 Le Tu Hoang1*
Le Tu Hoang1* Vu Tri Duc2Vo Van Duc Ngoc2Ngo Xuan Truong3Nguyen Thi Nhat Thanh3Phan Thi Thu Trang4Sumeet Saksena5
Vu Tri Duc2Vo Van Duc Ngoc2Ngo Xuan Truong3Nguyen Thi Nhat Thanh3Phan Thi Thu Trang4Sumeet Saksena5 Nguyen Thi Trang Nhung1
Nguyen Thi Trang Nhung1- 1Department of Biostatistics, Hanoi University of Public Health, Hanoi, Vietnam
- 2National Children’s Hospital, Hanoi, Vietnam
- 3Faculty of Information Technology, University of Engineering and Technology—Vietnam National University, Hanoi, Vietnam
- 4Department of Environmental Health, Hanoi University of Public Health, Hanoi, Vietnam
- 5East-West Center, Honolulu, HI, United States
Objectives: This paper explores the potential reduction in the number of deaths and the corresponding economic benefits in Vietnam that could have arisen from the decreased in concentrations of particulate matter with a diameter of 2.5 μm or less (PM2.5) and nitrogen dioxide (NO2).
Methods: Using Global Exposure Mortality Models, we estimated the potential health and economic benefits on people aged 25 and above across Vietnam’s 63 provinces. The counterfactual scenario assumed reducing PM2.5 and NO2 concentrations to levels observed during the two COVID-19 epidemic waves in 2021 with national lockdowns and activity restrictions.
Results: In 2019, PM2.5 concentrations ranged from 12.8 to 40.8 μg/m3 while NO2 concentrations ranged between 2.9 and 36.98 μg/m3. The reduced levels of PM2.5 and NO2 resulted in 3,807 (95% CI: 2,845–4,730) and 2,451 (95% CI: 2,845–4,730) avoided deaths of adults aged 25 and above due to non-injury-related causes, respectively. Considering that every prevented death represents potential tangible and intangible cost savings, reduced levels of PM2.5 and NO2 concentrations during COVID-19 restrictions would have resulted in economic benefits of $793.0 million (95% CI: 592.7–985.4) and $510.6 million (95% CI: 381.3–634.9), respectively.
Conclusion: The COVID-19 lockdown led to decreased PM2.5 and NO2 concentrations, benefiting health and economy in Vietnam. Our findings highlight the potential advantages of implementing air quality control policies in the country.
Introduction
Air pollution (AP) is a threat to health across the world, as evident in many epidemiological studies [1, 2]. Accordingly, air pollution is both the cause and the exacerbating factor of respiratory and cardiovascular diseases, cancer, stroke, and even millions of premature deaths each year globally [3, 4]. According to World Health Organization (WHO), AP is responsible for: 43% of deaths and morbidity from chronic obstructive pulmonary disease (COPD); 25% of deaths from coronary heart disease; 24% of deaths due to stroke; 17% of deaths and morbidity due to acute lower respiratory tract infections; and 29% of lung cancer deaths and illnesses [4]. In Vietnam, AP ranks in the top five risk factors for the burden of disease and premature death in 2019, just behind high blood pressure, smoking, diabetes, and nutritional risk [5].
Typically, human activities such as traffic, industrial activities and electricity generation contribute to ambient air pollution [6]. PM2.5 (particulate matter with aerodynamic diameter below 2.5 µm) and NO2 (nitro dioxide) rank as some of the most critical outdoor pollutants, as highlighted by the World Health Organization [4]. These sources can be modified by changing activity levels or reducing the intensity of the emissions [7]. In the United States, air pollution regulation has historically focused on reducing emission factors rather than modifying activity levels. While past studies have looked at how sudden changes in emission sources impact air quality [8–11], physical distancing measures introduced in response to COVID-19 provide a unique opportunity to observe and measure the effects of modifiable factors—such as large reductions in activity—on ambient air pollution in real time, with unprecedented scope, speed, and duration [12]. After the first COVID-19 case was detected, physical distancing had been implemented in Vietnam from a very early phase as one of the effective ways to mitigate the spread of COVID-19 [13]. During the physical distancing periods, Vietnam government had applied many proper solutions including residential area quarantine; closing of schools, supermarkets/markets, and restaurants; travel restrictions, public gathering restrictions, etc. [14, 15].
These solutions, which were implemented to prevent the spread of COVID-19, also reduced the emissions into the atmosphere, resulting in significantly cleaner air and, presumably, a healthier population [16–18]. A study conducted across 34 countries showed that the lockdown in 2020 reduced 31% of PM2.5 concentrations, leading to approximately 49,900 deaths avoided [16, 17]. Another study in 367 Chinese cities found that reductions in nitrogen dioxide (NO2) during the lockdown period helped avoid approximately 4,711 deaths [18]. In Vietnam, the implemented policies to control the spread of COVID-19 also improved the air quality. For instance, PM2.5 and NO2 concentrations obtained from the automatic ambient air quality monitoring station dropped by approximately 75.8% and 41.8%, respectively, during the lockdowns (1st–22nd of April 2020) in Hanoi [15]. Another study also showed that NO2 concentrations in Hanoi decreased between 24% and 32% in the 2 weeks after the COVID-19 lockdowns [14]. Among air pollutants, Vietnam is suffering from PM2.5 pollution as a result of local activities and long-range pollutant transport [15]. Despite the evidence of the air quality improvement, no study in Vietnam estimated the health effects of the change in the ambient pollution attributed to COVID-19 preventive measures.
In Vietnam, several studies have estimated the number of avoidable deaths if the air quality was controlled at certain levels [19–22]. The standard levels included the WHO air quality guidelines and the Vietnam National Ambient Air Quality Standards (denoted by QCVN 05:2013) [19–22]. On the other hand, the air pollutant reduction during COVID-19 provided an opportunity for a “natural experiment” to assess the health and economic benefits of pollution reduction. This paper aims to estimate the number of avoidable deaths and economic benefits in 63 provinces in Vietnam by reducing PM2.5 and NO2 concentrations to 2021 levels. The presumed reduction in concentration is based on the effects of lockdowns and activity restrictions.
Methods
Materials
PM2.5 Concentration Data
To obtain an annual average of PM2.5 in 2019 (before the COVID-19 pandemic) and 2021 (during COVID-19-related lockdowns and activity restrictions), the daily PM2.5 concentration maps in Vietnam were developed based on a Mixed Effects Model (MEM) [23] using data collected from 2012 to 2021. In 2021, there were two waves of the COVID-19 epidemic. The first wave occurred from January to April, while the second wave extended from April to December. During both waves, authorities implemented lockdowns and activity restrictions. Given the continuing occurrence of epidemic waves, we opted to select the 2021 level as the counterfactual scenario for analysis. The input data included air pollution monitoring station measurements, satellite products of Aerosol Optical Depth (AOD), meteorological maps for humidity, Planetary Boundary Layer Height (PBLH), land-use maps of traffic, normalized difference vegetation index (NDVI), and terrain.
Measured PM2.5 data was collected from standard stations nationwide under the management of the Northern Center of Environmental Monitoring, the US Embassy, and the Vietnam National University Ho Chi Minh City. Our satellite data consisted of AOD products of Aqua/Terra MODIS and Suomi NPP VIIRS from 2012 to 2021, obtained from the National Aeronautics and Space Administration (NASA) through their public open access sites. The meteorological data was the output of the Weather Research and Forecasting (WRF) model [24], customized for Vietnam, with the fifth generation ECMWF reanalysis (ERA-5) data used as the input. The Normalized difference vegetation index (NDVI) maps from Terra MODIS [25] were also collected from NASA from 2012 to 2021. A road map containing the shapes of road types was collected in vector format from the latest Open Street Map in 2022. Terrain map (DEM) containing information about terrain height was collected from ASTER Global source in 2019 [26].
The steps taken to develop the map included pre-processing the station measurements and maps data; enhancing the quality of the satellite AOD; integrating the map data with the station measurements; developing and validating the MEM model; estimating the daily PM2.5 values across the nation to make PM2.5 maps; aggregating the daily maps into the monthly and/or annual mean maps of PM2.5 for 2019 and 2021; and evaluating the maps with station measurements and comparing the outputs with the global PM2.5 products. Detailed methodology is presented by [27].
NO2 Concentration Data
This study used data on NO2 concentrations from results of Truong et al. in 2021 [28]. This data was created from validating NO2 satellite images of the troposphere and ground-level NO2 observations in Vietnam. The satellite data was collected spanning January to May of 2019 and the entirety of 2020 using the Level 2 TROPOMI sensor of the Sentinel-5P satellite. Ground observations data were collected from three automatic monitoring stations in North Vietnam (Hanoi, Quang Ninh, Viet Tri) and three in central Vietnam (Hue, Da Nang, and Nha Trang operated by the VEA (Vietnam Environment Administration), and a monitoring station in Hanoi belonging to Hanoi EPA (Environment Protection Agency). The detailed validation methodology was described by [28].
Population Data
The population data (Pop) in this study was extracted from the “Vietnam population and housing census in 2019” [29]. The data includes the total number of people for each age group and district in all 63 provinces of Vietnam.
Mortality Estimation
The age-specific mortality rate (per 100,000 population) due to non-injury causes, denoted by MR, for each district was estimated from two measurements, including the national crude mortality rate in 2019 and the injury-related mortality rate by age group [30, 31]. The first measurement was derived from the General Statistics Office webpage in Vietnam (denoted by GSO, 2019) [29]. This webpage provided the crude mortality rate (per 1,000 population) for each province in Vietnam. The second measurement was retrieved from the Vietnam National Injury Survey in 2010 (denoted by VNIS, 2010) [31]. We used the estimated mortality rate (per 100,000 population) for 5 years-age groups.
Three assumptions were made to calculate each district’s age-specific mortality rate due to all-natural causes. First, we hypothesized that the crude mortality rate was uniform within a province, meaning that within a province each district’s crude mortality rate in 2019 was the same. Second, we assumed that the injury-related mortality rate had stayed the same since 2010 as no other more recent national data were available. Third, we applied the mortality rate of each 5 years-age group from the Vietnam National Injury survey to all districts in Vietnam, meaning that the injury mortality rate of each age group is the same for every district.
Based on these assumptions, we estimate the number of deaths for non-injury causes (by age group in each district) by the following formula:
where
Calculation of Number of Avoidable Deaths
We hypothesized that if the same interventions that had been implemeted during the COVID-19 pandemic (2021) had been implemented during 2019, the annual concentration of PM2.5 and NO2 in 2019 would have been reduced to the corresponding concentration in 2021, and the number of non-injury mortality would have declined.
Concentration-Response Function for PM2.5
We estimated the number of avoidable deaths attributed to PM2.5 reduction using the Global Exposure Mortality Models for non-communicable diseases (e.g., cardiovascular diseases, chronic respiratory diseases, cancer…) and lower respiratory infections (denoted by GEMM NCD + LRI) [2]. This function was chosen because it was developed based on a study in multiple areas, where the PM2.5 concentration is high. This function was also validated and adjusted to used in different countries. The following formula was used:
where
Concentration-Response Function for NO2
For NO2, we applied the log-linear model with a beta coefficient (
where RR is the relative risk of death due to the change of NO2; β is the slope of the model; and
Number of Avoidable Deaths
The number of avoidable deaths attributed to the reduction of air pollutant concentrations was estimated as outlined below:
where AN is the avoidable number of deaths for each province/city, HR (or RR) is the hazard ratio (or the relative risk) estimated from the concentration-response function, MRi,j and Popi,j is the mortality rate and the total number of people of i age group and j district. This figure is reported along with its 95% confidence interval for each province, ecological zone, and region in Vietnam. The 95% confidence intervals were calculated using Monte Carlo simulation in BENMAP-CE software.
Economic Value Calculation
We used the value of a statistical life (VSL) approach to calculate the economic benefits of premature death. We calculated VSL using the individual willingness to pay (WTP) to decrease the risk of death [33]. This figure considers the intangible costs, including the value of suffering and leisure time lost, and demonstrates the tangible costs of medical treatment [34]. To assess the economic benefits in this study, we multiplied the predicted number of avoided deaths by a locally valid estimation of VSL [35]. Ideally, local studies should be utilized to estimate the economic loss. Owing to the absence of such local studies, however, we used the benefit-transfer approach to transfer unit health costs from foreign studies to the local context [33, 36] by using the formula:
where
The health economic value was calculated by multiplying the number of avoided deaths with an estimated economic value per case (VSLVietnam, 2019)—this estimated to be approximately $208,324.9. All calculations were done using BenMAP-CE 1.5.8 provided by the US Environmental Protection Agency (US EPA) [39]. We also used QGIS 3.30 to illustrate the results in three different regions (Northern, Central, and Southern Vietnam).
Ethical Considerations
The studies involving human participants were reviewed and approved by The Ethics Committee of Hanoi University of Public Health under Decision No. 318/2020/YTCC-HD3 dated 30 July 2020. The ethics committee waived the requirement of written informed consent for participation.
Results
Comparison of PM2.5 and NO2 Concentration Before and After COVID-19 in Vietnam
The results, presented in Figure 1, indicate that the Red River Delta region in the northern part of the country had the highest levels of PM2.5 and NO2 in all years. In 2019, the annual average PM2.5 concentrations in these provinces ranged from 12.8 to 40.8 μg/m3, whereas in 2021 they ranged from 11.5 to 36.9 μg/m3. The NO2 concentrations ranged from 2.9 to 36.9 μg/m3 in 2020 and from 2.8 to 36.1 μg/m3 in 2021, indicating some reduction in NO2 levels over the study period. Compared to 2019, the average PM2.5 concentrations in all ecological zones decreased in 2021, whereas NO2 concentrations decreased in only five of the eight zones, including the Red River Delta, Northeast, Northwest, North and South-Central coast. The reductions in annual PM2.5 concentrations across the 63 provinces of Vietnam ranged from 5.7% to 10.3%. Detailed information of PM2.5 and NO2 concentration for each province was described in Supplementary Table S1.
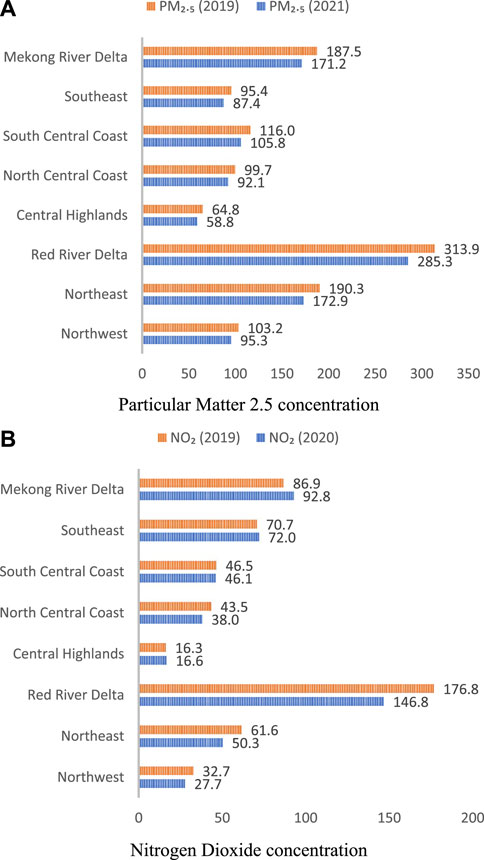
FIGURE 1. Annual average particular matter 2.5 (A) and nitrogen dioxide (B) concentrations by ecological zones (Vietnam. 2019–2021).
Table 1 shows that there was a reduction in PM2.5 concentrations in all ecological zones, ranging from 7.6% in the Northeast zone to 9.3% in the North central coast zone. In the case of NO2, the reductions varied across zones, ranging from 0.9% in the Central Highlands to 18.3% in the Northwest zone. However, due to agriculture activities (burning straw, crop residues and biomass), there was an increase in NO2 concentrations in some zones, including the North Central Coast (2.1%), Southeast (1.8%), and Mekong River Delta (6.8%).
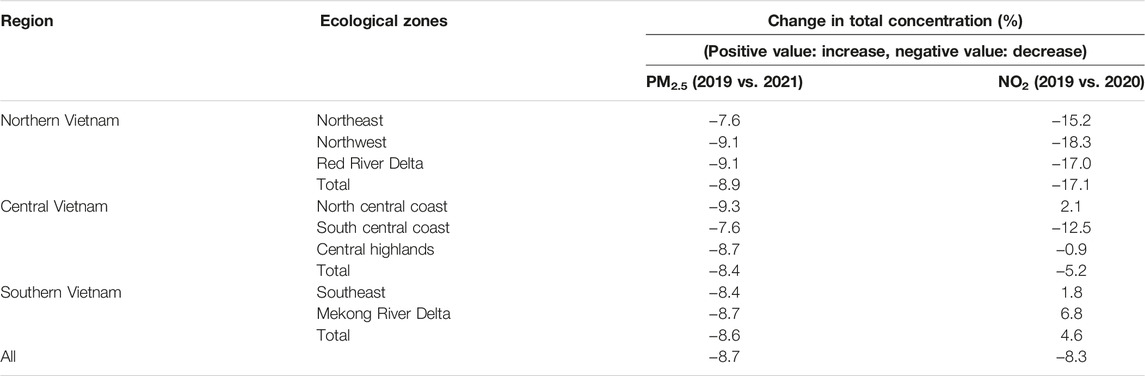
TABLE 1. Change in total concentrations of air pollutants by ecological zones (Vietnam. 2019–2021).
Crude Mortality Rate in Vietnam in 2019
Figure 2 displays the crude mortality rates of each Vietnamese province in 2019. The highest crude mortality rates were observed in the northern provinces, followed by the Central region and Southern region. In contrast, the Central highlands, including provinces such as Kon Tum, Gia Lai, Dak Lak, and Dak Nong, had lower mortality rates, with approximately less than six deaths per 1,000 population.
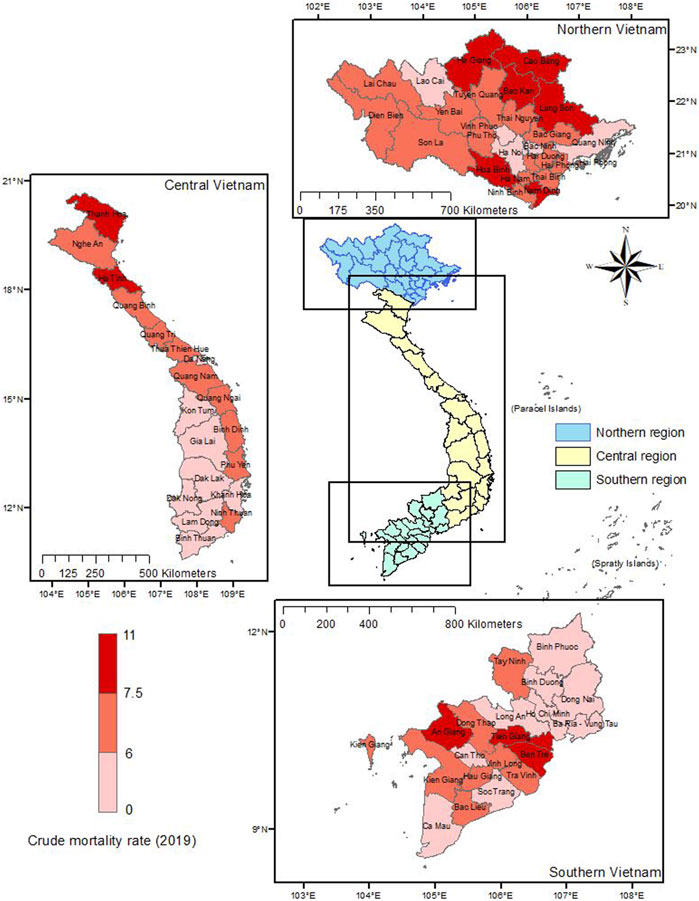
FIGURE 2. Crude mortality rate by province (Vietnam. 2019).
Avoidable Deaths
Figure 3 displays the number of avoidable deaths attributed to the reduction in PM2.5 concentrations in 2019. The highest number of avoidable deaths due to PM2.5 was observed in the Northern region, with a total of 1,990 deaths (95% CI: 1,488–2,472). In the Central region, this figure was lower at 1,071 deaths (95% CI: 801–1,331), while the Southern part of Vietnam had the lowest number of avoidable deaths at 745 (95% CI: 557–926). If air quality management measures had been implemented to maintain the air quality as it was during the COVID-19 pandemic, the highest number of avoidable deaths in 2019 would have been 430 cases (95% CI: 330–540). The province with the lowest avoidable deaths was Ba Ria–Vung Tau in the south, with only about 7 deaths (95% CI: 5.1–8.5). In the central areas of Vietnam, Thanh Hoa had the highest number of avoidable deaths, with approximately 250 cases (95% CI: 190–310).
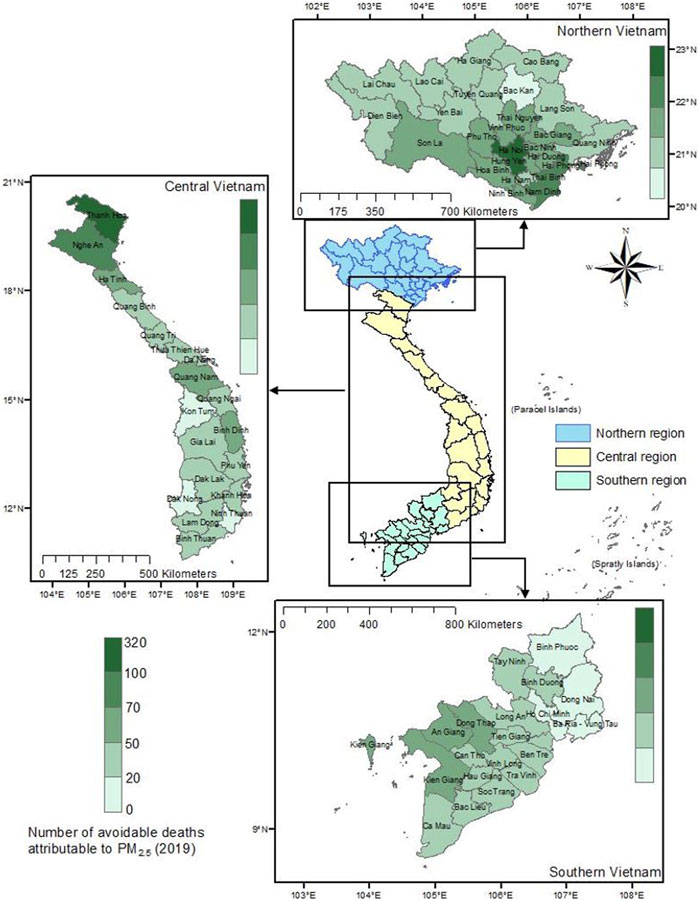
FIGURE 3. Number of avoidable deaths in 2019 by province if particular matter 2.5 concentrations were reduced to 2021 levels (Vietnam. 2019).
Avoidable Deaths When Adjusting the NO2 Concentration in Vietnam
Figure 4 illustrates the total number of avoidable deaths attributed to NO2. Similar to the trend observed for PM2.5, the Northern region of Vietnam had the highest number of avoidable deaths, with 1,494 deaths (95% CI: 1,117–1,857), while the Southern region had the lowest, with only 421 avoidable deaths (95% CI: 314–524). The highest number of avoidable deaths was seen in Ha Noi (315 avoidable deaths, 95% CI: 236–392), Thanh Hoa (174 avoidable deaths, 95% CI: 130–217), Nghe An (130 avoidable deaths, 95% CI: 98–163), and Bac Giang (107 avoidable deaths, 95% CI: 80–133). Compared to these provinces, the mortality rates in the Southern provinces were significantly lower, ranging from 3 (Ba Ria–Vung Tau) to 37 (Tien Giang) avoidable deaths. Even in Ho Chi Minh City, only approximately 5 deaths could have been avoided.
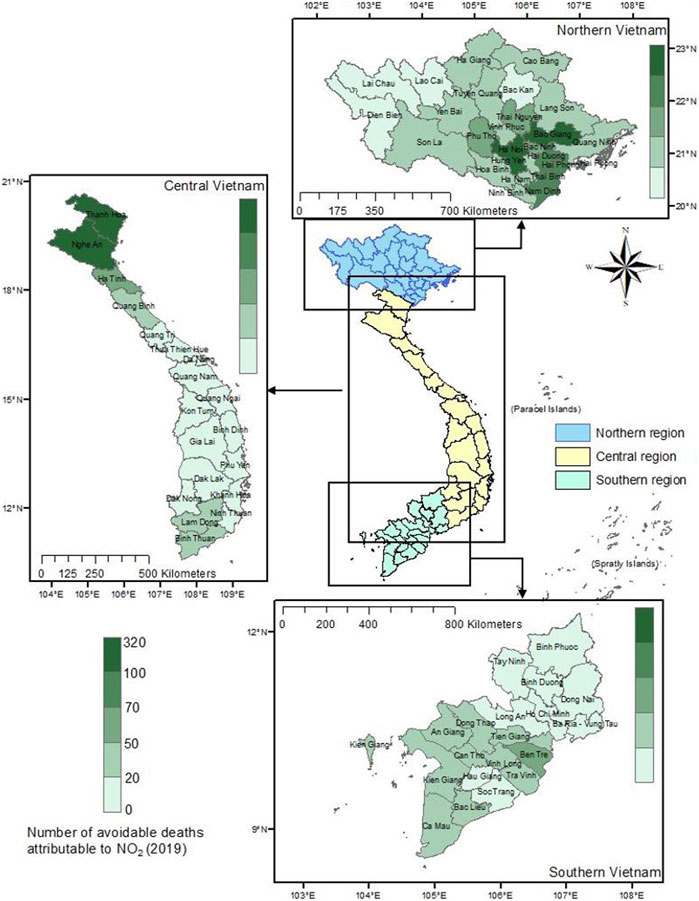
FIGURE 4. Number of avoidable deaths in 2019 by province if nitro dioxide concentrations were reduced to 2021 levels (Vietnam. 2019).
Economic Benefits
Table 2 displays the total number of avoidable deaths and corresponding economic benefits for each region in Vietnam. Considering that economic benefits represent the intangible costs, including the value of suffering and leisure time lost, and demonstrates the tangible costs of medical treatment. Overall, reducing PM2.5 concentrations could have prevented approximately 3,807 deaths (95% CI: 2,845–4,730) in Vietnam in 2019, resulting in potential savings of up to $793.0 million (95% CI: 592.7–985.4). The Red River Delta region would have benefited the most economically from this reduction, with potential savings of about $414.6 million. Additionally, reducing NO2 concentrations could have prevented a total of 2,451 deaths (95% CI: 1,830–3,047), resulting in potential savings of approximately $510.6 million (95% CI: 381.3–634.9). Once again, the Red River Delta region would have benefited the most economically from this reduction, with potential savings of almost $311.3 million.
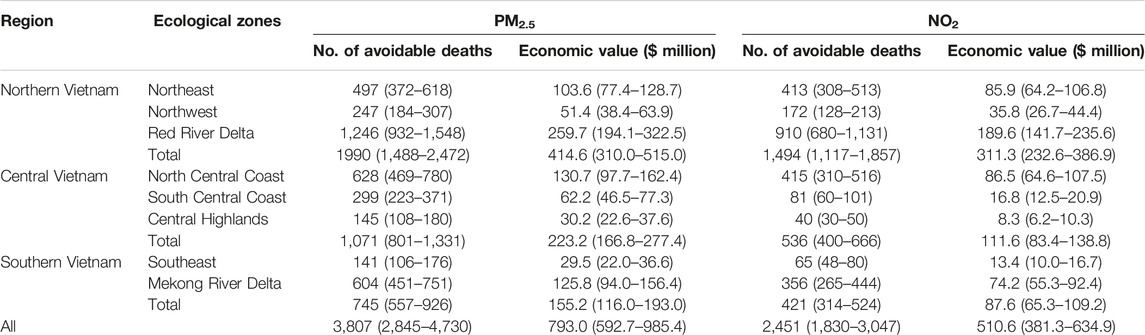
TABLE 2. Economic benefits of air pollutants concentration reduction (Vietnam. 2019).
Discussion
Our study is among the few studies to perform a nation-wide health impact assessment of air pollution in Vietnam. There have been several prior studies assessing the burden of mortality attributed to air pollution, typically PM2.5 [19–22]. However, these studies only estimated the burden of PM2.5 attributable deaths in smaller regions of the country, for example, in the megacities such as Hanoi [20] and Ho Chi Minh city [19, 22]. A recent study conducted such an assessment for multiple sites, including ten provinces in Northern Vietnam, and Ho Chi Minh City (which is in the south) [21]. However, such studies used the WHO Air Quality Guidelines (5 and 10 μg/m3 for annual PM2.5 and NO2, respectively) and the Vietnam National Ambient Air Quality Standards (QCVN 05:2013) (25 and 40 μg/m3 for annual PM2.5 and NO2, respectively) as the counterfactual level to estimate the attributable burden of air pollution [19–22]. These levels, however, were challenging to attain not only for recent periods but also in the near future since the air pollution level in 2019 of many provinces, especially in the Red River Delta, far exceeded the QCVN 05:2013 standards. While another study highlighted the failure of provinces to meet the WHO air quality guidelines [40], our results demonstrated that PM2.5 exceeded by 7–30 μg/m3 and NO2 by 1–26 μg/m3 in the majority of provinces. In contrast, we assessed the impact using the air pollutant concentration in 2021 as a counterfactual level. This level was achieved by implementing stringent interventions to prevent the spread of COVID-19. Thus, applying this realistically achievable level may provide more practical evidence of health benefits attributed to air pollution reduction.
In Vietnam, some primary emission sources of PM2.5 include agricultural by-product burning, traffic, industrial activities, and craft villages [41]. Craft villages in Vietnam contribute to air pollution emissions through their traditional production techniques, which involve the burning of diverse materials and fuels. Examples of such villages include pottery-making communities, incense stick crafting villages, and blacksmithing villages, all of which engage in practices that result in the release of pollutants into the atmosphere. During the COVID-19 pandemic, public health and social measures had been applied by the Vietnam government, including: work from home agreements, school closures, restriction on public gatherings, lockdowns, border closures, isolation, and quarantine areas [42]. Therefore, limiting daily activities inevitably led to reducing PM2.5 emissions [14–16]. For NO2, a recent study showed that the restriction of anthropogenic activities during the COVID-19 pandemic led to the decline of concentration, and the northern area in Vietnam observed a higher reduction in NO2 concentration than the south [14, 15, 28]. These results are consistent with our findings.
Air pollution reduction attributed to the constraint of human activities has helped gain health benefits, including a decrease in mortality. If Vietnam had applied stringent measures to control the PM2.5 and NO2 emissions in 2019 to reach 2021 levels, more than 3,000 and 2,000 deaths could have been avoided, respectively. The highest benefits were obtained in northern Vietnam, especially the Red River Delta region. This region is populous, with a population density reaching about 1,000 people/km2 [43]. It also includes Hanoi (the capital city of Vietnam) and other central provinces such as Bac Ninh, Thai Binh, Hung Yen, where anthropogenic activities happen frequently.
Moreover, we also estimated the economic benefit of air pollution reduction corresponding to the mortality decline. The result for Ho Chi Minh city was lower than what was found in other recently published research [22]. Several factors can explain this difference in findings. The first reason might be that while the previous research used air quality guidelines and QCVN 05:2013 as counterfactual level [22], our study measured the change in air pollution due to COVID-19 preventive measures, which only range from 0.47 to 2.29 μg/m3 for PM2.5. Even though this minor change in air pollution contributes to a smaller change in economic benefit, the burden estimated in this study remains significant. Another reason for the difference in results may be the use of different concentration-response functions. The prior research used the pooled effect of many other studies [22], while we used the global exposure mortality model (denoted as GEMM) [2]. Although many other approaches can be used to conduct health impact assessment [1, 33, 44], each calculation has advantages and limitations, therefore it is better to have a consistent measurement throughout the assessment in Vietnam to compare the result. Thus, national health impact assessment guidelines for each disease and each pollutant are essential.
Limitations
Our research had several limitations. First, we assumed that the mortality rate from the Vietnam National Injury Survey had stayed the same since 2010. A study found that the trend of deaths attributed to injury in Vietnam had not been significantly different from 2007 to 2017 [45]. Thus, this approach is acceptable, although it might introduce a certain amount of uncertainty. Second, we did not account for the impact of indoor air pollution because the required data and evidence for such an estimation were not available. We acknowledge that people may have had higher exposures to pollutants at home due to quarantines and physical distancing. It is an important consideration for future studies because indoor air pollution can significantly impact human health [46]. Third, the estimation for Vietnam Value of Statistical Life is still based on a non-updated database (from 2011) and OECD-standard price, so it might not reflect the actual economic benefits when controlling the air quality in Vietnam. However, our findings suggest further studies to construct a more fitting VSL within regions sharing greater similarities with Vietnam.
Conclusion
The implementation of COVID-19 transmission control measures such as lockdowns and social restrictions in Vietnam in 2021 led to a reduction in PM2.5 and NO2 concentration levels, particularly in provinces located in the Red River Delta region. This reduction suggests that if similar air quality levels were maintained in 2019, mortality could have been avoided, with potential economic benefits of $793.0 million (95% CI: 592.7–985.4) and $510.6 million (95% CI: 381.3–634.9) attributable to PM2.5 and NO2 concentration reductions, respectively. To better estimate health and economic benefits, there is a need for stronger public policies aimed at controlling air quality in Vietnam, as well as increased investment in automatic monitoring stations and health data collection, when calculations heavily relied on the precision of pollutant concentrations and mortality rates. Additionally, a reassessment of the Vietnam Value of Statistical Life using more recent parameters would enhance its precision.
Ethics Statement
The studies involving humans were approved by The Ethics Committee of Hanoi University of Public Health under Decision No. 318/2020/YTCC-HD3 dated 30 July 2020. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author Contributions
LTH and NTTN conceived the research idea and designed the study. PTTT, NTNT, NXT, VTD, and VVDN collected the data. LTH and VTD conducted the statistical analysis and interpreted the results. LTH drafted the manuscript and performed critical revisions. NTTN and SS provided guidance throughout the research process and contributed to the final manuscript. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by the Vietnam National Foundation for Science and Technology Development (NAFOSTED) under grant number 105.08-2019.331.
Conflict of Interest
The authors declare that they do not have any conflicts of interest.
Acknowledgments
This report used the outcome from the project the “Improving air pollution monitoring and management of Vietnam with satellite PM2.5 observation.” sponsored by the U.S. Agency for International Development (USAID) through the LASER (Longterm Assistance and SErvices for Research) PULSE (Partners for University-Led Solutions Engine). We sincerely acknowledge the invaluable support of Ms. Divya Gudur, Middlebury College, United States in enhancing the clarity and coherence of this manuscript.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.ssph-journal.org/articles/10.3389/ijph.2023.1606238/full#supplementary-material
References
1. Cardaba Arranz, M, Munoz Moreno, MF, Armentia Medina, A, Alonso Capitan, M, Carreras Vaquer, F, and Almaraz Gomez, A. Health Impact Assessment of Air Pollution in Valladolid, Spain. BMJ open (2014) 4(10):e005999. doi:10.1136/bmjopen-2014-005999
2. Burnett, R, Chen, H, Szyszkowicz, M, Fann, N, Hubbell, B, Pope, CA, et al. Global Estimates of Mortality Associated With Long-Term Exposure to Outdoor Fine Particulate Matter. Proc Natl Acad Sci U S A (2018) 115(38):9592–7. doi:10.1073/pnas.1803222115
3. Nassikas, NJ, Spangler, K, and Wellenius, GA. Asthma Exacerbations Attributable to Ozone Air Pollution in New England. R Med J (2013) (2021) 104(9):20–3.
4. World Health Organization. Exposure & Health Impacts of Air Pollution 2022 (2022). Available from: https://www.who.int/teams/environment-climate-change-and-health/air-quality-and-health/health-impacts/exposure-air-pollution (Accessed January 18, 2023).
5. Institute for Health Metrics and Evaluation (IHME). Health Data for Vietnam (2019). Available from: https://www.healthdata.org/vietnam (Accessed January 18, 2023).
6. World Health Organization. Air Pollution (2023). Available from: https://www.who.int/vietnam/health-topics/air-pollution (Accessed January 18, 2023).
7. Saleh, S, Shepherd, W, Jewell, C, Lam, NL, Balmes, J, Bates, MN, et al. Air Pollution Interventions and Respiratory Health: A Systematic Review. Int J tuberculosis Lung Dis (2020) 24(2):150–64. doi:10.5588/ijtld.19.0417
8. Rich, DQ, Liu, K, Zhang, J, Thurston, SW, Stevens, TP, Pan, Y, et al. Differences in Birth Weight Associated With the 2008 Beijing Olympics Air Pollution Reduction: Results From a Natural Experiment. Environ Health Perspect (2015) 123(9):880–7. doi:10.1289/ehp.1408795
9. Ransom, MR, and Arden Pope, C. External Health Costs of A Steel Mill. Contemp Econ Pol (1995) 13(2):86–97. doi:10.1111/j.1465-7287.1995.tb00745.x
10. Friedman, MS, Powell, KE, Hutwagner, L, Graham, LM, and Teague, WG. Impact of Changes in Transportation and Commuting Behaviors During the 1996 Summer Olympic Games in Atlanta on Air Quality and Childhood Asthma. Jama (2001) 285(7):897–905. doi:10.1001/jama.285.7.897
11. Heinrich, J, Hoelscher, B, Frye, C, Meyer, I, Pitz, M, Cyrys, J, et al. Improved Air Quality in Reunified Germany and Decreases in Respiratory Symptoms. Epidemiology (Cambridge, Mass) (2002) 13(4):394–401. doi:10.1097/00001648-200207000-00006
12. Tanzer-Gruener, R, Li, J, Eilenberg, SR, Robinson, AL, and Presto, AA. Impacts of Modifiable Factors on Ambient Air Pollution: A Case Study of COVID-19 Shutdowns. Environ Sci Technol Lett (2020) 7(8):554–9. doi:10.1021/acs.estlett.0c00365
13. Vo, HL, Nguyen, HAS, Nguyen, KN, Nguyen, HLT, Nguyen, HT, Nguyen, LH, et al. Adherence to Social Distancing Measures for Controlling COVID-19 Pandemic: Successful Lesson From Vietnam. Front Public Health (2020) 8:589900. doi:10.3389/fpubh.2020.589900
14. Dang, HA, and Trinh, TA. The Beneficial Impacts of COVID-19 Lockdowns on Air Pollution: Evidence From Vietnam. J Develop Stud (2022) 58(10):1917–33. doi:10.1080/00220388.2022.2069492
15. Nguyen, TPM, Bui, TH, Nguyen, MK, Nguyen, TH, Vu, VT, and Pham, HL. Impact of Covid-19 Partial Lockdown on PM(2.5), SO(2), NO(2), O(3), and Trace Elements in PM(2.5) in Hanoi, Vietnam. Environ Sci Pollut Res Int (2022) 29(28):41875–85. doi:10.1007/s11356-021-13792-y
16. Venter, ZS, Aunan, K, Chowdhury, S, and Lelieveld, J. COVID-19 Lockdowns Cause Global Air Pollution Declines. Proc Natl Acad Sci U S A (2020) 117(32):18984–90. doi:10.1073/pnas.2006853117
17. Venter, ZS, Aunan, K, Chowdhury, S, and Lelieveld, J. Air Pollution Declines During COVID-19 Lockdowns Mitigate the Global Health Burden. Environ Res (2021) 192:110403. doi:10.1016/j.envres.2020.110403
18. Ye, T, Guo, S, Xie, Y, Chen, Z, Abramson, MJ, Heyworth, J, et al. Health and Related Economic Benefits Associated With Reduction in Air Pollution During COVID-19 Outbreak in 367 Cities in China. Ecotoxicol Environ Saf (2021) 222:112481. doi:10.1016/j.ecoenv.2021.112481
19. Vu, HNK, Ha, QP, Nguyen, DH, Nguyen, TTT, Nguyen, TT, Nguyen, TTH, et al. Poor Air Quality and Its Association With Mortality in Ho Chi Minh City: Case Study. Atmosphere (2020) 11(7):750. doi:10.3390/atmos11070750
20. Nhung, NTT, Jegasothy, E, Ngan, NTK, Truong, NX, Thanh, NTN, Marks, GB, et al. Mortality Burden Due to Exposure to Outdoor Fine Particulate Matter in Hanoi, Vietnam: Health Impact Assessment. Int J Public Health (2022) 67:1604331. doi:10.3389/ijph.2022.1604331
21. Nhung, NTT, Duc, VT, Ngoc, VD, Dien, TM, Hoang, LT, Ha, TTT, et al. Mortality Benefits of Reduction Fine Particulate Matter in Vietnam, 2019. Front Public Health (2022) 10:4529. doi:10.3389/fpubh.2022.1056370
22. Ho, HT, Dang, VC, Pham, TBT, and Wangwongwatana, S. Assessment of Health and Economic Benefits of Reducing Fine Particulate Matter (PM2. 5) Concentration in Ho Chi Minh City, Vietnam. Hyg Environ Health Adv (2023) 6:100045. doi:10.1016/j.heha.2023.100045
23. Kloog, I, Chudnovsky, AA, Just, AC, Nordio, F, Koutrakis, P, Coull, BA, et al. A New Hybrid Spatio-Temporal Model for Estimating Daily Multi-Year PM2.5 Concentrations Across Northeastern USA Using High Resolution Aerosol Optical Depth Data. Atmos Environ (2014) 95:581–90. doi:10.1016/j.atmosenv.2014.07.014
24. Copernicus Climate Change Service. Climate Data Store (2022). Available from: https://cds.climate.copernicus.eu/ (Accessed March 25, 2023).
25. MODIS. Moderate Resolution Imaging Spectroradiometer (MODIS) - LAADS DAAC (2022). Available from: https://ladsweb.modaps.eosdis.nasa.gov/missions-and-measurements/modis/ (Accessed March 25, 2023).
26. Jet Propulsion Laboratory - NASA, California Institute of Technology. Advanced Spaceborne Thermal Emission and Reflection Radiometer (ASTER) (2019). Available from: https://asterweb.jpl.nasa.gov/gdem.asp (Accessed March 25, 2023).
27. Ngo, TX, Pham, HV, Phan, HDT, Nguyen, ATN, To, HT, and Nguyen, TTN. A Daily and Complete PM(2.5) Dataset Derived From Space Observations for Vietnam From 2012 to 2020. Sci Total Environ (2023) 857(3):159537. doi:10.1016/j.scitotenv.2022.159537
28. Ngo, TX, Do, NTN, Phan, HDT, Tran, VT, Mac, TTM, Le, AH, et al. Air Pollution in Vietnam During the COVID-19 Social Isolation, Evidence of Reduction in Human Activities. Int J Remote Sensing (2021) 42(16):6126–52. doi:10.1080/01431161.2021.1934911
29. General Statistics Office. Completed Results of the 2019 Viet Nam Population and Housing Census. Statistical Publish House (2019). Available from: https://www.gso.gov.vn/en/data-and-statistics/2020/11/completed-results-of-the-2019-viet-nam-population-and-housing-census/ (Accessed March 25, 2023).
30. General Statistics Office. Crude Birth Rate, Crude Death Rate and Natural Increase Rate by Province (2019). Available from: https://www.gso.gov.vn/en/px-web/?pxid=E0212-14&theme=Population%20and%20Employment (Accessed March 25, 2023).
31. Center for Injury Policy and Prevention Research. Vietnam National Injury Survey 2010. Hanoi: Hanoi School of Public Health (2012).
32. Ostro, B, World Health Organization. Outdoor Air Pollution: Assessing the Environmental burden of Disease at National and Local Levels. World Health Organization (2004).
33. Bayat, R, Ashrafi, K, Shafiepour Motlagh, M, Hassanvand, MS, Daroudi, R, Fink, G, et al. Health Impact and Related Cost of Ambient Air Pollution in Tehran. Environ Res (2019) 176:108547. doi:10.1016/j.envres.2019.108547
34. Zhu, B, Pang, R, Chevallier, J, Wei, YM, and Vo, DT. Including Intangible Costs Into the Cost-of-Illness Approach: A Method Refinement Illustrated Based on the PM(2.5) Economic burden in China. Eur J Health Econ (2019) 20(4):501–11. doi:10.1007/s10198-018-1012-0
35. United States Environmental Protection Agency Office of Policy, Resource Management Office of Policy Analysis. Guidelines for Performing Regulatory Impact Analysis. Washington, D.C.: US Environmental Protection Agency (1983).
36. Safari, Z, Fouladi-Fard, R, Vahedian, M, Mahmoudian, MH, Rahbar, A, and Fiore, M. Health Impact Assessment and Evaluation of Economic Costs Attributed to PM(2.5) Air Pollution Using BenMAP-CE. Int J biometeorology (2022) 66(9):1891–902. doi:10.1007/s00484-022-02330-1
37. World Bank. The Cost of Air Pollution: Strengthening the Economic Case for Action (2016). Available from: https://openknowledge.worldbank.org/handle/10986/25013 (Accessed March 27, 2023).
38. World Bank. GDP Per Capita (Current US$) (2019). Available from: https://data.worldbank.org/indicator/NY.GDP.PCAP.CD (Accessed March 27, 2023).
39. United States Environmental Protection Agency (US-EPA). Benefits Mapping and Analysis Program (BenMAP) (2023). Available from: https://www.epa.gov/benmap/benmap-downloads (Accessed March 27, 2023).
40. Nguyen, TNT. Current Status of PM2. 5 Pollution and Its Mitigation in Vietnam. Glob Environ Res (2018) 22.
41. University of Engineering and Technology - Vietnam National University - in Hanoi (VNU-UET), Live&Learn, United States Agency for International Development (USAID). State of PM2.5 in Vietnam During 2019-2020 Based on Multi-Source Data (2021). Available from: https://khisachtroixanh.com/tai-lieu/nghien-cuu-hien-trang-bui-pm2-5-o-viet-nam-giai-doan-2019-2020-su-dung-du-lieu-da-nguon/ (Accessed February 7, 2023).
42. Foo, C, Verma, M, Tan, SM, Haldane, V, Reyes, KA, Garcia, F, et al. COVID-19 Public Health and Social Measures: A Comprehensive Picture of Six Asian Countries. BMJ Glob Health (2022) 7(11):e009863. doi:10.1136/bmjgh-2022-009863
43. Vietnam General Statistics Office. Area, Population and Population Density by Provinces and Cities in Vietnam (2022). Available from: https://www.gso.gov.vn/en/statistical-data/ (Accessed March 25, 2023).
44. Boldo, E, Linares, C, Lumbreras, J, Borge, R, Narros, A, Garcia-Perez, J, et al. Health Impact Assessment of a Reduction in Ambient PM(2.5) Levels in Spain. Environ Int (2011) 37(2):342–8. doi:10.1016/j.envint.2010.10.004
45. Nguyen, QA, Nguyen, TH, Beardsley, J, Castle, CD, Dang, AK, Dingels, ZV, et al. Burden of Injuries in Vietnam: Emerging Trends From a Decade of Economic Achievement. Inj Prev (2020) 26(1):i75–i82. doi:10.1136/injuryprev-2019-043352
Keywords: health impact assessment, economic benefits, air pollution, air quality, Vietnam
Citation: Hoang LT, Duc VT, Ngoc VVD, Truong NX, Thanh NTN, Trang PTT, Saksena S and Nhung NTT (2023) Health and Economic Benefits of Air Pollution Reductions in Vietnam During 2020–2021. Int J Public Health 68:1606238. doi: 10.3389/ijph.2023.1606238
Received: 23 May 2023; Accepted: 21 September 2023;
Published: 10 October 2023.
Edited by:
Martin Röösli, Swiss Tropical and Public Health Institute (Swiss TPH), SwitzerlandCopyright © 2023 Hoang, Duc, Ngoc, Truong, Thanh, Trang, Saksena and Nhung. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Le Tu Hoang, bHRoMkBodXBoLmVkdS52bg==