.3–74.0 versus 83.7%, 95% CI: 78.0–88.1; p < 0.001 with 17 chronic conditions and 53.5%, 95% CI: 51.0–56.0 versus 74.9%, 95% CI: 70.8–78.6; p < 0.001 with 15 chronic conditions). Across sexes, this increase was driven by a higher prevalence of hypertension, diabetes, depressive symptoms, low grip strength, ischemic heart disease, signs of cognitive problems, stroke, underweight, chronic cough, and kidney disease at older age (p ≤ 0.040). Only obesity and HIV were less prevalent in the ≥60-year-olds compared to younger participants (p < 0.001) (Table 2; Figure 1; Supplementary Figures S3, S4).
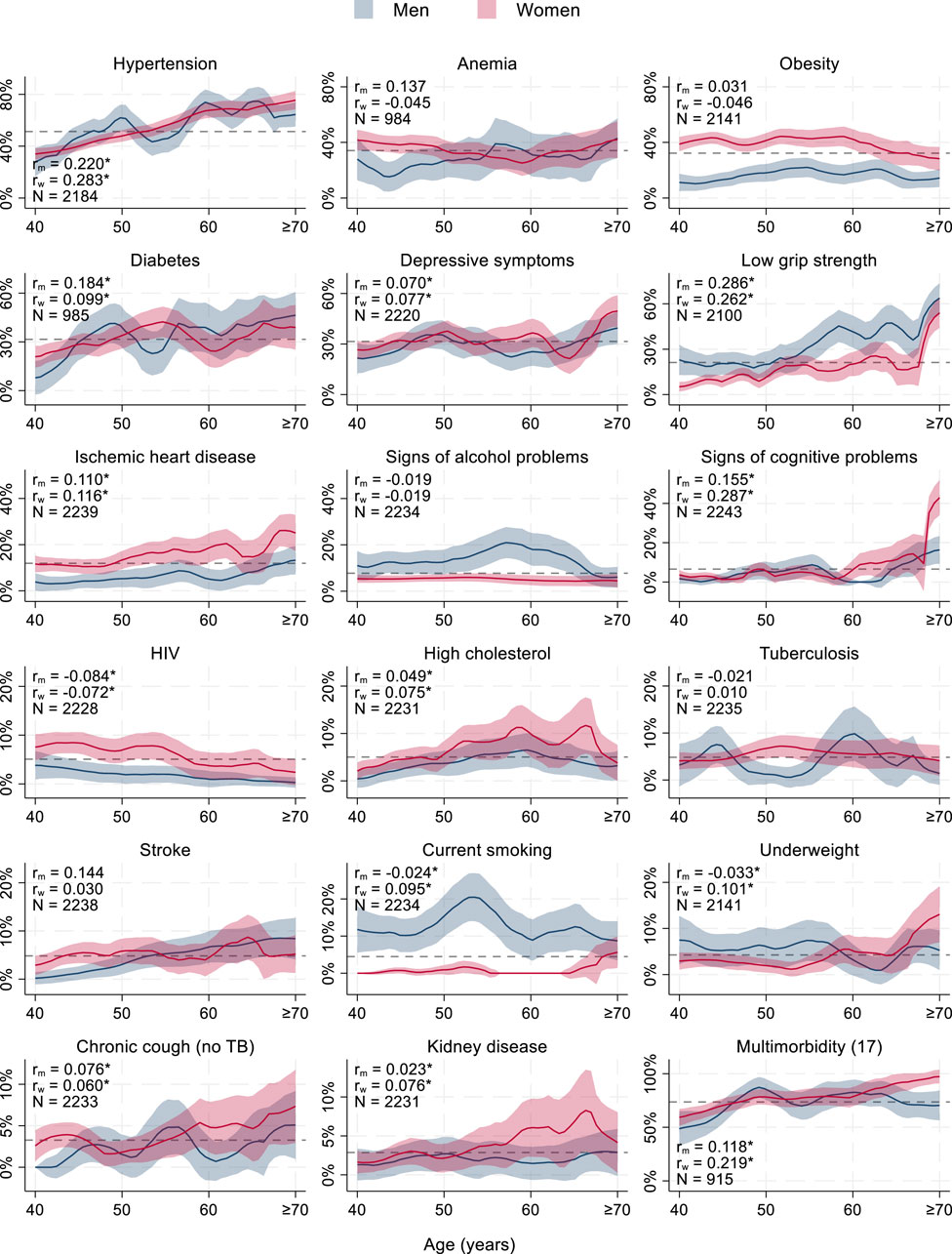
Figure 1. Prevalence of chronic conditions and multimorbidity among ≥40-year-old study participants (Dar es Salaam, Tanzania, 2024) *p < 0.05. r = point biserial correlation coefficient of chronic condition and age, m = men, w = women, N = number of observations, dashed line = average prevalence across ages and sexes (#) = number of chronic conditions used to assess multimorbidity, TB = tuberculosis. Epanechnikov kernel-weighted local polynomial regression with 95% confidence intervals. Scale of y-axis differs across graphs.
Correlation Between Chronic Conditions and Multimorbidity
Pairwise correlations between chronic conditions were often insignificant or low (Tetrachoric correlation r < 0.30). Correlations between chronic conditions and multimorbidity were mostly moderate (r = 0.30–0.50) or strong (r ≥ 0.50). The strongest positive correlations between individual chronic conditions were between signs of alcohol problems and current smoking (r = 0.42), depressive symptoms and ischemic heart disease (r = 0.41), high cholesterol and kidney disease (r = 0.39), obesity and high cholesterol (r = 0.38), HIV and tuberculosis (r = 0.35), current smoking and kidney disease (r = 0.35), hypertension and high cholesterol (r = 0.32), stroke and kidney disease (r = 0.32), tuberculosis and underweight (r = 0.31), signs of alcohol problems and chronic cough (r = 0.30), and smoking and underweight (r = 0.30). The strongest positive correlations (r ≥ 0.50) between individual chronic condition and multimorbidity (based on 17 chronic conditions) occurred for high cholesterol, chronic cough, and kidney disease (all r = 1), ischemic heart disease (r = 0.69), hypertension (r = 0.60), obesity, depressive symptoms (both r = 0.57), and diabetes (r = 0.50) (Table 3).
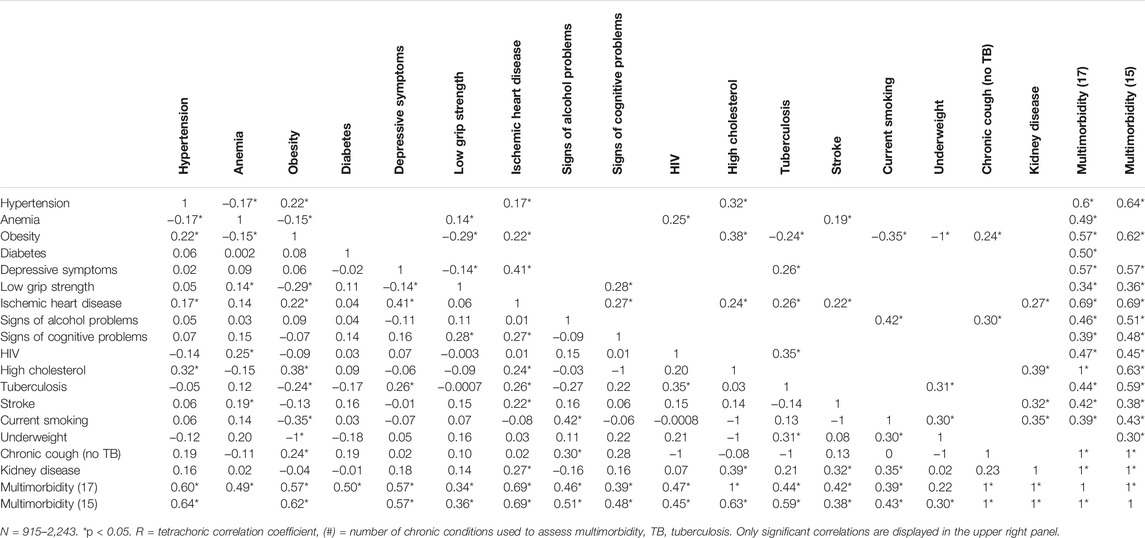
Table 3. Pairwise correlations between chronic conditions and multimorbidity among ≥40-year-old study participants (Dar es Salaam, Tanzania, 2024).
Association of Chronic Conditions and Multimorbidity With Sex and Age
In univariable regressions, women had higher odds than men for HIV (OR = 3.77, 95% CI: 2.10–6.77), obesity (OR = 3.46, 95% CI: 2.75–4.35), ischemic heart disease (OR = 2.40, 95% CI: 1.73–3.33), high cholesterol (OR = 1.58, 95% CI: 1.01–2.47), and anemia (OR = 1.39, 95% CI: 1.04–1.87). Women had lower odds than men for current smoking (OR = 0.06, 95% CI: 0.03–0.11), signs of alcohol problems (OR = 0.37, 95% CI: 0.27–0.51), low grip strength (OR = 0.37, 95% CI: 0.30–0.46), and hypertension (OR = 0.82, 95% CI: 0.68–0.98) (Table 4 column 1).
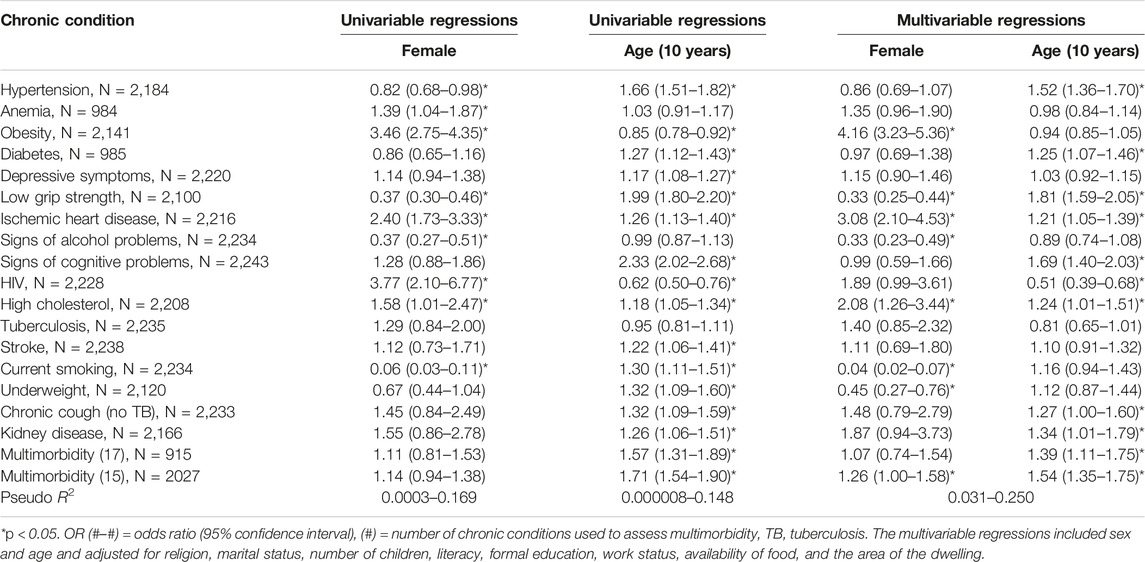
Table 4. Relationships of chronic conditions with age and sex among ≥40-year-old study participants (Dar es Salaam, Tanzania, 2024).
Older age (per 10 years) was associated with higher odds of signs of cognitive problems (OR = 2.33, 95% CI: 2.02–2.68), low grip strength (OR = 1.99, 95% CI: 1.80–2.20), hypertension (OR = 1.66, 95% CI: 1.51–1.82), underweight (OR = 1.32, 95% CI: 1.09–1.60), chronic cough (no TB) (OR = 1.32, 95% CI: 1.09–1.59), current smoking (OR = 1.30, 95% CI: 1.11–1.51), diabetes (OR = 1.27, 95% CI: 1.12–1.43), ischemic heart disease (OR = 1.26, 95% CI: 1.13–1.40), kidney disease (OR = 1.26, 95% CI: 1.06–1.51), stroke (OR = 1.22, 95% CI: 1.06–1.41), high cholesterol (OR = 1.18, 95% CI: 1.05–1.34), depressive symptoms (OR = 1.17, 95% CI: 1.08–1.27), and multimorbidity (OR = 1.57, 95% CI: 1.31–1.89 based on 17 chronic conditions, or OR = 1.71, 95% CI: 1.54–1.90 based on 15 chronic conditions). Older age was associated with lower odds of HIV (OR = 0.62, 95% CI: 0.50–0.76) and obesity (OR = 0.85, 95% CI: 0.78–0.92) (Table 4 column 2).
In multivariable regressions which included sex, age, and other socioeconomic characteristics, women had higher odds than men for obesity (adjusted OR = 4.16, 95% CI: 3.23–5.36), ischemic heart disease (adjusted OR = 3.08, 95% CI: 2.10–4.53), high cholesterol (adjusted OR = 2.08, 95% CI: 1.26–3.44), and multimorbidity based on 15 chronic conditions (adjusted OR = 1.26, 95% CI: 1.00–1.58). Women had lower odds than men for underweight (adjusted OR = 0.45, 95% CI: 0.27–0.76), low grip strength (adjusted OR = 0.33, 95% CI: 0.25–0.44), signs of alcohol problems (adjusted OR = 0.33, 95% CI: 0.23–0.49), and smoking (adjusted OR = 0.04, 95% CI: 0.02–0.07). Older age was associated with higher odds (per 10 years) of low grip strength (adjusted OR = 1.81, 95% CI: 1.59–2.05), signs of cognitive problems (adjusted OR = 1.69, 95% CI: 1.40–2.03), hypertension (adjusted OR = 1.52, 95% CI: 1.36–1.70), kidney disease (adjusted OR = 1.34, 95% CI: 1.01–1.79), chronic cough (no TB) (adjusted OR = 1.27, 95% CI: 1.00–1.60), diabetes (adjusted OR = 1.25, 95% CI: 1.07–1.46), high cholesterol (adjusted OR = 1.24, 95% CI: 1.01–1.51), ischemic heart disease (adjusted OR = 1.21, 95% CI: 1.05–1.39), and multimorbidity (adjusted OR = 1.39, 95% CI: 1.11–1.75 based on 17 chronic conditions and adjusted OR = 1.54, 95% CI: 1.35–1.75 based on 15 chronic conditions). Older age (per 10 years) was associated with lower odds of HIV (adjusted OR = 0.51, 95% CI: 0.39–0.68). Sex ceased to be associated with HIV, anemia, and hypertension after adjusting for age and other socioeconomic characteristics. In turn, women had lower odds of underweight and higher odds of multimorbidity (based on 15 chronic conditions without anemia and diabetes) after adjusting for age and other socioeconomic characteristics. Age ceased to be associated with underweight, smoking, stroke, depressive symptoms, and obesity after adjusting for sex and other socioeconomic characteristics (Table 4 columns 3–4).
Discussion
Main Findings of This Study
Multimorbidity based on 17 chronic conditions affected 73.7% of the ≥40-year-old study participants living in the peri-urban Ukonga and Gongolamboto wards of Dar es Salaam. Multimorbidity was associated with age and 83.7% of the ≥60-year-old study participants had multiple chronic conditions. After adjusting for other socioeconomic characteristics, women had higher odds of obesity, ischemic heart disease, and high cholesterol and they had lower odds of underweight, low grip strength, alcohol problems, and smoking. Age was associated with higher adjusted odds of low grip strength, cognitive problems, hypertension, kidney disease chronic cough, diabetes, high cholesterol, ischemic heart disease, and multimorbidity and with lower adjusted odds of HIV infection.
What Is Already Known
Previous estimates of multimorbidity of non-communicable diseases in low-income countries in sub-Saharan Africa were variable and mostly lower than our estimates [6–9]. A cross-sectional, population-based study in rural and urban Malawi reported that 1%–4% of men and 4%–7% of women had combinations of hypertension, diabetes, and obesity [29]. A cross-country study using the World Health Surveys (WHS) reported a prevalence of multimorbidity of 3.6% in Ghana, 4.2% in Kenya, 6.3% in Burkina Faso, and 7.9% in Namibia [30]. A cross-sectional study among adults in Botswana estimated a multimorbidity prevalence of 5.4% [31]. The Study on global AGEing and adult health (SAGE) reported 22% multimorbidity in a population-based sample from Ghana [32]. A cross-sectional study among community-dwelling people aged ≥60 in Burkina Faso found a multimorbidity prevalence of 65% [33]. Another study reported a 17.8% prevalence of non-communicable chronic diseases among ≥18-year-old hospital patients in Ethiopia [34].
Considering both communicable and non-communicable diseases, multimorbidity was estimated in 28.7% of the people living in two urban slums in Nairobi [35], in 15.3% of adults living with HIV in Zimbabwe [36], in 38.8% of patients of an urban clinic in Ghana [37], in 59.1% of elderly hospital patients in Ethiopia [38], and in 49% of elderly hospital patients in Nigeria [39]. A cross-country study of adults in six urban and rural centers in Ghana, Burkina Faso, Kenya, and South Africa reported a multimorbidity prevalence of 20.2%–51.7% among men and 24.1%–64.9% among women [10]. A previous study in five rural villages in northern Tanzania in 2017 found a prevalence of multimorbidity of 26.1% when chronic conditions were self-reported and 67.3% when chronic conditions were assessed through clinician diagnosis, screening tools, and blood pressure measurement [15]. A study among people living with HIV, diabetes, and/or hypertension in Tanzania or Uganda reported a multimorbidity prevalence of 25.6% [16].
Previous studies of the same sample of ≥40-year-old people in peri-urban Dar es Salaam reported a multimorbidity prevalence of 25.3% [12], 61.1% [13], and 73.8% (95% CI: 71.2–76.3) for women only [14]. Differences in multimorbidity estimates in the same sample result from assessing fewer chronic conditions (8, 13, and 15, respectively) and/or using only self-report [12] in the assessment of chronic conditions. Across studies, older adults were consistently more likely to have multimorbidity [12, 14, 29–37]. Several previous studies further reported that women were more likely multimorbid than man [12, 29–32, 35–37].
What This Study Adds
Multimorbidity has been called a priority for global health research [40]. A recent systematic review and meta-analysis estimated a pooled multimorbidity prevalence of 28.2% (95% CI: 15.6–40.8) in sub-Saharan Africa and conjectured that this low estimate could indicate high levels of undiagnosed chronic illness in this region [7]. We studied multimorbidity in a ≥40-year-old population based on assessing either 17 or 15 chronic conditions through a combination of self-report, measurement, and screening instruments. We estimated a prevalence of multimorbidity that is higher than previous estimates for sub-Saharan Africa and among the highest estimates that have been reported for low-income and middle-income countries [6]. Our estimate is consistent with a suspected large gap in diagnosing multimorbidity. Even more, finding 70.7% multimorbidity among the 40–59-year-old study participants and 83.7% multimorbidity among the ≥60-year-old study participants suggests that already most middle-aged people living in peri-urban Dar es Salaam and similar settings might benefit from a broad health assessment and subsequent care for multiple health conditions. Our findings further indicate that a broad assessment of chronic conditions can help detect different patterns of multimorbidity, as the chronic conditions determining multimorbidity differ between men and women. For instance, we estimated an association between multimorbidity and being a woman only when multimorbidity was assesses based on 15 chronic conditions without anemia and diabetes.
Practical Implications
Past studies have identified gaps in the preparedness of health facilities in Tanzania to treat non-communicable diseases such as hypertension and diabetes [41, 42]. A community-based survey from South Africa indicated that 93% of participants who screened positive for diabetes and 58% who screened positive for hypertension had unmet health needs [43]. We found hypertension and diabetes to be the most common and fourth most common chronic conditions, respectively. The study at hand further indicates that multiple chronic conditions are likely to be present among peri-urban dwellers in Tanzania aged ≥40-years. These findings underscore the scale of the challenge to develop care structures for multiple chronic conditions, especially for multiple non-communicable diseases, and broad health assessments for aging people in sub-Saharan Africa.
Approaches to caring for multiple chronic conditions may entail the integration of health programs for single diseases. A study, which piloted integrated HIV, diabetes, and hypertension care in ten health facilities offering primary care in Dar es Salaam and Kampala, has concluded that integrated management of chronic diseases is a feasible strategy [44]. A systematic review and meta-analysis on the effectiveness of integrated chronic care models in sub-Saharan Africa found positive effects on systolic blood pressure and mixed results for other health outcomes [45]. Expanding integrated care programs seems needed globally and continues to require addressing knowledge gaps, for instance, on joint care for communicable and non-communicable diseases [46], the costs of multimorbidity in low- and middle income countries [47], and the components making integrated care for multiple chronic conditions effective and cost-effective in Tanzania and other sub-Saharan African countries.
Strengths and Limitations
Strengths of this study include, first, that a wide range of chronic conditions was assessed in a general population. Second, we emphasized sensitivity in our assessment of chronic conditions by combining measurement, screening instruments, and self-report of chronic conditions. Third, we assessed multimorbidity and underlying chronic conditions by sex and age. Limitations of this study include, first, that the screening instruments have not been validated in our study population. Second, we used different approaches to assess chronic conditions, namely, self-reporting, screening instruments, and measurement. Seven chronic conditions were based only on self-report, which can be more prone to errors and bias than the use of screening instruments or measurement. Third, we used lifetime measures to assess the presence of chronic conditions. It is possible that certain conditions were no longer present at the time of data collection. Fourth, our study is likely affected by a selection bias, as only 2,299 of the randomly selected 4,840 individuals participated in the study and only 1,024 of 2,420 selected individuals agreed to undergo blood testing. Men were included less often than women in the study. People with few chronic conditions, who worked further away, or with severe comorbidities might have been less likely to participate in the study. We aimed to account for selective participation and non-responses by stratifying descriptive analyses by sex and age and by adjusting for sex, age, and other socioeconomic characteristics in the regression analyses. Fifth, it remains unknown how the prevalence of chronic conditions in the Dar es Salaam Urban Cohort Study (DUCS) population, from which we sampled, compares to other peri-urban or urban populations in Tanzania and elsewhere. Sixth, the study was conducted in 2017/18. The COVID-19 pandemic and other factors could have caused changes in the prevalence of chronic conditions. Seventh, multiple comparisons may have inflated the number of significant findings. Finally, the cross-sectional study design was not suitable to assess causal relationships.
Conclusion
The comprehensive assessment of chronic conditions and multimorbidity in this study suggests that multiple chronic conditions affect most middle-aged and elderly people in Tanzania. The prevalence of multimorbidity among ≥40-year-old peri-urban dwellers was higher than estimates for sub-Saharan Africa from previous studies. The estimated multimorbidity prevalence of 73.7% suggests a substantial need for the care and prevention of multimorbidity and chronic conditions in Tanzania. Sex and age differences in the prevalence of chronic conditions indicate that women and men have different causes of multimorbidity across the age spectrum that might require different screening, treatment, and preventive care.
Data Availability Statement
The data and code supporting the findings of this study are openly available in Harvard Dataverse at https://doi.org/10.7910/DVN/9EH23J and heiDATA at https://doi.org/10.11588/data/VVKWZK, respectively.
Ethics Statement
The study was approved by the Muhimbili University of Health and Allied Sciences in Tanzania (2015-04-22/AEC/Vol.IX/82) and the Harvard T. H. Chan School of Public Health in the United States (14-4282). The study was conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author Contributions
SK conducted the data analysis. SK and NP wrote the manuscript. TB, JK, and JKR acquired funding for data collection. GHL, PK, and JK led study implementation activities. All authors contributed intellectual content to the article and approved the submitted version.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. Research reported in this publication was supported by the National Institute on Aging of the National Institutes of Health under Award Number P30AG024409.
Conflict of Interest
The authors declare that they do not have any conflicts of interest.
Acknowledgments
The authors acknowledge financial support for the publishing fee by Heidelberg University. LMS further acknowledges support by the Else Kröner-Fresenius-Stiftung within the Heidelberg Graduate School of Global Health.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.ssph-journal.org/articles/10.3389/ijph.2024.1606387/full#supplementary-material
References
1. GBD 2019 Diseases and Injuries Collaborators. Global Burden of 369 Diseases and Injuries in 204 Countries and Territories, 1990-2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet (2020) 396(10258):1204–22. doi:10.1016/S0140-6736(20)30925-9
2. Li, Z, Shi, J, Wang, M, Jin, Y, and Zheng, ZJ. Temporal Trends in the Burden of Non-Communicable Diseases in Countries With the Highest Malaria Burden, 1990-2019: Evaluating the Double Burden of Non-Communicable and Communicable Diseases in Epidemiological Transition. Glob Health (2022) 18(1):90. doi:10.1186/s12992-022-00882-w
3. Gouda, HN, Charlson, F, Sorsdshl, K, Ahmadzada, S, Ferrari, AJ, Erskine, H, et al. Burden of Non-Communicable Diseases in Sub-Saharan Africa, 1990–2017: Results from the Global Burden of Disease Study 2017. Lancet Glob Health (2019) 7(10):e1375–e1387.
4. Reuter, A, Bärnighausen, T, and Kohler, S. Global Ageing and Health. In: DE Bloom, A Sousa-Poza, and U Sunde, editors. The Routledge Handbook of the Economics of Ageing. London: Routledge (2023). p. 657–70.
5. United Nations. Department of Economic and Social Affairs Population Division, World Population Prospects 2022 (2023). Available from: https://population.un.org/wpp/ (Accessed June 15, 2024).
6. Asogwa, OA, Boateng, D, Marzà-Florensa, A, Peters, S, Levitt, N, van Olmen, J, et al. Multimorbidity of Non-Communicable Diseases in Low-Income and Middle-Income Countries: A Systematic Review and Meta-Analysis. BMJ Open (2022) 12(1):e049133. doi:10.1136/bmjopen-2021-049133
7. Chowdhury, SR, Chandra Das, D, Sunna, TC, Beyene, J, and Hossain, A. Global and Regional Prevalence of Multimorbidity in the Adult Population in Community Settings: A Systematic Review and Meta-Analysis. eClinicalMedicine (2023) 57:101860. doi:10.1016/j.eclinm.2023.101860
8. Roomaney, RA, van Wyk, B, Turawa, EB, and Pillay-van Wyk, V. Multimorbidity in South Africa: Asystematic Review of Prevalence Studies. BMJ Open (2021) 11(10):e048676. doi:10.1136/bmjopen-2021-048676
9. Ho, IS, Azcoaga-Lorenzo, A, Akbari, A, Davies, J, Hodgins, P, Khunti, K, et al. Variation in the Estimated Prevalence of Multimorbidity: Systematic Review and Meta-Analysis of 193 International Studies. BMJ Open (2022) 12(4):e057017. doi:10.1136/bmjopen-2021-057017
10. Micklesfield, LK, Munthali, R, Agongo, G, Asiki, G, Boua, P, Choma, SS, et al. Identifying the Prevalence and Correlates of Multimorbidity in Middle-Aged Men and Women: A Cross-Sectional Population-Based Study in Four African Countries. BMJ Open (2023) 13(3):e067788. doi:10.1136/bmjopen-2022-067788
11. World Bank. World Development Indicators: The World by Income and Region (2024). Available from: https://datatopics.worldbank.org/world-development-indicators/the-world-by-income-and-region.html (Accessed June 15, 2024).
12. Tomita, A, Leyna, GH, Kim, HY, Moodley, Y, Mpolya, E, Mogeni, P, et al. Patterns of Multimorbidity and Their Association With Hospitalisation: A Population-Based Study of Older Adults in Urban Tanzania. Age Ageing (2021) 50(4):1349–60. doi:10.1093/ageing/afab046
13. Stieglitz, L-M, Adams, LB, Bärnighausen, T, Berghöfer, A, Kazonda, P, Killewo, J, et al. Depressive Symptoms and Their Association With Age, Chronic Conditions and Health Status Among Middle-Aged and Elderly People in Peri-Urban Tanzania. Cambridge Prisms: Glob Ment Health (2023) 10:e27. doi:10.1017/gmh.2023.17
14. Stieglitz, LM, Bärnighausen, T, Leyna, GH, Kazonda, P, Killewo, J, Rohr, JK, et al. Patterns of Comorbidity and Multimorbidity Among Middle-Aged and Elderly Women in Peri-Urban Tanzania. J Multimorbidity Comorbidity (2022) 12:26335565221076254. doi:10.1177/26335565221076254
15. Lewis, EG, Gray, WK, Walker, R, Urasa, S, Witham, M, and Dotchin, C. Multimorbidity and Its Socio-Economic Associations in Community-Dwelling Older Adults in Rural Tanzania; a Cross-Sectional Study. BMC Public Health (2022) 22(1):1918. doi:10.1186/s12889-022-14340-0
16. Shiri, T, Birungi, J, Garrib, AV, Kivuyo, SL, Namakoola, I, Mghamba, J, et al. Patient and Health Provider Costs of Integrated HIV, Diabetes and Hypertension Ambulatory Health Services in Low-Income Settings - an Empirical Socio-Economic Cohort Study in Tanzania and Uganda. BMC Med (2021) 19(1):230. doi:10.1186/s12916-021-02094-2
17. Leyna, GH, Berkman, LF, Njelekela, MA, Kazonda, P, Irema, K, Fawzi, W, et al. Profile: The Dar Es Salaam Health and Demographic Surveillance System (Dar Es Salaam HDSS). Int J Epidemiol (2017) 46(3):801–8. doi:10.1093/ije/dyw324
18. HAALSI. Health and Aging in Africa: A Longitudinal Study in South Africa (2023). Available from: https://haalsi.org/ (Accessed June 15, 2024).
19. Sullivan, KM, Mei, Z, Grummer-Strawn, L, and Parvanta, I. Haemoglobin Adjustments to Define Anaemia. Trop Med Int Health (2008) 13(10):1267–71. doi:10.1111/j.1365-3156.2008.02143.x
20. World Health Organization. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity. Vitamin and Mineral Nutrition Information System. Geneva: World Health Organization (2011).
21. Cruz-Jentoft, AJ, Bahat, G, Bauer, J, Boirie, Y, Bruyère, O, Cederholm, T, et al. Sarcopenia: Revised European Consensus on Definition and Diagnosis. Age Ageing (2019) 48(1):601–31. doi:10.1093/ageing/afz046
22. Rose, GA. The Diagnosis of Ischaemic Heart Pain and Intermittent Claudication in Field Surveys. Bull World Health Organ (1962) 27:645–58.
23. Rose, G, McCartney, P, and Reid, DD. Self-Administration of a Questionnaire on Chest Pain and Intermittent Claudication. Br J Prev Soc Med (1977) 31(1):42–8. doi:10.1136/jech.31.1.42
24. Radloff, LS. The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Appl Psychol Meas (1977) 1(3):385–401. doi:10.1177/014662167700100306
25. Andresen, EM, Malmgren, JA, Carter, WB, and Patrick, DL. Screening for Depression in Well Older Adults: Evaluation of a Short Form of the CES-D. Am J Prev Med (1994) 10(2):77–84. doi:10.1016/s0749-3797(18)30622-6
26. Ewing, JA. Detecting Alcoholism: The CAGE Questionnaire. JAMA (1984) 252(14):1905–7. doi:10.1001/jama.252.14.1905
27. Kobayashi, LC, Glymour, MM, Kahn, K, Payne, CF, Wagner, RG, Montana, L, et al. Childhood Deprivation and Later-Life Cognitive Function in a Population-Based Study of Older Rural South Africans. Soc Sci Med (2017) 190:20–8. doi:10.1016/j.socscimed.2017.08.009
28. Kobayashi, LC, Mateen, FJ, Montana, L, Wagner, RG, Kahn, K, Tollman, SM, et al. Cognitive Function and Impairment in Older, Rural South African Adults: Evidence From "Health and Aging in Africa: A Longitudinal Study of an INDEPTH Community in Rural South Africa. Neuroepidemiology (2019) 52(1-2):32–40. doi:10.1159/000493483
29. Price, AJ, Crampin, AC, Amberbir, A, Kayuni-Chihana, N, Musicha, C, Tafatatha, T, et al. Prevalence of Obesity, Hypertension, and Diabetes, and Cascade of Care in Sub-Saharan Africa: A Cross-Sectional, Population-Based Study in Rural and Urban Malawi. Lancet Diabetes Endocrinol (2018) 6(3):208–22. doi:10.1016/S2213-8587(17)30432-1
30. Afshar, S, Roderick, PJ, Kowal, P, Dimitrov, BD, and Hill, AG. Multimorbidity and the Inequalities of Global Ageing: A Cross-Sectional Study of 28 Countries Using the World Health Surveys. BMC Public Health (2015) 15(1):776. doi:10.1186/s12889-015-2008-7
31. Keetile, M, Navaneetham, K, and Letamo, G. Prevalence and Correlates of Multimorbidity Among Adults in Botswana: A Cross-Sectional Study. PLoS One (2020) 15(9):e0239334. doi:10.1371/journal.pone.0239334
32. Arokiasamy, P, Uttamacharya, U, Jain, K, Biritwum, RB, Yawson, AE, Wu, F, et al. The Impact of Multimorbidity on Adult Physical and Mental Health in Low- and Middle-Income Countries: What Does the Study on Global Ageing and Adult Health (SAGE) Reveal? BMC Med (2015) 13(1):178. doi:10.1186/s12916-015-0402-8
33. Hien, H, Berthé, A, Drabo, MK, Meda, N, Konaté, B, Tou, F, et al. Prevalence and Patterns of Multimorbidity Among the Elderly in Burkina Faso: Cross-Sectional Study. Trop Med Int Health (2014) 19(11):1328–33. doi:10.1111/tmi.12377
34. Woldesemayat, EM, Kassa, A, Gari, T, and Dangisso, MH. Chronic Diseases Multi-Morbidity Among Adult Patients at Hawassa University Comprehensive Specialized Hospital. BMC Public Health (2018) 18(1):352. doi:10.1186/s12889-018-5264-5
35. Mohamed, SF, Haregu, TN, Uthman, OA, Khayeka-Wandabwa, C, Muthuri, SK, Asiki, G, et al. Multimorbidity From Chronic Conditions Among Adults in Urban Slums: The AWI-Gen Nairobi Site Study Findings. Glob Heart (2021) 16:6. doi:10.5334/gh.771
36. Magodoro, IM, Esterhuizen, TM, and Chivese, T. A Cross-Sectional, Facility Based Study of Comorbid Non-Communicable Diseases Among Adults Living With HIV Infection in Zimbabwe. BMC Res Notes (2016) 9(1):379. doi:10.1186/s13104-016-2187-z
37. Nimako, BA, Baiden, F, Sackey, SO, and Binka, F. Multimorbidity of Chronic Diseases Among Adult Patients Presenting to an Inner-City Clinic in Ghana. Glob Health (2013) 9:61. doi:10.1186/1744-8603-9-61
38. Bhagavathula, AS, Seid, MA, Adane, A, Gebreyohannes, EA, Brkic, J, and Fialová, D. Prevalence and Determinants of Multimorbidity, Polypharmacy, and Potentially Inappropriate Medication Use in the Older Outpatients: Findings From EuroAgeism H2020 ESR7 Project in Ethiopia. Pharmaceuticals (2021) 14(9):844. doi:10.3390/ph14090844
39. Nwani, PO, and Isah, A. Chronic Diseases and Multimorbidity Among Elderly Patients Admitted in the Medical Wards of a Nigerian Tertiary Hospital. J Clin Gerontol Geriatr (2016) 7:83–6. doi:10.1016/j.jcgg.2015.10.001
40. Academy of Medical Sciences. Multimorbidity: A Priority for Global Health Research. United Kingdom: Academy of Medical Sciences (2018).
41. Peck, R, Mghamba, J, Vanobberghen, F, Kavishe, B, Rugarabamu, V, Smeeth, L, et al. Preparedness of Tanzanian Health Facilities for Outpatient Primary Care of Hypertension and Diabetes: A Cross-Sectional Survey. Lancet Glob Health (2014) 2(5):e285–92. doi:10.1016/S2214-109X(14)70033-6
42. Zack, RM, Irema, K, Kazonda, P, Leyna, GH, Liu, E, Spiegelman, D, et al. Determinants of High Blood Pressure and Barriers to Diagnosis and Treatment in Dar Es Salaam, Tanzania. J Hypertens (2016) 34(12):2353–64. doi:10.1097/HJH.0000000000001117
43. Singh, U, Olivier, S, Cuadros, D, Castle, A, Moosa, Y, Zulu, T, et al. The Met and Unmet Health Needs for HIV, Hypertension, and Diabetes in Rural KwaZulu-Natal, South Africa: Analysis of a Cross-Sectional Multimorbidity Survey. Lancet Glob Health (2023) 11(9):e1372–e1382. doi:10.1016/S2214-109X(23)00239-5
44. Birungi, J, Kivuyo, S, Garrib, A, Mugenyi, L, Mutungi, G, Namakoola, I, et al. Integrating Health Services for HIV Infection, Diabetes and Hypertension in Sub-Saharan Africa: A Cohort Study. BMJ Open (2021) 11(11):e053412. doi:10.1136/bmjopen-2021-053412
45. Peter, O, Agyemang, C, Wao, H, Wambiya, E, Ng'oda, M, Mwanga, D, et al. Effectiveness of Integrated Chronic Care Models for Cardiometabolic Multimorbidity in Sub-Saharan Africa: A Systematic Review and Meta-Analysis. BMJ Open (2023) 13(6):e073652. doi:10.1136/bmjopen-2023-073652
46. Yiu, KC, Rohwer, A, and Young, T. Integration of Care for Hypertension and Diabetes: A Scoping Review Assessing the Evidence From Systematic Reviews and Evaluating Reporting. BMC Health Serv Res (2018) 18(1):481. doi:10.1186/s12913-018-3290-8
Keywords: chronic conditions, infectious diseases, middle-aged, multimorbidity, non-communicable diseases, older adults, sub-Saharan Africa, Tanzania
Citation: Kohler S, Bärnighausen T, Kazonda P, Leyna GH, Lohmann J, Killewo J, Rohr JK, Stieglitz L-M and Paul N (2024) Chronic Conditions and Multimorbidity Among Middle-Aged and Elderly Peri-Urban Dwellers in Dar es Salaam, Tanzania. Int J Public Health 69:1606387. doi: 10.3389/ijph.2024.1606387
Received: 10 July 2023; Accepted: 10 June 2024;
Published: 26 June 2024.
Edited by:
Tobias Vogt, Population Research Centre, University of Groningen, NetherlandsReviewed by:
Mkhululi Wami, International Baccalaureate (IBO), NetherlandsOne reviewer who chose to remain anonymous
Copyright © 2024 Kohler, Bärnighausen, Kazonda, Leyna, Lohmann, Killewo, Rohr, Stieglitz and Paul. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Stefan Kohler, c3RlZmFuLmtvaGxlckB1bmktaGVpZGVsYmVyZy5kZQ==
†ORCID: Stefan Kohler, orcid.org/0000-0003-1365-7506; Till Bärnighausen, orcid.org/0000-0002-4182-4212; Patrick Kazonda, orcid.org/0000-0003-0215-433X; Germana H. Leyna, orcid.org/0000-0001-7016-544X; Julia Lohmann, orcid.org/0000-0003-4136-9296; Japhet Killewo, orcid.org/0000-0001-6998-6750; Julia K. Rohr, orcid.org/0000-0002-1180-8764; Laura-Marie Stieglitz, orcid.org/0000-0002-0780-9246; Nicolas Paul, orcid.org/0000-0003-2228-3980
This Original Article is part of the IJPH Special Issue “Ageing and Health in Sub-Sahara Africa”