 Stéphane Cullati1,2,3*
Stéphane Cullati1,2,3* Norbert K. Semmer4,5,6Franziska Tschan5,7Gaëlle Choupay1,2Pierre Chopard1,2Delphine S. Courvoisier1,2
Norbert K. Semmer4,5,6Franziska Tschan5,7Gaëlle Choupay1,2Pierre Chopard1,2Delphine S. Courvoisier1,2- 1Quality of Care Service, University Hospitals of Geneva, Geneva, Switzerland
- 2Faculty of Medicine, University of Geneva, Geneva, Switzerland
- 3Population Health Laboratory (#PopHealthLab), University of Fribourg, Fribourg, Switzerland
- 4Department of Psychology, University of Bern, Bern, Switzerland
- 5National Center for Competence in Research on Affective Sciences, Geneva, Switzerland
- 6Biological Work and Health Psychology, University of Konstanz, Konstanz, Germany
- 7Institute for Work and Organizational Psychology, University of Neuchâtel, Neuchâtel, Switzerland
Objectives: The current study investigates the prevalence of illegitimate tasks in a hospital setting and their association with patient safety culture outcomes, which has not been previously investigated.
Methods: We conducted a cross-sectional survey in a tertiary referral hospital. Patient safety culture outcomes were measured using the Hospital Survey on Patient Safety Culture questionnaire; the primary outcome measures were a low safety rating for the respondent’s unit and whether the respondent had completed one or more safety event reports in the last 12 months. Analyses were adjusted for hospital department and staff member characteristics relating to work and health.
Results: A total of 2,276 respondents answered the survey (participation rate: 35.0%). Overall, 26.2% of respondents perceived illegitimate tasks to occur frequently, 8.1% reported a low level of safety in their unit, and 60.3% reported having completed one or more safety event reports. In multivariable analyses, perception of a higher frequency of illegitimate tasks was associated with a higher risk of reporting a low safety rating and with a higher chance of having completed event reports.
Conclusion: The prevalence of perceived illegitimate tasks was rather high. A programme aiming to reduce illegitimate tasks could provide support for a causal effect of these tasks on safety culture outcomes.
Introduction
Illegitimate tasks are defined as tasks that people think they cannot properly be expected to carry out, either because the tasks should not exist or are not needed (unnecessary tasks), or because they are not part of their specific role as employees (unreasonable tasks) [1–3]. Such tasks do not represent meaningful contributions to the fulfilment of one’s occupational role and often detract from the core tasks that define that role [3]. The problem of illegitimate tasks is widespread in the world of work, and is observable in companies in most sectors of the economy [2, 3], including healthcare [4–6]. In hospital settings, the complexity of patient care suggests that acute care hospitals may be an environment at risk for illegitimate tasks. For example, nurses use the special term “non-nursing activities” [7, 8], and many physicians complain about non-medical tasks [5, 9, 10]. However, evidence on the prevalence of illegitimate tasks in hospital settings remains scarce. Furthermore, although illegitimate tasks have been linked to health and well-being, to the best of our knowledge no study has yet investigated their association with patient safety culture.
Risks factors for poor patient safety culture have been examined in multiple healthcare settings; the findings of this research have pointed to the importance of healthcare professionals’ characteristics, including their number of years of experience in the hospital [11] or the unit [12], their type of profession [12–18], their level of seniority in their profession [18], the number of hours worked per week [17], and sociodemographic factors [16, 19, 20]. Moreover, there is a body of literature reporting on variability in patient safety culture as related to numerous hospital characteristics, including certification [21], accreditation [11], medical departments [22], hospital size [11, 17] and type [17], and level of staffing in the units [23]. However, the way in which work and tasks are distributed and organised within units or wards has not been studied in relation to patient safety culture. Poor organisation of work and tasks is a stressor for identification with one’s professional role [24] and with the organization [25] and can hamper staff performance [25–27], for instance by rendering their use of time inefficient [28, 29]. In a healthcare setting, we can assume that tasks perceived as “illegitimate” could decrease work satisfaction among staff [4, 30], demotivate staff [5], reduce satisfaction with performance [31], and reflect a lack of good management in the unit [25]. In non-healthcare settings, perception of illegitimate tasks has been found to be associated with more counterproductive work behaviour [32, 33] and with lower self-esteem [33, 34], work engagement [5], job identity [35], and supervisor-rated task performance [35]. However, at present, we do not know whether perception of illegitimate tasks among hospital staff is associated with safety culture.
The objectives of this study were (1) to describe the prevalence of illegitimate tasks among healthcare staff in a tertiary referral hospital, and (2) to assess the association between perception of illegitimate tasks and patient safety culture.
Methods
Design
We conducted a cross-sectional survey using a self-administered questionnaire. Specifically, the current study used data from a census of healthcare professionals in a single hospital, the primary aim of which was to monitor the safety culture of the hospital through repeated cross-sectional surveys.
Population and Sample
The survey was conducted at the Geneva University Hospitals, Switzerland, in November/December of 2016. The Geneva University Hospitals form a 1700-bed tertiary referral hospital for the State of Geneva, an international metropolitan area of almost one million inhabitants. The inclusion criteria for the survey were (1) being a healthcare professional and (2) working with patients, either “directly” (having direct contact, at the patient bedside), or “indirectly” (work related to patient clinical care, such as laboratory, pathology, radiology, and pharmacy work).
Procedure
The survey was first advertised on the hospital intranet and through posters in various departments and wards. All healthcare professionals at the hospital were then contacted by email with a request to complete the online survey. Email addresses were obtained from the human resources department. Three reminders were sent, 7 days apart.
Ethical Considerations
The survey was exempted from ethical review by the Cantonal Ethics Commission of Geneva (reference number: req-2023-00049). The confidentiality and protection of data was guaranteed in accordance with the Swiss Federal Data Protection Act.
Dependent Variables
Safety culture was measured via two variables of the French version [36] of the Hospital Survey on Patient Safety Culture (HSOPSC) questionnaire version 1 [37]: 1) the patient safety grade in the unit/service of the respondent (hereafter, “safety rating”) and 2) whether the respondent had completed one or more safety event reports in the last 12 months. The French version of the HSOPSC questionnaire version 1 consists of 43 items measuring 12 safety culture processes (each process consisting of 3–4 items) and 2 safety culture outcomes (each outcome measured with a single item). Only the safety culture outcome items were used in this study. We hypothesised that these two outcome indicators from the HSOPSC questionnaire could serve as proxies for patient safety culture. The item assessing safety rating was “Please give your work area/unit in this hospital an overall grade on patient safety,” with the following answer options: “failing,” “poor,” “acceptable,” “very good,” and “excellent.” Safety ratings were recoded as “low” (failing and poor) or “adequate” (acceptable, very good, and excellent). The item assessing the number of safety events reports was “In the past 12 months, how many patient safety events reports have you reported?”, with the answer options “no safety event reports,” “1 to 2,” “3 to 5,” “6 to 10,” “11 to 20,” and “21 or more”; responses were recoded as “no event report” or “at least 1 event report.”
Main Independent Variable
Perception of illegitimate tasks was measured using the French version of the Bern Illegitimate Tasks Scale (BITS; full scale reported in Supplementary Table S1) [38]. This consists of two facets: unnecessary tasks (4 items, Cronbach’s alpha = 0.85 in the analytical sample; sample item: “Do you have work tasks to take care of, which keep you wondering if they make sense at all?”) and unreasonable tasks (4 items, Cronbach’s alpha = 0.83; sample item: “Do you have work tasks to take care of, which you believe should be done by someone else?”). The two subscales reflect different aspects of illegitimacy; they may therefore be analysed separately, but the common denominator of illegitimacy is well reflected in the total scale [38], which had a Cronbach’s alpha of 0.87. Principal component analysis confirmed the unidimensionality of each dimension. To obtain a measure of the frequency of self-perceived illegitimate tasks for the description of prevalence (objective 1), we carried out the following calculations. First, we dichotomised responses to each item as either 0 (= “never, very rarely”, “quite rarely”, and “sometimes”) or 1 (= “quite often” and “very often”). Subsequently, we computed the mean value of the dichotomised responses to items, both for the entire scale and for each facet (unnecessary and unreasonable tasks). Finally, we dichotomised each continuous variable into two groups: 0–0.49 (coded as 0) and 0.50–1.00 (coded as 1), where the prevalence of illegitimate tasks was equal to either 1 (meaning that respondents answered half or more of the items with the response “quite often” or “very often”) or 0 (meaning that respondents answered less than half of the items response with the response “quite often” or “very often”; in other words, the majority of respondents gave answers such as “never, very rarely,” “quite rarely,” or “sometimes”). This measure is new and is not based on previous validation studies; we interpreted it as representing the prevalence of the perception among participants that illegitimate tasks were frequent. In the analyses related to objective 2, we treated these three variables relating to illegitimate tasks as continuous variables, using the mean scores obtained on the relevant items, ranging from 1 (“never, very rarely”) to 5 (“very often”).
Control Variables
Healthcare professionals were asked to provide the following information: duration of their work experience in the unit/service (0–10 years vs. 11 years or more), their clinical department, and their degree of satisfaction with their work. These three factors are associated with safety culture [22, 39]. Work experience was assessed with a single question: “How long have you worked in your unit or department or sector?” The response options were “less than 1 year,” “1–5 years,” “6–10 years,” “11–15 years,” “16–20 years,” and “21 years or more,” and responses were recoded as “0–10 years” or “11 years or more.” Satisfaction with work was measured with the question “How satisfied are you with your work in general?”, and response options ranged from 1 (extremely unsatisfied) to 7 (extremely satisfied) [40]. In addition, we asked healthcare professionals about their health status; this section consisted of one item assessing their feelings of burnout or emotional exhaustion[41], one assessing their self-rated general health, and one assessing their self-esteem. The emotional exhaustion item read: “I feel burned out from my work,” with the response options “never,” “a few times a year or less,” “once a month or less,” “a few times a month,” “once a week,” and “a few times a week/every day” [42]. Self-rated general health was assessed using one question (with response options “poor,” “fair,” “good,” “very good,” “excellent”) [43], and responses were recoded to improve the continuous properties of the data [44]. This self-rated health item is a frequently used item in health research as an umbrella indicator of health, capturing the main dimension of health [45]. Finally, self-esteem was a measured using the item “I have high self-esteem” [46], with responses given on a 5-point scale ranging from 1 (“not at all”) to 5 (“absolutely”). Furthermore, we controlled for several additional self-reported characteristics: number of hours worked per week (less than 10 h, 10–29 h, 30–49 h, 50–69 h, or more than 69 h); profession (nurse, nursing auxiliary, doctor, multidisciplinary health professional, medical technician, or other profession); professional status in terms of management function (none, middle management, or top management); and whether the respondent had direct contact with patients or not.
Statistical Analyses
Mean values for the illegitimate tasks scale (and subscales) are reported with 95% confidence intervals (95% CIs). To estimate the prevalence of illegitimate tasks, we computed the proportion of healthcare professionals who answered half or more of the questions on the Bern Illegitimate Tasks Scale with “quite often” or “very often.” The prevalence by several sociodemographic and professional control variables, such as years of experience, was also computed, and the associations between these variables and prevalence of illegitimate tasks was estimated using the chi-square test for nominal variables (e.g., department) and a test for trend for continuous variables. To assess the association between perception of illegitimate tasks (continuous) and the two dichotomised variables relating to patient safety culture outcomes (safety rating in the unit/service, and having completed one or more safety event reports in the last 12 months), we used logistic regression models, adjusting for hospital department, work-related factors (experience, hours worked, profession, managerial responsibilities, satisfaction with work), health-related factors (emotional exhaustion, self-rated health), and self-esteem. Missing data on covariates were rare (<4%) and were imputed using multiple imputation with chained equations (50 samples, predictive mean matching algorithm). Health status and self-esteem factors have previously been found to be associated with patient safety culture [19, 47] and to be predicted by the presence of illegitimate tasks [1, 4, 5, 33, 48].
We ran three robustness analyses (RAs): first, treating both exposure and outcomes as dichotomous variables (RA1); second, treating both exposure and outcomes as continuous variables (RA2); and third, treating exposure as dichotomous and outcomes as continuous variables (RA3).
Results
Of 8,332 healthcare professionals (hereafter, “professionals”) who were invited to participate, 2,917 completed the survey (35.0% participation rate). After removal of participants with missing data on the outcomes (n = 302) or the main independent variable (illegitimate tasks) (n = 431), data from 2,478 respondents remained for analysis. Among the 2,478 respondents, data on control variables were sporadically missing, from missing emotional exhaustion scores for 0.5% of respondents to missing information on department for 3.9% of respondents.
Professionals’ characteristics are reported in Table 1 and Figure 1. The professionals were mostly nurses (58.0%) and had significant amounts of professional experience, with almost two in three (65.2%) reporting 11 years or more of experience in their profession. More than three in four (77.3%) had no managerial responsibilities. Professionals reported good satisfaction with their work (mean 4.45, standard deviation (SD) 1.39, min 1, max 7) and good self-rated health (mean 4.05, SD 0.72, min 1, max 5). The average self-esteem score was 3.52 (SD 0.87, min 1, max 5). The mean level of emotional exhaustion was 3.09 (SD 1.33, min 1, max 6), and 35.6% of professionals reported feeling emotionally exhausted “every day” or “a few times a month.”
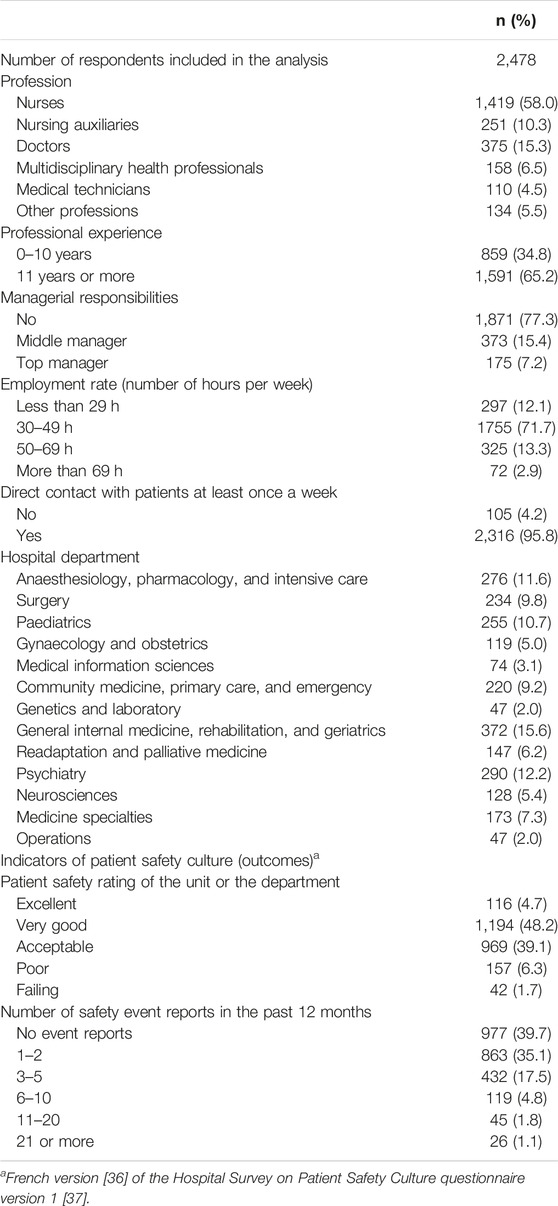
TABLE 1. Characteristics of a sample of healthcare professionals at Geneva University Hospitals (Switzerland, 2016).
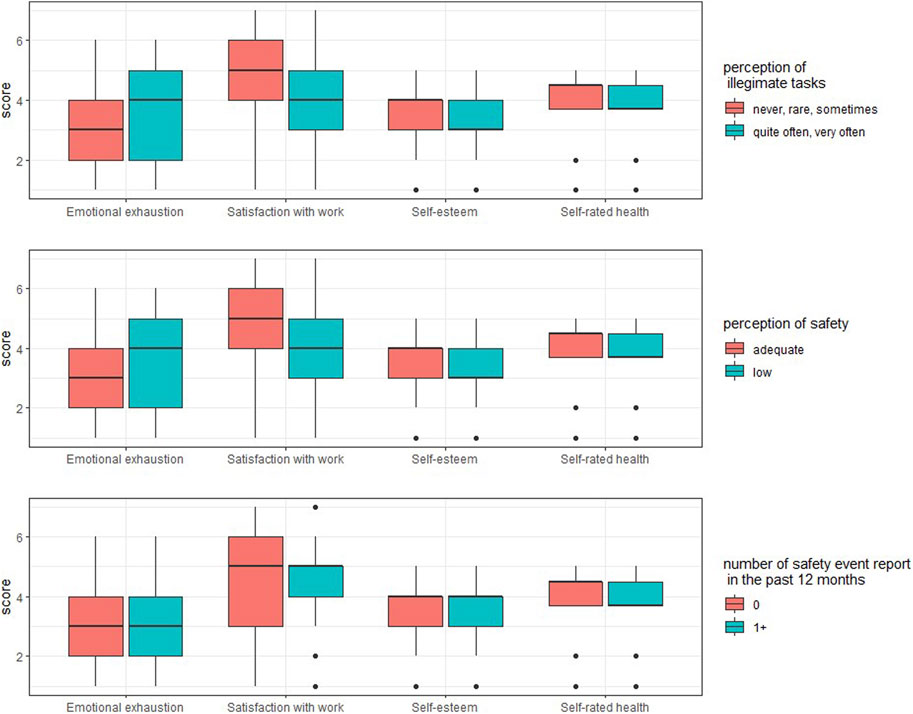
FIGURE 1. Box plot of emotional exhaustion, satisfaction with work, self-rated health and self-esteem among healthcare professionals at Geneva University Hospitals (Switzerland, 2016).
Comparing the proportions of professional categories in our sample with the proportions across the whole hospital (based on the hospital’s 2016 activity reports), two groups were over-represented in our sample: nurses (58% in our sample versus 45% across the whole hospital) and multidisciplinary health professionals (7% versus 4%). For doctors, the proportion in our sample was similar to that across the hospital (15% versus 16%).
Prevalence of Illegitimate Tasks
The response frequencies for each item of the illegitimate tasks scale (BITS) are reported in the Supplementary Table S1. Overall, 19.7% of professionals perceived illegitimate tasks to occur frequently (defined as selecting “quite often” or “very often” for half or more of their responses; hereafter, “frequent” illegitimate tasks), and 31.0% and 15.5% perceived unnecessary and unreasonable tasks, respectively, to occur frequently. The mean score on the illegitimate tasks scale was 2.62 (95% CI 2.59–2.64). The mean scores for each dimension and by profession are reported in the Supplementary Table S2.
The prevalence of frequent illegitimate tasks varied by profession, professional experience, managerial responsibilities, employment rate, direct patient contact, and hospital department (Table 2, first column) and by respondents’ levels of emotional exhaustion (p < 0.001), satisfaction with work (p < 0.001), self-esteem (p = 0.002), and self-rated health (p < 0.001) (Figure 2); the same patterns of variation were observed for unnecessary and unreasonable tasks (Supplementary Table S3; Supplementary Figure S1). Doctors and medical technicians, top managers, professionals with less experience (0–10 years), those working more hours per week, and those having direct contact with patients perceived illegitimate tasks, unnecessary tasks, and unreasonable tasks to occur more frequently. The perception that illegitimate tasks, unnecessary tasks, and unreasonable tasks occurred frequently was associated with greater dissatisfaction with work, lower self-esteem, poor self-rated health, and more emotional exhaustion.
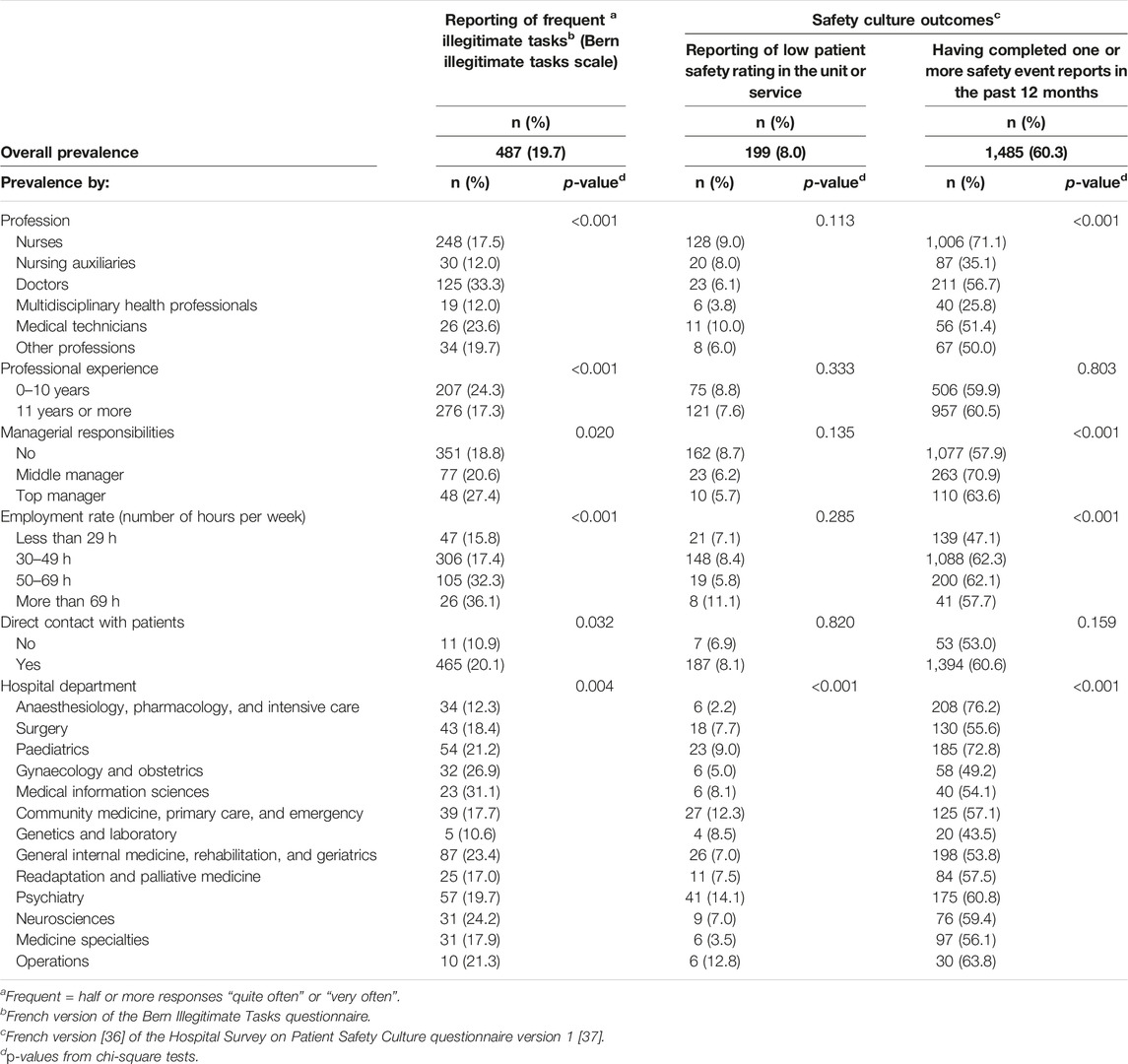
TABLE 2. Prevalence of perceived illegitimate tasks at work and of safety culture outcomes (low patient safety rating; completion of safety event reports), overall and by professional characteristics (Switzerland, 2016).
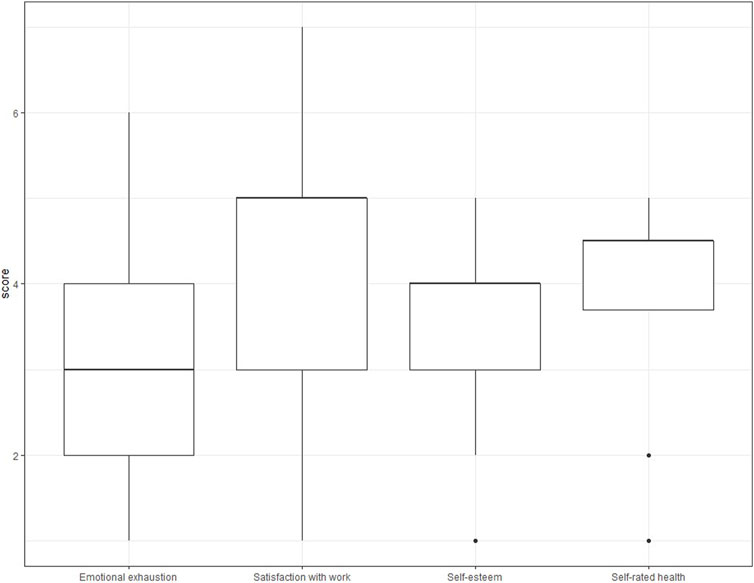
FIGURE 2. Box plots of emotional exhaustion, satisfaction with work, self-esteem, and self-rated health, by prevalence of frequent (quite/very often) illegitimate tasks (French version of the Bern illegitimate tasks questionnaire), low patient safety in the unit or service and having completed one or more safety event reports (French version of the Hospital Survey on Patient Safety Culture questionnaire version 1), (Switzerland, 2016).
Prevalence of Safety Culture Outcomes
The proportion of professionals who reported a low safety rating (poor or failing) in their unit/service was 8.0% (Table 1). No differences in this proportion by profession, professional experience, managerial status, employment rate, or patient contact were observed, but a difference between hospital departments was observed (Table 2, second column). Professionals reported lower safety ratings when they were more dissatisfied with their work, had lower self-esteem, reported poor self-rated health, and were more often emotionally exhausted (ps < 0.001; Figure 2).
The proportion of professionals who reported having completed one or more event reports in the past 12 months was 60.3% (Table 1). Nurses, managers (top or middle), and professionals working more hours per week were more likely to have completed one or more event reports (Table 2, third column), as were those with fair self-rated health (p = 0.003) and those who were more often emotionally exhausted (p = 0.001); no differences according to level of work satisfaction (p = 0.802) or self-esteem (p = 0.083) were observed (Figure 2).
Association Between Self-Reported Illegitimate Tasks and Safety Culture Outcomes
Higher perceived frequency of illegitimate tasks was associated with higher odds of a low safety rating in the unit/service (odds ratio (OR): 2.72, 95% CI 2.25–3.29; Table 3). In adjusted multivariable models, this association was attenuated, but remained significant (OR: 2.30, 95% CI 1.86–2.87). In analyses of the sub-dimensions of illegitimate tasks, higher perceived frequency of both unnecessary and unreasonable tasks was associated with higher odds of a low safety rating, in both unadjusted and adjusted models.
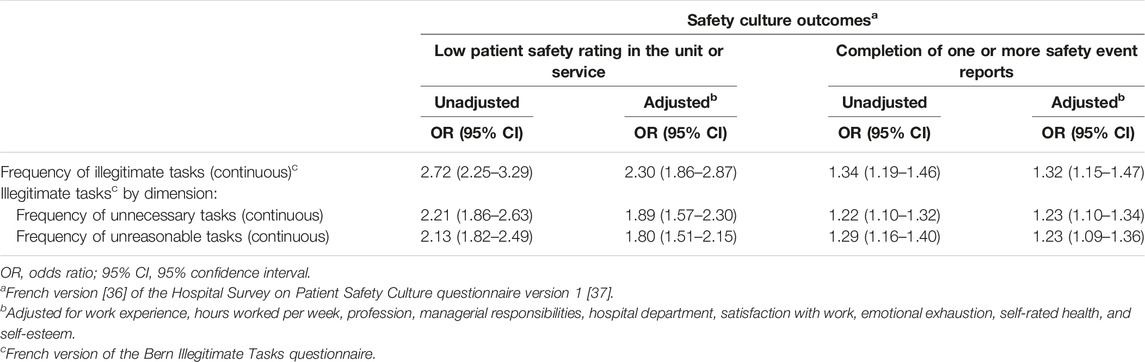
TABLE 3. Associations between perception of the frequency illegitimate tasks and two safety culture outcomes (Switzerland, 2016).
Higher perceived frequency of illegitimate tasks was also associated with 34% higher odds of having completed one or more event reports in the past 12 months (OR: 1.34, 95% CI 1.19–1.46). In adjusted multivariable models, this association was slightly attenuated, but remained significant (OR: 1.32, 95% CI 1.15–1.47). In analyses of the sub-dimensions of illegitimate tasks, higher perceived frequency of both unnecessary and unreasonable tasks was associated with higher odds of having completed event reports, in both unadjusted and adjusted models.
Robustness Analyses
We checked the robustness of the main analysis by testing different coding schemes for the exposure and outcome variables (Supplementary Table S4). First (RA1), we treated the illegitimate tasks variable (and the sub-dimensions of this scale) as a dichotomous variable. For the safety grade outcome, the results were similar to those obtained in the main analysis. For the completed safety event reports outcome, the results were similar for illegitimate tasks overall, but the association with the perception that unreasonable tasks occurred frequently became non-significant in the adjusted model (OR: 1.30, 95% CI 0.99–1.63). Second (RA2), we treated both the outcome and the exposure variables as continuous variables. All results were similar to those obtained in the main analysis. Of note, higher perceived frequency of unreasonable tasks was marginally associated with having completed safety event reports in the adjusted model (b = 0.08, 95% CI 0.03–0.12). Third (RA3), we treated the outcome variables as continuous variables and the exposure variables as dichotomous variables. For safety grade, the results were similar to those obtained in the main analysis. For completion of safety event reports, the results were similar for illegitimate tasks overall, but higher perceived frequency of unreasonable tasks was only marginally associated with this outcome in the adjusted model (b = 0.12, 95% CI 0.04–0.27).
Discussion
Illegitimate Tasks
The mean score for perceived frequency of illegitimate tasks—the tasks that people feel they should not have to do—was 2.62 (95% CI 2.59–2.65) as rated on the BITS scale, with response options ranging from 1 to 5, among our sample of healthcare professionals working in a tertiary referral hospital. Despite the rather low rate of participation in our survey (35%), this result was similar to that of a study by [6], who reported a mean score of 2.66 for the perceived frequency of unreasonable tasks among physicians working in a Norwegian hospital (participation rate: 72%); the corresponding score in our subgroup of physicians was 2.59 (95% CI 2.48–2.67). It is worth noting, although the sample is not directly comparable with ours, that [4] reported a mean value of 3.06 for the perceived frequency of illegitimate tasks among general practitioners in Germany, in a study with an approximate participation rate of 6%. In studies carried out in Switzerland but with non-health professions, the mean values reported range between 1.46 [34] and 2.64 [49]. Thus, with regard to mean values on the BITS scale, the perceived frequency of illegitimate tasks remains within a range comparable to that reported among non-health professions.
In terms of prevalence, almost 20% of the participants perceived illegitimate tasks as occurring frequently (according to our coding scheme for the BITS scale, i.e., the mean of dichotomised items). It is worth noting that illegitimate tasks were perceived as occurring frequently by one-third of physicians, who thus reported the highest prevalence of frequent occurrence of illegitimate tasks among all hospital occupations (as well as on both dimensions of the illegitimate tasks scale). One hypothesis may explain this finding: with the development of healthcare management for quality improvement, all healthcare professionals are required to document their activities more regularly (reporting, indicators) and to adapt their activities to quality-oriented patient care protocols (clinical pathways). We know that doctors suffer from the burden of tasks that are perceived as “administrative” [50, 51]. In addition, with the development of evidence-based medicine, healthcare professionals need to adapt their patient care protocols to new recommendations for good clinical practice. All health professionals are affected by these developments, but it may be that doctors are more reluctant than other professionals to accommodate them, because these developments affect all professions in more or less the same way, which may be at odds with the social position of doctors in a hospital (where they are at the top of the social hierarchy) [52]. This reluctance may be reflected in the perception of a higher frequency of illegitimate tasks. After physicians, approximately 4 out of 10 professionals from the “medical technicians” group perceived illegitimate tasks as occurring frequently (24%). Considering the two dimensions of illegitimate tasks, our participants more perceived unnecessary tasks (tasks that should not exist or are not needed) as occurring more frequently than unreasonable tasks (tasks not part of their specific role), at rates of 31% and 16%, respectively; these results correspond to those reported by [5] with regard to physicians, but in the study by Kilponen et al., nurses perceived comparatively higher rates of unreasonable tasks (tasks outside their professional role). Exact comparisons with other studies are difficult, as the coding schemes used are quite different. For instance, [28] conducted a survey among staff members at 11 primary care centres in Sweden (participation rate: 89%) using a different coding scheme with the illegitimate tasks scale (taking the mean of the scale items and then dichotomising the value using a cut-off of 3.5). They reported that 3% of their participants perceived illegitimate tasks to occur at a rate above this score, with an 11% rate for the dimension of unnecessary tasks (primary care physicians 27%, nurses 9%) and 5% for the dimension of unreasonable tasks. Thus, there is no clear picture of prevalence in the healthcare field yet.
In summary: firstly, the occurrence of illegitimate tasks can certainly be regarded as a phenomenon that is non-negligible [5, 9], and doctors are probably the profession that perceive illegitimate tasks as occurring most frequently. Secondly, given that tertiary acute care hospitals provide complex care and accommodate high-needs patients, and given the growth of interdisciplinary care involving a variety of health professionals (nurses, doctors, physiotherapists, nutritionists, etc.) needing to communicate and coordinate effectively to provide the best care to patients [53–56], a high level of occurrence of perceived illegitimate tasks might have been expected in our hospital. However, the results suggested a reasonable and not excessively high level.
Our results also showed that the level of perception of illegitimate tasks is likely to vary between clinical departments in the hospital. We are not aware of any studies comparing illegitimate tasks between clinical departments. Further research to compare the level of occurrence in different clinical settings and to examine whether the risk factors differ between settings would be worthwhile.
Safety Culture Outcomes
Roughly 60% of participants reported having completed at least one safety event report in the last year, and roughly 8% reported low safety ratings (poor or failing) in their unit. These findings suggest that the patient safety culture was relatively good in this hospital. On the one hand, a proportion of six out of ten healthcare professionals reporting having completed safety records reflects a good safety culture. This proportion was based on self-reported data, not actual reports, and may be biased, but was high compared to other hospitals, according to data from systematic reviews and meta-analysis [57, 58]. On the other hand, a rate of almost one in ten health professionals indicating that safety is low (poor or failing) in their unit is not negligible either, and this level was similar to or lower than the rates occurring in other European hospitals [59, 60].
Associations between both indicators of patient safety culture and the occurrence of illegitimate tasks emerged, as expected. A higher frequency of illegitimate tasks was associated with a higher risk of low reported patient safety ratings and a higher chance of completing at least one safety event report. These results held when controlling for work experience, hours worked per week, profession, managerial responsibilities, hospital department, satisfaction with work, burnout, self-rated health, and self-esteem; this is especially remarkable because some of these potential confounders (specifically, work satisfaction, burnout, self-rated health, and self-esteem) can themselves be regarded as being influenced by the occurrence of illegitimate tasks, as indicated by previous research [3]. To obtain significant results with these variables controlled suggests a unique role for illegitimate tasks, and the outcome variable of patient safety culture is undoubtedly an important one. Ultimately, the perception of illegitimate tasks can also impact the health of staff, with effects such as increased stress [38], increased feelings of resentment, exhaustion and burnout [1, 4, 5], poor sleep quality [61], and musculoskeletal pain [62].
The nature of the concept of illegitimate tasks implies that this type of stressor is often avoidable—indeed, the judgment that it should have been avoided is an important part of the appraisal as illegitimate. An obvious practical implication, therefore, is that it is important to analyse work processes with regard to illegitimate tasks; as this concept is not salient for many people, especially people who make decisions about task assignment [7, 8], some illegitimate tasks are likely to be assigned inadvertently, and sensitising people in leadership positions to this issue may already represent an important first step [3, 38]. If such assignments are unavoidable, explaining why they are unavoidable can mitigate, or even eliminate, the demeaning message entailed by the assignment of such tasks, and thus their stressful nature [63].
One implication of our (and others’) results is that it is important to sensitise leaders and managers to the concept of illegitimate tasks. This will require comprehensive interventions to optimise job design. Lean management [64, 65], participatory approaches assessing productivity [66], interventions aiming to improve social climate and avoid devaluing messages (e.g., CREW interventions [67]), and stress-oriented interventions in general [68], as well as the concept of MAGNET hospitals [69, 70], could be approaches to the optimisation of job design. However, the implementation of comprehensive approaches is challenging [65, 66, 71–73]. More small-scale interventions aiming to reduce illegitimate tasks, such as relieving physicians from administrative duties by employing scribes [74, 75], should not be neglected, although such approaches also require careful implementation [76].
Finally, although this study has indicated the relationship between perceptions of illegitimate tasks and two outcome indicators of safety culture, we consider these results to be a first step, as safety culture is a complex concept consisting of several dimensions. For example, the HSOPC questionnaire version 1 covers 12 safety culture processes, and in this study, we did not analyse the associations between illegitimate tasks and these safety culture processes. However, analysis of these associations may provide insight into the mechanisms that explain the relationship between illegitimate tasks and safety culture.
Strengths and Limitations
The strengths of this study are its relatively large sample size, the use of validated scales for assessment of exposure as well as outcomes, and the consistency of the findings across adjustment, robustness, and sensitivity analyses while controlling for many potential confounders. Its limitations include the cross-sectional design, which prohibits causal conclusions. Furthermore, the participation rate was rather low. Low participation rates are of concern, but increasing them may have only a modest influence on a study’s conclusions [77], and our results for the physician subgroups were close to those of the Thun study, which had a reasonably high participation rate [6]. The influence of low participation rates relates mainly to prevalence, and not to the associations observed between variables [78–80], especially when analyses are adjusted for factors influencing participation rates. Additionally, the survey did not ask about the gender of the participants. In existing work, gender differences have not consistently been found; for instance, [81] reported a somewhat higher occurrence of illegitimate tasks for women, but neither [82] nor Omansky et al. [30] replicated this finding, although the latter reported a stronger association between illegitimate tasks and effort–reward imbalance [83] for men, which resulted in stronger negative indirect associations with job satisfaction and intrinsic motivation. The BITS scale captures an individual assessment of whether or not a professional task is legitimate, i.e., a subjective assessment, and this assessment may be independent of whether or not the task is legitimate for the hospital. Finally, our results are based on a hospital in a French-speaking culture; their generalisability has yet to be determined.
Conclusion
The prevalence of the experience of illegitimate tasks among staff was not negligible: one in five perceived illegitimate tasks as occurring frequently. Perception of frequent occurrence of illegitimate tasks was associated with perception of low patient safety grades but with a higher number of safety event reports. Perception of illegitimate tasks is a modifiable factor, and quality improvement interventions in units with a high prevalence of illegitimate tasks may improve perceptions of patient safety among staff.
Ethics Statement
The studies involving humans were approved by Cantonal Ethics Commission of Geneva. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’legal guardians/next of kin because the survey has been exempted from ethical review by the Cantonal Ethics Commission of Geneva (reference number: req-2023-00049).
Author Contributions
Conceived and designed the study: SC, NS, FT, GC, PC, and DC. Analysed the data: SC. Drafted the manuscript: SC. Reviewed the first draft: NS and FT. Read and commented on the complete manuscript: SC, NS, FT, GC, PC, and DC. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that they do not have any conflicts of interest.
Acknowledgments
We thank Delphine Berner for her work during the data collection phase of the study.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.ssph-journal.org/articles/10.3389/ijph.2023.1606078/full#supplementary-material
References
1. Semmer, NK, Jacobshagen, N, Meier, LL, and Elfering, A. Occupational Stress Research: The “Stress-as-Offense-to-Self” Perspective. In: J Houdmont, and S McIntyre, editors. Occupational Health Psychology: European Perspectives on Research, Education and Practice. Vol. 2. Castelo da Maia, Portugal: ISMAI Publishing (2007). p. 43–60.
2. Fila, MJ, Semmer, NK, and Eatough, EM. Illegitimate Tasks as Offense to the Self. In: AM Rossi, JA Meurs, and PL Perrewé, editors. Stress and Quality of Working Life Finding Meaning in Grief and Suffering. Charlotte, NC, USA: Information Age Publishing (2020). p. 215–34.
3. Semmer, NK, Tschan, F, Jacobshagen, N, Beehr, TA, Elfering, A, Kälin, W, et al. Stress as Offense to Self: A Promising Approach Comes of Age. Occup Health Sci (2019) 3:205–38. doi:10.1007/s41542-019-00041-5
4. Werdecker, L, and Esch, T. Burnout, Satisfaction and Happiness Among German General Practitioners (GPs): A Cross-Sectional Survey on Health Resources and Stressors. PLOS ONE (2021) 16:e0253447. doi:10.1371/journal.pone.0253447
5. Kilponen, K, Huhtala, M, Kinnunen, U, Mauno, S, and Feldt, T. Illegitimate Tasks in Health Care: Illegitimate Task Types and Associations With Occupational Well-Being. J Clin Nurs (2021) 30:2093–106. doi:10.1111/jocn.15767
6. Thun, S, Halsteinli, V, and Løvseth, L. A Study of Unreasonable Illegitimate Tasks, Administrative Tasks, and Sickness Presenteeism Amongst Norwegian Physicians: An Everyday Struggle? BMC Health Serv Res (2018) 18:407. doi:10.1186/s12913-018-3229-0
7. Hamm-Vida, DE. Cost of Non-Nursing. Nurs Manage (1990) 21:46–52. doi:10.1097/00006247-199004000-00012
8. Sabo, K. Protecting the Professional Role. A Study to Review Non-Nursing Activities and Recommendations for Change. Can J Nurs Adm (1990) 3:15–8.
9. Holzer, E, Tschan, F, Kottwitz, MU, Beldi, G, Businger, AP, and Semmer, NK. The Workday of Hospital Surgeons: What They Do, What Makes Them Satisfied, and the Role of Core Tasks and Administrative Tasks; a Diary Study. BMC Surg (2019) 19:112. doi:10.1186/s12893-019-0570-0
10. Freidson, E. Profession of Medicine: A Study of the Sociology of Applied Knowledge. New York: Dodd and Mead (1970).
11. El-Jardali, F, Jaafar, M, Dimassi, H, Jamal, D, and Hamdan, R. The Current State of Patient Safety Culture in Lebanese Hospitals: A Study at Baseline. Int J Qual Health Care (2010) 22:386–95. doi:10.1093/intqhc/mzq047
12. Shu, Q, Cai, M, Tao, HB, Cheng, ZH, Chen, J, Hu, YH, et al. What Does a Hospital Survey on Patient Safety Reveal About Patient Safety Culture of Surgical Units Compared With that of Other Units? Medicine (2015) 94:e1074. doi:10.1097/MD.0000000000001074
13. Hickner, J, Smith, SA, Yount, N, and Sorra, J. Differing Perceptions of Safety Culture Across Job Roles in the Ambulatory Setting: Analysis of the AHRQ Medical Office Survey on Patient Safety Culture. BMJ Qual Saf (2016) 25:588–94. doi:10.1136/bmjqs-2014-003914
14. Listyowardojo, TA, Nap, RE, and Johnson, A. Variations in Hospital Worker Perceptions of Safety Culture. Int J Qual Health Care (2011) 24:9–15. doi:10.1093/intqhc/mzr069
15. Berry, JC, Davis, JT, Bartman, T, Hafer, CC, Lieb, LM, Khan, N, et al. Improved Safety Culture and Teamwork Climate Are Associated With Decreases in Patient Harm and Hospital Mortality Across a Hospital System. J Patient Saf (2020) 16:130–6. Publish Ahead of Print. doi:10.1097/PTS.0000000000000251
16. Carney, BT, Mills, PD, Bagian, JP, and Weeks, WB. Sex Differences in Operating Room Care Giver Perceptions of Patient Safety: A Pilot Study From the Veterans Health Administration Medical Team Training Program. Qual Saf Health Care (2010) 19:128–31. doi:10.1136/qshc.2008.028233
17. Hamdan, M, and Saleem, AA. Assessment of Patient Safety Culture in Palestinian Public Hospitals. Int J Qual Health Care (2013) 25:167–75. doi:10.1093/intqhc/mzt007
18. Nie, Y, Mao, X, Cui, H, He, S, Li, J, and Zhang, M. Hospital Survey on Patient Safety Culture in China. BMC Health Serv Res (2013) 13:228. doi:10.1186/1472-6963-13-228
19. Kirwan, M, Matthews, A, and Scott, PA. The Impact of the Work Environment of Nurses on Patient Safety Outcomes: A Multi-Level Modelling Approach. Int J Nurs Stud (2013) 50:253–63. doi:10.1016/j.ijnurstu.2012.08.020
20. Ali, H, Ibrahem, SZ, Al Mudaf, B, Al Fadalah, T, Jamal, D, and El-Jardali, F. Baseline Assessment of Patient Safety Culture in Public Hospitals in Kuwait. BMC Health Serv Res (2018) 18:158. doi:10.1186/s12913-018-2960-x
21. Mallouli, M, Tlili, MA, Aouicha, W, Ben Rejeb, M, Zedini, C, Salwa, A, et al. Assessing Patient Safety Culture in Tunisian Operating Rooms: A Multicenter Study. Int J Qual Health Care (2017) 29:176–82. doi:10.1093/intqhc/mzw157
22. Deilkås, E, and Hofoss, D. Patient Safety Culture Lives in Departments and Wards: Multilevel Partitioning of Variance in Patient Safety Culture. BMC Health Serv Res (2010) 10:85. doi:10.1186/1472-6963-10-85
23. Lee, S-H, Phan, PH, Dorman, T, Weaver, SJ, and Pronovost, PJ. Handoffs, Safety Culture, and Practices: Evidence From the Hospital Survey on Patient Safety Culture. BMC Health Serv Res (2016) 16:254. doi:10.1186/s12913-016-1502-7
24. Pratt, MG, Rockmann, KW, and Kaufmann, JB. Constructing Professional Identity: The Role of Work and Identity Learning Cycles in the Customization of Identity Among Medical Residents. Acad Manage J (2006) 49:235–62. doi:10.5465/amj.2006.20786060
25. Gillet, N, Colombat, P, Michinov, E, Pronost, A-M, and Fouquereau, E. Procedural Justice, Supervisor Autonomy Support, Work Satisfaction, Organizational Identification and Job Performance: The Mediating Role of Need Satisfaction and Perceived Organizational Support. J Adv Nurs (2013) 69:2560–71. doi:10.1111/jan.12144
26. Gurses, AP, Ozok, AA, and Pronovost, PJ. Time to Accelerate Integration of Human Factors and Ergonomics in Patient Safety. BMJ Qual Saf (2012) 21:347–51. doi:10.1136/bmjqs-2011-000421
27. Pham, JC, Aswani, MS, Rosen, M, Lee, H, Huddle, M, Weeks, K, et al. Reducing Medical Errors and Adverse Events. Annu Rev Med (2012) 63:447–63. doi:10.1146/annurev-med-061410-121352
28. Anskär, E, Lindberg, M, Falk, M, and Andersson, A. Legitimacy of Work Tasks, Psychosocial Work Environment, and Time Utilization Among Primary Care Staff in Sweden. Scand J Prim Health Care (2019) 37:476–83. doi:10.1080/02813432.2019.1684014
29. Duffield, C, Gardner, G, and Catling-Paull, C. Nursing Work and the Use of Nursing Time. J Clin Nurs (2008) 17:3269–74. doi:10.1111/j.1365-2702.2008.02637.x
30. Omansky, R, Eatough, EM, and Fila, MJ. Illegitimate Tasks as an Impediment to Job Satisfaction and Intrinsic Motivation: Moderated Mediation Effects of Gender and Effort-Reward Imbalance. Front Psychol (2016) 7:1818. doi:10.3389/fpsyg.2016.01818
31. Gabriel, AS, Diefendorff, JM, and Erickson, RJ. The Relations of Daily Task Accomplishment Satisfaction With Changes in Affect: A Multilevel Study in Nurses. J Appl Psychol (2011) 96:1095–104. doi:10.1037/a0023937
32. Semmer, NK, Tschan, F, Meier, LL, Facchin, S, and Jacobshagen, N. Illegitimate Tasks and Counterproductive Work Behavior. Appl Psychol (2010) 59:70–96. doi:10.1111/j.1464-0597.2009.00416.x
33. Schulte-Braucks, J, Baethge, A, Dormann, C, and Vahle-Hinz, T. Get Even and Feel Good? Moderating Effects of Justice Sensitivity and Counterproductive Work Behavior on the Relationship Between Illegitimate Tasks and Self-Esteem. J Occup Health Psychol (2019) 24:241–55. doi:10.1037/ocp0000112
34. Eatough, EM, Meier, LL, Igic, I, Elfering, A, Spector, PE, and Semmer, NK. You Want Me to Do what? Two Daily Diary Studies of Illegitimate Tasks and Employee Well-Being. J Organizational Behav (2016) 37:108–27. doi:10.1002/job.2032
35. Ma, J, Peng, Y, Wang, Z, Zan, J, Cao, L, Feng, Z, et al. The Performance Costs of Illegitimate Tasks: The Role of Job Identity and Flexible Role Orientation. J Vocational Behav (2019) 110:144–54. doi:10.1016/j.jvb.2018.11.012
36. Occelli, P, Quenon, JL, Kret, M, Domecq, S, Delaperche, F, Claverie, O, et al. Validation of the French Version of the Hospital Survey on Patient Safety Culture Questionnaire. Int J Qual Health Care (2013) 25:459–68. doi:10.1093/intqhc/mzt047
37. Sorra, JS, and Dyer, N. Multilevel Psychometric Properties of the AHRQ Hospital Survey on Patient Safety Culture. BMC Health Serv Res (2010) 10:199. doi:10.1186/1472-6963-10-199
38. Semmer, NK, Jacobshagen, N, Meier, LL, Elfering, A, Beehr, TA, Kälin, W, et al. Illegitimate Tasks as a Source of Work Stress. Work & Stress (2015) 29:32–56. doi:10.1080/02678373.2014.1003996
39. Abdi, Z, Delgoshaei, B, Ravaghi, H, Abbasi, M, and Heyrani, A. The Culture of Patient Safety in an Iranian Intensive Care Unit. Journal of Nurs Manage (2015) 23:333–45. doi:10.1111/jonm.12135
40. Wanous, JP, Reichers, AE, and Hudy, MJ. Overall Job Satisfaction: How Good Are Single-Item Measures? J Appl Psychol (1997) 82:247–52. doi:10.1037/0021-9010.82.2.247
41. Dolan, ED, Mohr, D, Lempa, M, Joos, S, Fihn, SD, Nelson, KM, et al. Using a Single Item to Measure Burnout in Primary Care Staff: A Psychometric Evaluation. J Gen Intern Med (2015) 30:582–7. doi:10.1007/s11606-014-3112-6
42. West, CP, Dyrbye, LN, Sloan, JA, and Shanafelt, TD. Single Item Measures of Emotional Exhaustion and Depersonalization Are Useful for Assessing Burnout in Medical Professionals. J Gen Intern Med (2009) 24:1318–21. doi:10.1007/s11606-009-1129-z
43. Idler, EL, and Benyamini, Y. Self-Rated Health and Mortality: A Review of Twenty-Seven Community Studies. J Health Soc Behav (1997) 38:21–37. doi:10.2307/2955359
44. Perneger, TV, Gayet-Ageron, A, Courvoisier, DS, Agoritsas, T, and Cullati, S. Self-Rated Health: Analysis of Distances and Transitions Between Response Options. Qual Life Res (2013) 22:2761–8. doi:10.1007/s11136-013-0418-5
45. Cullati, S, Bochatay, N, Rossier, C, Guessous, I, Burton-Jeangros, C, and Courvoisier, DS. Does the Single-Item Self-Rated Health Measure the Same Thing Across Different Wordings? Construct Validity Study. Qual Life Res (2020) 29:2593–604. doi:10.1007/s11136-020-02533-2
46. Robins, RW, Hendin, HM, and Trzesniewski, KH. Measuring Global Self-Esteem: Construct Validation of a Single-Item Measure and the Rosenberg Self-Esteem Scale. Personal Soc Psychol Bull (2001) 27:151–61. doi:10.1177/0146167201272002
47. Vifladt, A, Simonsen, BO, Lydersen, S, and Farup, PG. The Association Between Patient Safety Culture and Burnout and Sense of Coherence: A Cross-Sectional Study in Restructured and Not Restructured Intensive Care Units. Intensive Crit Care Nurs (2016) 36:26–34. doi:10.1016/j.iccn.2016.03.004
48. Kottwitz, MU, Meier, LL, Jacobshagen, N, Kälin, W, Elfering, A, Hennig, J, et al. Illegitimate Tasks Associated With Higher Cortisol Levels Among Male Employees When Subjective Health Is Relatively Low: An Intra-Individual Analysis. Scand J Work, Environ Health (2013) 39:310–8. doi:10.5271/sjweh.3334
49. Stocker, D, Jacobshagen, N, Semmer, NK, and Annen, H. Appreciation at Work in the Swiss Armed Forces. Swiss J Psychol (2010) 69:117–24. doi:10.1024/1421-0185/a000013
50. Perneger, TV, Deom, M, Cullati, S, and Bovier, PA. Growing Discontent of Swiss Doctors, 1998-2007. Eur J Public Health (2012) 22(4):478–83. doi:10.1093/eurpub/ckr114
51. Wenger, N, Méan, M, Castioni, J, Marques-Vidal, P, Waeber, G, and Garnier, A. Allocation of Internal Medicine Resident Time in a Swiss Hospital: A Time and Motion Study of Day and Evening Shifts. Ann Intern Med (2017) 166(8):579–86. doi:10.7326/M16-2238
53. Cullati, S, Perneger, TV, Scherer, F, Nendaz, M, and Escher, M. Physicians’ Views and Agreement about Patient- and Context-Related Factors Influencing ICU Admission Decisions: A Prospective Study. J Clin Med (2021) 10:3068. doi:10.3390/jcm10143068
54. Bajwa, NM, Bochatay, N, Muller-Juge, V, Cullati, S, Blondon, KS, Junod Perron, N, et al. Intra Versus Interprofessional Conflicts: Implications for Conflict Management Training. J Interprofessional Care (2020) 34:259–68. doi:10.1080/13561820.2019.1639645
55. Cullati, S, Bochatay, N, Maître, F, Laroche, T, Muller-Juge, V, Blondon, KS, et al. When Team Conflicts Threaten Quality of Care: A Study of Health Care Professionals' Experiences and Perceptions. Mayo Clinic Proc Innov Qual Outcomes (2019) 3:43–51. doi:10.1016/j.mayocpiqo.2018.11.003
56. Muller-Juge, V, Cullati, S, Blondon, KS, Hudelson, P, Maître, F, Vu, NV, et al. Interprofessional Collaboration Between Residents and Nurses in General Internal Medicine: A Qualitative Study on Behaviours Enhancing Teamwork Quality. PLOS ONE (2014) 9:e96160. doi:10.1371/journal.pone.0096160
57. Azami-Aghdash, S, Ebadifard Azar, F, Rezapour, A, Azami, A, Rasi, V, and Klvany, K. Patient Safety Culture in Hospitals of Iran: A Systematic Review and Meta-Analysis. Med J Islam Repub Iran (2015) 29:251.
58. Reis, CT, Paiva, SG, and Sousa, P. The Patient Safety Culture: A Systematic Review by Characteristics of Hospital Survey on Patient Safety Culture Dimensions. Int J Qual Health Care (2018) 30:660–77. doi:10.1093/intqhc/mzy080
59. Verbeek-Van Noord, I, Wagner, C, Van Dyck, C, Twisk, JWR, and De Bruijne, MC. Is Culture Associated With Patient Safety in the Emergency Department? A Study of Staff Perspectives. Int J Qual Health Care (2014) 26:64–70. doi:10.1093/intqhc/mzt087
60. Danielsson, M, Nilsen, P, Rutberg, H, and Årestedt, K. A National Study of Patient Safety Culture in Hospitals in Sweden. J Patient Saf (2019) 15:328–33. doi:10.1097/PTS.0000000000000369
61. Pereira, D, Semmer, NK, and Elfering, A. Illegitimate Tasks and Sleep Quality: An Ambulatory Study. Stress and Health (2014) 30:209–21. doi:10.1002/smi.2599
62. Faes, Y, and Elfering, A. When Unnecessary Tasks Weigh Heavily on the Back: A Diary Study on Musculoskeletal Pain. Workplace Health Saf (2021) 69:410–8. doi:10.1177/2165079921994830
63. Minei, EM, Eatough, EM, and Cohen-Charash, Y. Managing Illegitimate Task Requests Through Explanation and Acknowledgment: A Discursive Leadership Approach. Manage Commun Q (2018) 32:374–97. doi:10.1177/0893318918755506
64. Hihnala, S, Kettunen, L, Suhonen, M, and Tiirinki, H. The Finnish Healthcare Services Lean Management. Leadersh Health Serv (2018) 31:17–32. doi:10.1108/LHS-03-2017-0020
65. Prado-Prado, JC, García-Arca, J, Fernández-González, AJ, and Mosteiro-Añón, M. Increasing Competitiveness Through the Implementation of Lean Management in Healthcare. Int J Environ Res Public Health (2020) 17:4981. doi:10.3390/ijerph17144981
66. Arapovic-Johansson, B, Wåhlin, C, Hagberg, J, Kwak, L, Björklund, C, and Jensen, I. Participatory Work Place Intervention for Stress Prevention in Primary Health Care. A Randomized Controlled Trial. Eur J Work Organizational Psychol (2018) 27:219–34. doi:10.1080/1359432x.2018.1431883
67. Osatuke, K, Leiter, M, Belton, L, Dyrenforth, S, and Ramsel, D. Civility, Respect and Engagement at the Workplace (CREW): A National Organization Development Program at the Department of Veterans Affairs. J Manage Policies Practices (2013) 1:25–34.
68.K Nielsen, and A Noblet, editors. Organizational Interventions for Health and Well-Being: A Handbook for Evidence-Based Practice. London: Routledge (2018).
69. Anderson, VL, Johnston, ANB, Massey, D, and Bamford-Wade, A. Impact of Magnet Hospital Designation on Nursing Culture: An Integrative Review. Contemp Nurse (2018) 54:483–510. doi:10.1080/10376178.2018.1507677
70. Anstee, S, Ball, J, and Saville, C. Evaluating the Evidence: Are Magnet Hospitals Better for Staff and Patients? Nurs Times (2020) 116:45–6.
71.M Karanika-Murray, and C Biron, editors. Derailed Organizational Interventions for Stress and Well-Being. Confessions of Failure and Solutions for Success. Dordrecht, Heidelberg, New York, London: Springer (2015).
72. Parkhi, SS. Lean Management Practices in Healthcare Sector: A Literature Review. Benchmarking: Int J (2019) 26:1275–89. doi:10.1108/bij-06-2018-0166
73. Semmer, NK. Job Stress Interventions and the Organization of Work. Scand J Work, Environ Health (2006) 32:515–27. doi:10.5271/sjweh.1056
74. Bates, DW, and Landman, AB. Use of Medical Scribes to Reduce Documentation Burden: Are They Where We Need to Go With Clinical Documentation? JAMA Intern Med (2018) 178:1472–3. doi:10.1001/jamainternmed.2018.3945
75. Mishra, P, Kiang, JC, and Grant, RW. Association of Medical Scribes in Primary Care With Physician Workflow and Patient Experience. JAMA Intern Med (2018) 178:1467–72. doi:10.1001/jamainternmed.2018.3956
76. Ash, JS, Corby, S, Mohan, V, Solberg, N, Becton, J, Bergstrom, R, et al. Safe Use of the EHR by Medical Scribes: A Qualitative Study. J Am Med Inform Assoc (2021) 28:294–302. doi:10.1093/jamia/ocaa199
77. Perneger, TV, Chamot, E, and Bovier, PA. Nonresponse Bias in a Survey of Patient Perceptions of Hospital Care. Med Care (2005) 43:374–80. doi:10.1097/01.mlr.0000156856.36901.40
78. Cheung, KL, ten Klooster, PM, Smit, C, de Vries, H, and Pieterse, ME. The Impact of Non-Response Bias Due to Sampling in Public Health Studies: A Comparison of Voluntary Versus Mandatory Recruitment in a Dutch National Survey on Adolescent Health. BMC Public Health (2017) 17:276. doi:10.1186/s12889-017-4189-8
79. Nohr, EA, Frydenberg, M, Henriksen, TB, and Olsen, J. Does Low Participation in Cohort Studies Induce Bias? Epidemiology (2006) 17:413–8. doi:10.1097/01.ede.0000220549.14177.60
80. Rindfuss, RR, Choe, MK, Tsuya, NO, Bumpass, LL, and Tamaki, E. Do Low Survey Response Rates Bias Results? Evidence From Japan. Demographic Res (2015) 32:797–828. doi:10.4054/demres.2015.32.26
81. Björk, L, Bejerot, E, Jacobshagen, N, and Härenstam, A. I Shouldn't Have to Do This: Illegitimate Tasks as a Stressor in Relation to Organizational Control and Resource Deficits. Work Stress (2013) 27:262–77. doi:10.1080/02678373.2013.818291
82. Stein, M, Vincent-Höper, S, Schümann, M, and Gregersen, S. Beyond Mistreatment at the Relationship Level: Abusive Supervision and Illegitimate Tasks. Int J Environ Res Public Health (2020) 17(8):2722. doi:10.3390/ijerph17082722
Keywords: illegitimate tasks, patient safety, safety culture, patient care management, teamwork
Citation: Cullati S, Semmer NK, Tschan F, Choupay G, Chopard P and Courvoisier DS (2023) When Illegitimate Tasks Threaten Patient Safety Culture: A Cross-Sectional Survey in a Tertiary Hospital. Int J Public Health 68:1606078. doi: 10.3389/ijph.2023.1606078
Received: 10 April 2023; Accepted: 18 August 2023;
Published: 07 September 2023.
Edited by:
Olaf von dem Knesebeck, University Medical Center Hamburg-Eppendorf, GermanyCopyright © 2023 Cullati, Semmer, Tschan, Choupay, Chopard and Courvoisier. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Stéphane Cullati, c3RlcGhhbmUuY3VsbGF0aUB1bmlmci5jaA==