 Herney Rengifo-Reina1
Herney Rengifo-Reina1 Tonatiuh Barrientos-Gutiérrez1*Nancy López-Olmedo1Brisa N. Sánchez2Ana V. Diez Roux3
Tonatiuh Barrientos-Gutiérrez1*Nancy López-Olmedo1Brisa N. Sánchez2Ana V. Diez Roux3- 1Center for Population Health Research, National Institute of Public Health (Mexico), Cuernavaca, Mexico
- 2Department of Epidemiology and Biostatistics, Drexel University, Philadelphia, PA, United States
- 3Urban Health Collaborative, Dornsife School of Public Health, Drexel University, Philadelphia, PA, United States
Objective: We investigated the association between the density of internal human migration, in the urban neighborhood, on frailty in the older adult population in Colombia.
Methods: The data used in this study are from four Colombian population surveys. We analyzed 633 census tracts with a sample of 2,194 adults 60 years and over for frailty (measured using the Fried criteria). We considered the proportion of inhabitants in a census tract with a history of internal migration as the exposure variable considering three temporalities. For contextual forced migration, we identified two types: 5-year, and 1-year. Poisson multivariable regression models with two hierarchical levels (individual and census tracts) were estimated.
Results: The prevalence of pre-fragile/frailty was 80.63% [CI 95%: 77.67, 83.28]. The prevalence ratio were significantly higher for the older adults who live in neighborhoods where a higher proportion of internal migrants reside.
Conclusion: We conclude that older adults who lived in neighborhoods with a high proportion of internal migrants experience more frailty. Potential explanations are that neighborhoods with high internal migration could experience social (l increase in cultural heterogeneity, in the perception of insecurity, violence and physical conditions (pressure on local economies and services, leading elderly residents to compete for neighborhood resources), translated into social stress.
Introduction
Latin American countries are experiencing an accelerated population aging process. The percentage of older adults in Latin America increased from 6% in 1965 to 11.8% in 2017 and is expected to reach 20% by 2050 (1). Colombia is in a moderately advanced aging stage, with 13.5% of its population over 60 years of age in 2020 (2); yet, its demographic transition has been fast, since in 1950 only 5% of the population had more than 60 years of age and by 2050 this percentage will be more than 23%. The acceleration of aging already poses a significant public policy and public health challenge for the country.
The elderly in Colombia are expected to experience an increase in the prevalence of non-communicable, degenerative and disabling diseases (3). Frailty is one of the most important syndromes in this age group, yet, little is known about how frailty interacts with social processes. Frailty is a biological syndrome by which biological reserve and resistance are diminished by stressors as a result of multiple physiological systems that become unbalanced (4, 5), leading to functional deterioration and adverse events that worsen health, decrease quality of life and can even cause death (6). The origin of frailty is multicausal (4, 6); however, the evidence has mainly focused on the magnitude and coexistence of individual and social care factors (7, 8) rather than contextual and neighborhood factors, such as human migration.
Colombia has experienced an important increase in internal migration, defined as a situation where a person moves within a country, outside of their usual residence (9), often related to forced migration due to conflict. More than 30% of the population in Colombia has relocated within the country in the past 3 decades (10), a third of them due to forced migration but also because of economic reasons and natural disasters (11). Human migration is a social determinant of health that can positively or negatively influence people’s health (12). Internal migration can affect an individual’s health through different pathways, including social stress and social cohesion (13).
Most of the evidence about the association between general migration and health/disease is observed in high-income countries (HICs) (14). Human migration has also been studied in African countries in the context of refugees, but most analyses have focused on the impacts on the host population around economic issues, mainly followed by the provision of public services and health, environment and infectious diseases (15). Nevertheless, it is unclear how this link is presented in Latin American Countries (LACs). Moreover, most of the studies have focused on assessing the effects of migration on migrants themselves’. However, little is known about whether contextual migration potentially impacts the host population (16–18), especially when considering older adults. In summary, the association between contextual migration as a social exposure and frailty among the elderly population in urban settings has been no been studied, as the existing literature revolves around the experience of the elderly as an international migrant, with a greater probability of frailty being observed in migrants from low-income countries (19, 20).
The large internal migration experienced by Colombia provides a unique opportunity to assess how the proportion of migration in a neighborhood influences frailty beyond the individual experience of migration. We aimed to assess the association between the proportion of people in a neighborhood who migrated within the country for forced and non-forced reasons and the prevalence of frailty in older adults in urban areas of Colombia.
Methods
Study Population
This is a cross-sectional study based on an analysis of secondary data. The data was obtained from four Colombian population surveys: Health, Wellbeing, and Aging (SABE—2015), Demography and Health (ENDS 2015), Nutritional Situation of Colombia (ENSIN 2015), and Mental Health (ENSM 2015), with a response rate of 77%, 93.4%, 85.0%, and 97.4%, respectively. The protocols and sample sizes for each survey are published elsewhere (3, 21–23). The sample design of each survey followed the guidelines of the master sample of households for health studies that was designed by the Ministry of Health and Social Protection (24). Groups of contiguous blocks of the same sector were formed and randomly sampled for each survey; thus, while surveys did not cover the same households they sampled the same census tracts. This creates an opportunity for linkage of contextual data across surveys. Based on this premise, census tracts with information on the four surveys (n = 633) were selected to represent urban neighborhoods, with a sample of 2,194 participants 60 years of age and older. This study was approved by the ethics, research, and biosecurity committee of the National Institute of Public Health of Mexico (Protocol 1183).
Outcome Variables—Frailty
We obtained information on frailty from the SABE survey (3). We defined frailty using the criteria established by Fried et al. (5): 1) Self-reported unintended weight loss in the last 3 months; 2) Measured grip strength adjusted according to gender and body mass index; 3) Self-reported physical fatigue or exhaustion; 4) Observed difficulty walking; 5) Self-reported physical activity. Participants were considered frail or pre-frail if they experienced any of the five criteria.
Individual-Level Covariates
We included individual-level social, demographic, and economic characteristics of the older adults from the SABE survey. We considered: sex, age in 5-year groups and educational level into four categories (neither, primary schooling, secondary schooling, university education). Marital status was categorized as living alone or with a partner (married, free union). Health insurance was categorized into insured (contributory regimen - formal workers and subsidized regimen—non-workers, subsidized by the government), or uninsured. We also identified if participants received a pension (yes/no). Socioeconomic position (SEP) was categorized into low, medium, and high according to the DANE classification (25). Living arrangements (with whom the participant lived) included living with a son/daughter and living with friends or caregivers. And the individual experience of migration (lifetime migrant).
Exposure Variables—Contextual Internal Migration at the Census Tracts Level
Contextual migration information was obtained from the sociodemographic questionnaires of the four surveys. We considered internal migration as the change in residence within the same country for Colombian-born participants. We identified three types of contextual internal migration: 1) lifetime: participants that resided in a place other than the one where they were born and have remained in the current residence for the past 5 years; 2) 5-year: change of residence during the previous 5 years, and 3) 1-year: change of residence during the last 12 months. For contextual forced migration (main reason for changing residence was armed conflict or insecurity), we identified two types: forced displacement during the previous 5 years and forced displacement during the last 12 months.
We formed categories of total migration based on the distribution by quintiles for each of the temporal frames (where neighborhoods with less than 1% of migrants in their structure were in the first category): lifetime, 5 years and 1 year: <1%, 1%–2%, 3%–5%, 6%–10%, and 11% or more. For people with forced migration within 5 and 1 years, the categories were: <1%, 1%–2%, and 3% and more.
Census Tract Level Covariates
At the census tract level, we included socioeconomic level (level 1: very-low to 6: high), and age distribution (proportion of people 0 to 14, 15 to 64, and 65 and over), which were obtained from the 2018 national census (26).
Although it is true that migration matrices are a fundamental tool for migration analysis, they are built from censuses and are given mainly for large administrative units of the countries (provinces and states). When performing analysis in smaller administrative units such as neighborhoods, the matrix becomes more complex due to the number of crossings and the difficulty of obtaining information at that level.
For this study, the migration matrix could not be fully structured because the information available was obtained only for people entering the neighborhood and no information was obtained for people leaving the neighborhood (data source: surveys. The census information was not available at the level of analysis). Resulting in the characterization of a type of migratory movement that of arrival of internal migrants. We are not built other types of indicators such as net migration, gross migration, among others and focusing the analysis on the migration proportions mentioned.
Statistical Analysis
The study sample was analyzed using relative frequencies with 95% confidence intervals (95% CI) for categorical variables and measures of central tendency and dispersion for continuous variables. Directed acyclic graphs (DAGs) guided our statistical analysis (Supplementary Figure S1). Weights were used to describe the population at the individual level. Because the probability of frailty is high, odds ratios could overestimate prevalence ratios, thus, the association of variables at the individual and contextual level with frailty was estimated using Poisson models with robust standard errors, which yields accurate prevalence ratio estimates (27). We started with an empty model (intercept only) and continued with the inclusion of individual-level variables (first level). The third model included contextual variables at the census tract level (second level). We modeled the probability of frailty using the following general equation:
Where Yij = 1 denotes the presence of frailty in person i in the census tract j. The variable X(ij) represents the exposure variable of interest, measured as the proportion of people in urban neighborhood j who are migrants. The vectors Zij and Zj represent covariates at the person and neighborhood level. βoj is the average of log(y) (log of the prevalence of frailty) of the jth neighborhood.
Finally, four sensitivity analyses were conducted, we excluded the population under 18 years of age from the calculation of contextual internal migration, recognizing that adult migration is generally motivated by economic, social or individual decisions, while the migration of minors usually responds to parental decisions. The second sensitivity analysis sought to describe the behavior of the frailty prevalence ratios by categorizing the exposure variable into quartiles and whether there were differences in PR with the category originally used (Supplementary Table S1). For the third, different types of individual migration history for each participant were included as an adjustment variable to reduce the potential impact of personal migration experience on the main association (Supplementary Table S2). And fourth sensitivity analysis including forced migration (both 5 years and 1 year) as an adjustment variable in the migration models. All analyses were performed with Stata version 16.0 (StataCorp LP, College Station, United States).
Results
The total sample consisted of 2,194 participants living in 633 census tracts from urban areas. Participants had a mean age of 68.5 years [CI 95%: 68.3, 68.7] and 53.8% of them [CI 95%: 49.0, 58.4] were women. Over half of the participants had a partner (53.3% [CI: 47.6, 58.8]), 8.6% did not have formal education [CI 95%: 5.7, 12.7], and 88.8% did not have the benefit of a retirement pension [CI 95%: 80.5, 93.8]. Prevalence of pre-frailty and frailty was 80.6% [CI 95%: 77.67, 83.28]. People with pre-frailty/frailty were in average 3 years older, more frequently women (56.9% [CI 95%: 52.1, 61.6]), without pension (91.0% [CI 95%: 87.1, 93.8]) and receiving a government support program (84.0% [CI 95%: 78.5, 88.3]) (Table 1).
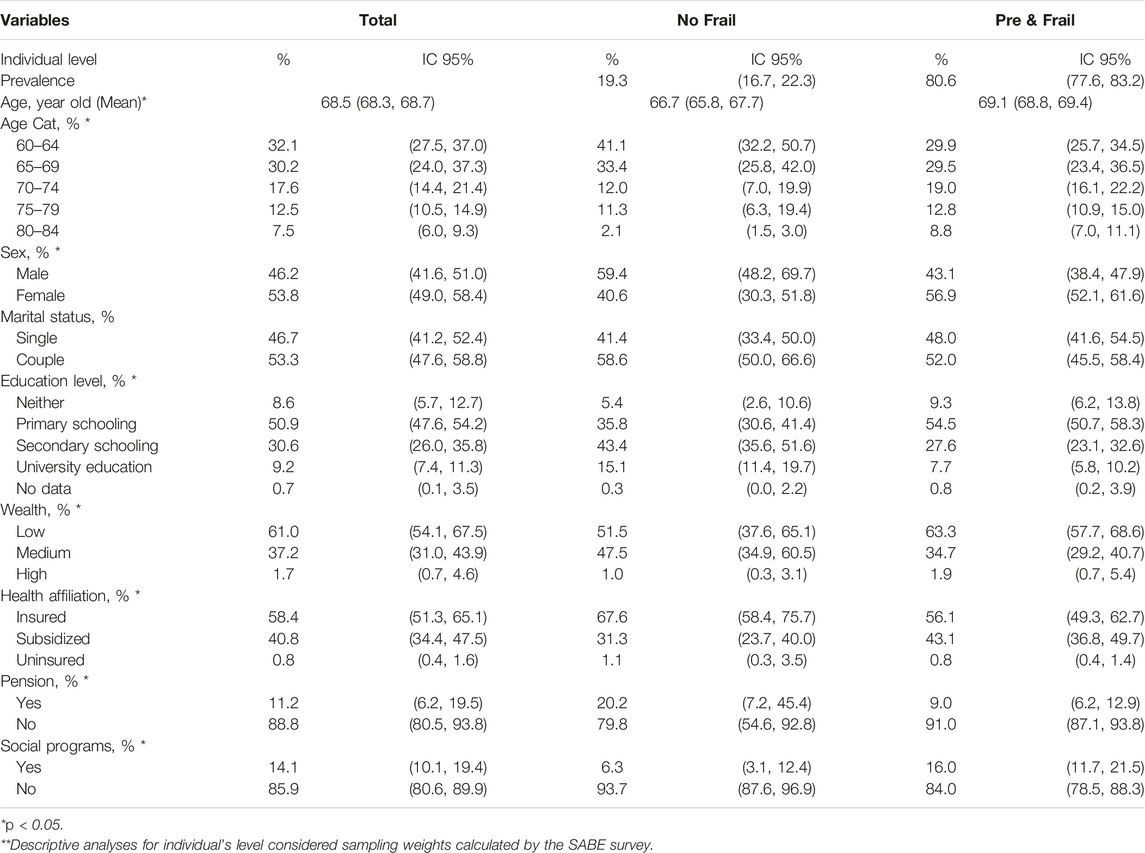
TABLE 1. Demographic and social characteristics of study population for frailty—individual level considered sampling weights**, Colombia, 2016.
Of the total census tracts, 62.7% (397) belonged to the very-low and low socioeconomic level, 31.7% (201) to the medium-low, and 5.5% (35) to medium, medium -high and high. Across census tracts, 70.1%, 19.6%, and 10.3% of people were in the 15 to 64, 0 to 14, and 65 or more years’ age group, respectively. For sex, women represented 52.4% of the population across census tracts. A total of 42 census tracts did not have frail adults. In the individual distribution, Table 2 shows that, of the total number of participants, 24.4% of older adults resided in neighborhoods with less than 1% of life migration in its residents, 17.0% in neighborhoods with less than 1% migrants of 5 years, and 20% with less than 1% migrants of 1 year. Of the frail participants, 43.8%, 46.9%, and 25.7% lived in neighborhoods with a percentage of lifetime, 5-year and 1-year migrants of 6% and higher.
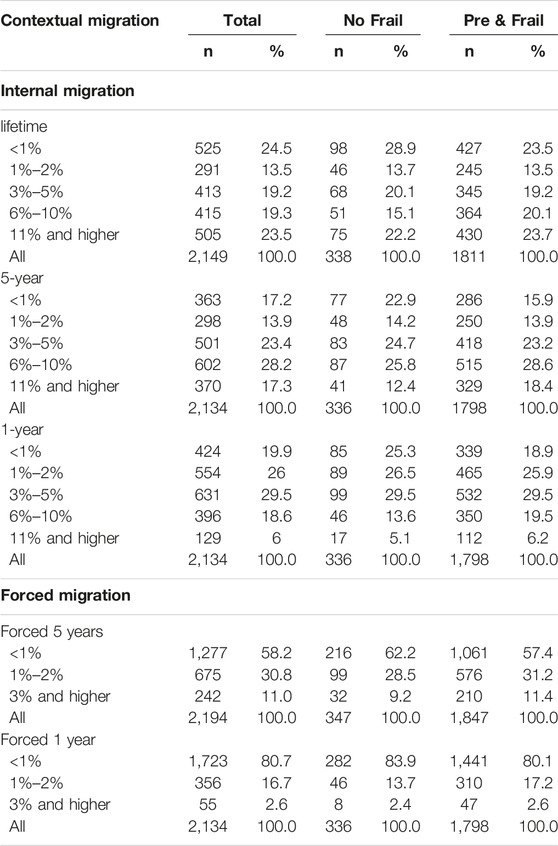
TABLE 2. Distribution of the contextual migration measures among the study sample overall and by and frailty status at the individual level, Colombia, 2016.
Figure 1 shows the prevalence of pre/frailty among older adults in neighborhoods with different levels of internal contextual migration. In neighborhoods with less than 1% migration, the prevalence of pre/frailty was up to 80% for all types of migration. The prevalence of pre/frailty increased as the percentage of migrants increased, being higher than 84% in neighborhoods with 11% or more migrants. For forced migration, the differences were not as evident as for internal contextual migration in general, but an increasing trend is observed as the percentage of migrants in the neighborhood increases.
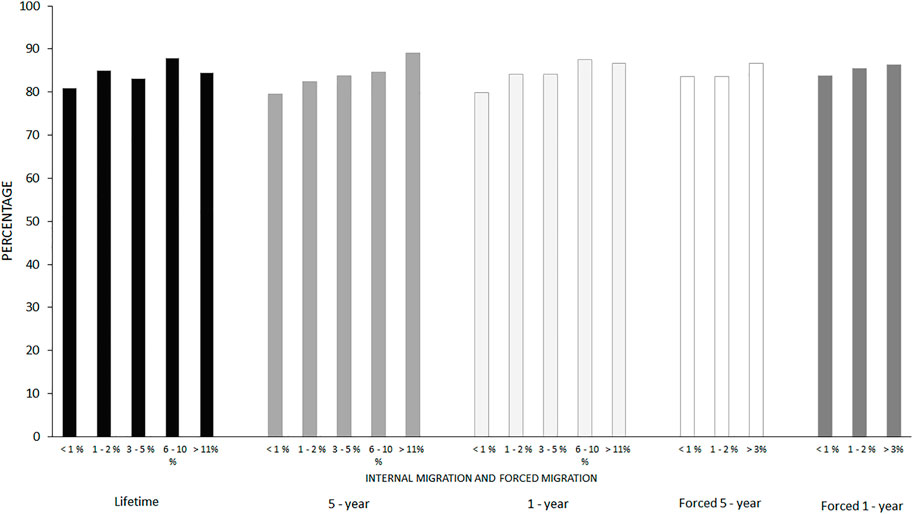
FIGURE 1. Prevalence of pre/frailty by type of migration and percentage of migrants in the neighborhood, Colombia, 2016.
Table 3 shows the results of the analysis of the association of all types of contextual internal migration with pre-frailty and frailty. The prevalence ratio of pre-frailty/frailty increases as the proportion of the migrant population in the neighborhood increases, being greater and statistically significant for participants who lived in neighborhoods with more than 6% of the migrant population in their environment. In the crude model, the prevalence ratio of pre-frailty/frailty in older adults was 1.07 (CI 95%: 1.01, 1.14), comparing neighborhoods with 6% or more contextual lifetime migrants to neighborhoods with <1% lifetime migrants. This association remained when adjusting for all the covariates considered in model 3 (PR = 1.08, CI 95%: 1.02, 1.15).
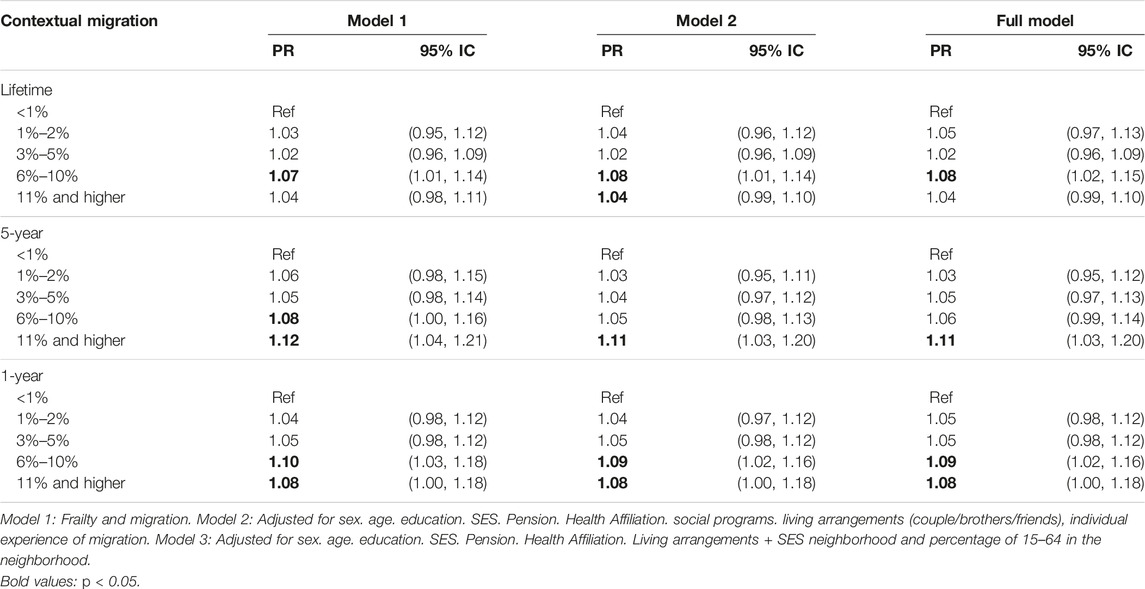
TABLE 3. Multilevel model results for pre/frailty and internal and forced contextual migration categories, Colombia, 2016.
Although attenuated, the association between contextual internal and frailty remained statistically significant when adjusting for all the covariates when comparing neighborhoods with 11% and higher versus those with <1% of 5-year migrants (model 3, PR = 1.11, CI 95%: 1.03, 1.20). For contextual internal migration in the last year, the prevalence ratios were similar across models, being statistically significant for neighborhoods with 6%–10% and 11% and higher versus <1% of migrants (model 3, PR: 1.09, CI95% 1.02, 1.16 for the category of 6%–10%; PR: 1.08, CI 95%: 1.00, 1.18 for the category of 11% and higher).
Forced migration estimators followed a similar pattern to internal migration. The prevalence of pre-frailty/frailty increased as the percentage of forced migrants in the neighborhood increased, although associations were not statistically significant (Table 4).
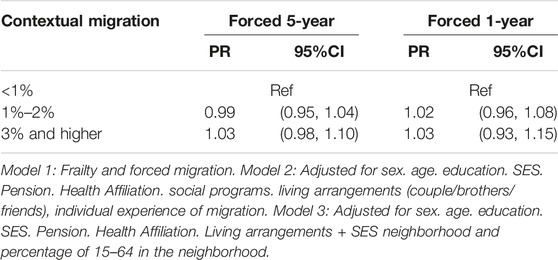
TABLE 4. Multilevel model results for pre/frailty and Neighborhood forced migrants, Colombia, 2016.
Sensitivity Analysis
The estimated associations of the three types of contextual internal migration with pre/fragility excluding the population under 18 years of age for lifetime migrants had the same direction as the main results, but were not statistically significant. For 5-year migration, results were similar to those obtained when considering the entire population, and for migration of 1 year, the prevalence ratio increased from 1.08 to 1.22 (Figure 2). In the second sensitivity analysis, the estimations obtained by categorizing the different types of migration in quartiles (Supplementary Table S1) remained similar to those observed when classifying by percentages. The prevalence ratio of pre-frailty/frailty increased as the proportion of the migrant population in the neighborhood increased, being higher and statistically significant for older adults who lived in neighborhoods within the fourth quartile of the migrant population. For the third sensitivity analysis, the estimated associations of the three types of contextual internal migration with pre/frailty when including the migratory background of the elderly in the final models were similar to those obtained when considering the entire population (Supplementary Table S2). And the fourth analysis when including forced migration (both 5 years and 1 year) as an adjustment variable in the migration models, no major changes were observed (Supplementary Table S3). Only a slight increase was observed in the prevalence of pre-frailty/frailty in neighborhoods with internal migration 11% and higher versus <1% within the past 5 years (PR = 1.12, CI 95%: 1.03, 1.21).
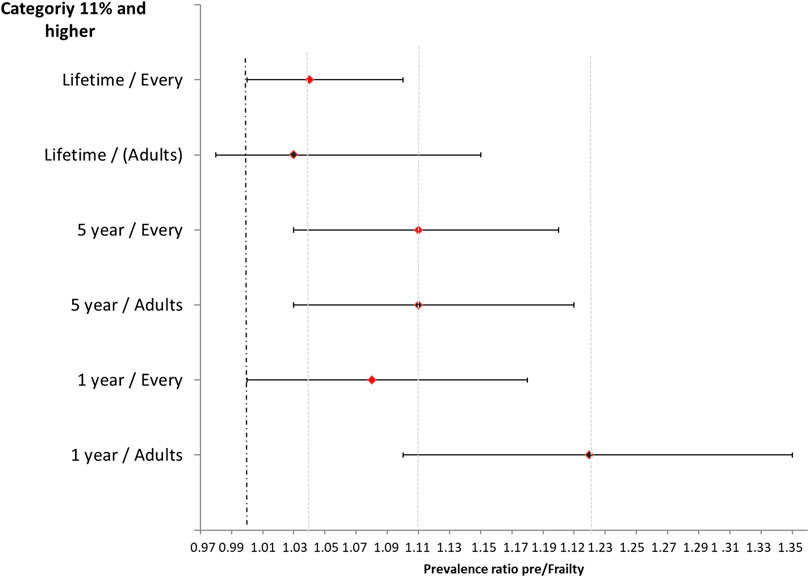
FIGURE 2. Prevalence ratio behavior for frailty in relation to types internal migration (>6%) for the entire population and only adults, Colombia, 2016.
Discussion
In this study, we aimed to analyze the association between contextual levels of internal and forced migration at the neighborhood level and frailty among older adults in Colombia. Most previous research has focused instead on individual experiences of migration instead of contextual effects. We found that the prevalence of pre-frailty/frailty was significantly higher in the elderly living in neighborhoods with a high proportion of internal migration compared to participants living in neighborhoods with low internal migration. We did not observe the same behavior for forced migration, where the proportion of forced migration in the neighborhood did not show an association with frailty.
The influence of contextual internal and forced migration on health outcomes has been scarcely studied. Specifically, to our knowledge no studies about the impacts of contextual migration on frailty are available, precluding the comparison of our findings with similar studies. Studies about frailty and migration are based on the migration background history of the elderly especially with international migration, where a greater probability of frailty has been evidenced in migrants from low-income countries based on ethnic origin (29, 30), the ethnic density of the neighborhood (living in a neighborhood characterized by a higher density of African Americans and with more residential instability) (31), the loss of protective social networks with experiences of discrimination and language barriers (19, 32) and in early adverse experiences that are reflected in old age (20, 29). One study did not show this association between a history of migration and frailty (33).
In Colombia, we observed that contextual internal migration was positively associated with frailty. Several potential mechanisms could explain this association, related to how internal migration could change the neighborhood environment or its perception from the perspective of older adults. According to social stress theory, if internal migration is negatively perceived, receiving migrants in the neighborhood could constitute a stressor (16), activating neuroinflammatory signaling that provokes inflammatory mediators (interleukins/cortisol), predisposing older adults to frailty (6, 15). In this way, internal migration could affect the perception or the objective conditions of the social environment, the physical and built environment and become a stressor for older adults. As seen with the arrival of refugees in a community in Ethiopia, the socio-cultural norms of the host peoples were altered in terms of their social insecurity and the introduction of health-related challenges (34).
From human-ecological theory (35) and social environment perspective, the increase in the proportion of internal migrants in the neighborhood increases cultural heterogeneity (28), which may be related to an increase in the perception of insecurity and the rejection of migrants by long-term inhabitants (36), with feelings of resentment that prevent social integration and the inclusion of the host population in the process of adaptation of migrants or refugees (37). Residents could also perceive migrants as a threat to the social structure and resent the external aid received by migrants (38). Other aspect are when the older adults are be considered the minority group the neighborhood leading them to be potentially discriminated against because of their age and your health factors being affected (28, 39, 40).
From the perspective of physical environments, the changes in the perception of neighborhood cohesion and safety show other mechanisms that could directly impact frailty through changes in the physical environment. This is especially relevant for frailty criteria of physical activity and prehensile strength (21) as the arrival of Internal migrants can put pressure on physical environments that were used by older adults, potentially reducing their interactions with the built environment and therefor reducing utilitarian or leisure walking or by reducing the attendance to recreational facilities subsequently decreasing physical activity in the elderly (41).
While we found that internal migration was associated with increased frailty in older adults, this association is likely to vary according to the characteristics of the receiving community (17, 18) and the intensity and characteristics of the migration process. Rapid migration of large groups, such as the one frequently experienced in Colombia, will likely produce a larger disruption in the receiving community due to perceived threats to identity, employment, and socio-cultural and religious values (36). Also, the characteristics of the receiving community could modify the effect of migration; for instance, if the community has a strong economic and social structure that facilitates the integration of migrants, that could reduce the negative perception of internal migration (17, 18).
Limitations include the cross-sectional design that precludes a causal interpretation of the relationship between internal migration and pre/frailty. Also, we do not rule out residual confusion due to variables not considered in the study or the analysis; for example, the density of local resources in the neighborhood can show the strengths or weaknesses of the neighborhood to welcome the migrant population, or the history of migration in the neighborhood. Also frailty is a complex construct linked to many factors so it’s hard to argue that migration itself impacts frailty in a direct way. There are many other factors related to frailty that could co vary with migration, also lifecourse processes.
Not being able to characterize the different migratory flows at the neighborhood level (includes exit and entry) could lead to implications such as not being able to identify attractive or rejection neighborhoods for migrants and with them the possibility of relating them to characteristics of older adults for the benefit or not of the frailty development. And another relevant aspect is not accurately knowing the spatial redistribution of the population in the period studied based on migratory flows, which would allow to some extent to know social, cultural and economic effects in the environment of the receiving and sending place of migrants and with this, quality of life variables that can influence the wellbeing of the older adults.
We found that internal migration is associated with frailty among the elderly. It is important to recognize the health status of the populations that host migrants, evaluating local resources. The internal migratory processes in the country should not be stigmatized, considering migrants as actors of cohesion and social development of the neighborhoods from the construction from the differences. We seek to fill the knowledge gap around the social etiology of frailty outside the individual context of the elderly. We also highlight the importance of studying internal migration in a country with social characteristics such as Colombia and in the urban environment.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics, research, and biosecurity committee of the National Institute of Public Health of Mexico (Protocol 1183). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
HR-R: conceptualization, methodology design, data cleaning, data analysis, preparation and writing of the initial draft, and preparation and writing of the final draft. TB-G: conceptualization, methodology design, validation, critical review, comments and review of the initial draft, and critical review, comments of the final draft. NL-O and BS: methodology design, validation, review of the initial draft, critical review, and comments on the final draft. AD: critical review and comments on the final draft.
Conflict of Interest
The authors declare that they do not have any conflicts of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.ssph-journal.org/articles/10.3389/ijph.2023.1605379/full#supplementary-material
References
1. Huenchuan, S. Envejecimiento, personas mayores y Agenda 2030 para el Desarrollo Sostenible: perspectiva regional y de derechos humanos Libros de la CEPAL. N° 154 (LC. Santiago (2018). 1–259. Available at: https://www.cepal.org/es/publicaciones/44369-envejecimiento-personas-mayores-agenda-2030-desarrollo-sostenible-perspectiva (Accessed August 22, 2022).
2.Departamento Administrativo Nacional de Estadística DANE. Proyecciones nacionales y departamentales de población 2005 -2020. Bogotá Colombia (2010). Available at: https://www.dane.gov.co/files/censos/Grupo3_Version0902.pdf (Accessed August 12, 2022).
3.Ministerio de Salud y de la Protección SocialColcienciasValle U delCaldas U de. Encuesta SABE Colombia: Situación de Salud, Bienestar y Envejecimiento en Colombia. Colombia (2016). 476. Available at: https://www.minsalud.gov.co/ (Accessed August 12, 2022).
4. García-García, FJ, Larrión Zugasti, JL, and Rodríguez Mañas, L. Fragilidad: Un fenotipo en revisión. Gac Sanit (2011) 25:51–8. doi:10.1016/j.gaceta.2011.08.001
5. Fried, LP, Tangen, CM, Walston, J, Newman, AB, Hirsch, C, Gottdiener, J, et al. Frailty in Older Adults: Evidence for a Phenotype. Journals Gerontol Ser A Biol Sci Med Sci (2001) 56(3):M146–M156. doi:10.1093/gerona/56.3.m146
6. Chen, X, Mao, G, and Leng, S. Frailty Syndrome: an Overview. Clin Interv Aging (2014) 19(9):433–41. doi:10.2147/CIA.S45300
7. Abe, T, Carver, A, and Sugiyama, T. Associations of Neighborhood Built and Social Environments with Frailty Among Mid-to-older Aged Australian Adults. Geriatr Gerontol Int (2021) 21(10):893–9. doi:10.1111/ggi.14253
8. Miao, J, Wu, X, and Sun, X. Neighborhood, Social Cohesion, and the Elderly’s Depression in Shanghai. Soc Sci Med (2019) 229:134–43. doi:10.1016/j.socscimed.2018.08.022
9.The International Organization for Migration (IOM). Peace, Dignity and equality on a Healthy Planet (2020). Available from: https://www.un.org/es/sections/issues-depth/migration/index.html (Accessed August 22, 2022).
10. Cuervo Ramirez, SM, Barbieri, AF, and Rangel Rigotti, JI. La migración interna en Colombia en la transición al siglo xxi. Una aproximación multiescalar. Rev Latinoam Población (2018) 12(22):50–68. doi:10.31406/n22a4
11.Departamento Administrativo Nacional de Estadística DANE. Censo Nacional de población y vivienda 2018 (2019). Available from: https://www.dane.gov.co/index.php/estadisticas-por-tema/demografia-y-poblacion/censo-nacional-de-poblacion-y-vivenda-2018 (Accessed August 12, 2022).
12. Fernández-Niño, J, and Navarro-Lechuga, E. Migración humana y salud: un campo emergente de investigación en Colombia. Rev Salud Pública (2018) 20(4):404–5. doi:10.15446/rsap.v20n4.74970
13. Diez Roux, AV. Neighborhoods and Health: What Do We Know? what Should We Do? Am J Public Heal (2016) 106(3):430–1. doi:10.2105/AJPH.2016.303064
14. Lu, Y, Hu, PE, and Treiman, DJ. Migration and Depressive Symptoms in Migrant-Sending Areas: Findings from the Survey of Internal Migration and Health in China. Int J Public Heal (2012) 57(4):691–8. doi:10.1007/s00038-011-0314-0
15. Ruiz, I, and Vargas-Silva, C. The Consequences of Forced Migration for Host Communities in Africa. Dans Rev D’économie Du Dév (2017) 25(135 154). doi:10.3917/edd.313.0135 Available at: https://ora.ox.ac.uk/objects/uuid:0d0331d2-a1a3-4693-8075-388817f8e142/files/m6b52aa479379707d1e7bbba73221547c.
16. Ghimire, S, Raj Singh, D, Nath, D, Jeffers, EM, and Kaphle, M. Adult Children’s Migration and Well-Being of Left behind Nepalese Elderly Parents. J Epidemiol Glob Health (2018) 8(3–4):154–1 61. doi:10.2991/j.jegh.2018.07.004
17. Robinson, D. The Neighbourhood Effects of New Immigration. Environ Planin A (2010) 42:2451–66. doi:10.1068/a4364
18. Robinson, D, and Walshaw, A. New Migration, Neighbourhood Effects and Community Change (2016). Available at: https://www.researchgate.net/publication/249313089_New_Migration_Neighbourhood_Effects_and_Community_Change (Accessed August 22, 2022).
19. Brothers, TD, Theou, O, and Rockwood, K. Frailty and Migration in Middle-Aged and Older Europeans. Arch Gerontol Geriatr (2014) 58(1):63–8. doi:10.1016/j.archger.2013.07.008
20. Walkdena, G, Andersonb, E, Vinkc, M, Tillinga, K, Howeb, L, and Ben-Shlomoa, Y. Frailty in Older-Age European Migrants: Cross-Sectional and Longitudinal Analyses of the Survey of Health, Aging and Retirement in Europe (SHARE). Soc Sci Med (2018) 213:1–11. doi:10.1016/j.socscimed.2018.07.033
21.Ministerio de Salud y Proteccion SocialColcienciasJaveriana University. Encuesta Nacional de Salud Mental (2015). Available at: https://www.minsalud.gov.co/ (Accessed August 12, 2022).
22.Instituto Colombiano de Bienestar FamiliarMinisterio de Salud y Protección SocialInstituto Nacional de SaludDepartamento Administrativo para la Prosperidad SocialUniversidad Nacional de ColombiaENSIN: Encuesta Nacional de Situación Nutricional. 2015 Encuesta Situacion nutricional en Colombia, ENSIN. Available at: https://www.minsalud.gov.co/ (Accessed August 12, 2022)
23.Ministerio de Salud y de la Protección SocialProfamilia. Encuesta Nacional de Demografia y Salud (2015). Available at: https://www.minsalud.gov.co/ (Accessed August 12, 2022).
24.Ministerio de Salud y de la Protección Social. Muestra Maestra para hogares - Sistema nacional de Estudios y Encuestas poblacionales parala salud. Bogotá Colombia (2014). Available at: https://www.minsalud.gov.co/ (Accessed August 12, 2022).
25.Departamento Administrativo Nacional de Estadística DANE. Estratificación socioeconómica para servicios públicos domiciliarios (2022). Available from: https://www.dane.gov.co/index.php/servicios-al-ciudadano/servicios-informacion/estratificacion-socioeconomica#:∼:text=La estratificación socioeconómica es una,cobrar contribuciones en esta área (Accessed August 12, 2022).
26.Departamento Administrativo Nacional de Estadística DANE. Censo Nacional de Población y Vivienda 2018. Colombia (2019). Available from: https://www.dane.gov.co/index.php/estadisticas-por-tema/demografia-y-poblacion/censo-nacional-de-poblacion-y-vivenda-2018 (cited Jul 12, 2021).
27. Spiegelman, D, and Hertzmark, E. Easy SAS Calculations for Risk or Prevalence Ratios and Differences. Am J Epidemiol (2005) 162:199–200. doi:10.1093/aje/kwi188
28. Fox, M, Thayerc, Z, and Wadhw, P. Acculturation and Health: the Moderating Role of Socio-Cultural Contex. Am Anthr (2017) 119(3):405–21. doi:10.1111/aman.12867
29. Majid, Z, Welcha, C, Davies, J, and Jackson, T. Global Frailty: The Role of Ethnicity, Migration and Socioeconomic Factors. Maturitas (2020) 139:33–41. doi:10.1016/j.maturitas.2020.05.010
30. Hoogendijk, E, Muntinga, M, Breij, S, Huisman, M, and Klokgieters, SS. Inequalities in Frailty Among Older Turkish and Moroccan Immigrants and Native Dutch: Data from the Longitudinal Aging Study Amsterdam. J Immigr Minor Heal (2022) 24:385–93. doi:10.1007/s10903-021-01169-9
31. Caldwell, JT, Lee, H, and Cagney, KA. Disablement in Context: Neighborhood Characteristics and Their Association with Frailty Onset Among Older Adults. J Gerontol B Psychol Sci Soc Sci (2019) 74(7):e40b–e49. doi:10.1093/geronb/gbx123
32. Anand, A, Syamala, T, Kanchan, I, and Bhatt, N. Understanding Frailty, Functional Health and Disability Among Older Persons in India: A Decomposition Analysis of Gender and Place of Resident. J Res Heal Sci (2020) 20(3):e00484. doi:10.34172/jrhs.2020.20
33. Ye, L, Elstgeest, L, Zhang, X, Alhambra-Borrás, T, Tan, S, and Raat, H. Factors Associated with Physical,psychological and Social Frailty Amongcommunity-Dwelling Older Persons in Europe: a Cross-Sectional Study of UrbanHealth Centres Europe (UHCE). BMC Geriatr (2021) 21:422. doi:10.1186/s12877-021-02364-x
34. Gebrehiwet, K, Abrha, F, Gebreyesus, H, and Teweldemedhin, M. The Social Health Impact of Eritrean Refugees on the Host Communities: the Case of May-Ayni Refugee Camp, Northern Ethiopia. BMC Res Notes (2020) 13(182):182. doi:10.1186/s13104-020-05036-y
35. McLaren, L, and Hawe, P. Ecological Perspectives in Health Research. J Epidemiol Community Heal (2005) 59:6–14. doi:10.1136/jech.2003.018044
36. Vos, S, Clark-Ginsberg, A, Puente-Duran, S, Salas-Weight, C, Al, E, Herrera, IC, et al. The Family Crisis Migration Stress Framework: A Framework to Understand the Mental Health Effects of Crisis Migration on Children and Families Caused by Disasters. New Dir Child Adolesc Dev (2021) 2021(176):41–59. doi:10.1002/cad.20397
37. Kreibaum, M. Their Suffering, Our burden? How Congolese Refugees Affect the Ugandan Population. World Dev (2016) 78(262–287)–87. Available at: http://www.worldbank.org/content/dam/Worldbank/Feature%20Story/Africa/afr-merle-kreibaum.pdf. doi:10.1016/j.worlddev.2015.10.019
38. Cantor, D, Swartz, J, Roberts, B, Abbara, A, Ager, A, Bhutta, Z, et al. Understanding the Health Needs of Internally Displaced Persons: A Scoping Review. J Migr Heal (2021) 29(4):100071. doi:10.1016/j.jmh.2021.100071
39. Ferrer, R, Palacio, J, Hoyos, O, and Madariaga, C. Acculturation Process and Immigrant’s Adaptation: Individual Characteristics and Social Networks. Psicol desde el Caribe (2014) 31(3):557–76. Available at: http://www.scielo.org.co/scielo.php?script=sci_abstract&pid=S0123-417X2014000300009. doi:10.14482/psdc.31.3.4766
40. Paolillo, R, and Jager, W. Simulating AcculturationDynamics between Migrants and Locals in Relation to Network Formation. Soc Sci Comput Rev (2020) 38(4):365–86. doi:10.1177/0894439318821678
41. Kim, M-J, Seo, S-H, Seo, A-R, Kim, B-K, Lee, G-Y, Choi, Y-S, et al. The Association of Perceived Neighborhood Walkability and Environmental Pollution with Frailty Among Community-Dwelling Older Adults in Korean Rural Areas: A Cross-Sectional Study. J Prev Med Public Heal (2019) 52:405–15. doi:10.3961/jpmph.19.166
Keywords: Colombia, older adults, urban areas, migration, frailty, neighborhoods, host population
Citation: Rengifo-Reina H, Barrientos-Gutiérrez T, López-Olmedo N, Sánchez BN and Diez Roux AV (2023) Frailty in Older Adults and Internal and Forced Migration in Urban Neighborhood Contexts in Colombia. Int J Public Health 68:1605379. doi: 10.3389/ijph.2023.1605379
Received: 06 September 2022; Accepted: 20 April 2023;
Published: 05 May 2023.
Edited by:
Sonja Merten, Swiss Tropical and Public Health Institute, SwitzerlandReviewed by:
Valentina Rotondi, University of Applied Sciences and Arts of Southern Switzerland, SwitzerlandCopyright © 2023 Rengifo-Reina, Barrientos-Gutiérrez, López-Olmedo, Sánchez and Diez Roux. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tonatiuh Barrientos-Gutiérrez, dGJhcnJpZW50b3NAaW5zcC5lZHUubXg=
This Original Article is part of the IJPH Special Issue “Migration Health Around the Globe—A Construction Site With Many Challenges”