 Sara Brolin Låftman1Bitte Modin1Maria Granvik Saminathen1Viveca Östberg1Petra Löfstedt2Kristiina Rajaleid1,3*
Sara Brolin Låftman1Bitte Modin1Maria Granvik Saminathen1Viveca Östberg1Petra Löfstedt2Kristiina Rajaleid1,3*- 1Department of Public Health Sciences, Faculty of Social Sciences, Stockholm University, Stockholm, Sweden
- 2Department of Public Health and Community Medicine, Institute of Medicine, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
- 3Stress Research Institute, Department of Psychology, Faculty of Social Sciences, Stockholm University, Stockholm, Sweden
Objectives: To investigate mid-adolescent boys’ and girls’ experiences of school demands, teacher support, and classmate support, and explore the associations of these factors with mental wellbeing.
Methods: Data were derived from the Swedish Health Behaviour in School-aged Children (HBSC) study of 2017/18, with information collected among 1,418 students in grade 9 (∼15–16 years). School demands, teacher support, and classmate support were measured by indices based on three items each. Mental wellbeing was measured by the Short Warwick-Edinburgh Mental Wellbeing Scale (SWEMWBS). Linear regression analyses were performed.
Results: Higher demands were associated with lower mental wellbeing. Conversely, mental wellbeing increased with greater teacher support and classmate support. Interactions between demands and the support variables showed that at the lowest levels of teacher and of classmate support, mental wellbeing was low and not associated with school demands. With increasing levels of teacher and classmate support, the overall level of mental wellbeing increased and revealed an inverse association between school demands and mental wellbeing.
Conclusion: The study contributes with knowledge about how psychosocial conditions in school may hinder or enhance wellbeing among students.
Introduction
School is an important context for children and young people where they spend a significant amount of time during their formative years. The school environment contains both stressors and resources that may affect children’s mental wellbeing. According to the Swedish Education Act [1], schools in Sweden are obliged to engage in both health prevention and promotion. While preventative efforts aim to fend off and protect against health adversities, health-promoting work revolves around strengthening the prerequisites for good health.
Although psychosocial school conditions may be linked to both adverse and positive health outcomes, previous research has largely focused on aspects of the former, such as depressive symptoms [2] or multiple health complaints, i.e., psychological complaints such as feeling sad or down, or feeling nervous, and somatic complaints such as headache and stomach-ache [3–12]. A more limited number of studies have assessed the links between psychosocial school conditions and aspects of students’ positive mental health. Yet, identifying school-related determinants of students’ mental wellbeing has the potential to support schools’ health-promoting work.
The concept of mental wellbeing can be understood in light of WHO’s definition of mental health as “a state of wellbeing in which an individual realises his or her own abilities, can cope with the normal stresses of life, can work productively and is able to make a contribution to his or her community.” [13] More specifically, mental wellbeing covers both a hedonic component (feelings of happiness and pleasure), and a eudaimonic one (feelings of meaning and self-realisation, and positive functioning) [14–17].
Previous Research on Psychosocial School Conditions and Health Outcomes
Much prior research on psychosocial school conditions has applied a stress-theoretical perspective and studied aspects of the school environment in relation to various health problems. One commonly examined outcome is adolescents’ subjective health complaints, which can be seen as a marker for stress [18]. Studies have shown that students who experience high school demands tend to report higher levels of perceived stress [19], subjective health complaints [3–12, 19, 20], and conduct problems [21]. By contrast, supportive relations at school are inversely linked with health problems among students. Perceived teacher support has been shown to be associated with fewer depressive symptoms [2] and fewer health complaints [10, 12, 21–23]. Similarly, higher levels of classmate support have been shown to be linked with fewer health complaints [10, 21, 22, 24], whereas students with problematic classmate relations report more health complaints [3]. In line with the demand-control-support model, it has also been suggested that high control as well as high levels of social support may buffer against the association between school demands and health complaints [5, 10].
While a relatively large number of studies have addressed psychosocial school conditions in relation to various health problems, the links with salutogenic health outcomes are somewhat less explored. However, research has shown associations between different aspects of positive mental health and school pressure and demands [11, 20, 25] as well as classmate support [3, 11, 25, 26, 27], and teacher support [25–28]. To the best of our knowledge, however, there is a shortage of studies that simultaneously address students’ perceptions of school demands, teacher support, and classmate support in relation to measures of positive mental health (but see [25] as well as [29, 30] which were based on the same data as the current study). There is also a lack of studies examining if teacher and classmate support can moderate the association between school demands and mental wellbeing.
With regards to mental wellbeing, higher levels tend to be reported for boys than for girls [26, 31, 32]. Furthermore, girls tend to report higher school demands than boys [19, 21, 23, 28, 33]. While previous findings regarding gender differences in perceived teacher support are mixed [21, 23, 27], boys have been shown to report higher levels of peer support than girls [21, 27]. Studies have also indicated that the association between school demands and health outcomes is stronger among girls than among boys [2, 3, 19, 23, 34]. Concerning gender differences in the associations between social support and adolescent mental health outcomes, the evidence is however more mixed [21]. Taken together, it seems clear that gender needs to be taken into consideration when examining psychosocial school conditions and student mental wellbeing.
Socioeconomic status in terms of family affluence has been shown to be positively related with students’ mental wellbeing [14]. However, the international Health Behaviour in School-aged Children (HBSC) 2013/14 report concluded that there was no clear pattern by family affluence for school pressure or classmate support [35]. Nonetheless, other studies have shown that adolescents in families with economic hardship have fewer friends in the class [36, 37] and are more often socially isolated [37]. Students from economically vulnerable households have also reported less teacher support [38]. Hence, in an analysis of psychosocial school conditions and mental wellbeing, adjusting for family affluence is relevant.
Aim of the Study
The aim of the present study was to investigate mid-adolescent boys’ and girls’ experiences of school demands, teacher social support, and classmate social support and the associations of these factors with mental wellbeing as captured through the Short Warwick-Edinburgh Mental Wellbeing Scale (SWEMWBS). A second aim was to examine if teacher social support and classmate social support modified the association between school demands and mental wellbeing.
Methods
Data Material
The data were derived from the Swedish HBSC study conducted among students in grades 5, 7, and 9 in the school year 2017/18. The HBSC is a cross-national World Health Organization (WHO) collaborative study that has been performed every fourth year since the 1980s. It includes standard questionnaires with mandatory questions used by all the participating countries to enable cross-national comparisons. In addition, there are optional packages enabling analyses of specific topics, as well as national, country-specific items [39, 40].
For the Swedish 2017/18 survey, a two-step cluster sampling was performed. First, a random sample of schools were selected. Then a class was randomly selected in school. All students in that class were invited to participate. The students completed the questionnaires with paper and pencil in their classrooms. Upon completion, they handed over the questionnaires to the teacher in sealed envelopes without any personal identification information, and the questionnaires were subsequently sent to Statistics Sweden. The students remained anonymous and were informed that participation was voluntary. In the 2017/18 survey, 4,294 students participated. The response rate was 47% at the school level, and 87%–90% at the student level [41]. The current study covers only students in grade nine (∼15–16 years) since the measure of mental wellbeing was included only in the questionnaires for this age group (n = 1,661). After exclusion of cases due to internal non-response (n = 243), the study sample included information from 1,418 students distributed across 78 classes. More information about the data collection is provided elsewhere [41].
Measures
Mental wellbeing was operationalised by the Short Warwick-Edinburgh Mental Wellbeing Scale (SWEMWBS), transformed according to the conversion table presented by Stewart-Brown et al. [42]. The skewness of the (converted) index was 0.21 (boys: 0.17; girls: 0.23) and the kurtosis 2.93 (boys: 2.54; girls: 3.35). The SWEMWBS has been validated in samples of adolescents in several countries including England and Scotland [14], Ireland [32], Australia [17] and Norway [43]. The SWEMWBS is not included in the HBSC protocol, but was added to the Nordic countries’ questionnaires of the HBSC 2017/18 survey as part of a Nordic research collaboration on positive health [44].
School demands were constructed from three items. The same, or similar, items have been used in previous studies to capture school demands [7, 10, 21, 27, 29, 30]. While the question on feeling pressured by schoolwork is mandatory in the HBSC study, the other two items are optional and therefore included in the questionnaire in only some of the countries participating in the HBSC.
Teacher support was based on the Teacher Support Scale [45, 46]. Classmate support was based on the Classmate Support Scale [45, 46].
See Table 1 for more detailed information about the above-mentioned scales.
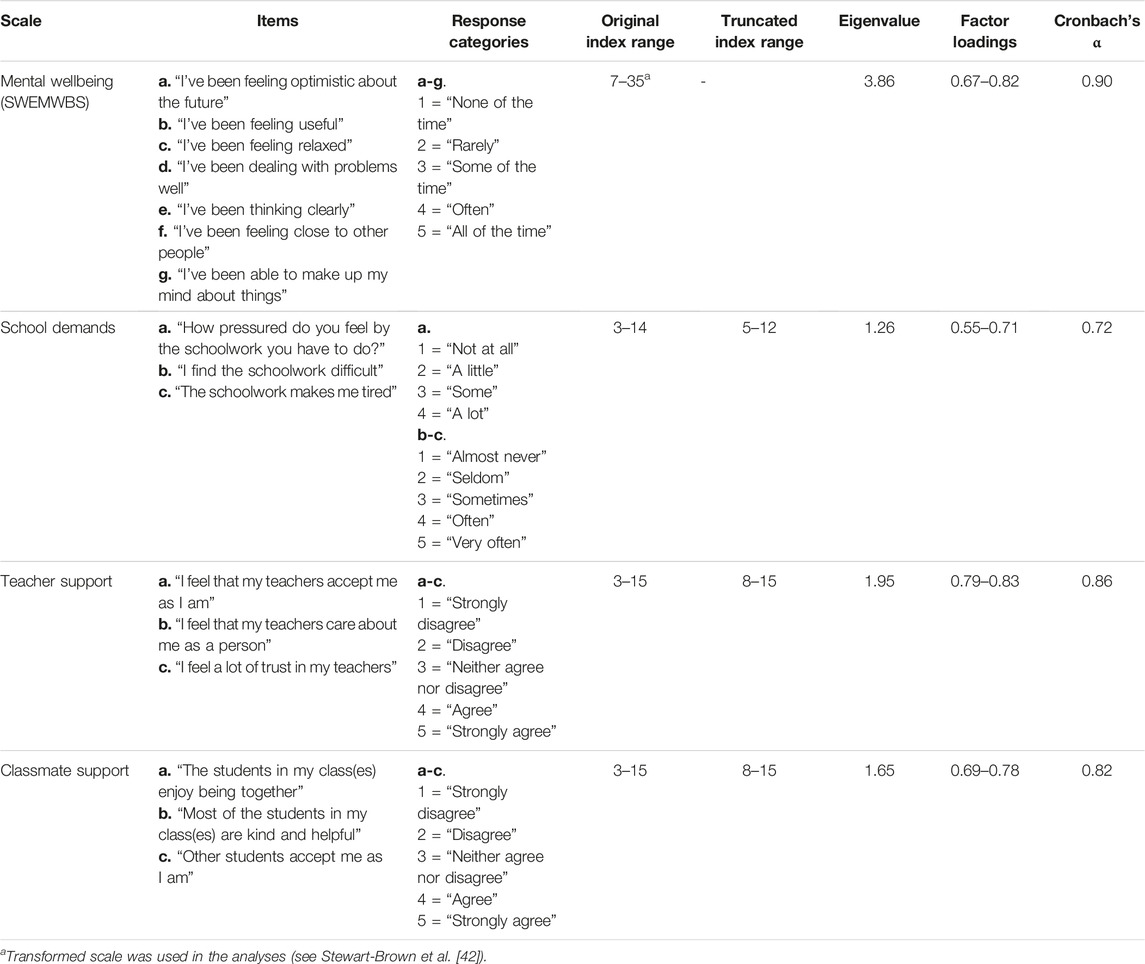
TABLE 1. Description of the measures of mental wellbeing, school demands, teacher support and classmate support. Swedish Health Behaviour in School-aged Children study 2017/18. (Sweden. 2017/2018).
Gender had the values 0 = “Boy” and 1 = “Girl.”
The Family Affluence Scale (FAS) was used to capture the family’s level of affluence, representing a proxy for socioeconomic status. Responses from six items were used to construct version III of FAS [47]: number of computers (0 = none, 1 = one, 2 = two, 3 = more than two); number of cars (0 = none, 1 = one, 2 = two or more); own bedroom (0 = no, 1 = yes); number of holidays abroad in the past year (0 = none, 1 = one, 2 = two, 3 = three or more); whether or not the family owns a dishwasher (0 = no, 1 = yes); and number of bathrooms (0 = none, 1 = one, 2 = two, 3 = three or more). Responses to these six items were summed to an index ranging between 0–13, with higher values indicating higher levels of affluence.
Statistical Method and Analytical Strategy
All the analyses were run separately for boys and girls. Descriptive statistics were retrieved for the total sample and separately by gender. Differences were tested by means of t-tests.
We plotted the mean values of mental wellbeing across the scales of school demands, teacher support and classmate support, respectively (see Supplementary File). School demands had few very low and very high values, and the mean values of mental wellbeing were thus unstable at the low and high ends of the scale, potentially influencing the results of further analyses. Therefore, the values 3–4 of school demands were recoded as 5, and the values 13–14 as 12 (in total, 12% of the values were recoded). Teacher support and classmate support had few very low values, and the values 3-7 were recoded as 8 (8% and 6% of the values, respectively).
To examine the associations between psychosocial school conditions and mental wellbeing, we estimated a series of linear ordinary least squares regression models, using the truncated scales of school demands, teacher support, and classmate support. Since the students were clustered in school classes, robust standard errors were estimated using Stata’s “robust cluster” option. In Model 1, the crude association between school demands and mental wellbeing was assessed. In Model 2, the association was adjusted for family affluence, and in Model 3, teacher and classmate support were added. Gender differences in the associations between each of the independent variables on one hand, and mental wellbeing on the other hand, were assessed by linear regression models of the total sample that included an interaction term between the respective variable and gender. Models 4 and 5 included an interaction term of the continuous measure of school demands, with the continuous measure of teacher support and classmate support, respectively. The results of the interaction analyses were visualised by means of margins plots (adjusted predictions by Stata’s “margins” command). The analyses were performed with StataSE 16.1 [48].
Results
Descriptive statistics of the study variables are presented in Table 2. On average, boys reported higher mental wellbeing than girls, as measured by the SWEMWBS. Girls experienced higher school demands than boys, on average, whereas boys on average experienced greater teacher and classmate support than girls. All gender differences were statistically significant. As expected, no gender difference in family affluence was observed.
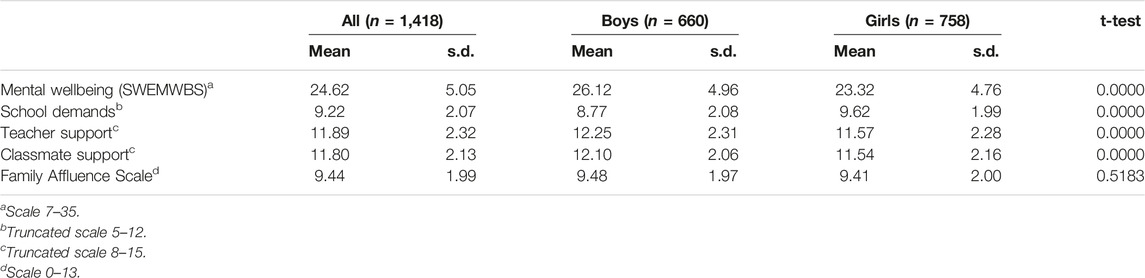
TABLE 2. Description of the study sample. Swedish Health Behaviour in School-aged Children study 2017/18. (Sweden. 2017/2018).
Results from the linear regression analyses of mental wellbeing are presented in Table 3. In the unadjusted Model 1, school demands were negatively associated with mental wellbeing in both boys (b = −0.67, 95% CI −0.86, −0.48) and girls (b = −0.93, 95% CI −1.12, −0.75). FAS was positively associated with mental wellbeing but adjusting for FAS had almost no effect on the association between school demands and mental wellbeing (Model 2). In Model 3, positive associations with mental wellbeing were observed for both teacher support (boys: b = 0.53, 95% CI 0.34, 0.72; girls: b = 0.56, 95% CI 0.40, 0.72) and classmate support (boys: b = 0.70, 95% CI 0.50, 0.69; girls: b = 0.50, 95% CI 0.31, 0.69), while the estimate for school demands was closer to the null in this model, compared to previous models.
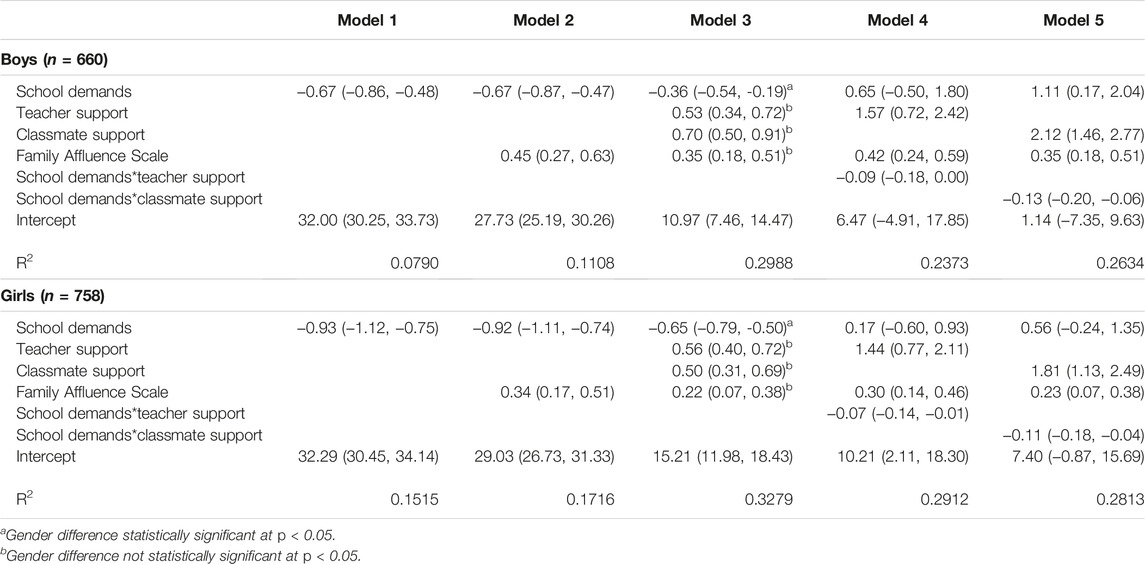
TABLE 3. Results from linear regression analyses. Predicted change in mental wellbeing per unit increase in the predictor variables, b coefficients and robust 95% confidence intervals (clustering for school class). Swedish Health Behaviour in School-aged Children study 2017/18. (Sweden. 2017/2018).
Models 4 and 5 included interaction terms of school demands with teacher support and classmate support, respectively. Figure 1 illustrates the interaction effects, depicting the association between school demands and mental wellbeing at low (index value 8), intermediate (at the median of the sample, index value 12) and high (index value 15) levels of teacher support (Figures 1A, B) and of classmate support (Figures 1C, D). In both boys and girls, higher levels of teacher support and classmate support were associated with higher overall levels of mental wellbeing. The negative interaction terms indicated an inverse association between school demands and mental wellbeing for both genders that was weaker at low levels of the support variables and became stronger with increasing levels of the respective support variables.
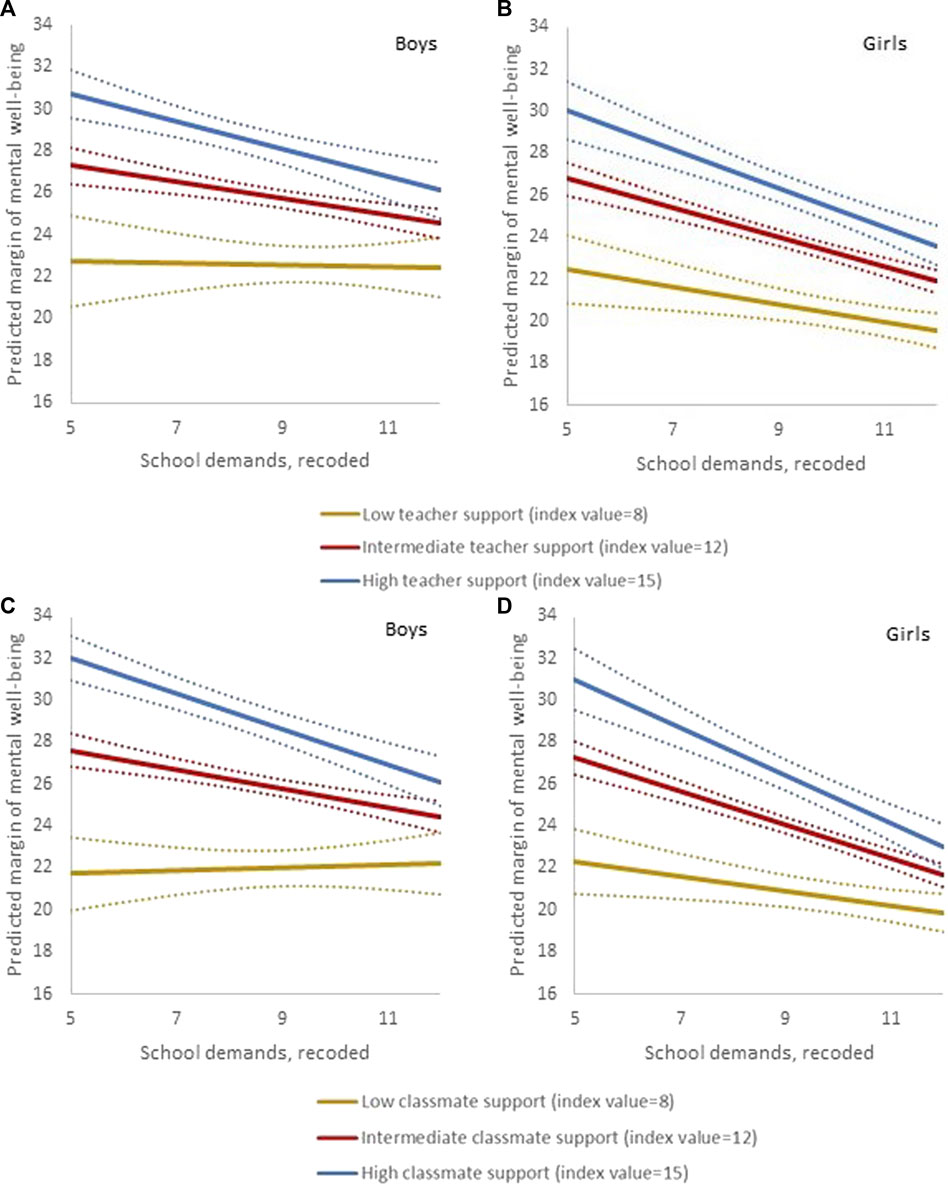
FIGURE 1. Visualisation of the interaction between school demands and teacher support, and school demands and classmate support, in gender-stratified linear regression models predicting mental wellbeing. The association between school demands and mental wellbeing is plotted at different levels of teacher support (A,B) and of classmate support (C,D) in boys (n = 660, left) and girls (n = 758, right). Dotted lines indicate 95% confidence intervals. Swedish Health Behaviour in School-aged Children study 2017/18. (Sweden. 2017/2018).
All the regression analyses were performed using the truncated indices of demands, teacher support and classmate support. As a sensitivity check, we also ran analyses using the original indices (data not shown). The results were similar to those presented, however the R2 in these models tended to be lower and the coefficients closer to the null. As another sensitivity check, we performed the same analyses as those presented in Models 4 and 5 whilst including both teacher and classmate support simultaneously (not shown). The results of the interaction analyses in these models were very similar to those presented in Table 3.
One of the items in the SWEMWBS, “I’ve been feeling close to other people”, relates to the respondent’s social relations with other persons and may thus be conflated with teacher and classmate support. However, pairwise correlations with the item “I’ve been feeling close to other people” were only moderate for teacher support (r = 0.38) and classmate support (r = 0.36). We also performed a sensitivity analysis where we omitted the item from the mental wellbeing measure (producing a scale ranging between 6-30). The results were similar to those reported (data not presented), indicating that the associations were not driven by this particular item.
Analyses of the total sample, including interaction terms between gender and each of the independent variables (not presented in table), showed that the negative association between school demands and mental wellbeing was statistically significantly stronger among girls than boys, while the associations between the other independent variables (FAS, teacher support, and classmate support) and mental wellbeing did not differ by gender.
Discussion
Focusing on indicators of psychosocial school conditions as possible determinants of positive mental health among students, this study showed that, overall, school demands were negatively, and support from teachers and classmates positively associated with mental wellbeing among both boys and girls. We furthermore observed two interaction effects, which both pointed to a negative association between perceived demands and mental wellbeing at high levels of support, but to a correspondingly weak or non-existent association at lower levels of support. Thus, at higher levels of perceived teacher- or classmate support, the average decrease in mental wellbeing of experiencing high demands was markedly steeper than at lower levels of such support. This finding does not align well with the theoretical idea that social support can buffer against the link between perceived demands and health [5, 10]. However, the results showed that low social support was in itself clearly associated with poorer wellbeing, in line with the main effect model of social support [49]. According to this theoretical model, social support enhances wellbeing since it provides positive affect as well as a sense of predictability and stability, and also promotes feelings of self-worth [49]. Following this reasoning, it is also likely that low levels of social support may be stressful in themselves. One interpretation of our finding that school demands were more strongly linked with wellbeing at higher levels of support, is that the experience of low social support may “overshadow” the potential additional impact of a high burden of school demands.
A number of prior studies have reported that greater school demands are associated with more health complaints [3–12, 19, 20]. This study demonstrated that there were clear associations also with mental wellbeing, as one aspect of positive health, with higher demands being linked with lower wellbeing. Furthermore, school demands were more strongly and negatively associated with mental wellbeing among girls than among boys. This result reflects previous findings in relation to health complaints [8, 9, 12, 19, 23, 34]. In other words, the association seems to be consistent across different types of outcomes, suggesting that school demands seem to be more important for girls’ stress-related ill-health as well as their mental wellbeing. One interpretation of this pattern is that girls, due to gendered norms, tend to place greater emphasis on schoolwork and performance than boys [19], and that school demands therefore have greater implications for both their health complaints and mental wellbeing. Girls also reported greater school demands compared with boys. Given girls’ on average higher school performance, this result may be somewhat surprising but is, again, in accordance with earlier research [19, 21, 23, 27, 33]. Also, this finding may be interpreted in light of gendered aspirations. In other words, it is possible that girls on average perceive greater school demands than boys because they, on average, tend to aim higher in terms of their school performance [19, 50].
The associations that were shown between teacher and classmate support and mental wellbeing were not surprising. Nonetheless, they add to the existing body of research by showing that support from teachers and classmates are associated not only with fewer health complaints [5, 7, 10, 12, 21–24] but also with higher levels of positive mental health. No gender differences were found in the associations between teacher and classmate support and mental wellbeing, indicating that these types of social relations are equally important for the wellbeing of boys and girls. However, boys reported higher average levels of teacher and classmate support than girls.
Although family affluence was only a control variable in the present study, the finding that it was positively associated with mental wellbeing deserves to be highlighted. A previous study based on Danish HBSC data reported differences in low, but not in high, mental wellbeing by parents’ occupational class [51]. Future studies should examine whether social health inequities in positive mental health among adolescents exist also when using other indicators of socioeconomic status, such as parents’ education or income, preferably based on information collected from parents or from official registers.
The main strength of this study is the use of a measure of mental wellbeing that has been previously validated in similar age groups in various country settings [14, 17, 32, 43]. Another benefit is the relatively large sample size. However, there are also limitations. First, we acknowledge the difficulties in drawing conclusions about the size of the (statistical) effects of school-related conditions on mental wellbeing and about the qualitative implications of our findings for policymakers and stakeholders. Since our measure of mental wellbeing was based on a self-reported and subjective scale rather than a clinical measure, it is a delicate issue to define values that indicate an absolute “high” or “low” level of mental wellbeing. The same is true for the measures of school demands and support. In other words, we examined the general patterns between psychosocial school conditions and mental wellbeing, but are inhibited to make any claims in more absolute or practical terms with support in the data. To do this, other types of measures and/or another research approach (e.g., studying the effects of a specific intervention, or applying qualitative methods) would have been needed. Furthermore, the cross-sectional nature of the data inhibits causal explanations with support in the data. Although it seems reasonable to assume that students’ perceptions of school demands and social support may affect their mental wellbeing, it cannot be ruled out that the emotional state of students impacts on their perception of their psychosocial school conditions. To disentangle the directionality of the associations, future research should assess the links between psychosocial school conditions and mental wellbeing by use of longitudinal data. Another limitation concerns the possible systematic bias related to the attrition in two steps: at the school-level, a number of the sampled schools did not participate; and at the student-level, 13% of the ninth graders did not participate due to absence on the day of the survey [41]. Furthermore, since information is lacking about which schools in the sample that participated and which did not, there are limited possibilities of estimating the response bias at the school-level. With regards to student non-response, there may be a risk of systematic bias. One can assume that students who were absent due to truancy or illness have on average lower mental wellbeing, and possibly also experience greater school demands and less teacher and classmate support than students who took part in the study. However, we do not see any reasons why this possible bias would affect the associations found to any substantial degree; if anything, we believe that they may have been underestimated rather than the other way around.
Finally, it should be underlined that the current study was based on information collected among ninth grade students in Sweden. Grade nine is the final year of compulsory school, and academic performance is especially critical during this school year as the applications for upper secondary school are based on the student’s final grades from compulsory school. Thus, given the particular importance of school performance in grade 9, it is possible that school-related conditions are particularly strongly associated with student wellbeing (and adverse health) during this school year. Consequently, assessing the generalisability of the associations between school demands, teacher support, and classmate support and mental wellbeing requires data collected among students in other age groups and in other school systems.
Conclusion
This study contributes with knowledge about how psychosocial conditions in school may hinder or enhance positive mental health among students. The analyses showed that mental wellbeing increased with greater teacher support and classmate support among both boys and girls. Higher school demands were associated with lower mental wellbeing among students experiencing higher levels of support, while the level of school demands did not have a strong association with mental wellbeing when teacher and classmate support were reported as low. Based on the study’s findings, it is possible to suggest that in order to promote students’ mental wellbeing, schools should support their students so that they feel that the demands are manageable, ascertain that their teachers have the time and possibilities to provide adequate support to their students, and enhance a positive social climate among students.
Ethics Statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent from the participants’ legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author Contributions
All authors SL, BM, MS, VÖ, PL, and KR contributed to the conceptualisation and the design of the study. KR planned and performed the statistical analyses. SL and MS drafted a first version of the manuscript. All authors SL, BM, MS, VÖ, PL, and KR critically revised drafts of the manuscript, and read and approved of the final version.
Funding
The study was conducted within the research project “Health Behaviour in School-aged Children: Individual and contextual associations with psychological (ill-)health” funded by the Public Health Agency of Sweden. Open access funded by Stockholm University Library.
Conflict of Interest
The authors declare that they do not have any conflicts of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.ssph-journal.org/articles/10.3389/ijph.2022.1605167/full#supplementary-material
References
1.Skollag. Swedish Education Act (SFS 2010:800). Stockholm: Swedish Ministry of Education (2010). Retrieved from: https://www.riksdagen.se/sv/dokument-lagar/dokument/svensk-forfattningssamling/skollag-2010800_sfs-2010-800 (Accessed June 27, 2022).
2. Undheim, AM, and Sund, AM. School Factors and the Emergence of Depressive Symptoms Among Young Norwegian Adolescents. Eur Child Adolesc Psychiatr (2005) 14:446–53. doi:10.1007/s00787-005-0496-1
3. Gillander Gådin, K, and Hammarström, A. Do changes in the Psychosocial School Environment Influence Pupils’ Health Development? Results from a Three-Year Follow-Up Study. Scand J Public Health (2003) 31:169–77. doi:10.1080/14034940210134121
4. Murberg, TA, and Bru, E. School-related Stress and Psychosomatic Symptoms Among Norwegian Adolescents. Sch Psychol Int (2004) 25:317–32. doi:10.1177/0143034304046904
5. Modin, B, and Östberg, V. The Psychosocial Work Environment and Stress-Related Health Complaints. An Analysis of Children’s and Adolescents’ Situation in School. In: Fritzell, J, and Lundberg, O, editors. Health Inequalities and Welfare Resources. Continuity and Change in Sweden. Bristol, UK: Policy Press (2007). p. 109–33.
6. Eriksson, U, and Sellström, E. School Demands and Subjective Health Complaints Among Swedish Schoolchildren: A Multilevel Study. Scand J Public Health (2010) 38(4):344–50. doi:10.1177/1403494810364683
7. Sonmark, K, Godeau, E, Augustine, L, Bygren, M, and Modin, B. Individual and Contextual Expressions of School Demands and Their Relation to Psychosomatic Health. A Comparative Study of Students in France and Sweden. Child Ind Res (2016) 9:93–109. doi:10.1007/s12187-015-9299-1
8. Aanesen, F, Meland, E, and Torp, S. Gender Differences in Subjective Health Complaints in Adolescence: The Roles of Self-Esteem, Stress from Schoolwork and Body Dissatisfaction. Scand J Public Health (2017) 45(4):389–96. doi:10.1177/1403494817690940
9. Giota, J, and Gustafsson, J-E. Perceived Demands of Schooling, Stress and Mental Health: Changes from Grade 6 to Grade 9 as a Function of Gender and Cognitive Ability. Stress and Health (2017) 33(3):253–66. doi:10.1002/smi.2693
10. Sonmark, K, and Modin, B. Psychosocial Work Environment in School and Students’ Somatic Health Complaints: An Analysis of Buffering Resources. Scand J Public Health (2017) 45:64–72. doi:10.1177/1403494816677116
11. Markkanen, I, Välimaa, R, and Kannas, L. Associations between Students’ Perceptions of the Psychosocial School Environment and Indicators of Subjective Health in Finnish Comprehensive Schools. Child Soc (2019) 33:chso.12334–502. doi:10.1111/chso.12334
12. Redmond, G, García-Moya, I, Moreno, C, Mooney, A, and Brooks, F. Gender Differences in the Relationship between Pressure from Schoolwork and Health Complaints: a Three Country Study. Child Ind Res (2022) 15:763–80. doi:10.1007/s12187-021-09879-0
13.World Health Organization. Mental Health: Strengthening Our Response (2020). Retrieved from: https://www.who.int/news-room/fact-sheets/detail/mental-health-strengthening-our-response (Accessed June 27, 2022).
14. Clarke, A, Friede, T, Putz, R, Ashdown, J, Martin, S, Blake, A, et al. Warwick-Edinburgh Mental Well-Being Scale (WEMWBS): Validated for Teenage School Students in England and Scotland. A Mixed Methods Assessment. BMC Public Health (2011) 11:487. doi:10.1186/1471-2458-11-487
15. Ryan, RM, and Deci, EL. On Happiness and Human Potentials: a Review of Research on Hedonic and Eudaimonic Wellbeing. Annu Rev Psychol (2001) 52:141–66. doi:10.1146/annurev.psych.52.1.141
16. Tennant, R, Hiller, L, Fishwick, R, Platt, S, Joseph, S, Weich, S, et al. The Warwick-Edinburgh Mental Well-Being Scale (WEMWBS): Development and UK Validation. Health Qual Life Outcomes (2007) 5:63. doi:10.1186/1477-7525-5-63
17. Hunter, S, Houghton, S, and Wood, L. Positive Mental Well-Being in Australian Adolescents: Evaluating the Warwick-Edinburgh Mental Well-Being Scale. Aust Educ Develop Psychol (2015) 32:93–104. doi:10.1017/edp.2015.12
18. Corell, M, Friberg, P, Löfstedt, P, Petzold, M, and Chen, Y. Subjective Health Complaints in Early Adolescence Reflect Stress: A Study Among Adolescents in Western Sweden. Scand J Public Health (2022) 50:516–23. doi:10.1177/14034948211008555
19. Östberg, V, Plenty, S, Låftman, SB, Modin, B, and Lindfors, P. School Demands and Coping Resources – Associations with Multiple Measures of Stress in Mid-adolescent Girls and Boys. Int J Environ Res Public Health (2018) 15:2143. doi:10.3390/ijerph15102143
20. Cosma, A, Stevens, G, Martin, G, Duinhof, EL, Walsh, SD, Garcia-Moya, I, et al. Cross-National Time Trends in Adolescent Mental Well-Being from 2002 to 2018 and the Explanatory Role of Schoolwork Pressure. J Adolesc Health (2020) 66:S50–S58. doi:10.1016/j.jadohealth.2020.02.010
21. Plenty, S, Östberg, V, Almquist, YB, Augustine, L, and Modin, B. Psychosocial Working Conditions: an Analysis of Emotional Symptoms and Conduct Problems Amongst Adolescent Students. J Adolesc (2014) 37:407–17. doi:10.1016/j.adolescence.2014.03.008
22. Bergh, D, Hagquist, C, and Starrin, B. Social Relations in School and Psychosomatic Health Among Swedish Adolescents—The Role of Academic Orientation. Eur J Public Health (2011) 21(6):699–704. doi:10.1093/eurpub/ckq140
23. Låftman, SB, and Modin, B. School-performance Indicators and Subjective Health Complaints: Are There Gender Differences? Sociol Health Illn (2012) 34:608–25. doi:10.1111/j.1467-9566.2011.01395.x
24. Almquist, YB, Modin, B, and Augustine, L. Peer Acceptance in the School Class and Subjective Health Complaints: A Multilevel Approach. J Sch Health (2013) 83(10):690–6. doi:10.1111/josh.12082
25. Lábiscsák-Erdélyi, Z, Veres-Balajti, I, Somhegyi, A, and Kósa, K. Self-Esteem Is Independent Factor and Moderator of School-Related Psychosocial Determinants of Life Satisfaction in Adolescents. Int J Environ Res Public Health (2022) 19(9):5565–5. doi:10.3390/ijerph19095565
26. Warne, M, Snyder, K, and Gillander Gådin, K. Participation and Support – Associations with Swedish Pupils’ Positive Health. Int J Circumpolar Health (2017) 76:1373579. doi:10.1080/22423982.2017.1373579
27. Plenty, S, Östberg, V, and Modin, B. The Role of Psychosocial School Conditions in Adolescent Prosocial Behaviour. Sch Psychol Int (2015) 36:283–300. doi:10.1177/0143034315573350
28. García-Moya, I, Brooks, F, Morgan, A, and Moreno, C. Subjective Well-Being in Adolescence and Teacher Connectedness. A Health Asset Analysis. Health Educ J (2015) 74(6):641–54. doi:10.1177/0017896914555039
29. Låftman, SB, Granvik Saminathen, M, Modin, B, and Löfstedt, P. Excellent Self-Rated Health Among Swedish Boys and Girls and its Relationship with Working Conditions in School: A Cross-Sectional Study. Int J Environ Res Public Health (2021) 18(3):1310. doi:10.3390/ijerph18031310
30. Wahlström, J, Låftman, SB, Modin, B, and Löfstedt, P. Psychosocial Working Conditions in School and Life Satisfaction Among Adolescents in Sweden: A Cross-Sectional Study. Int J Environ Res Public Health (2021) 18(10):5337. doi:10.3390/ijerph18105337
31. Knudsen, L. Mental Health and Well-Being, Chapter 1 in Campbell-Jack, D, Hinchcliffe, S, and Rutherford, L, (Eds.). Scottish Health Survey 2015 – Volume 1: Main Report, (2016). Retrieved from: https://www.gov.scot/publications/scottish-health-survey-2015-volume-1-main-report/pages/6/ (Accessed June 27, 2022).
32. McKay, MT, and Andretta, JR. Evidence for the Psychometric Validity, Internal Consistency and Measurement Invariance of Warwick Edinburgh Mental Well-Being Scale Scores in Scottish and Irish Adolescents. Psychiatry Res (2017) 255:382–6. doi:10.1016/j.psychres.2017.06.071
33. Löfstedt, P, García-Moya, I, Corell, M, Paniagua, C, Samdal, O, Välimaa, R, et al. School Satisfaction and School Pressure in the WHO European Region and North America: An Analysis of Time Trends (2002–2018) and Patterns of Co-occurrence in 32 Countries. J Adolesc Health (2020) 66(6):S59-S69–S69. doi:10.1016/j.jadohealth.2020.03.007
34. Högberg, B, Strandh, M, and Hagquist, C. Gender and Secular Trends in Adolescent Mental Health over 24 Years – the Role of School-Related Stress. Soc Sci Med (2020) 250:112890. doi:10.1016/j.socscimed.2020.112890
35. Inchley, JC, Currie, DB, Young, T, Samdal, O, Torsheim, T, Augustson, L, et al. Growing up Unequal: Gender and Socioeconomic Differences in Young People's Health and Well-Being. Copenhagen, Denmark: World Health Organization. Regional Office for Europe (2016). Retrieved from: https://apps.who.int/iris/handle/10665/326320 (Accessed June 27, 2022).
36. Olsson, E. The Economic Side of Social Relations: Household Poverty, Adolescents' Own Resources and Peer Relations. Eur Sociol Rev (2007) 23:471–85. doi:10.1093/esr/jcm016
37. Hjalmarsson, S, and Mood, C. Do poorer Youth Have Fewer Friends? the Role of Household and Child Economic Resources in Adolescent School-Class Friendships. Child Youth Serv Rev (2015) 57:201–11. doi:10.1016/j.childyouth.2015.08.013
38. Olsson, E. The Role of Relations: Do Disadvantaged Adolescents Benefit More from High-Quality Social Relations? Acta Sociol (2009) 52(3):263–86. doi:10.1177/0001699309339802
39. Inchley, JC, Stevens, GWJM, Samdal, O, and Currie, DB. Enhancing Understanding of Adolescent Health and Well-Being: The Health Behaviour in School-Aged Children Study. J Adolesc Health (2020) 66(6):S3–S5. doi:10.1016/j.jadohealth.2020.03.014
40. Inchley, J, Currie, D, Budisavljevic, S, Torsheim, T, Jåstad, A, Cosma, A, et al. editors. Spotlight on Adolescent Health and Well-Being. Findings from the 2017/2018 Health Behaviour in School-Aged Children (HBSC) Survey in Europe and Canada. International Report. Volume 1. Key Findings. Copenhagen: WHO Regional Office for Europe (2020). Retrieved from: https://apps.who.int/iris/handle/10665/332091 (Accessed June 27, 2022).
41.Public Health Agency of Sweden. Skolbarns Hälsovanor 2017/18. Grundrapport [Health Behaviour in School-Aged Children 2017/18. Basic Report]. Stockholm/Östersund: Public Health Agency of Sweden (2019). Retrieved from: https://www.folkhalsomyndigheten.se/publikationer-och-material/publikationsarkiv/s/skolbarns-halsovanor-i-sverige-201718–-grundrapport/ (Accessed June 27, 2022).
42. Stewart-Brown, S, Tennant, A, Tennant, R, Platt, S, Parkinson, K, and Weich, S. Internal Construct Validity of the Warwick-Edinburgh Mental Well-Being Scale (WEMWBS): a Rasch Analysis Using Data from the Scottish Health Education Population Survey. Health Qual Life Outcomes (2009) 7:15. doi:10.1186/1477-7525-7-15
43. Ringdal, R, Bradley Eilertsen, M-E, Nissen Bjørnsen, H, Espnes, GA, and Moksnes, UK. Validation of Two Versions of the Warwick-Edinburgh Mental Well-Being Scale Among Norwegian Adolescents. Scand J Public Health (2018) 46:718–25. doi:10.1177/1403494817735391
44. Eriksson, C, Arnarsson, AM, Damsgaard, MT, Löfstedt, P, Potrebny, T, Suominen, S, et al. Towards Enhancing Research on Adolescent Positive Mental Health. Nordic Welfare Res (2019) 4:113–28. doi:10.18261/issn.2464-4161-2019-02-08
45. Torsheim, T, Wold, B, and Samdal, O. The Teacher and Classmate Support Scale. Sch Psychol Int (2000) 21(2):195–212. doi:10.1177/0143034300212006
46. Torsheim, T, Samdal, O, Rasmussen, M, Freeman, J, Griebler, R, and Dur, W. Cross-national Measurement Invariance of the Teacher and Classmate Support Scale. Soc Ind Res (2010) 105(1):145–60. doi:10.1007/s11205-010-9770-9
47. Torsheim, T, Cavallo, F, Levin, KA, Schnohr, C, Mazur, J, Niclasen, B, et al. Psychometric Validation of the Revised Family Affluence Scale: a Latent Variable Approach. Child Ind Res (2016) 9:771–84. doi:10.1007/s12187-015-9339-x
49. Cohen, S, and Wills, TA. Stress, Social Support, and the Buffering Hypothesis. Psychol Bull (1985) 98(2):310–57. Retrieved from: https://psycnet.apa.org/doi/10.1037/0033-2909.98.2.310 (Accessed June 27, 2022).
50. Låftman, SB, Almquist, YB, and Östberg, V. Students' Accounts of School-Performance Stress: a Qualitative Analysis of a High-Achieving Setting in Stockholm, Sweden. Sweden J Youth Stud (2013) 16:932–49. doi:10.1080/13676261.2013.780126
Keywords: school demands, teacher support, classmate support, wellbeing, school
Citation: Låftman SB, Modin B, Granvik Saminathen M, Östberg V, Löfstedt P and Rajaleid K (2023) Psychosocial School Conditions and Mental Wellbeing Among Mid-adolescents: Findings From the 2017/18 Swedish HBSC Study. Int J Public Health 67:1605167. doi: 10.3389/ijph.2022.1605167
Received: 27 June 2022; Accepted: 19 December 2022;
Published: 05 January 2023.
Edited by:
Stéphanie Baggio, University of Bern, SwitzerlandReviewed by:
Lorena Charrier, University of Turin, ItalyJoanna Mazur, University of Zielona Góra, Poland
Copyright © 2023 Låftman, Modin, Granvik Saminathen, Östberg, Löfstedt and Rajaleid. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kristiina Rajaleid, a3Jpc3RpaW5hLnJhamFsZWlkQHN1LnNl