 Sirinya Phulkerd1*†
Sirinya Phulkerd1*† Sasinee Thapsuwan1†Rossarin Soottipong Gray1†Aphichat Chamratrithirong1†Umaporn Pattaravanich1†Chantana Ungchusak2Pairoj Saonuam2†
Sasinee Thapsuwan1†Rossarin Soottipong Gray1†Aphichat Chamratrithirong1†Umaporn Pattaravanich1†Chantana Ungchusak2Pairoj Saonuam2†- 1Institute for Population and Social Research, Mahidol University, Nakhon Pathom, Thailand
- 2Healthy Lifestyle Promotion Section of Thai Health Promotion Foundation, Bangkok, Thailand
Objective: To investigate prevalence of life satisfaction in the Thai population before and during the COVID-19 epidemic, and factors associated with life satisfaction during the epidemic.
Methods: Multistage sampling was used to draw a sample from the Thai population. A total of 3,115 Thai participants age 15 years or older from a nationally-representative longitudinal survey in 2019 and in 2021 were included in this study. The study applied the Scale with Life Satisfaction (SWLS) instrument to measure life satisfaction among the Thai population before and during the COVID-19 epidemic. Multiple regression analysis was used to investigate the association between life satisfaction and other variables. The follow-up survey response rate for individuals was 44.8%.
Results: An average life satisfaction score during the COVID-19 epidemic (in 2021) was 22.4 which decreased from 25.5 before the COVID-19 epidemic (in 2019). More than one-third of the participants (36.5%) reported having less life satisfaction during the epidemic, which was nearly 20 percentage points higher than before the epidemic (17.7%). Controlling for life satisfaction in 2019, the analysis found statistical associations between demographic and economic characteristics and health-related behaviours, and life satisfaction during 2021. People in the older age cohorts (p ≤ 0.001), in a rural area (p ≤ 0.05), having higher education (p ≤ 0.001), still being employed (p ≤ 0.01) and becoming unemployed (p ≤ 0.01) had higher life satisfaction. The possibility of higher life satisfaction was also found in people who maintained good health (p ≤ 0.01), sufficient physical activity (p ≤ 0.001), and fruit and vegetable intake (p ≤ 0.01). People with income loss during the epidemic had lower life satisfaction (p ≤ 0.05).
Conclusion: The findings suggest that policies and systems for resilience and social protection are needed for empowering individuals—especially the poor and vulnerable—to cope with crises, and improve health and wellbeing outcomes.
Introduction
The COVID-19 pandemic has had both positive and negative psychological effects on populations worldwide. Recent COVID-19 studies have demonstrated such positive benefits for people as more opportunity for strengthening family relationships and finding new hobbies [1], and for reducing air pollution, improving air and water quality and lowering noise levels [2]. However, more studies have documented the adverse effects of COVID-19 and harsh control measures on psychological outcomes, such as anxiety, distress, depression, anger, and fear [3] that can erode wellbeing and life satisfaction [4, 5]. This unhealthy state may impact negatively on physical health and longevity [6]. It is also well-known that wellbeing in childhood is predictive of wellbeing in adulthood [7].
The spread of COVID-19 has an impact on individual life satisfaction in many countries. Previous studies showed the negative correlation between life satisfaction and COVID-19 in Northern Europe; however, there was insignificant correlation in Southern and Western Europe [8]. A study with university students in European and Latin America countries found that poor self-rated physical health was a distinct predictor of low life satisfaction during the pandemic [9]. Another study in Poland investigated an influence of fear of COVID-19 on life satisfaction during the pandemic [10]. The results showed a negative association between these two variables that health-related hardiness and sense of coherence were found to be important mediators between them. These findings point to the importance of giving special public health attention that should be focused on psychologically supporting people during and after the pandemic.
The COVID-19 epidemic in Thailand began in March 2020 (as the 1st wave), where the first outbreaks were traced to a group of spectators at a boxing event and a cluster of nighttime entertainment establishments. COVID-19 then spread to 68 of Thailand’s 77 provinces [11]. Harsh government containment measures (e.g., closing international borders, closing nighttime entertainment establishments, closing schools, nighttime curfews, area-specific lockdowns, etc.) managed to slow spread of COVID-19 to a trickle for most of the rest of 2020. However, as the virus evolved into more infectious variants, new outbreaks occurred, starting with a 2nd wave in December 2020, a 3rd wave in April 2021, a 4th wave in June 2021, and a 5th wave in January 2022. Research studies started to report the negative effects of the epidemic on mental health of Thais. University students reported having stress, anxiety, and depression during the epidemic [12]. The anxiety was the most common affliction among students, followed by depression, and stress. One study examined the effect of the epidemic on wellness of students enrolled in health profession curricula and found elevated levels of anxiety [13]. That study also reported increased sedentary behavior and undesirable weight gain. Thai healthcare workers also experienced negative mental health outcomes during the epidemic, such as burnout, anxiety, depression, and post-traumatic stress [14].
Despite a growing number of studies on the impact of the COVID-19 epidemic on various aspects of mental health outcomes among Thais, there is limited evidence on how the epidemic may be affecting general wellbeing of the population, especially life satisfaction. The United Nations Population Fund reported that Thai older persons had lower life satisfaction during the epidemic compared with before COVID-19 [15]. Those in urban areas were twice as likely as their rural counterparts to report lower life satisfaction. Another study found a positive correlation between life satisfaction and receiving government relief payments and other financial support for the working-age population [16]. As yet, no studies have investigated the prevalence of life satisfaction among Thais at the population level and across age groups, with a comparison before and during the epidemic. In addition, there has not been a clear identification of determinants of vulnerability to life satisfaction during a national disaster such as COVID-19.
Therefore, this study investigated the prevalence of life satisfaction in the Thai population before and during the COVID-19 epidemic, and identified factors associated with individual life satisfaction during the epidemic. Findings of this study should help the Thai government and other stakeholders to better understand the situation of life satisfaction among Thais across age groups. This information can be used to design programs and interventions to restore life satisfaction to pre-epidemic levels, and intensify the effort to “leave no one behind” which is the central promise of the 2030 Sustainable Development Agenda. Ultimately, it can be expected that improved wellbeing, especially among vulnerable groups, will contribute to better individual performance at work [17], as well as better national economic performance for the nation as a whole [18].
Methods
Study Design and Participants
This study used individual-level data from a nationally-representative, population-based longitudinal survey of the Thai population in 2019 (pre-epidemic) and in 2021 (during the 3rd and 4th waves) that follows food consumption, health behaviour, and wellbeing of Thais age 6 years or older.
This study focused on the sub-group of the sample age 15 years or older who responded to questions on life satisfaction. The study recruited participants in the 2019 survey using multistage stratified sampling design to obtain a representative sample of Thai population that can generate generalisable findings of the study. The sampling design and sample size calculation were conducted by the National Statistical Office of Thailand (NSO) - the Thai government’s official statistics surveyor - which is responsible for conducting and facilitating census and sample surveys for national statistical information database.
In the 2019 survey the NSO conducted the stratified sampling in four stages. The first stage involved a systematic sampling of two provinces within each geographic region. The selected provinces were Nakhon Pathom and Prachin Buri in Central region, Nakhon Sawan and Lampang in Northern region, Surin and Udon Thani in Northeast region, and Songkhla and Phatthalung in South region. Bangkok was also included as it is the sole special administrative area in Thailand. In total, nine provinces were sampled in this study. In the second stage, a systematic sampling of postal districts within each province by considering administrative boundaries (urban and rural areas) was conducted. This involved the selection of enumeration areas (EAs) and households (20 households in each EA). A household list was provided by the National Statistical Office. In the third stage, a systematic sampling of households nested within each selected EA was obtained. Each household was then contacted for study participation. At the final stage, all the household members who met the following inclusion criteria were invited to take part in the study.
Inclusion criteria for participation in this study were that a participant must have/have been: 1) lived in the selected household, 2) available during a visit by research team, 3) at least 15 years of age, 4) fluent in Thai (i.e., able to speak, read and write), and willing and able to participate in a face-to-face interview. A participant who had a condition or was in a situation which may have put him/her at significant risk, or may have confounded the study results was excluded.
The 2021 survey was a nested study within the 2019 survey. All the 2019 participants were recruited to take part the 2021 survey.
Data Collection
Of the total 3,720 sampled households in the initial year, 3,297 households in 2019 (response rate 88.6%) and 2,647 households in 2021 (follow-up rate 80.3%) successfully participated in the survey (Table 1). Participant recruitment was conducted during 1st July in 2019 and 15th December in 2021. The total number of respondents who successfully completed the survey in 2019 and both surveys in 2019 and 2021 was 6,956 and 3,115 (follow-up rate 44.8%), respectively. Each respondent was interviewed in person by the research team. Responses of the respondents were recorded in a tablet computer, and then uploaded to Qualtrics when an Internet connection was available.
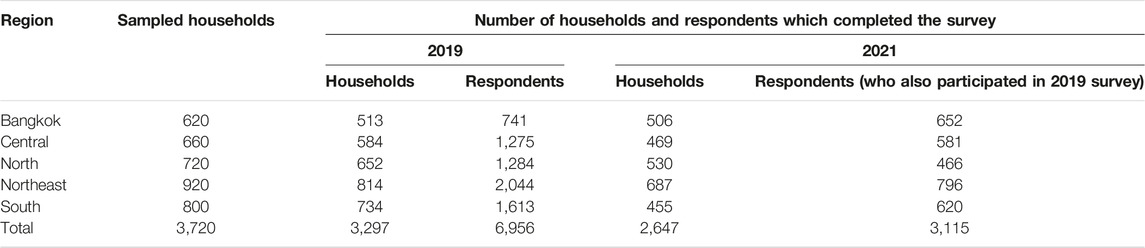
TABLE 1. Number of sampled households and respondents in 2019 and 2021 (Thailand, 2019 and 2021).
Measurement
The study questionnaires used in 2019 and 2021 include questions on demographic and economic characteristics, life satisfaction and health-related factors (available in Supplementary Information).
Study Variables
Life Satisfaction
This study used life satisfaction score as the outcome variable to measure life satisfaction among the Thai population before and during the COVID-19 epidemic. The study applied the Scale with Life Satisfaction (SWLS) instrument, developed by Diener and colleagues [19] which codes life satisfaction across a 7-level scale. The SWLS has been proven as a valid and reliable tool, and it is widely used in many countries and in diverse populations. This study used the Thai-language version of the SWLS which is available at https://eddiener.com/scales/7. The tool was assessed for an internal consistency and reliability using Cronbach’s alpha prior to data collection. The alpha value of the Thai SWLS is reported elsewhere [20].
Life satisfaction was measured by response to following statements: 1) In most ways my life is close to ideal; 2) The conditions of my life are excellent; 3) I am satisfied with my life; 4) So far, I have gotten the important things I want out of life; and 5) If I could live my life over, I would change almost nothing.
The individual respondent was asked to specify their level of agreement with each statement on a seven-point scale: 1) Strongly disagree; 2) Disagree; 3) Slightly disagree; 4) Neither agree nor disagree; 5) Slightly agree; 6) Agree; and 7) Strongly agree. Each statement was assigned one to seven points. The respondent’s score is the sum of the level of agreement with the five statements, generating a potential range from 5 to 35 points. A higher score indicates a higher level of life satisfaction.
Demographic and Economic Characteristics
This study used demographic and economic characteristics as independent variables. Demographic and economic variables are sex, age, marital status, place of residence, education, employment status, and income. The study used the latest demographic and economic data on sex, age, place of residence, and education in 2021, and the data from 2019 to 2021 for changes in marital status, place of residence, and job status. This is because previous literature reported significant changes in marital status, employment status, and income during the COVID-19 epidemic [21–23]. Details of each variable in the analysis are described below.
Sex was coded as male or female.
Age was coded according to age classification of the system of the National Statistical Office (NSO). The study classified age into four groups: Early-working age (15–29 years); middle-working age (30–44 years); late-working age (45–59 years); and older person (60 years or older).
Place of residence was coded as rural or urban.
Educational attainment was coded as completing primary school education or lower; completing secondary school education or equivalent; and completing a Bachelor’s degree or higher.
Marital status was coded for the respondent’s status before and during COVID-19 as follows: single/single; single/married; married/married; married/widowed; divorced, separated, widowed, divorced, or separated/widowed; and divorced or separated, widowed, divorced or separated/married.
Employment status was coded for a respondent’s status in 2019 and 2021 as follows: unemployed/unemployed, employed/employed, employed/unemployed, and unemployed/employed.
Income was coded for change in the respondent’s monthly income before and during COVID-19: more income; less income; and same income.
Health-Related Factors
Health status, physical activity and fruit and vegetable consumption were included in the analysis.
For the health status variable, each respondent was asked to self-assess his or her personal health status. For example, the respondent was asked if they currently had a chronic disease(s), and response was coded either “yes” or “no.” Health status was coded for the period before and during the COVID-19 epidemic as follows: yes/yes, no/yes, yes/no, and no/no.
For physical activity variable, respondents were assessed whether they achieved a sufficient level of physical activity per day with the following question: “Do you engage in physical activity for at least 30 min per day and at least 3 days per week (i.e., totalling 210 min a week of moderate intensity activity, e.g., brisk walking, running, aerobics, competitive games, and sports)?” Response was coded “yes” or “no.” Physical activity was coded for the period before and during the COVID-19 as follows: insufficient/insufficient, sufficient/insufficient, insufficient/sufficient and sufficient/sufficient.
For fruit and vegetable consumption, respondents were asked the following questions:
1. “Did you eat the following fruits/vegetables in the past week?”
2. ‘If yes, how many days did you eat them per week?”
3. “How many times a day did you eat them?”
4. “How much is the average daily amount (in rice ladle unit) of your consumption of each fruit/vegetable group?”
After completing the last question, the average daily amount reported was converted into number of grams based on the standard serving adapted from the Thailand Nutrition Flag [24]. Responses from Questions #2–4 were then calculated for average consumption per person (grams per day) of fruits and vegetables combined, by multiplying all answers from these questions and then dividing by seven.
Accordingly, each respondent was categorised into two groups: “Sufficient consumption (eating at least 400 g of fruits/vegetables combined per day [25])” and “Insufficient consumption (eating less than 400 g of fruits/vegetables combined per day).”
The fruit and vegetable consumption variable was coded for the data reported before and during the COVID-19 epidemic as follows: insufficient/insufficient, sufficient/insufficient, insufficient/sufficient and sufficient/sufficient.
Statistical Analysis
This study analysed the population-representative survey data in 2019 and 2021 to determine individual levels of life satisfaction, and associations between life satisfaction and the independent variables. The study measured the levels of life satisfaction using descriptive statistics (frequency and percentage), and the relationship between independent variables and life satisfaction in 2021 using ANOVA. The multiple regression analysis was also employed to analyse the association between life satisfaction during the COVID-19 and each of the independent variables, adjusting for the covariates sequentially, controlling for life satisfaction before the COVID-19.
The dependent variable of the analysis was life satisfaction. The independent variables in the multiple regression equation were age, gender, marital status, place of residence, education, employment, income, health status, physical activity and fruit & vegetable consumption. Any relationship with a p-value of 0.05 or less (2-tailed) was considered statistically significant. All analyses were performed with SPSS Statistics Version 18.
Results
Life Satisfaction Levels
An average life satisfaction score during the COVID-19 epidemic (in 2021) was 22.4 which decreased from 25.5 before the COVID-19 epidemic (in 2019) (Table 2). Life satisfaction scores were divided into two groups: 1) Less life satisfaction (scores 5–20); and 2) More life satisfaction (scores 21–35) [26]. Of the total 3,115 respondents, 36.5% reported having less life satisfaction during the epidemic, which was nearly 20 percentage points higher than before the epidemic (17.7%).

TABLE 2. Mean and median scores of life satisfaction of the Thai population before and during the COVID-19 epidemic (N = 3,115) (Thailand, 2019 and 2021).
Table 3 presents general characteristics of the respondents, and distributions and changes (in brackets) in life satisfaction scores before and during the COVID-19 epidemic. Respondents who were female (−3.2), were age 15–29 years (−3.7), lived in an urban area (−3.4), and attained secondary school education or equivalent (−3.3) had the greatest decrease in life satisfaction compared with other groups. Respondents who had status changes before and during the epidemic in terms of marital status (from being widowed, divorced or separated to married) (−3.7), employment status (from being employed to unemployed) (−3.7), and income status (to less income) (−3.5) had the greatest decrease in life satisfaction.
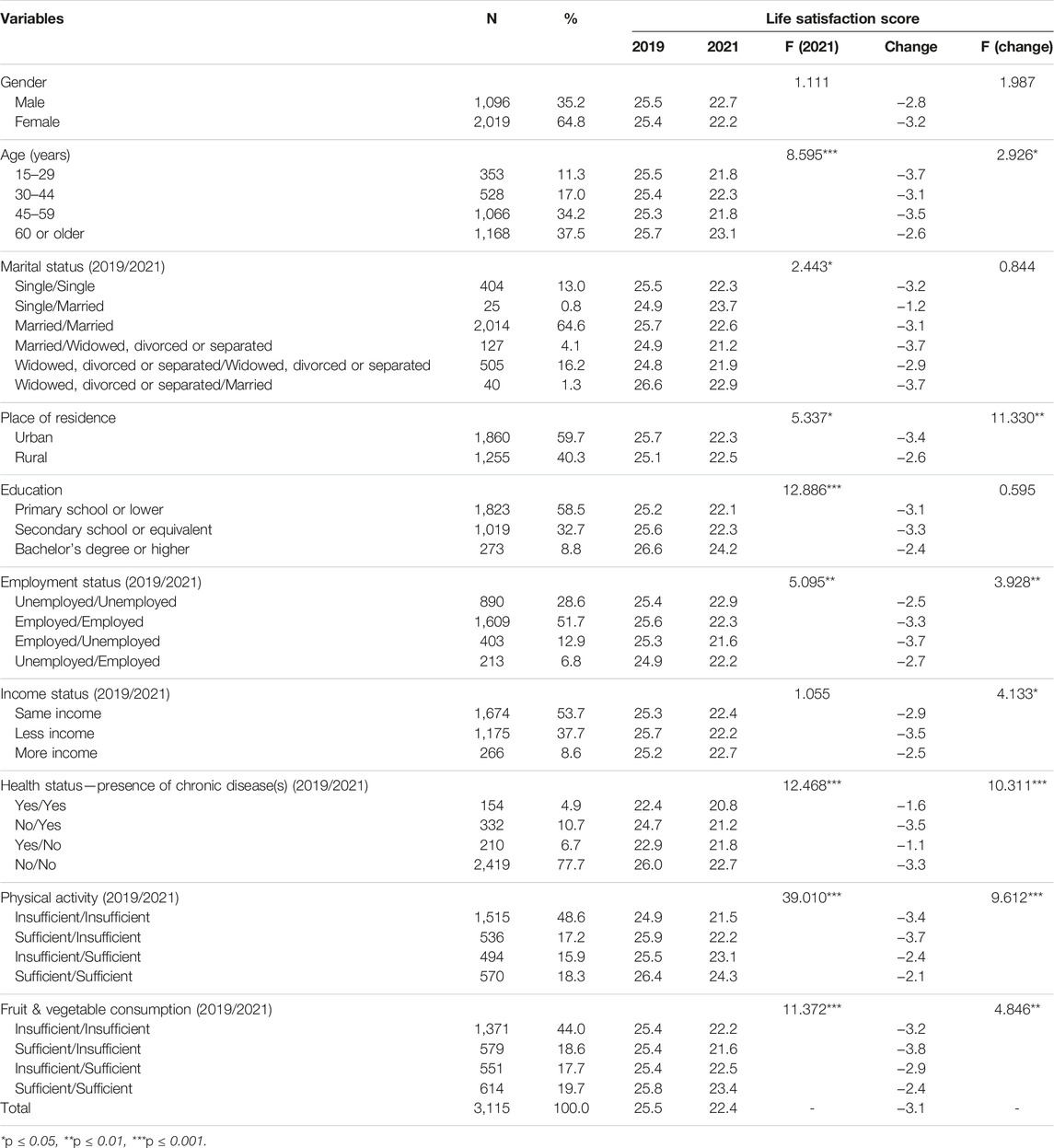
TABLE 3. Distribution and change in mean score of life satisfaction before and during the COVID-19 epidemic (N = 3,115) (Thailand, 2019 and 2021).
Some changes in life satisfaction scores were observed in health–related variables. Greatest changes were reported by respondents living with no chronic disease before the epidemic to living with a chronic disease during the epidemic (−3.5), from having sufficient physical activity before the epidemic to having insufficient physical activity during the epidemic (−3.7), and from having sufficient fruit and vegetable consumption before the epidemic to having insufficient fruit and vegetable consumption during the epidemic (−3.8).
Multiple Regression of Life Satisfaction by Sociodemographic and Socioeconomic Characteristics and Health-Related Factors
Table 4 presents results of the regression analysis of associations between life satisfaction during the COVID-19 and demographic and economic characteristics and health-related factors, controlled by life satisfaction in 2019, before the Thai COVID-19 epidemic.

TABLE 4. Multiple regression of life satisfaction by demographic and economic characteristics and health-related factors (N = 3,115) (Thailand, 2019 and 2021).
Level of life satisfaction in 2021 was strongly associated with level of life satisfaction in 2019 (β = 0.209; p ≤ 0.001). There were significant associations between life satisfaction and some demographic characteristics, i.e., age, place of residence, and education. Respondents who were at age 60 years or older (β = 0.212; p ≤ 0.001), resided in a rural area (β = 0.042; p ≤ 0.05), and had at Bachelor’s degree or higher (β = 0.091; p ≤ 0.001) were more likely to have higher life satisfaction.
For other economic factors, changes in employment status were found to be significantly associated with life satisfaction. Respondents who were still employed (β = −0.082; p ≤ 0.01), lost their job (β = −0.062; p ≤ 0.01), or got hired (β = −0.050; p ≤ 0.05) during the epidemic were more likely to have lower life satisfaction than those who were jobless during the epidemic. Respondents who earned less income during the epidemic had lower life satisfaction (β = −0.058; p ≤ 0.05).
Considering other health-related factors, respondents living with no chronic disease before and during the epidemic were more likely to have higher life satisfaction (β = 0.089; p ≤ 0.01) than other groups. Respondents who had sufficient levels (daily) of physical activity and fruit and vegetable consumption before and during the epidemic were more likely to have higher life satisfaction (β = 0.146; p ≤ 0.001 and β = 0.059; p ≤ 0.01, respectively) than other groups.
Discussion
This study drew upon longitudinal data from a nationally-representative sample of the Thai population to examine contributing factors associated with life satisfaction during the COVID-19 epidemic. This study is the first investigation to compare life satisfaction score and associated factors during the COVID-19 epidemic in Thailand and in the group of lower- and middle-income countries in Asia. The study identified potential predictors of life satisfaction, and suggests that wellbeing is influenced by a number of sociodemographic and health-related factors.
This study highlights a number of key findings from the multiple regression analysis. First, people who reported having life satisfaction before the epidemic remained satisfied with their life during the epidemic. This is not surprising since people with a positive disposition toward life in general may be more resilient in coping with adversity that may arise. In addition, older persons were more likely to have higher life satisfaction than their younger counterparts. This finding is consistent with a previous study in South Korea which found that people age 60 years or older were less dissatisfied with their life than people age 19 and 29 years [27]. This finding can be explained, perhaps, by the older generation’s accumulation of experience and having had more time to develop a lifestyle which helps them cope. Moreover, Thailand has social welfare and health services for older persons, such as long-term care insurance under the Universal Health Coverage scheme, a state pension for retirees from the Social Security Fund, pensions for retired government civil servants, and a National Savings Fund, and a minimal monthly old-age allowance for everyone else which increases with age. These safety nets can help ease the financial burden and improve daily life for senior citizens. This finding also suggests that there is ample opportunity for intergenerational activities that can bring the younger and older generations together to interact, and where older persons can transmit their life experience and lessons learned to the next generation to help them acquire coping skills and strategies to improve life satisfaction.
Other factors affecting life satisfaction include residential area and employment status. People living in an urban area tend to have lower life satisfaction than those living in a rural area. This finding is consistent with previous studies for other countries, in that, people living in cities were more dissatisfied or less satisfied with their life than those living in towns and villages [27–29]. This might be a function of the harsher COVID-19 containment measures and travel restrictions, and mandates for social distancing which are more enforced and harder to comply with in more densely-populated areas of the country. The forced isolation in cities limits social interaction among family, friends, and acquaintances more than it would in a village, all of which erodes life satisfaction.
Changes in employment status also impacted on life satisfaction of Thai population during the COVID-19. A striking finding in the present study is that people who became employed (being jobless before COVID-19) or continued to work during the epidemic had lower life satisfaction compared with people who remained jobless before and during the epidemic. This could be explained by the fact that the invisible, airborne transmission of a lethal pathogen is more threatening to workers in jobs which require them to interact with strangers or many other co-workers. This is particularly true for frontline jobs which are in a physical workplace and in proximity of a constant flow of people who might be carriers of COVID-19. Thus, these types of workers were in high demand during COVID-19, especially healthcare workers, cashiers, personal care workers, food processing workers, construction workers, and assembly workers, among many other types. These workers were, thus, at risk by being employed. Many of these jobs are also concentrated among the young, lower-educated, migrants, ethnic minorities, and other low-skilled workers in minimum-wage jobs. The work itself is stressful even without an epidemic, and the threat of COVID-19 certainly increased the stress and anxiety significantly for these vulnerable members of the labour force [30]. At the same time, the people who lost full-time work during the epidemic had an immediate negative impact on their ability to make ends meet, since many of these workers probably had limited or no savings, and little options for alternative work. Thus, sudden unemployment would certainly erode satisfaction with their life. In particular, the young, lower-educated, migrants, racial/ethnic minorities, and low-skilled workers were at a higher risk of job loss and were expected to recover more slowly than other population groups [31].
This study found an association between income loss and lower life satisfaction, and that is consistent with a previous study [32]. During the COVID-19 epidemic, a wide range of government responses to mitigate and suppress spread of the virus were implemented, which included school closures, travel restrictions, bans on public gatherings, stay-at-home orders, and severe reduction of public transportation [33]. These restrictions unavoidably imposed high social and economic costs on people, especially putting them at higher risk of income loss through working-hour reductions or job termination [30]. Together with differences in household structures and inequalities in access to savings, workers from vulnerable and minority groups and migrants were found to be hit hardest by the containment measures, since they were already living at the margins of the society and economy, and could ill-afford any shocks such as an epidemic [34]. This negative employment change can lead workers in at-risk jobs to suffer particularly large losses in income, and thus erasing any life satisfaction they may have felt before the epidemic.
This study identified other sources of life satisfaction, such as health status and lifestyle behaviours. People who can maintain a healthy lifestyle—living without chronic disease and meeting a sufficient level of physical activity and fruit and vegetable intake reported that the epidemic actually had a positive impact on life satisfaction. The WHO addressed the significant challenge for healthy individuals during stay-at-home restrictions as what they ate, drank, and level of physical activity. Those adaptations are key predictors in a person’s ability to prevent and recover from COVID-19 infection [35, 36]. Unhealthy diet and low levels of physical activity can have negative effects on individual health, mental health, and overall wellbeing. Thus, WHO strongly recommends that individuals remain eating a healthy diet and being physically active during the COVID-related restrictions, as they are essential to avert other health problems, including obesity and noncommunicable diseases or other debilitating conditions. Healthy behaviour maintenance and improvement in Thai wellbeing during the epidemic are possibly the effect of continued implementation of public education campaigns by the government, i.e., to promote a healthy, balanced lifestyle including regular physical activity and nutritious diet to boost the immune system against COVID-19. The findings from this study confirm the importance of resilience among a population during the epidemic through maintaining a heathy lifestyle. More government attention should be given to building resilience at the individual and household levels so that Thais can adapt to difficult or challenging life experiences under uncertain circumstances or sudden adversity they may face.
This study has some limitations. First, data collection used an interviewed questionnaire which relies on an individual’s ability to remember their past experience, i.e., daily levels of physical activity and fruit and vegetable intake, may affect estimates and calculation of such behaviours in the sample. Recall bias could cause an overestimate or underestimate of the various indicators and variables. Measurement of life satisfaction is also reliant on self-reports and is rather subjective it its own right. Thus, the life satisfaction ratings are subject to recall bias and whether a person has an optimistic or pessimistic disposition in general. However, the measurement used in this study has been proved to be valid in various contexts, and has been widely used in examining life satisfaction in various groups of populations and countries with different income levels. That said, this study did not include other variables that may influence life satisfaction, such as exposure to COVID-19, personal and social contact and support, and living conditions [9, 37, 38]. The study also did not analyse differences in life satisfaction and its predictors based on household. Further research should explore the influence of other factors on an individual’s life satisfaction, and conduct a household-level analysis.
Another limitation involves loss to follow-up which is usually a limitation of longitudinal studies. This can lead to attrition bias which can affect the validity and reliability of the study findings. There are significant challenges associated with following participants during the Thai COVID-19 epidemic. For example, fears of the COVID-19, COVID-19 infection and high risk of getting infection can lead to dropping out of the study. Therefore, strategic follow-up plan that can enhance study retention and minimise attrition bias is needed in the future. This can include frequent contact with participants and secondary contacts (i.e., a village leader), creation of connections with relevant local government offices, and complementary to other existing relevant datasets which can strengthen the validity of the study findings.
Policy Implications
The findings suggest that it is important for the government to address root causes of the demographic and economic disparities, which contribute to persistent structural disadvantages and, thus, negative mental wellbeing faced by groups of the population, but especially vulnerable and marginalised. The government should give priority to building resilience and social protection systems for empowering individuals to cope with crises and shocks, improve productivity, improve health, and improve education outcomes. People need to seek opportunity to lift themselves and their families out of adversity and toward a better life [39]. Well-designed and targeted policies for resilience and social protection can promote self-reliance or self-sufficiency of individuals to meet essential needs or attain an acceptable level of functioning in daily life [40, 41]. Ultimately the goal is to promote greater equity, improve human capital and stimulate economic growth. Social protection has also become a global priority as a key factor in accelerating progress towards the Social Development Goals (SDG) especially SDGs 1.3, 3.8 and 8.b [41]. Accordingly, public sector investment for improving resilience and social protection policies are urgently needed. These assets are important for building adaptive capacity of individuals and households. Finally, the government needs to consider fiscal measures (e.g., taxes, social transfers) to increase universal social protection and ensuring sustainable domestic financing.
Conclusion
This study identified a significant association between life satisfaction and various demographic, economic and health-related variables. Changes in employment status and income were found to predict greater challenge in maintaining life satisfaction. This is probably attributable to their limited savings and weak social safety net during the epidemic. Lifestyle changes which led to insufficient physical activity and reduced fruit and vegetable intake had an adverse effect on level of life satisfaction. That change made it more difficult for people to cope with daily life during the epidemic. These findings suggest that policies and strategies which address the root causes of the sociodemographic and socioeconomic disparities and lifestyle changes in the Thai population are needed. Specific recommended actions include building resilience and social protection systems to empower individuals—especially the poor and vulnerable—to cope with a crisis, improve health and wellbeing outcomes, and seek opportunity to lift themselves and their families out of adversity toward a better life.
Ethics Statement
The studies involving human participants were reviewed and approved by the Institutional Review Board of the Institute for Population and Social Research of Mahidol University. Written informed consent to participate in this study was provided by the participants or parent/guardian if the participant is under 18 years of age.
Author Contributions
SP: Conceptualization, Formal analysis, Funding Acquisition, Investigation, Methodology, Project administration, Visualization, Writing—Original Draft Preparation, Writing—review and editing. ST: Formal analysis, Investigation, Methodology, Writing—review and editing. AC: Conceptualization, Methodology, Writing—review and editing. RG: Conceptualization, Methodology, Writing—review and editing. UP: Conceptualization, Methodology, Writing—review and editing, CU: Writing—review and editing. PS: Writing—review and editing.
Funding
This research was funded by Thai Health Promotion Foundation (Grant # 62-00-0837 and 64-00-0020).
Conflict of Interest
CU and PS declare that they are serving as a steering committee and a Division Director of the Thai Health Promotion Foundation, respectively.
The remaining authors declare that they do not have any conflicts of interest.
Acknowledgments
The authors gratefully acknowledge the survey participants for taking the time to complete the questionnaire survey, and the field staff who untiringly contributed to data collection and completion of the study. The authors would also like to thank the National Statistical Office for constructive comments and assistance during survey sampling and data analysis, and the Institute for Population and Social Research at Mahidol University for administrative and logistical support.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.ssph-journal.org/articles/10.3389/ijph.2023.1605483/full#supplementary-material
SUPPLEMENTARY FILE S1 | The 2019 Survey questionnaire.
References
1. Evans, S, Mikocka-Walus, A, Klas, A, Olive, L, Sciberras, E, Karantzas, G, et al. From “It Has Stopped Our Lives” to “Spending More Time Together Has Strengthened Bonds”: The varied experiences Aust families during COVID-19. Front Psycho (2020) 11:588667. doi:10.3389/fpsyg.2020.588667
2. Praveena, SM, and Aris, AZ. The Impacts of COVID-19 on the Environmental Sustainability: a Perspective from the Southeast Asian Region. Environ Sci Pollut Res (2021) 28(45):63829–36. doi:10.1007/s11356-020-11774-0
3. Le, K, and Nguyen, M. The Psychological Consequences of COVID-19 Lockdowns. Int Rev Appl Econ (2021) 35(2):147–63. doi:10.1080/02692171.2020.1853077
4. Rissanen, T, Viinamäki, H, Honkalampi, K, Lehto, SM, Hintikka, J, Saharinen, T, et al. Long Term Life Dissatisfaction and Subsequent Major Depressive Disorder and Poor Mental Health. BMC psychiatry (2011) 11:140. doi:10.1186/1471-244X-11-140
5. Fergusson, DM, McLeod, GF, Horwood, LJ, Swain, NR, Chapple, S, and Poulton, R. Life Satisfaction and Mental Health Problems (18 to 35 Years). Psychol Med (2015) 45(11):2427–36. doi:10.1017/S0033291715000422
6. Diener, E, Pressman, SD, Hunter, J, and Delgadillo-Chase, D. If, Why, and when Subjective Well-Being Influences Health, and Future Needed Research. Appl Psychol Health well-being (2017) 9(2):133–67. doi:10.1111/aphw.12090
7. Richards, M, and Huppert, FA. Do positive Children Become Positive Adults? Evidence from a Longitudinal Birth Cohort Study. J positive Psychol (2011) 6(1):75–87. doi:10.1080/17439760.2011.536655
8. Bachmann, R, Gonschor, M, Korfhage, T, and Wübker, A. Covid-19 and Life Satisfaction across Europe. Appl Econ Lett (2023) 30(5):635–9. doi:10.1080/13504851.2021.2005766
9. Rogowska, AM, Ochnik, D, Kuśnierz, C, Jakubiak, M, Schütz, A, Held, MJ, et al. Satisfaction with Life Among university Students from Nine Countries: Cross-National Study during the First Wave of COVID-19 Pandemic. BMC Public Health (2021) 21(1):2262. doi:10.1186/s12889-021-12288-1
10. Dymecka, J, Gerymski, R, Machnik-Czerwik, A, Derbis, R, and Bidzan, M. Fear of COVID-19 and Life Satisfaction: The Role of the Health-Related Hardiness and Sense of Coherence. Front Psychiatry (2021) 12:712103. doi:10.3389/fpsyt.2021.712103
11. Rajatanavin, N, Tuangratananon, T, Suphanchaimat, R, and Tangcharoensathien, V. Responding to the COVID-19 Second Wave in Thailand by Diversifying and Adapting Lessons from the First Wave. BMJ Glob Health (2021) 6(7):e006178. doi:10.1136/bmjgh-2021-006178
12. Jiang, N, Yan-Li, S, Pamanee, K, and Sriyanto, J. Depression, Anxiety, and Stress during the COVID-19 Pandemic: Comparison among higher Educ students four countries Asia-Pacific Region. Journal of Population and Social Studies (2021) 29: 370-383. doi:10.25133/JPSSv292021.023
13. Tiaprapong, K, Sirikul, A, Krajangmek, C, Duangthongkul, N, Pandam, N, and Piya-Amornphan, N. Awareness of COVID-19 Influences on the Wellness of Thai Health Professional Students: An Ambulatory Assessment during the Early "new normal" Informing Policy. PloS one (2021) 16:e0252681. doi:10.1371/journal.pone.0252681
14. Chinvararak, C, Kerdcharoen, N, Pruttithavorn, W, Polruamngern, N, Asawaroekwisoot, T, Munsukpol, W, et al. Mental Health Among Healthcare Workers during COVID-19 Pandemic in Thailand. PloS one (2022) 17:e0268704. doi:10.1371/journal.pone.0268704
15.UNFPA. COVID-19 and Older Persons: Evidence from the Survey in Thailand. Bangkok: United Nations Population Fund and College of Population Studies, Chulalongkorn University (2021).
16. Bui, D, Dräger, L, Hayo, B, and Nghiem, G. The Effects of Fiscal Policy on Households during the COVID-19 Pandemic: Evidence from Thailand and Vietnam. World Dev (2022) 153:105828. doi:10.1016/j.worlddev.2022.105828
17. Knapp, M, McDaid, D, and Parsonage, M. Mental health promotion and mental illness prevention: The economic case. London: Personal Social Services Research Unit, London School of Economics and Political Science (2011).
18. Deaton, A. Income, Health, and Well-Being Around the World: Evidence from the Gallup World Poll. J Econ Perspect (2008) 22(2):53–72. doi:10.1257/jep.22.2.53
19. Diener, E, Emmons, R, Larsen, R, and Griffin, S. The Satisfaction with Life Scale. J Pers Assess (1985) 49:71–5. doi:10.1207/s15327752jpa4901_13
20. Phulkerd, S, Thapsuwan, S, Chamratrithirong, A, and Gray, RS. Influence of Healthy Lifestyle Behaviors on Life Satisfaction in the Aging Population of Thailand: a National Population-Based Survey. BMC Public Health (2021) 21(1):43. doi:10.1186/s12889-020-10032-9
21. Peng, J, Wu, WH, Doolan, G, Choudhury, N, Mehta, P, Khatun, A, et al. Marital Status and Gender Differences as Key Determinants of Covid-19 Impact on Wellbeing, Job Satisfaction and Resilience in Health Care Workers and Staff Working in Academia in the UK during the First Wave of the Pandemic. Front Public Health (2022) 10:928107. doi:10.3389/fpubh.2022.928107
22. Carotta, CL, Lavender-Stott, ES, Garcia, AS, and Liu, H-L. Relationship Status and Well-Being in the Context of the COVID-19 Pandemic. J Fam Issues (2022) 0 (0):1–20. doi:10.1177/0192513x221105242
23. Eø, C, Caspersen, IH, Ask, H, Brandlistuen, RE, Trogstad, L, and Magnus, P. Association between Work Situation and Life Satisfaction during the COVID-19 Pandemic: Prospective Cohort Study in Norway. BMJ open (2022) 14:(4). e049586. doi:10.1136/bmjopen-2021-049586
24.Bureau of Nutrition. Healthy Eating Guideline. Thailand: Nonthaburi: Department of Health, Ministry of Public Health Thailand (2007).
25.World Health Organization. Fruit and Vegetables for Health: Report of a Joint FAO/WHO Workshop. Kobe, Japan: World Health Organization (2004).
26. Pavot, WG, and Diener, E. Review of the Satisfaction with Life Scale. Psychol Assess (1993) 5:164–72. doi:10.1037/1040-3590.5.2.164
27. Byeon, H. Influence of the COVID-19 Pandemic on the Subjective Life Satisfaction of South Korean Adults: Bayesian Nomogram Approach. Bayesian Nomogram Approach (2022) 12(3):761. doi:10.3390/diagnostics12030761
28. Gonzalez-Bernal, JJ, Rodríguez-Fernández, P, Santamaría-Peláez, M, González-Santos, J, León-Del-Barco, B, Minguez, LA, et al. Life Satisfaction during Forced Social Distancing and home Confinement Derived from the COVID-19 Pandemic in Spain. Int J Environ Res Public Health (2021) 18:1474. doi:10.3390/ijerph18041474
29. Brogårdh, C, Hammarlund, CS, Eek, F, Stigmar, K, Lindgren, I, Schouenborg, AT, et al. Self-perceived Life Satisfaction during the First Wave of the COVID-19 Pandemic in Sweden: A Cross-Sectional Study. Int J Environ Res Public Health (2021) 18(12):6234. doi:10.3390/ijerph18126234
30.OECD. OECD Policy Responses to Coronavirus (COVID-19). The Unequal Impact of COVID-19: A Spotlight on Frontline Workers, Migrants and Racial/ethnic Minorities. Paris: Organisation for Economic Co-operation and Development (2022).
31.OECD. The Unequal Impact of COVID-19: A Spotlight on Frontline Workers, Migrants and Racial/ethnic Minorities. Paris: Organisation for Economic Co-operation and Development (2022).
32. Cheng, TC, Kim, S, and Koh, K. The Impact of COVID-19 on Subjective Well-Being: Evidence from Singapore. Bonn, Germany: The IZA - Institute of Labor Economics (2020).
33.Internaitonal Monetary Fund. Policy Responses to COVID-19 (2022). Available from: https://www.imf.org/en/Topics/imf-and-covid19/Policy-Responses-to-COVID-19#T (Accessed July 11, 2022).
34. Platt, L, and Warwick, R. COVID-19 and Ethnic Inequalities in England and Wales*. Fiscal Stud (2020) 41(2):259–89. doi:10.1111/1475-5890.12228
35.WHO. #HealthyAtHome: Healthy Diet Geneva: World Health Organization (2022). Available at: https://www.who.int/campaigns/connecting-the-worldto-combat-coronavirus/healthyathome/healthyathome–healthy-diet (Accessed July 26, 2022).
36.Europe WHO. Stay Physically Active during Self-Quarantin. Copenhagen: World Health Organization Regional Office for Europe (2022). Available from: https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/publications-and-technical-guidance/noncommunicable-diseases/stay-physically-active-during-self-quarantine (Accessed July 26, 2022).
37. Lim, C, and Putnam, RD. Religion, Social Networks, and Life Satisfaction. Am Sociological Rev (2010) 75(6):914–33. doi:10.1177/0003122410386686
38. Sujarwoto, S, Tampubolon, G, and Pierewan, AC. Individual and Contextual Factors of Happiness and Life Satisfaction in a Low Middle Income Country. Appl Res Qual Life (2018) 13(4):927–45. doi:10.1007/s11482-017-9567-y
39.World Bank Group. Resilience, Equity, and Opportunity: The World Bank's Social protection and Labor Strategy 2012-2022 (English). Washington, DC: World Bank Group (2012).
40.IOM. Social protection – an Operational Tool for the Humanitarian, Development and Peace Nexus: Linkages between Cash-Based Interventions and Social protection in Humanitarian and Non-humanitarian Settings. Cairo: International Organization for Migration IOM (2022).
Keywords: COVID-19, sociodemographic factors, healthy lifestyle, life satisfaction, socioeconomic factors, Thailand
Citation: Phulkerd S, Thapsuwan S, Soottipong Gray R, Chamratrithirong A, Pattaravanich U, Ungchusak C and Saonuam P (2023) Life Satisfaction Before and During COVID-19 Pandemic in Thailand. Int J Public Health 68:1605483. doi: 10.3389/ijph.2023.1605483
Received: 13 October 2022; Accepted: 29 June 2023;
Published: 13 July 2023.
Edited by:
Olaf von dem Knesebeck, University Medical Center Hamburg-Eppendorf, GermanyReviewed by:
Adekunle Adedeji, Hamburg University of Applied Sciences, GermanyLuiz Alexandre Chisini, Federal University of Pelotas, Brazil
Copyright © 2023 Phulkerd, Thapsuwan, Soottipong Gray, Chamratrithirong, Pattaravanich, Ungchusak and Saonuam. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sirinya Phulkerd, c2lyaW55YS5waHVAbWFoaWRvbC5hYy50aA==
†ORCID: Sirinya Phulkerd, orcid.org/0000-0001-9373-3120; Sasinee Thapsuwan, orcid.org/0000-0002-7967-2779; Rossarin Soottipong Gray, orcid.org/0000-0002-9877-8253; Aphichat Chamratrithirong, orcid.org/0000-0001-5094-8770; Umaporn Pattaravanich, orcid.org/0000-0002-3750-9172; Pairoj Saonuam, orcid.org/0000-0002-5601-8782