 Filip Meckovsky
Filip Meckovsky Jana Furstova1
Jana Furstova1 Alice Kosarkova
Alice Kosarkova Zdenek Meier
Zdenek Meier Klara Malinakova
Klara Malinakova- 1Olomouc University Social Health Institute, Palacky University Olomouc, Olomouc, Czechia
- 2Department of Christian Education, Sts Cyril and Methodius Faculty of Theology, Palacky University Olomouc, Olomouc, Czechia
Objectives: This study aimed to assess the associations between loneliness and the frequency of substance use and problematic Internet use (PIU) in different age groups.
Methods: Data were collected in April 2021 from a sample of 1,293 participants with main characteristics close to a nationally representative sample (mean age = 50.1 ± 15.4 years; 56% male). We measured loneliness with the Three-Item Loneliness Scale (TILS), PIU with the General Problematic Internet Use Scale-2 (GPIUS-2) and the frequency of drugs, alcohol, smoking or caffeine consumption. Spearman’s correlation, the t-test, and one-way and multivariate linear regression models were used to analyze the data.
Results: In our study, 43.8% of respondents reported moderate to severe levels of loneliness. Loneliness was associated with the severity of PIU [F (3, 1,277) = 15.25, p < 0.001], with higher loneliness corresponding to higher PIU. No significant relationship was found between loneliness and drugs, alcohol, smoking or caffeine consumption.
Conclusion: Regardless of age, loneliness is associated with PIU but not with the frequency of substance use. Professional help for lonely people should focus on problematic Internet use in all age groups.
Introduction
Due to its severe health consequences, loneliness is considered one of the major public health threats in the 21st century [1, 2]. It is defined as a subjective socioemotional state of missing quality relationships [3], which involves feelings of not belonging and disconnectedness [4]. As the prevalence of loneliness has rapidly increased due to the COVID-19 pandemic [5, 6] and is placing a burden on both the health and the economic systems, researchers are urging governments to put loneliness among the top health policy priorities [7, 8]. Based on the data from 113 countries, Surkalim et al. [9] concluded that loneliness is occurring at problematic levels globally, with the highest rates of loneliness consistently found in Eastern European countries, which include the Czech Republic. A higher risk of loneliness has been linked to the female sex, low socioeconomic status, young and older people and chronic medical conditions [10].
Loneliness has a significant impact on both physical and mental health. So far, it has been associated with depression and anxiety [11], psychotic symptoms [12], cognitive impairment [13], paranoia [14] and even suicidal ideation and behaviors [15]. Regarding physical health, lonely people are more likely to develop coronary heart disease and stroke [16], Alzheimer’s disease [17] and have a higher risk of premature mortality, hospitalization and an emergency department visit [18]. Overall, the mortality risk connected with loneliness and social isolation is similar to obesity, substance use, mental health problems or a lack of access to healthcare [19].
As a painful experience, loneliness can lead to unhealthy behaviors, such as alcohol and drug use [20, 21], smoking, caffeine intake [22] or problematic Internet use [23]. However, some studies have come to different conclusions. For example, the study of [24] found a positive association for non-cannabis drugs only. Similarly, the relationship between the frequency of alcohol consumption and loneliness remains ambiguous, as studies have reported mixed results: loneliness was connected to more frequent or risky alcohol use by [25] or [26], whereas [11] and [27] reported a negative link between these variables. Moreover, some studies, e.g., [28] or [29], found no significant association between these variables. Recent systematic reviews have shown that considerably less research has been paid to the relationship between loneliness and smoking [30] and loneliness and coffee intake [31]. A study by [32] concluded that smokers felt lonelier than non-smokers, whereas [33] yielded the opposite result. A systematic review by Dyal and Valente [30] reported that merely half of the studies conducted found any association between loneliness and smoking, with a negative association in only one of the studies. Regarding the impact of social isolation due to the COVID-19 lockdown on changes in caffeine consumption, results show that for most individuals, caffeine consumption has not changed [31].
There is growing evidence that loneliness is associated with problematic Internet use (PIU), defined as excessive or poorly controlled urges or behavior connected to Internet use, leading to distress and disrupting major areas of life [34]. These associations have been found in various countries in Europe, Asia, and the United States [23, 35]. According to a recent meta-analytic review [36], the relationships between PIU and loneliness were stronger in studies from South Asia and Europe. However, based on current reviews [35, 37], the majority of these studies were focused on adolescents and young adults [38–40] and there is a lack of research targeting middle-aged and older adults, e.g., [41, 42]. Therefore, the aim of this study is to identify sociodemographic determinants of loneliness and to investigate the relationship between loneliness and frequency of substance use and PIU in different age groups in Czech society.
Methods
Participants and Procedure
We designed an online questionnaire to gather the necessary data. This survey was distributed by a professional agency (The Czech National Panel, Prague, Czech Republic) through its network of regular respondents. To achieve a balanced sample close to national characteristics regarding age and gender, the respondents were selected randomly using socio-demographic quotas of the Czech population. The data were obtained on the Czech adult population in April 2021 during a partial COVID-19 lockdown, when social distancing measures were in place [43]. Given the online nature of the questionnaire, to ensure high data quality, the following exclusion criteria were introduced: 1. completing the survey too quickly (under 15 min for a survey which normally lasted about 45 min); 2. inconsistent responses for repeated questions on age, height and weight (i.e., a difference of two or more units of the measure); 3. missing answers on our variables of interest). In total, 1,662 participants finished the survey, and 369 were excluded due to the criteria mentioned above. Therefore, the final sample comprised 1,293 participants aged 18–92 years (mean age = 50.1 years, SD = 15.4; 56% male).
At the beginning of the survey, participants were informed in writing about the purpose of the study, anonymization and the confidential treatment of the data. Participation in the research was fully voluntary. Respondents were required to express explicit agreement with each key point of the informed consent before starting the survey. While filling in the survey, participants could continue to the next question only after finishing the current one. However, they had the option to withdraw at any time without giving a reason. Prior to the main study, a pilot study was conducted among volunteers at Palacky University Olomouc. The study design was approved by the Ethics Committee of Palacky University Olomouc (No. 2020/06).
Measures
Loneliness
The Three-Item Loneliness Scale (TILS) [4] was used to measure perceived loneliness. It was designed for large surveys by selecting items from the UCLA Loneliness Scale [44]. The responses are coded on a three-point Likert scale: 1 = Hardly ever, 2 = Some of the time, 3 = Often. Individual scores were summed up, with the total score ranging from 3 to 9. A higher score corresponds to greater feelings of loneliness. For statistical analyses and the graphical representation, the summary score of loneliness was categorized according to [45]: none (3), mild (4–5), moderate (6–7) and severe (8–9). In the present study, the reliability of the scale was satisfactory, with Cronbach’s alpha = 0.72.
Substance Use
To assess the frequency of drug use, alcohol use, smoking and caffeine consumption, participants were asked the questions: “How often in the past month have you: a) used illegal drugs? b) drunk alcohol? c) smoked? d) drunk coffee?” with response possibilities: 1 = Never, 2 = About once or twice, 3 = About every week, 4 = More than once a week, 5 = Everyday, 6 = Many times a day.
To capture the tendency of individuals to use addictive substances, we introduced the All-substance use score, which was calculated by summing the scores for each substance, such as drugs, alcohol, smoking and caffeine. We are aware that the health consequences of frequent use of caffeine, cigarettes, alcohol and drugs are not identical. However, we included caffeine in the study because it has negative health consequences when exceeding a daily dose that is equivalent to 400 mg/day for healthy adults and is significantly lower for groups with health limitations [46]and because of its addictive character, which produces behavioral and physiological effects similar to other addictive substances [47]. Thus, in our study, we reasoned similarly as Bruno et al. [22], who added a point for each increase in consumption of alcohol, cigarettes, coffee, hypnotics, and comfort foods on a scale characterizing unhealthy lifestyle change. Scores ranged from 4 to 24, with higher scores corresponding to more frequent substance use. Since the substance use scale is not a homogeneous scale, Cronbach’s alpha was not reported.
Problematic Internet Use
The General Problematic Internet Use Scale-2 (GPIUS-2) [48] was used to measure PIU. The GPIUS-2 consists of 15 items divided into five subscales: Preference for Online Social Interaction, Mood Regulation, Cognitive Preoccupation, Compulsive Internet Use and Negative Outcomes. Items were rated on a seven-point Likert scale ranging from 1 = Definitely disagree to 7 = Definitely agree. The total score (ranging from 15 to 105) was obtained by adding up all items, with higher scores indicating greater severity of PIU. Although the GPIUS2 scale has been adapted and validated in adult populations, e.g., in the United States [48], Portugal [49], the older population has been underrepresented. Caplan [48] notes that studies on PIU include individuals who are likely to use the Internet frequently. Therefore, caution is needed in generalising the results, especially to older populations where frequent Internet use may not be as prevalent. In the present study, the reliability of the scale was high, with Cronbach’s alpha = 0.92.
Sociodemographic characteristics, such as gender (male-female), age, family status, employment status and education level, were obtained by the questionnaire. The questionnaires used can be found in Supplementary File S1.
Statistical Analysis
In the first step, we described the sociodemographic characteristics of the study sample and perceived loneliness in each group. To compare the differences in loneliness among the sociodemographic groups, we used the t-test for gender and one-way ANOVA for the rest of the variables with more than two categories. To evaluate the relationship between loneliness and substance use, non-parametric Spearman’s correlation coefficients were used for each age group, since loneliness was coded as an ordinal variable. Next, the effect of loneliness and sociodemographic groups (predictors) on substance use and PIU (dependent variables) were assessed with multivariate linear regression models. In order to assess the interaction effect of loneliness and age in the final regression models, the two predictor variables were employed in their original continuous version. All analyses were performed using the statistical software IBM SPSS version 21 (IBM Corp., Armonk, NY, United States).
Results
Table 1 describes the sociodemographic characteristics of the study sample. Of all the respondents, 229 (17.7%) reported that they were not lonely, 497 (38.4%) reported mild loneliness, 471 (36.4%) reported moderate loneliness and 96 (7.4%) reported severe loneliness. There were significant differences (p < 0.001) in the level of loneliness found between the sociodemographic groups in gender, age, marital status, employment status, as well as education level. The highest levels of perceived loneliness were associated with young people, female gender, having no partner, no paid employment and elementary education. The levels of PIU between the sociodemographic groups were differed significantly (p < 0.05) in age, employment status and education level. The highest PIU rates were associated with young age, no paid employment and elementary education. In terms of all-substance use, significant differences were found between sociodemographic groups in age and education, with the highest values for the late-middle age and secondary vocational education level.
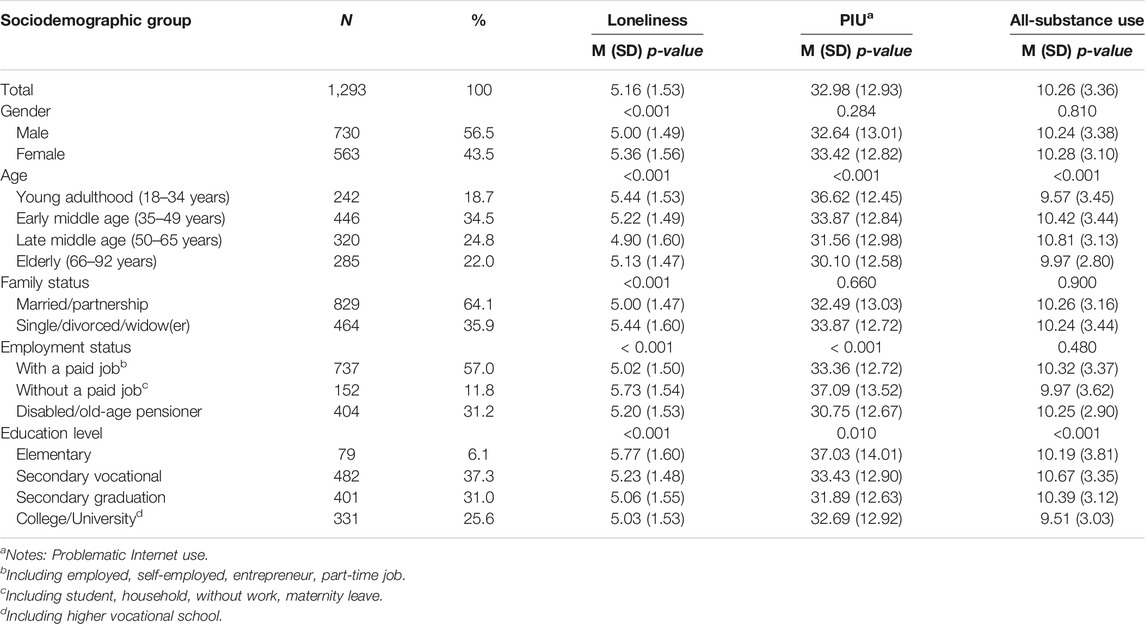
TABLE 1. Descriptive characteristics of the sample (Czechia, 2021).
The associations between loneliness and substance use are shown in Table 2. No significant relationship was found between loneliness and drugs, alcohol, smoking or caffeine consumption. The analysis revealed a significant positive correlation between loneliness and PIU for all age groups, with a medium effect size for young adults and a small effect size for other age groups. The age groups differed the most in all-substance use, with only the young group having a significant positive relationship, with a small effect size.
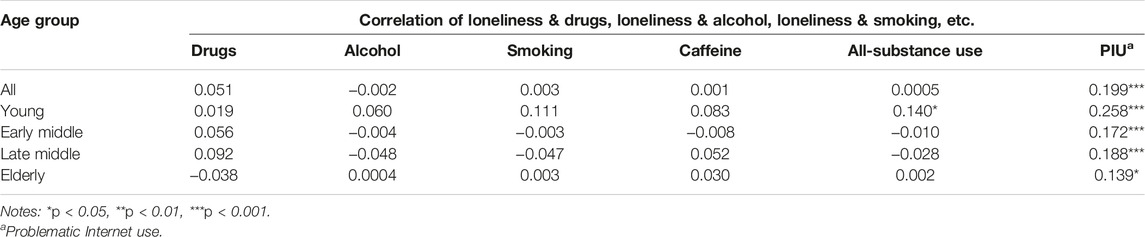
TABLE 2. Spearman’s correlation coefficients between loneliness and substance use, and loneliness and problematic Internet use stratified by the age groups (Czechia, 2021).
The effect of loneliness and the sociodemographic variables on PIU and all-substance use is presented in Supplementary Files S2, S3. The only significant predictors of PIU were loneliness and age. The sole significant predictor of all-substance use was age. Therefore, only loneliness and age were considered for further analyses.
Descriptive statistics (Table 3) showed that the severity of PIU increased with increasing levels of loneliness. There was a significant difference between loneliness groups in PIU. Post-hoc comparisons show the largest difference between the non–severe loneliness group, with a large effect size (MD = −8.562, pbonf < 0.001; d = 0.685). There was no significant difference between loneliness groups in all-substance use.
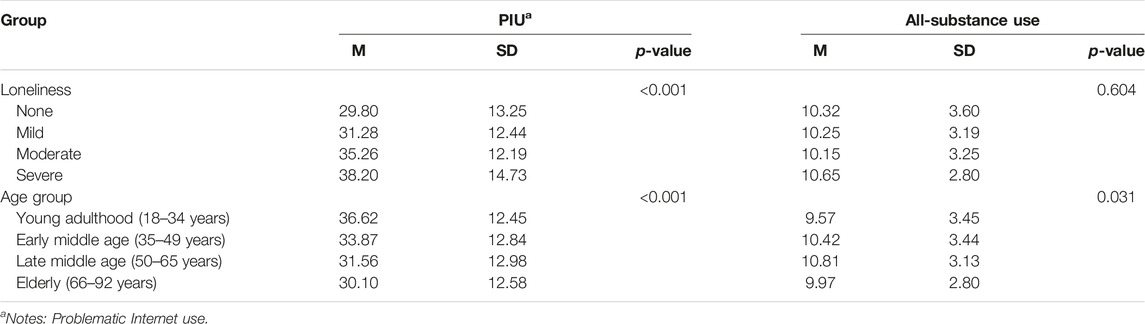
TABLE 3. Descriptive table of problematic internet use and all-substance use, stratified by loneliness groups and age groups (Czechia, 2021).
Descriptive statistics (Table 3) showed that PIU decreased with age regardless of loneliness, with the highest level found in the young group and the lowest in the elderly group. According to the post hoc analysis, the largest difference was found between the young and the elderly group, with a medium effect size (MD = −5.306, pbonf < 0.001, d = 0.424). Regarding all-substance use, the highest frequency was found in the late middle-aged and the lowest in the young group. The post hoc analysis revealed no significant difference between age groups in all-substance use.
To explore the effect of loneliness and age together with their interaction on PIU and all-substance use, further multivariate linear regression models were employed (see Table 4). Loneliness was positively associated with PIU, i.e., higher level of loneliness corresponded to higher level of PIU. Age was not a significant predictor of PIU, neither was the interaction of age and loneliness. In case of all-substance use, age was a positive significant predictor while loneliness and the interaction term were not significant at the confidence level of 95%.
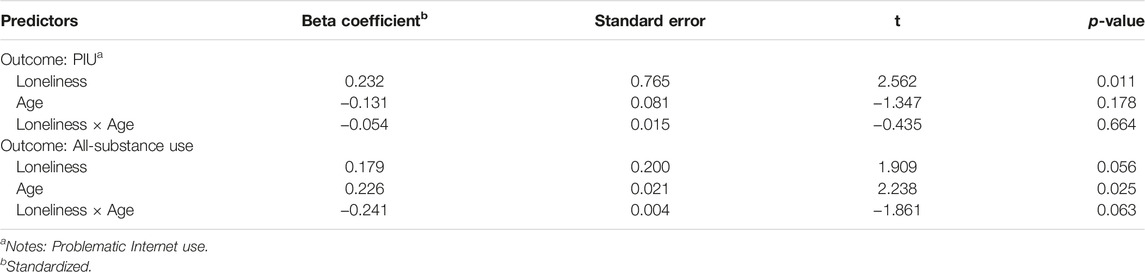
TABLE 4. Results of multivariate linear regression models assessing the effect of loneliness and age (predictors) on PIU and all-substance use (dependent variables) (Czechia, 2021).
To better understand the relationship between loneliness, PIU and all-substance according to age, group means were graphically compared (see Figures 1, 2). Figure 1 illustrates the association between loneliness and PIU stratified by age groups. It suggests that the young and late middle-age groups show an increasing trend, i.e., the level of PIU increases with higher loneliness. In the young group, however, the line segments show greater slopes, and the PIU score is higher for all loneliness levels. Therefore, the young group seems more affected by loneliness than the late middle-age group. The curve for the early middle-age group shows an increase in PIU connected to a moderate level of loneliness, followed by a decrease in PIU in the severe loneliness group. The curve for the elderly is U-shaped, with the highest PIU values in the severe loneliness group. In the mild, moderate and severe levels of loneliness, the young group scores the highest on the PIU scale compared to the other age groups.
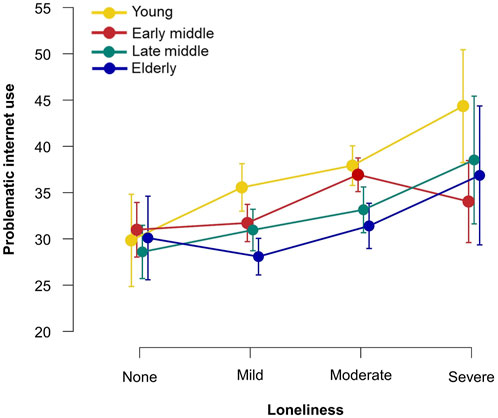
FIGURE 1. Loneliness and problematic internet use across age groups, group means and 95% confidence interval values are depicted (Czechia, 2021).
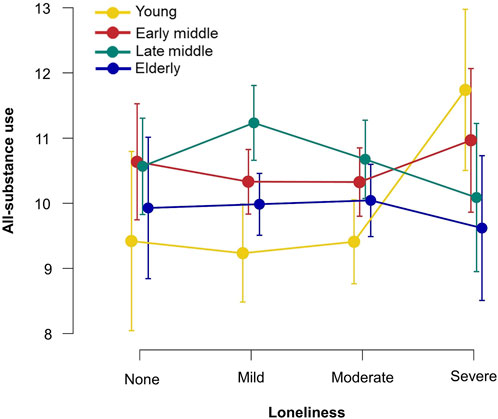
FIGURE 2. Loneliness and all-substance use across the age groups, group means, and 95% confidence interval values are depicted (Czechia, 2021).
Figure 2 shows the associations between loneliness and all-substance use, stratified by age groups. There is no clear downward or upward trend for any age group. For the young group, there is a large difference in all-substance use at the severe level of loneliness compared to lower levels. The figure shows that the early middle-age and elderly groups are not greatly affected by loneliness, as their curve does not differ by more than one point in the all-substance use scale. The curve for late middle-age has an inverted U-shaped, with the highest values in the mild loneliness group and the lowest in the severe loneliness group.
Discussion
This study aimed to assess the associations between loneliness and the frequency of substance use—such as alcohol and drug use, caffeine intake, smoking—and PIU in different age groups. Nearly half of the respondents reported moderate to severe loneliness. The highest levels of perceived loneliness were associated with young people, female gender, having no partner, no paid employment and with elementary education. The results showed no significant effect of loneliness on all-substance use. Specifically, there was no significant relationship between loneliness and the frequency of alcohol or drug use, caffeine intake or smoking. Loneliness affected the rates of PIU for each age group, with higher loneliness corresponding to higher PIU.
In our study, nearly half of the respondents reported moderate to severe levels of loneliness during a partial COVID-19 lockdown. Compared to data measured prior to the COVID-19 pandemic [50], there has been a noticeable increase in loneliness of 20% in the Czech Republic. According to a systematic review [5], there was a small increase in loneliness during COVID-19 in most countries studied in Europe and the United States. However, the results are heterogeneous due to the time and intensity of the restrictions, the population studied and the instruments used to measure loneliness. The significant increase in loneliness in the Czech Republic at the time of the COVID-19 pandemic may have been due to strict restrictions that lasted intermittently for about 7 months [43] and were loosened only at the time of our data collection.
In line with previous studies [10, 11], higher loneliness in the Czech Republic was associated with female gender, low socioeconomic status and not having a partner. However, women’s more frequent feelings of loneliness may be explained by the fact that men are more reluctant than women to express negative feelings such as loneliness [51]. This is consistent with our results, though using an online questionnaire may, according to [52], provide a safer environment for respondents to express negative feelings. Women also tend to live longer than men, so they are more likely to experience the loss of a spouse, which can be a significant factor in loneliness [52].
In line with Hansen and Slagsvold [50], loneliness was lower in groups with higher education, which may be due to their better social competence and higher economic status. In terms of age, the research to date is not entirely consistent; for example, a meta-analysis by [9] found the highest rates of loneliness in older age groups, whereas a meta-synthesis by [10] found the highest loneliness in the young and older people. Our results are in agreement with [10], where the relationship between age and loneliness was U-shaped, with high values for young and elderly compared to middle age. A likely explanation is that middle-aged people tend to be more socially involved in work and family life than the younger and older age groups.
The results did not show an effect of loneliness on substance use. Our results are consistent with [28] and [29], who found no relationship between loneliness and alcohol consumption, and with [31], who found no change in coffee consumption during the COVID-19 lockdown for most people. In contrast to our findings, a study by [22] concluded that social isolation leads to a tendency towards unhealthy habits, which included the increased frequency of alcohol, tobacco and coffee use. A possible explanation for the different results is offered by [24], who found different results between within-person and between-person effects of loneliness on alcohol, implying that loneliness increases solitary consumption but decreases social consumption. As with alcohol, we can assume that drug use, smoking and coffee drinking may represent solitary consumption or, conversely, a means of social interaction.
Our study showed the effect of loneliness on problematic Internet use, with PIU increasing with higher levels of loneliness, which is consistent with previous literature [35]. Based on this finding, we hypothesize that nowadays, the Internet represents a quicker and easier way for most people to cope with the feeling of loneliness than substance use. Internet use itself can exacerbate or reduce loneliness [37] and represents a valuable tool for deepening relationships and establishing new ones [53]. However, PIU leads to increased loneliness and, according to our results, represents a means of escape from the social world rather than a way to connect with others.
Given the lack of research examining the role of age in the relationship between PIU and loneliness, Moretta and Buodo [37] suggest exploring it more closely. In our data, no interaction effect of loneliness and age group was found for PIU. We discovered that PIU rates increased with increasing loneliness regardless of age; however, age groups differ in the strength of this relationship. Therefore, PIU appears to be a more common maladaptive method of coping with loneliness than substance use in every age group.
Strengths and Limitations
The strength of the study was the use of a large sample close to the characteristics of a nationally representative sample regarding age and gender distribution. To the best of our knowledge, this study provides the most up-to-date information on loneliness in one of the countries with the highest loneliness rates, which is the Czech Republic [9]. It is also the first to use the TILS scale in the Czech society. A limitation of our data is that the continuous variables used in the analyses do not meet the assumption of normality. Nevertheless, violation of normality of the error terms should not bias the results, as the linear regression is a robust method by the law of large numbers and the central limit theorem [54]. Further, we have used self-rating scales that may be biased by social desirability and impression management. These are particularly sensitive issues related to substance use, where people may tend not to admit the frequency of substance use. Given the online environment and the assurance of anonymity, bias could be reduced. The data were collected during the COVID-19 pandemic, which may bias the results, especially in terms of the observed prevalence of loneliness. The last limitation is the use of a cross-sectional design from which causal inferences cannot be drawn.
Implications
Our findings highlight the large degree of loneliness experienced by almost half of the Czech population in the context of the COVID-19 pandemic. Higher rates of loneliness were linked to higher rates of PIU. Therefore, professional help for lonely people should focus not only on substance use but turn its attention to PIU in all age groups. Professionals can help people find ways to use the Internet to build and deepen relationships. This may include helping clients in finding friends who share their interests, communicate online with those close to them and look for interest groups and leisure time activities to join.
For future research, we recommend distinguishing between social and lonely substance use [55], mainly smoking, coffee and alcohol drinking, which could offer deeper insight into this area. Future research could also provide information on the current state of loneliness after the end of the COVID-19 pandemic and causal inferences to confirm our claims.
Conclusion
Our results show that almost half of the people in the Czech Republic experienced problematic levels of loneliness during the COVID-19 pandemic. Higher loneliness was associated with greater severity of PIU. This trend occurs regardless of age. The result adds further evidence for addressing the problem of loneliness, which is becoming a health policy priority in the 21st century.
Ethics Statement
The studies involving humans were approved by Ethics Committee of Palacky University Olomouc (No. 2020/06). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author Contributions
Conceptualization: FM, ZM, and KM. Methodology: FM, JF, and KM. Statistical analysis: FM and JF. Interpreting results: FM and JF. Writing—original draft preparation: FM. Writing—review and editing: JF, AK, and KM. Visualization: FM. Supervision: KM, ZM, and PT. Project administration: KM, ZM, and PT. Funding acquisition: KM and PT. All authors contributed to the article and approved the submitted version.
Funding
This study was supported by the Sts Cyril and Methodius Faculty of Theology of Palacky University Olomouc, internal project Social, psychological, and spiritual determinants of health (grant number IGA_CMTF_2023_001).
Conflict of Interest
The authors declare that they do not have any conflicts of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.ssph-journal.org/articles/10.3389/ijph.2023.1606537/full#supplementary-material
References
1. Allen, J, Darlington, O, Hughes, K, and Bellis, MA. The Public Health Impact of Loneliness During the COVID-19 Pandemic. BMC Public Health (2022) 22(1):1654. doi:10.1186/s12889-022-14055-2
2. Lim, MH, Eres, R, and Vasan, S. Understanding Loneliness in the Twenty-First Century: An Update on Correlates, Risk Factors, and Potential Solutions. Soc Psychiatry Psychiatr Epidemiol (2020) 55(7):793–810. doi:10.1007/s00127-020-01889-7
3. De Jong Gierveld, J, and Van Tilburg, T. A 6-Item Scale for Overall, Emotional, and Social Loneliness - Confirmatory Tests on Survey Data. Res Aging (2006) 28(5):582–98. doi:10.1177/0164027506289723
4. Hughes, ME, Waite, LJ, Hawkley, LC, and Cacioppo, JT. A Short Scale for Measuring Loneliness in Large Surveys - Results From Two Population-Based Studies. Res Aging (2004) 26(6):655–72. doi:10.1177/0164027504268574
5. Ernst, M, Niederer, D, Werner, AM, Czaja, SJ, Mikton, C, Ong, AD, et al. Loneliness Before and During the COVID-19 Pandemic: A Systematic Review With Meta-Analysis. Am Psychol (2022) 77(5):660–77. doi:10.1037/amp0001005
6. Smith, B, and Lim, M. How the COVID-19 Pandemic Is Focusing Attention on Loneliness and Social Isolation. Public Health Res Pract (2020) 30(2):e3022008. doi:10.17061/phrp3022008
7. O’Sullivan, R, Leavey, G, and Lawlor, B. We Need a Public Health Approach to Loneliness. BMJ (2022) 376:o280. doi:10.1136/bmj.o280
8. Veazie, S, Gilbert, J, Winchell, K, Paynter, R, and Guise, JM. Addressing Social Isolation to Improve the Health of Older Adults: A Rapid Review. Rockville MD: Agency for Healthcare Research and Quality US (2019). Available from: https://pubmed.ncbi.nlm.nih.gov/30830728/ (Accessed July 18, 2023).
9. Surkalim, DL, Luo, M, Eres, R, Gebel, K, van Buskirk, J, Bauman, A, et al. The Prevalence of Loneliness Across 113 Countries: Systematic Review and Meta-Analysis. BMJ (2022) 376:e067068. doi:10.1136/bmj-2021-067068
10. Solmi, M, Veronese, N, Galvano, D, Favaro, A, Ostinelli, EG, Noventa, V, et al. Factors Associated With Loneliness: An Umbrella Review of Observational Studies. J Affect Disord (2020) 271:131–8. doi:10.1016/j.jad.2020.03.075
11. Beutel, ME, Klein, EM, Brähler, E, Reiner, I, Jünger, C, Michal, M, et al. Loneliness in the General Population: Prevalence, Determinants and Relations to Mental Health. BMC Psychiatry (2017) 17(1):97. doi:10.1186/s12888-017-1262-x
12. da Rocha, BM, Rhodes, S, Vasilopoulou, E, and Hutton, P. Loneliness in Psychosis: A Meta-Analytical Review. Schizophr Bull (2018) 44(1):114–25. doi:10.1093/schbul/sbx036
13. Peltzer, K, and Pengpid, S. Loneliness Correlates and Associations With Health Variables in the General Population in Indonesia. Int J Ment Health Syst (2019) 13(1):24. doi:10.1186/s13033-019-0281-z
14. Veronese, N, Galvano, D, D’Antiga, F, Vecchiato, C, Furegon, E, Allocco, R, et al. Interventions for Reducing Loneliness: An Umbrella Review of Intervention Studies. Health Soc Care Community (2021) 29(5):E89–96. doi:10.1111/hsc.13248
15. McClelland, H, Evans, JJ, Nowland, R, Ferguson, E, and O’Connor, RC. Loneliness as a Predictor of Suicidal Ideation and Behaviour: A Systematic Review and Meta-Analysis of Prospective Studies. J Affect Disord (2020) 274:880–96. doi:10.1016/j.jad.2020.05.004
16. Valtorta, NK, Kanaan, M, Gilbody, S, Ronzi, S, and Hanratty, B. Loneliness and Social Isolation as Risk Factors for Coronary Heart Disease and Stroke: Systematic Review and Meta-Analysis of Longitudinal Observational Studies. Heart (2016) 102(13):1009–16. doi:10.1136/heartjnl-2015-308790
17. Salinas, J, Beiser, AS, Samra, JK, O’Donnell, A, DeCarli, CS, Gonzales, MM, et al. Association of Loneliness With 10-Year Dementia Risk and Early Markers of Vulnerability for Neurocognitive Decline. Neurology (2022) 98(13):e1337–48. doi:10.1212/WNL.0000000000200039
18. National Academies of Sciences, Engineering, and Medicine. Social Isolation and Loneliness in Older Adults. Washington, D.C.: National Academies Press (2020). Available From: https://nap.nationalacademies.org (Accessed May 20, 2023).
19. Holt-Lunstad, J, Smith, TB, Baker, M, Harris, T, and Stephenson, D. Loneliness and Social Isolation as Risk Factors for Mortality: A Meta-Analytic Review. Perspect Psychol Sci (2015) 10(2):227–37. doi:10.1177/1745691614568352
20. Greig, F, Perera, G, Tsamakis, K, Stewart, R, Velayudhan, L, and Mueller, C. Loneliness in Older Adult Mental Health Services During the COVID-19 Pandemic and Before: Associations With Disability, Functioning and Pharmacotherapy. Int J Geriatr Psychiatry (2021) 37(1):10.1002/gps.5630. doi:10.1002/gps.5630
21. Ingram, I, Kelly, PJ, Deane, FP, Baker, AL, Goh, MCW, Raftery, DK, et al. Loneliness Among People With Substance Use Problems: A Narrative Systematic Review. Drug Alcohol Rev (2020) 39(5):447–83. doi:10.1111/dar.13064
22. Bruno, S, Bazzani, A, Marantonio, S, Cruz-Sanabria, F, Benedetti, D, Frumento, P, et al. Poor Sleep Quality and Unhealthy Lifestyle During the Lockdown: An Italian Study. Sleep Med (2022) 90:53–64. doi:10.1016/j.sleep.2022.01.002
23. Savolainen, I, Oksanen, A, Kaakinen, M, Sirola, A, and Paek, HJ. The Role of Perceived Loneliness in Youth Addictive Behaviors: Cross-National Survey Study. Jmir Ment Health (2020) 7(1):e14035. doi:10.2196/14035
24. Bragard, E, Giorgi, S, Juneau, P, and Curtis, BL. Daily Diary Study of Loneliness, Alcohol, and Drug Use During the COVID-19 Pandemic. Alcohol Clin Exp Res (2022) 46(8):1539–51. doi:10.1111/acer.14889
25. Gutkind, S, Gorfinkel, LR, and Hasin, DS. Prospective Effects of Loneliness on Frequency of Alcohol and Marijuana Use. Addict Behav (2022) 124:107115. doi:10.1016/j.addbeh.2021.107115
26. Wakabayashi, M, Sugiyama, Y, Takada, M, Kinjo, A, Iso, H, and Tabuchi, T. Loneliness and Increased Hazardous Alcohol Use: Data From a Nationwide Internet Survey With 1-Year Follow-Up. Int J Environ Res Public Health (2022) 19(19):12086. doi:10.3390/ijerph191912086
27. Canham, SL, Mauro, PM, Kaufmann, CN, and Sixsmith, A. Association of Alcohol Use and Loneliness Frequency Among Middle-Aged and Older Adult Drinkers. J Aging Health (2015) 28(2):267–84. doi:10.1177/0898264315589579
28. Rhew, IC, Cadigan, JM, and Lee, CM. Marijuana, But Not Alcohol, Use Frequency Associated With Greater Loneliness, Psychological Distress, and Less Flourishing Among Young Adults. Drug Alcohol Depend (2021) 218:108404. doi:10.1016/j.drugalcdep.2020.108404
29. Richardson, T, Elliott, P, and Roberts, R. Relationship Between Loneliness and Mental Health in Students. J Public Ment Health (2017) 16(2):48–54. doi:10.1108/jpmh-03-2016-0013
30. Dyal, SR, and Valente, TW. A Systematic Review of Loneliness and Smoking: Small Effects, Big Implications. Subst Use Misuse (2015) 50(13):1697–716. doi:10.3109/10826084.2015.1027933
31. Bakaloudi, DR, Evripidou, K, Jayawardena, R, Breda, J, Dardavessis, T, Poulia, KA, et al. The Impact of Lockdowns on Caffeine Consumption: A Systematic Review of the Evidence. Int J Environ Res Public Health (2022) 19(9):5255. doi:10.3390/ijerph19095255
32. Habibi, M, Hosseini, F, Darharaj, M, Moghadamzadeh, A, Radfar, F, and Ghaffari, Y. Attachment Style, Perceived Loneliness, and Psychological Well-Being in Smoking and Non-Smoking University Students. J Psychol (2018) 152(4):226–36. doi:10.1080/00223980.2018.1446894
33. Zhang, CL, Xu, YM, and Zhong, BL. The Association Between Smoking and Loneliness Among Chinese University Freshmen. Ann Transl Med (2020) 8(10):649. doi:10.21037/atm-20-3523
34. Banz, BC, Yip, SW, Yau, YHC, and Potenza, MN. Behavioral Addictions in Addiction Medicine: From Mechanisms to Practical Considerations. Prog Brain Res (2016) 223:311–28. doi:10.1016/bs.pbr.2015.08.003
35. Saadati, HM, Mirzaei, H, Okhovat, B, and Khodamoradi, F. Association Between Internet Addiction and Loneliness Across the World: A Meta-Analysis and Systematic Review. Ssm-Popul Health. (2021) 16:100948. doi:10.1016/j.ssmph.2021.100948
36. Cai, Z, Mao, P, Wang, Z, Wang, D, He, J, and Fan, X. Associations Between Problematic Internet Use and Mental Health Outcomes of Students: A Meta-Analytic Review. Adolesc Res Rev (2023) 8(1):45–62. doi:10.1007/s40894-022-00201-9
37. Moretta, T, and Buodo, G. Problematic Internet Use and Loneliness: How Complex Is the Relationship? A Short Literature Review. Curr Addict Rep (2020) 7(2):125–36. doi:10.1007/s40429-020-00305-z
38. Bayat, N, Fokkema, T, Mujakovic, S, and Ruiter, RAC. Contextual Correlates of Loneliness in Adolescents. Child Youth Serv Rev (2021) 127:106083. doi:10.1016/j.childyouth.2021.106083
39. Costa, RM, Patrao, I, and Machado, M. Problematic Internet Use and Feelings of Loneliness. Int J Psychiatry Clin Pract (2019) 23(2):160–2. doi:10.1080/13651501.2018.1539180
40. Ozsaker, M, Muslu, GK, Kahraman, A, Beytut, D, Yardimci, F, and Basbakkal, Z. A Study on the Effects of Loneliness, Depression and Perceived Social Support on Problematic Internet Use Among University Students. Anthropologist (2015) 19(2):533–42. doi:10.1080/09720073.2015.11891688
41. Meshi, D, Cotten, SR, and Bender, AR. Problematic Social Media Use and Perceived Social Isolation in Older Adults: A Cross-Sectional Study. Gerontology (2020) 66(2):160–8. doi:10.1159/000502577
42. Khalaila, R, and Vitman-Schorr, A. Internet Use, Social Networks, Loneliness, and Quality of Life Among Adults Aged 50 and Older: Mediating and Moderating Effects. Qual Life Res (2018) 27(2):479–89. doi:10.1007/s11136-017-1749-4
43. Slabá, J. Vládní Boj Proti Pandemii: Přehled Opatření Vydaných v Souvislosti s Pandemií Onemocnění Covid-19 v Česku v Letech 2020 a 2021. Demografie (2022) 64(2):175–96. doi:10.54694/dem.0303
44. Russell, D, Peplau, L, and Cutrona, C. The Revised Ucla Loneliness Scale - Concurrent and Discriminant Validity Evidence. J Pers Soc Psychol (1980) 39(3):472–80. doi:10.1037//0022-3514.39.3.472
45. Matthews, T, Bryan, BT, Danese, A, Meehan, AJ, Poulton, R, and Arseneault, L. Using a Loneliness Measure to Screen for Risk of Mental Health Problems: A Replication in Two Nationally Representative Cohorts. Int J Environ Res Public Health (2022) 19(3):1641. doi:10.3390/ijerph19031641
46. Temple, JL, Bernard, C, Lipshultz, SE, Czachor, JD, Westphal, JA, and Mestre, MA. The Safety of Ingested Caffeine: A Comprehensive Review. Front Psychiatry (2017) 8:80. doi:10.3389/fpsyt.2017.00080
47. Meredith, SE, Juliano, LM, Hughes, JR, and Griffiths, RR. Caffeine Use Disorder: A Comprehensive Review and Research Agenda. J Caffeine Res (2013) 3(3):114–30. doi:10.1089/jcr.2013.0016
48. Caplan, SE. Theory and Measurement of Generalized Problematic Internet Use: A Two-Step Approach. Comput Hum Behav (2010) 26(5):1089–97. doi:10.1016/j.chb.2010.03.012
49. Pontes, HM, Caplan, SE, and Griffiths, MD. Psychometric Validation of the Generalized Problematic Internet Use Scale 2 in a Portuguese Sample. Comput Hum Behav (2016) 63:823–33. doi:10.1016/j.chb.2016.06.015
50. Hansen, T, and Slagsvold, B. Late-Life Loneliness in 11 European Countries: Results From the Generations and Gender Survey. Soc Indic Res (2016) 129(1):445–64. doi:10.1007/s11205-015-1111-6
51. Office for National Statistics. Loneliness - What Characteristics and Circumstances Are Associated With Feeling Lonely? (2018). Available From https://www.basw.co.uk/ (Accessed July 20, 2023).
52. Barreto, M, Victor, C, Hammond, C, Eccles, A, Richins, MT, and Qualter, P. Loneliness Around the World: Age, Gender, and Cultural Differences in Loneliness. Personal Individ Differ (2021) 169:110066. doi:10.1016/j.paid.2020.110066
53. Nowland, R, Necka, EA, and Cacioppo, JT. Loneliness and Social Internet Use: Pathways to Reconnection in a Digital World? Perspect Psychol Sci (2018) 13(1):70–87. doi:10.1177/1745691617713052
54. Gelman, A, Hill, J, and Vehtari, A. Regression and Other Stories. Cambridge: Cambridge University Press (2020).
55. Cooper, ML, Kuntsche, E, Levitt, A, Barber, LL, and Wolf, S. Motivational Models of Substance Use: A Review of Theory and Research on Motives for Using Alcohol, Marijuana, and Tobacco. In: The Oxford Handbook of Substance Use and Substance Use Disorders, Vol 1. New York, NY, US: Oxford University Press (2016). p. 375–421.
Keywords: loneliness, social isolation, problematic internet use, substance use, COVID-19
Citation: Meckovsky F, Furstova J, Kosarkova A, Meier Z, Tavel P and Malinakova K (2023) Loneliness Is Associated With Problematic Internet Use but Not With the Frequency of Substance Use: A Czech Cross-Sectional Study. Int J Public Health 68:1606537. doi: 10.3389/ijph.2023.1606537
Received: 22 August 2023; Accepted: 22 October 2023;
Published: 02 November 2023.
Edited by:
Daniela Husarova, University of Pavol Jozef Šafárik Kosice, SlovakiaReviewed by:
Maddalena Fiordelli, University of Italian Switzerland, SwitzerlandJoanna Mazur, University of Zielona Góra, Poland
Copyright © 2023 Meckovsky, Furstova, Kosarkova, Meier, Tavel and Malinakova. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Filip Meckovsky, ZmlsaXAubWVja292c2t5QG91c2hpLnVwb2wuY3o=