 Daicia Price1*
Daicia Price1* Tore Bonsaksen2,3
Tore Bonsaksen2,3 Janni Leung4Caitlin McClure-Thomas4
Janni Leung4Caitlin McClure-Thomas4 Mary Ruffolo1Gary Lamph5Isaac Kabelenga6Amy Ostertun Geirdal7
Mary Ruffolo1Gary Lamph5Isaac Kabelenga6Amy Ostertun Geirdal7- 1School of Social Work, University of Michigan, Ann Arbor, MI, United States
- 2Department of Health and Nursing Science, Faculty of Social and Health Sciences, Inland Norway University of Applied Sciences, Elverum, Norway
- 3Department of Health, Faculty of Health Studies, VID Specialized University, Stavanger, Norway
- 4Faculty of Health and Behavioural Sciences, The University of Queensland, Brisbane, QLD, Australia
- 5Department of Health Social Care and Medicine, Edge Hill University, Ormskirk, United Kingdom
- 6Department of Social Work and Sociology, School of Humanities and Social Sciences, University of Zambia, Lusaka, Zambia
- 7Department of Social Work, Child Welfare and Social Policy, Faculty of Health Sciences, Oslo Metropolitan University, Oslo, Norway
Objectives: This study aimed to examine the levels of trust in information provided by public authorities 2 years after the COVID-19 outbreak and to examine factors associated with trust.
Methods: Using a cross-national approach, online survey data was collected from four Western countries—Australia, Norway, the United Kingdom, and the United States of America. Differences in reports of very low or low levels of trust were examined by age, gender, area of residence, and the highest level of education in the four countries.
Results: Levels of trust in the public authorities’ information were highest among Norwegian respondents and lowest among U.K. respondents. Lower levels of trust in public authorities were found among males, individuals living in rural or remote areas, and those with lower levels of education.
Conclusion: The outcomes contribute to knowledge regarding differences between socio-demographic groups and countries regarding the levels of trust people have in public authorities’ information concerning a crisis, such as COVID-19. Strategies to promote trust in societies in different countries could consider these socio-demographic differences.
Introduction
The coronavirus (COVID-19) was declared a global pandemic on 11 March 2020, as media outlets shared information about a virus spreading rapidly and having fatal outcomes. Following the acknowledgment of a public health crisis, questions and concerns about the potential responses of public authorities to protect public health and safety surfaced across various forms of media [1–4].
As public authorities across the globe began to respond to the emerging pandemic, disparities among approaches were observed [1]. Each country determined its policies and procedures for health, safety, and fiscal management [1, 5, 6]. Governmental entities in Western countries responded similarly, including limiting travel, requiring face coverings, and closing businesses and schools. Despite the similar preventive measures implemented globally, compliance levels and sentiments toward the implementation differed between countries. Citizen responses to these actions varied from frustration to relief. While some individuals felt confident in the decisions of government entities to implement restrictions and follow mandates, others described a lack of trust in the information provided and beliefs that the government had hidden motives [2, 7].
Trust in government officials is developed and maintained by delivering accurate information, having consistency in responses, transparency in challenges and decision-making, and producing positive outcomes for citizens by providing valuable resources to address identified needs [4, 7, 8]. Theories of trust and social capital offer a framework to examine the connection between trust and engagement in recommendations related to a public health crisis. The theory of social capital highlights the interdependence of trust and a society that can function effectively [9]. Relationships between the general civilian public and officials with a responsibility to deliver safety and security are critical during healthcare emergencies to increase positive attitudes and behaviors from citizens that support compliance with recommendations and enhance the social efficacy of public health and wellness [10, 11].
Trust is needed to incorporate self-efficacy in the most effective and efficient ways during any stressful situation [9, 12]. People’s trust in the medical advice and information received from the government about COVID-19 had an impact on the public’s compliance with mandated lockdowns and safety recommendations [6, 7, 13–18]. Without trust, the likelihood of individuals making independent decisions to adhere to safety recommendations, even during a health crisis, is reduced. During a global crisis, the level of control a person feels they have over their situation can adversely impact their ability to engage in behaviors that are identified as helpful [7, 10, 17–19]. Associations between rates of trust in public authorities and cooperation from citizens have been noted during previous crises [9, 20]. The impact of trust in public authorities has been magnified during and after the COVID-19 pandemic as individuals are encouraged to participate in prevention strategies such as minimizing contact with others, wearing masks, and obtaining a vaccine to prevent the rapid spread of the virus [2, 21, 22].
Studies examining trust in public authorities during COVID-19 have provided information about ongoing connections between trust and outcomes. Goldfinch et al. (2021) found that levels of trust in public authorities were associated with how the government responded to the pandemic. If the responses of the government were viewed to be effective in reducing the spread and lethality of the coronavirus, trust levels were increased, and the adverse impacts of COVID-19 were less than in areas where rates of trust were lower [5, 17, 22]. This is consistent with previous public health issues reported [16, 23–25]. In a cross-national study nine months after the COVID-19 outbreak, identifying as female, having higher levels of education, and living in urban areas were associated with trust in public authorities; however, being infected with the coronavirus was associated with distrust [26].
Researchers note that the U.S. and the U. K. had higher levels of infection and fatalities and citizens were more likely to report distrust in the responsiveness of public authorities to COVID-19 [7, 14, 19, 24, 26]. A focus on supporting the national economy and not the health and safety of citizens, along with perceived slow and disjointed responses at the federal and state or provincial levels to respond to the global pandemic, has been noted as a contributor to the lack of trust in public authorities [2, 5, 7, 17, 19, 27].
As COVID-19 continues to be a leading cause of death globally, with 6,897,025 deaths as of 11 April 2023, ongoing interventions are critical (WHO, 2022). Coronavirus has highlighted disparities between confidence and trust in public authorities. The inconsistencies require ongoing knowledge contribution to examine population responses in countries with similar social-political contexts [28]. As citizens worldwide vary in their willingness to engage in COVID-19 prevention and intervention measures, understanding levels of trust in public authorities is critical in the ongoing efforts to address the continuous disruption that COVID-19 has on individual lives and communities.
To contribute to the scientific knowledge, examining trust in public authorities can provide information for public authorities to engage citizens unwilling or hesitant to adhere to policy, procedure, and practice recommendations to reduce the spread and lethality of COVID-19 at various time intervals of an international health crisis. The primary source of information specific to COVID-19 often relies on information provided by public authorities [25]. Increasing the availability of independent findings based on individual reports is critical when considering levels of trust in public authorities to offer additional references for knowledge.
To expand on existing knowledge, this study examines the levels of trust in information provided by public authorities two years after the COVID-19 outbreak in four Western countries—Australia, Norway, the United Kingdom, and the United States—to examine factors associated with trust.
Methods
Design and Procedures
This study reports from the third cross-sectional survey disseminated openly in four countries (Norway, U.K., U.S., and Australia) during the COVID-19 pandemic. Participants were recruited from the countries where the researchers were based. The current survey was available for the general public’s participation between November 2021 and January 2022. A public landing site for the web-based survey was established and shared through personal and professional networks using electronic mail communication and various social media platforms (e.g., Facebook ads; university Facebook and Twitter websites). The initiator of the project was AØG from OsloMet. Due to ethical considerations and permissions, each country had its own project lead. The survey was simultaneously co-developed by the researchers in two languages—Norwegian and English. It was based on previous surveys conducted by the research group in the early phase (April 2020) and mid-point (November 2020) of the pandemic outbreak [26, 29–32]. Language and cultural differences were considered during the survey development process. During this period, access to COVID-19 vaccinations was available in each country where participants were recruited, and many public health restrictions were lifted. While the participants were recruited from four different countries, the survey captured the perspectives of individuals in those countries who completed the survey and is not intended to be representative of the country’s population.
Inclusion
To be included in the study, participants had to be 18 years or older, understand Norwegian or English, live in Norway, USA, U.K., or Australia, and have access to an electronic device and internet.
Measures
Sociodemographic Characteristics
The sociodemographic variables include age group (categories measured were: 18–29 years, 30–39 years, 40–49 years, 50–59 years, 60–69 years, 70 years and above), gender identity (male, female, other, prefer not to respond), place of residence (rural or farming area; town or suburb; city), and highest completed education level (high school or associated/technical degree or lower, Bachelor’s degree, Master’s/doctoral degree).
Trust in Public Authorities
The primary outcome variable—trust in communications issued by authorities—was constructed from the following question: “What is your level of trust in the information provided to the public by government and public authorities about the COVID-19 pandemic?” Participants were asked to respond using a 5-point scale with options of very low, low, moderate, high, or very high.
Statistical Analysis
Descriptive statistics were examined for each variable by country, and chi-square tests were conducted to examine differences. Responses to the level of trust were analyzed as (1) very low or low, and (2) moderate, high, or very high. Proportions of participants reporting very low or low trust were cross-tabulated by the socio-demographic variables with chi-squared tests to examine the bi-variate associations. Multivariate logistic regression was conducted with all socio-demographic variables included on low or very low levels of trust as the outcome (reference: moderate, high, or very high trust). Odds ratios with 95% confidence intervals (CI) were presented with p-values. First, a regression was conducted, testing for all main effects. Second, the regression analysis was repeated, including interaction terms of each socio-demographic variable by country, to test for the robustness of effects by country. For following up significant country interactions, stratified regression analyses (separate analysis for each country) were conducted, and odds ratios of the socio-demographic variables on trust that had a significant by-country interaction were presented. There was no missing data.
Ethics
The data collected in this study was anonymous. The researchers adhered to all relevant regulations in their respective countries concerning ethics and data protection.
Results
Participants
The total number of participants was 1,649, with 242 (14.7%) from Norway, 255 (15.15%) from the U.K., 915 (55.5%) from the U.S., and 237 (14.4%) from Australia (see Table 1). The age distribution shows a spread of ages, skewing towards younger ages in the U.K. and USA samples and older ages in the Australian sample. Women comprised the larger part of the sample (75% identified as female, 20% identified as male, and 4% identified as other/prefer not to respond), particularly in the Australian sample (81% female). The majority of the sample from Norway and Australia lived in city areas, while the majority of the sample from the U.K. and USA were in towns or suburbs. Over 70% of participants had a bachelor’s degree or higher; the Australian sample had the highest proportion of individuals with vocational training, and the USA sample had the highest proportion with a Master’s degree or above.
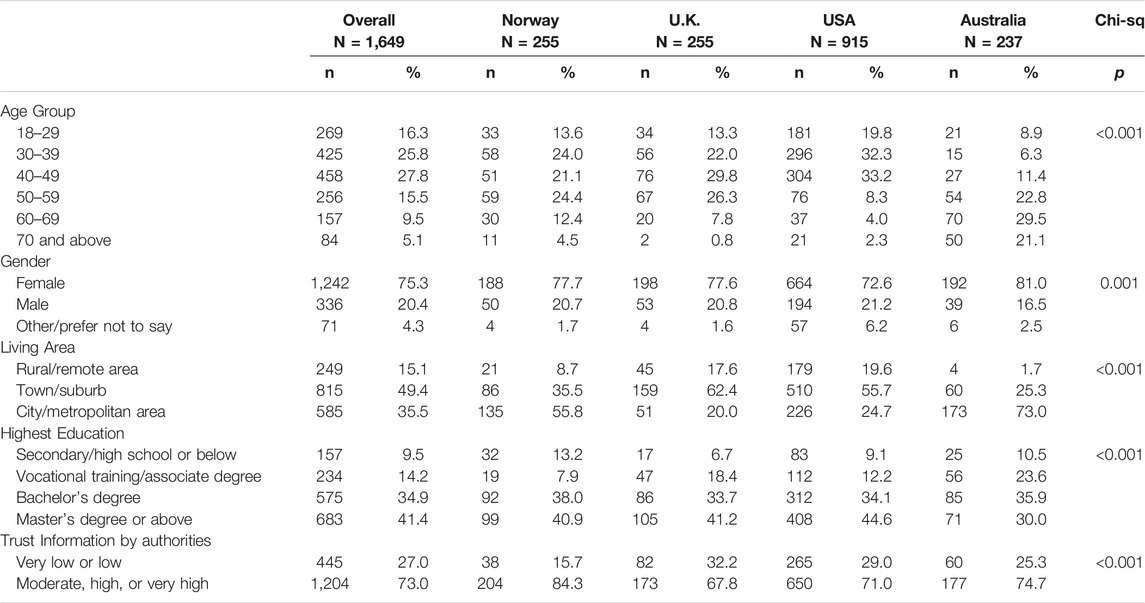
TABLE 1. Descriptive Statistics (Factors Associated with Trust in Public Authorities Among Adults in Norway, UK, US, and Australia Two Years after the COVID-19 Outbreak, Norway, United Kingdom, United States, and Australia. 2022).
In our overall sample, 27% reported very low or low trust. The U.K. had the highest proportion reporting very low or low trust (32%), followed by the USA (29%), Australia (25%), and Norway with the lowest proportion (16%), p < 0.001.
Trust in Sample Subgroups
Significant group differences in the level of trust in information from public authorities are shown in Table 2. Significant differences (≤0.001) were observed in reports of trust in information between countries, age groups, genders, living areas, and educational levels. Self-reports of very low or low trust were more common in the 40–49 age group, male or other genders, individuals living in rural or remote areas, and those with lower levels of education.
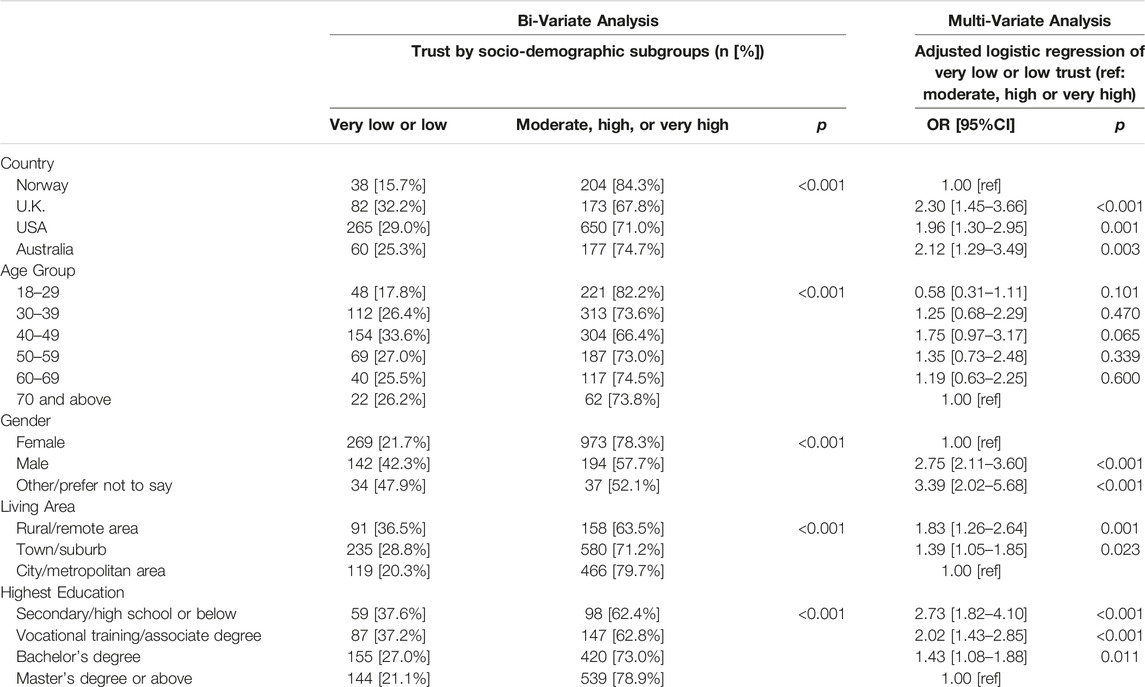
TABLE 2. Cross-tabulation of trust by socio-demographic factors and adjusted regression on trust (Factors Associated with Trust in Public Authorities Among Adults in Norway, UK, US, and Australia Two Years after the COVID-19 Outbreak, Norway, United Kingdom, United States, and Australia. 2022).
Regression of Socio-Demographic Factors Associated With Trust
Factors associated with trust in public authorities’ information are shown in Table 2. Levels of trust in information varied by country (p < 0.001); the odds of reporting very low or low trust were about two times higher in the U.K., USA, and Australia, compared to Norway. In the unadjusted analysis, the 40–49 age group had higher odds of reporting very low or low trust than the 70+ group. Still, it was not statistically significant after controlling for all other variables examined. After adjustment for all variables, males and those who selected “other” or “preferred not to say” had 2.75 [2.11–3.60] and 3.39 [2.02–5.68] higher odds of reporting very low or low trust (p < 0.001) than females, respectively. Area of residence was associated with trust, with those living in rural or remote areas and those living in towns or suburbs more likely to report low or very low trust than those living in city or metropolitan areas. A dose-response trend was observed with education, such that the lower the level of education, the higher odds of reporting very low or low trust.
Significant interactions were observed for gender*country and education*country. Stratified regression analyses by country show that the dose-response trend of lower education with lower trust was only observed in the USA (see Table 3). In the U.K., the lowest education group had higher odds of low or very low trust, but it was not statistically significant. In Australia, the lowest education group had the lowest odds of low trust (p < 0.001). For the Norway participants, only the lowest education group had higher odds of very low or low trust compared to the highest education group (p = 0.003).
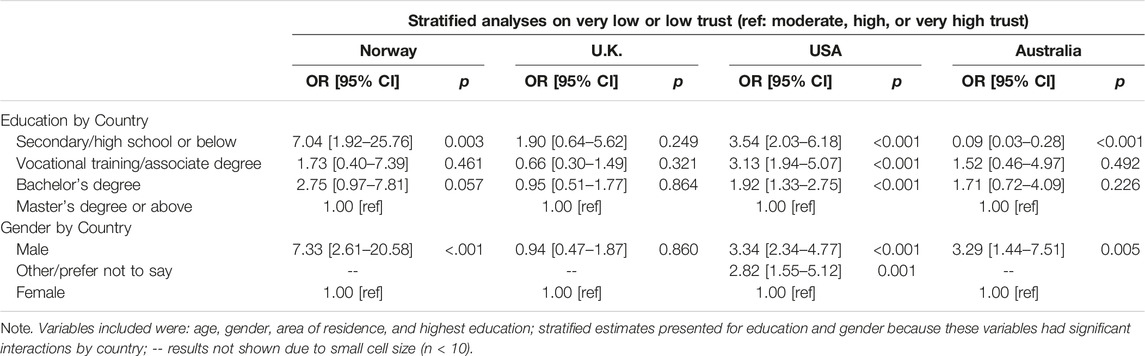
TABLE 3. Associations of Education and Gender on Very Low or Low Trust by Country (Factors Associated with Trust in Public Authorities Among Adults in Norway, UK, US, and Australia Two Years after the COVID-19 Outbreak, Norway, United Kingdom, United States, and Australia. 2022).
For gender, only the U.S. had an adequate sample size to show that the “other” or “prefer not to say” gender group had higher odds of very lower trust. In the U.K., there were no significant gender differences found in trust in the adjusted analysis (p = 0.860). Males consistently had higher odds of having low trust in the other countries (see Table 3).
Discussion
The main findings in this study were that respondents that were residents of Norway, compared to those from Australia, the United Kingdom, and the United States, had higher levels of trust in information provided by public authorities after two years of being in a global pandemic. Middle age, male or other genders, living in rural or remote areas, and lower levels of education were significantly associated with very low or low trust, as were gender and education when including interaction terms by country, to test for the robustness of effects by country.
Norway was identified as a country that was immediately responsive and provided daily information through press conferences that were easily accessible to citizens [33, 34]. Outcomes from the Norwegian, but also Australian authority responses that were identified as strong, collaborative, and intentional demonstrate that a response focused on engaging citizens to work collectively can be effective in addressing a global pandemic [33, 35, 36]. In contrast, the U.K. and the U.S. have both been criticized for lack of immediate response to COVID-19 and continue to receive criticism for a delayed response by public authorities as the public quarantine requirements occurred after Norway [37, 38]. The U.K. and the U.S. had a high rate of infections and fatalities, and several researchers reported distrust in the public authority’s responses.
Trust can be associated with the current political climate; therefore, observing differences among countries can support the understanding of factors that impact levels of trust. Political stability, transparency in decision-making, and distribution of access to resources in the U.S. and the U.K. can be a potential explanation for the observed lower levels of trust in responses [9, 23, 24, 35, 39]. Public critiques of the public authorities in leadership in the U.S. and U.K. label leaders as careless and not adhering to global recommendations. The public opinions and critiques of leadership may be contributing factors to the lower trust levels of respondents in these countries. It may be a plausible argument for the odds of reporting very low or low trust, about two times higher in these countries compared to Norway.
The findings provide additional support to adhering to Idowu et al.’s [2] recommendations regarding the social responsibility in the health sector during a global pandemic. Findings from this study also align with examinations of trust among British individuals during COVID-19 [14]. Balaet et al. examined the relationship between feelings of trust, thoughts about COVID-19, and behaviors. To promote public health during a pandemic, it may be imperative to engage with individuals and groups with low levels of trust, as they may be hesitant to engage in prevention strategies recommended by public authorities. Identifying methods of public engagement and trust-building used in countries that have higher rates of trust can provide guidance on ways to improve public trust and compliance. One method of public engagement is to publish data collected directly from participants instead of large datasets collected by public authorities or entities that have lower levels of trust and analyzed by research teams that do not receive funding from public authorities [7, 10, 11, 17–19, 40]. This information can support recent literature reports that trust in the information of public authorities remains a critical factor when addressing a global health crisis [2, 9, 22, 23, 25].
Ongoing efforts to be responsive to people who have low levels of trust in public authorities should be incorporated into policies, procedures, and protocols globally to continue to enhance the safety of individuals and communities.
Study Limitations
Participants were invited electronically and via social media platforms to participate in our online survey; therefore, those in the population who did not use social media or the internet are not represented in this study. The study included a higher proportion of female respondents and those with higher levels of education. Although anyone with access to the internet within the four countries could participate, we may have a higher number of participants geographically located closer to our landing sites due to recruitment through the universities. The results are, therefore, not representative of the population in the four countries. As the survey was open to an unlimited amount of people, we are unable to report on response rates. The U.S. respondents comprised more than half of the total sample, having a larger influence on the results of the total sample. This study had a small sample of people who identified as other gender (than male or female), which did not reach the sample size required for analysis. Thus, we have a limited understanding of the experience of non-binary respondents. Trust was measured in relation to the COVID-19 pandemic. Since we did not ask about trust in general, we do not have information to compare general levels of trust in the community. There are pre-existing differences in the general levels of trust of the general population between the countries in our study, which may have increased or decreased due to how the government and authorities have responded to the pandemic [41, 42]. Racial identity was not examined as an independent variable concerning trust due to the cultural differences among the participating countries and differences in the interpretation of race. There was no analysis of the types of information received by respondents from public authorities.
Conclusion
This study examined trust in public authorities held by the general population two years after COVID-19 was declared a global pandemic. We find significant differences in levels of trust between countries and between sociodemographic groups observed.
This study provides input for public authorities on the need to identify and target groups based on their trust level, which may impact their willingness to obtain a vaccine and utilize other prevention strategies, especially regarding the information provided by public officials. It is critical that public authorities use engagement strategies that promote trust in information and policies. Specific consideration to populations that have lower rates of trust should be made along with an understanding of the historical context that impacts engagement.
Practices that increase levels of trust in public authorities implemented by some countries should be expanded to mitigate the ongoing negative impacts of COVID-19 across the globe. Future research needs to continue to measure change over time and focus on shifts in trust in public authorities after the COVID-19 pandemic to consider additional behavioral trends.
Professionals responsible for social welfare, policy development, and program administration should be aware of the differences in the general public’s likelihood to trust information and financial support offerings when developing programs that target diverse population groups. Trust among citizens may be a vital component when seeking to increase the effectiveness of interventions used to support community safety and wellness. Increasing trust may foster higher levels of public health compliance to reduce the spread of COVID-19 and other public health concerns.
Ethics Statement
The studies involving human participants were reviewed and approved by the OsloMet (20/03676) and the regional committees for medical and health research ethics (REK; ref. 132066) in Norway, reviewed by the University of Michigan Institutional Review Board for Health Sciences and Behavioral Sciences (IRB HSBS) and designated as exempt (HUM00180296) in USA, and the University of Central Lancashire (Health Research Panel) (HEALTH 0246) in the UK, and The University of Queensland (HSR1920-080 2020000956) in Australia. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Conflict of Interest
The authors declare that they do not have any conflicts of interest.
References
1. Elgin, C, Basbug, G, and Yalaman, A. Economic Policy Responses to a Pandemic: Developing the COVID-19 Economic Stimulus index. In: Covid Economics: Vetted and Real Time Papers, 3 (2020). p. 40–54.
2. Idowu, SO, Idowu, MT, and Idowu, AO. Corporate Social Responsibility in the Health Sector – CSR and COVID-19 in Global Health Service Institutions. Geneva: Springer (2023).
3. Kabelenga, I, and Chola, J. Social Protection and COVID-19: Impacts on Informal Economy Workers in Rural and Urban Zambia. Lusaka: Fredrich Ebert Stiftung FES (2021).
5. Hale, T, Petherick, A, Phillips, T, and Webster, S. Variation in Government Responses to COVID-19. Oxford: Oxford University (2020).
6.OECD. Trust in Government, Policy Effectiveness and the Governance Agenda. In: Government at a Glance 2013. Paris: OECD Publishing (2013). doi:10.1787/gov_glance-2013-6-en
7. Jakovljevic, M, Bedov, S, Mustac, F, and Jakovljevic, I. COVID-19 Infodemic and Public Trust from the Perspective of Public and Global Mental Health. Psychiatr Danubina (2020) 32(3-4):449–57. doi:10.24869/psyd.2020.449
8. Bouckaert, G, and Van de Walle, S. Government Performance and Trust in Government. In: Paper for the Permanent Study Group of Productivity and Quality in the Public Sector at the European Group of Public Administration Annual Conference; Vaasa: Finland (2001).
9. Rothstein, B, and Stolle, D. The State and Social Capital: An Institutional Theory of Generalized Trust. Comp Polit (2008) 40(4):441–59. doi:10.5129/001041508x12911362383354
10. Kabelenga, I, and Noyoo, N. The Private Sector’s Role in Strengthening Hospitals in Zambia during the Coronavirus (COVID-19) Pandemic: A Corporate Social Responsibility (CSR) Perspective. In: Corporate Social Responsibility in the Health Sector – CSR and COVID-19 in Global Health Service Institutions. Geneva: Springer (2023).
11. Levi, M, and Stoker, L. Political Trust and Trustworthiness. Annu Rev Polit Sci (2000) 3(1):475–507. doi:10.1146/annurev.polisci.3.1.475
12. Bandura, A. Self-efficacy in Changing Societies. Cambridge, England: Cambridge University Press (1995).
13. Anastasiou, E, and Duquenne, M. First-wave COVID-19 Pandemic in Greece: The Role of Demographic, Social, and Geographical Factors in Life Satisfaction during Lockdown. Soc Sci (2021) 10:186. doi:10.3390/socsci10060186
14. Balaet, M, Kurtin, D, Gruia, D, Lerede, A, Custovic, D, Trender, W, et al. Who and Why: A Study of British Distrust in the Government and media during the COVID-19 Pandemic. (2022). doi:10.21203/rs.3.rs-1564442/v1
15. Guillon, M, and Kergall, P. Attitudes and Opinions on Quarantine and Support for a Contact-Tracing Application in France during the COVID-19 Outbreak. Public Health (London) (2020) 188:21–31. doi:10.1016/j.puhe.2020.08.026
16. Majid, U, Wasim, A, Truong, J, and Bakshi, S. Public Trust in Governments, Health Care Providers, and the media during Pandemics: A Systematic Review. J Trust Res (2021) 11(2):119–41. doi:10.1080/21515581.2022.2029742
17. Newton, K. Government Communications, Political Trust and Compliant Social Behaviour: The Politics of COVID-19 in Britain. Polit Q (2020) 91(3):502–13. doi:10.1111/1467-923X.12901
18. Wong, C, and Jensen, O. The Paradox of Trust: Perceived Risk and Public Compliance during the COVID-19 Pandemic in Singapore. J Risk Res (2020) 23(7–8):1021–30. doi:10.1080/13669877.2020.1756386
19. Oude-Groeniger, J, Noordzij, K, Van Der Waal, J, and De Koster, W. Dutch COVID-19 Lockdown Measures Increased Trust in Government and Trust in Science: A Difference-In-Differences Analysis. Soc Sci Med (2021) 275:113819. doi:10.1016/j.socscimed.2021.113819
20. Chanley, V, Rudolph, T, and Rahn, W. The Origins and Consequences of Public Trust in Government: A Time Series Analysis. Public Opin Q (2000) 64(3):239–56. doi:10.1086/317987
21. Deslatte, A. The Erosion of Trust during a Global Pandemic and How Public Administrators Should Counter it. Am Rev Public Adm (2020) 50(6–7):489–96. doi:10.1177/0275074020941676
22. Pak, A, McBryde, E, and Adegboye, O. Does High Public Trust Amplify Compliance with Stringent COVID-19 Government Health Guidelines? A Multi-Country Analysis Using Data from 102,627 Individuals. Risk Manage Healthc Pol (2021) 14:293–302. doi:10.2147/RMHP.S278774
23. Bargain, O, and Aminjonov, U. Trust and Compliance to Public Health Policies in Times of COVID-19. J Public Economy (2020) 192:104316. doi:10.1016/j.jpubeco.2020.104316
24. Goldfinch, S, Taplin, R, and Gauld, R. Trust in Government Increased during the COVID-19 Pandemic in Australia and New Zealand. Aust J Public Adm (2021) 80(1):3–11. doi:10.1111/1467-8500.12459
25. Shanka, MS, and Menebo, MM. When and How Trust in Government Leads to Compliance with COVID-19 Precautionary Measures. J Business Res (2022) 139(2):1275–83. doi:10.1016/j.jbusres.2021.10.036
26. Price, D, Bonsaksen, T, Ruffolo, M, Leung, J, Chiu, V, Thygesen, H, et al. Perceived Trust in Public Authorities Nine Months after the COVID-19 Outbreak: A Cross-National Study. Soc Sci (2021) 10(9):349. doi:10.3390/socsci10090349
27. Goldstein, D, and Wiedemann, J. Who Do You Trust? the Consequences of Partisanship and Trust for Public Responsiveness to COVID-19 Orders. Perspect Polit (2022) 20(2):412–38. doi:10.1017/S1537592721000049
28. Mathieu, E, Ritchie, H, Ortiz-Ospina, E, Roser, M, Hasell, J, Appel, C, et al. A Global Database of COVID-19 Vaccinations. Nat Hum Behav (2021) 5(7):947–53. doi:10.1038/s41562-021-01122-8
29. Bonsaksen, T, Schoultz, M, Thygesen, H, Ruffolo, M, Price, D, Leung, J, et al. Loneliness and its Associated Factors Nine Months after the COVID-19 Outbreak: A Cross-National Study. Int J Environ Res Public Health (2021) 18(6):2841. doi:10.3390/ijerph18062841
30. Geirdal, AØ, Ruffolo, M, Leung, J, Thygesen, H, Price, D, Bonsaksen, T, et al. Mental Health, Quality of Life, Wellbeing, Loneliness and Use of Social media in a Time of Social Distancing during the COVID-19 Outbreak: A Cross-Country Comparative Study. J Ment Health (2021) 30(2):148–55. doi:10.1080/09638237.2021.1875413
31. Ruffolo, M, Price, D, Schoultz, M, Leung, J, Bonsaksen, T, Thygesen, H, et al. Employment Uncertainty and Mental Health during the COVID-19 Pandemic Initial Social Distancing Implementation: A Cross-National Study. Glob Soc Welfare (2021) 8(2):141–50. doi:10.1007/s40609-020-00201-4
32. Thygesen, H, Bonsaksen, T, Schoultz, M, Ruffolo, M, Leung, J, Price, D, et al. Use and Self-Perceived Effects of Social media before and after the COVID-19 Outbreak: a Cross-National Study. Health Technol (2021) 11:1347–57. doi:10.1007/s12553-021-00595-x
33. Moss, SM, and Sandbakken, EM. “Everybody Needs to Do Their Part, So We Can Get This under control.” Reactions to the Norwegian Government Meta-Narratives on COVID-19 Measures Polit Psychol (2021) 42(5):881–98. doi:10.1111/pops.12727
34. Ursin, G, Skjesol, I, and Tritter, J. The COVID-19 Pandemic in Norway: The Dominance of Social Implications in Framing the Policy Response. Health Pol Technol (2020) 9(4):663–72. doi:10.1016/j.hlpt.2020.08.004
35. Christensen, T, and Lægreid, P. Trust in Government: The Relative Importance of Service Satisfaction, Political Factors, and Demography. Public Perform Manage Rev (2005) 28(4):487–511. doi:10.1080/15309576.2005.11051848
36. Holley, A, Coatsworth, N, and Lipman, J. The Australian Response to the COVID-19 Pandemic: A Co-ordinated and Effective Strategy. Anaesth Crit Care Pain Med (2021) 40(2):100859. doi:10.1016/j.accpm.2021.100859
37. Hick, R, and Murphy, MP. Common Shock, Different Paths? Comparing Social Policy Responses to COVID-19 in the U.K. And Ireland. Soc Pol Adm (2021) 55(2):312–25. doi:10.1111/spol.12677
38. Unruh, L, Allin, S, Marchildon, G, Burke, S, Barry, S, Siersbaek, R, et al. A Comparison of 2020 Health Policy Responses to the COVID-19 Pandemic in Canada, Ireland, the United Kingdom and the United States of America. Health Policy (2022) 126(5):427–37. doi:10.1016/j.healthpol.2021.06.012
39. Enria, L, Waterlow, N, Rogers, N, Brindle, H, Lal, S, Eggo, R, et al. Trust and Transparency in Times of Crisis: Results from an Online Survey during the First Wave (April 2020) of the COVID-19 Epidemic in the U.K. PloS one (2021) 16(2):e0239247. doi:10.1371/journal.pone.0239247
40. Charron, N, and Rothstein, B. Does Education lead to Higher Generalized Trust? the Importance of Quality of Government. Int J Educ Dev (2016) 50:59–73. doi:10.1016/j.ijedudev.2016.05.009
41. Dalton, R. The Social Transformation of Trust in Government. Int Rev Sociol (2005) 15(1):133–54. doi:10.1080/03906700500038819
Keywords: coronavirus, pandemic, vaccination, trust, public authorities
Citation: Price D, Bonsaksen T, Leung J, McClure-Thomas C, Ruffolo M, Lamph G, Kabelenga I and Ostertun Geirdal A (2023) Factors Associated with Trust in Public Authorities Among Adults in Norway, United Kingdom, United States, and Australia Two Years after the COVID-19 Outbreak. Int J Public Health 68:1605846. doi: 10.3389/ijph.2023.1605846
Received: 04 February 2023; Accepted: 07 June 2023;
Published: 02 August 2023.
Edited by:
Andrea Madarasova Geckova, University of Pavol Jozef Šafárik, SlovakiaReviewed by:
Pauline Kergall, Université de Montpellier, FranceMichal Kentos, Slovak Academy of Sciences (SAS), Slovakia
Copyright © 2023 Price, Bonsaksen, Leung, McClure-Thomas, Ruffolo, Lamph, Kabelenga and Ostertun Geirdal. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daicia Price, ZGFpY2lhcnNAdW1pY2guZWR1