 Lise Eriksson
Lise Eriksson Andrey Tibajev1,2
Andrey Tibajev1,2- 1Department of Women’s and Children’s Health, Faculty of Medicine, Uppsala University, Uppsala, Sweden
- 2Institute for Futures Studies, Stockholm, Sweden
Objectives: Women’s healthcare is a potential source of cross-cultural conflicts. Diverging values between healthcare providers and patients challenges the provision of culturally sensitive care and meeting migrant women’s needs. The aim is to investigate healthcare providers’ values in relation to sexual and reproductive rights, gender equality, migration and religion in Swedish sexual and reproductive healthcare.
Methods: A national cross-sectional study was carried out. The questionnaire was distributed through a non-probability sample to midwives or other nurses, gynaecologists and obstetricians, and hospital social workers (n = 1,041). Through descriptive statistics, we mapped their values, comparing healthcare provider data to external representative population survey data.
Results: Healthcare providers in sexual and reproductive healthcare displayed homogeneous liberal social values, being permissive towards sexual and reproductive rights and restrictive against gender-based violence. They were for gender equality, expressed low anti-immigrant sentiments, and had even more liberal values than the Swedish population and a demographically comparative sub-population.
Conclusion: Individuals with very liberal values are selected to work in Swedish sexual and reproductive healthcare. Healthcare providers need self-reflexivity to avoid conflicts in clinical encounters in a diversified society.
Introduction
The human rights perspective of sexual and reproductive rights includes reproductive decision-making free of discrimination, coercion and violence [1]. The Guttmacher-Lancet Commission emphasized; “All individuals have a right to make decisions governing their bodies and to access services that support that right” [2]. Hence, sexual and reproductive healthcare services, including abortion and contraceptive counselling, are potential contentious spaces and sources of cross-cultural conflicts and conflicts between private and professional values. In the context of migrant healthcare, diverging values between healthcare providers (HCPs) and patients challenges the provision of culturally sensitive care and meeting migrant women’s specific health needs.
Healthcare providers relate to the politicized area of sexual and reproductive rights, gender equality, migration and religion with influence by personal values, ideologies, professional ethos, laws and policy guidelines. By “professional ethos” we refer to a set of internalized professional norms and values guiding professional practice. International studies have shown that moral and religious values may affect HCPs’ clinical decisions and patient care [3, 4]. By international comparison, people in Sweden display the most liberal and individualistic values on reproduction and sexuality [5]. However, values of Swedish HCPs are under-researched, despite contributing to tensions in healthcare between equality and cultural diversity, and between secularity and religious diversity. Previous studies have shown that the dilemma of gender equality and cultural diversity in Swedish healthcare encounters involves tensions between the values of cultural and religious diversity and liberal, individualistic values on sexual and reproductive rights matters [6, 7]. By investigating values at the intersection of the individual, professional and policy levels, this study also contributes to research on structural asymmetries in healthcare access in Sweden and other European countries [8]. For example, qualitative studies have found indications of ethnic minority healthcare staff and healthcare users experiencing racism in Swedish healthcare [8]. In multicultural consultations in women’s healthcare, HCPs’ awareness of their own values and patients’ values is of great importance for successful consultations by preventing misunderstandings and thus suboptimal care [6, 9, 10].
Sweden became a country of net immigration in the post-war years and after an acceleration of immigration in the 21st century, a fifth of the Swedish population are currently foreign born with the Nordic countries, former Yugoslavia, Syria, and Iraq being the most common backgrounds [11]. Healthcare providers caring for Sweden’s diverse population use policy strategies to handle differences in language, health literacy, cultural norms and values [6]. Migrants’ public health research suggests that multicultural integration policies, characterising Sweden, have a positive effect on self-rated health of migrants in comparison to assimilationist and exclusionist policy models [12]. In light of Sweden’s changed demography due to immigration from low-income countries, Swedish policies emphasize, on the one hand, that public welfare institutions should promote cultural and religious diversity [13]. Sweden’s attempts to address health inequalities among migrants include promotion of culturally sensitive care, which takes into account how perceptions of sexual and reproductive rights and gender equality are influenced by cultural norms [14]. The purpose of culturally sensitive care is to improve communication between HCPs and diverse populations, enhance migrants’ health literacy, and acknowledge the impact of the migration process on health [14]. On the other hand, as part of the Swedish Government’s gender mainstreaming program, HCPs are encouraged to incorporate gender equality perspectives [15].
Sexual and reproductive healthcare is internationally the foremost medical field allowing conscientious objection [16]. Unlike law in most EU countries, Swedish policy does not grant HCPs conscientious objection and protection of women’s reproductive rights has broad societal support. Since the 1990s, access to abortion care is better than in most Western countries, because midwives can provide counselling and medical abortion—although prescribed by physicians—and women do not need to travel for abortions [3]. Historically, controversies surrounded abortion in Sweden since the introduction of abortion for socio-medical reasons in 1946 until the 1975 Abortion Act permitting abortion on demand [17, 18]. During these decades, some prominent gynaecologists joined Christian conservatives in campaigns against abortion [18].
Most professional associations of HCPs were open to liberalization of abortion law in early 1970s [17]. In statements to the government report The right to abortion (1971) the Swedish Medical Association, the Swedish Gynecological Association and the Swedish Hospital Social Workers’ Association advocated women’s decision-making power in early pregnancy. However, the Swedish Association of Midwives was critical of women’s statutory right to abortion and advocated established indications for abortion [17, 19]. Since the 1980s, there has been strong support for abortion on demand, and Swedish anti-abortion campaigns demanding a conscience clause in the 1990s had no political success [20]. Still today, heated political debates on abortion and freedom of conscience occur in several European countries in relation to HCPs’ right to refuse to provide or refer for abortion [21]. To prevent conflicts and discrimination, we need more knowledge about HCPs’ values about sexual and reproductive rights, gender equality, migration and religion in relation to policies governing sexual and reproductive healthcare.
The aim is to investigate self-expressed values in relation to sexual and reproductive rights, gender equality, migration and religion among Swedish HCPs in sexual and reproductive healthcare in comparison with the Swedish population. We analyse the following research questions: 1) What are the values in relation to sexual and reproductive rights, gender equality, migration, and religion among HCPs in sexual and reproductive healthcare? 2) To what extent do these values among HCPs differ from values among the Swedish population in general, and if so, why do they differ? We expect that the differences between the values among HCPs and the Swedish population correlate with socio-demographic attributes, selection into healthcare professions, as well as professional ethos and clinical experience.
Methods
Study Setting
The target group was midwives or other nurses, gynaecologists and obstetricians, and hospital social workers within sexual and reproductive healthcare in Sweden. This includes outpatient and inpatient care in gynaecology, obstetric care and reproductive medicine. Most nurses are midwives, and most physicians in sexual and reproductive healthcare are gynaecologists and obstetricians. Social workers in Swedish healthcare are since 2019 licensed as healthcare counsellors. We refer to both licensed and unlicensed social workers in healthcare by the term “hospital social workers.” When we onwards use the term HCPs, we refer to Swedish HCPs in sexual and reproductive healthcare.
Study Design
We conducted a cross-sectional study using an online questionnaire. The questionnaire was pilot tested twice—first with 20 respondents within the target group including follow-up qualitative interviews, second with 200 respondents outside the target group to test the used measures. All respondents were anonymous, and no identifying data were collected [22].
Variables
The questionnaire included questions about HCPs’ demographic and work characteristics, as well as values within sexual and reproductive rights, gender equality, migration and religion. To allow for comparison with the general Swedish population, value questions were taken from the European Social Survey (ESS2002), European Values Study (EVS2017), International Social Survey Programme (ISSP2018) and World Values Survey (WVS2011) where applicable [23–26]. Table 1 displays an overview of the included value questions with information about data source for the Swedish comparison group. As noted, some of the questions did not appear in the Swedish population-wide surveys.
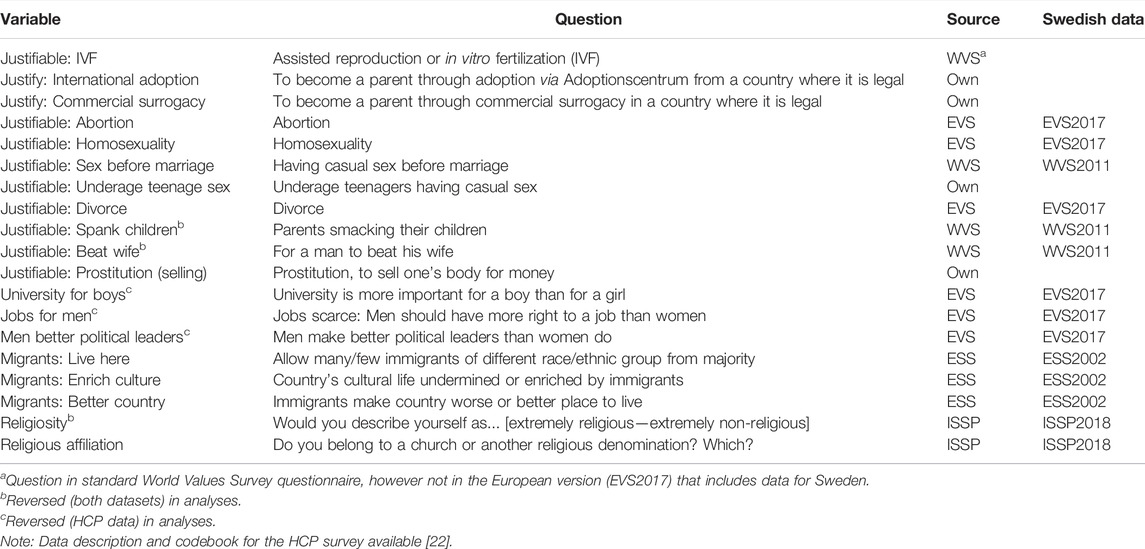
TABLE 1. Overview of variables, survey questions about values, and data sources for the Swedish comparison group. MigraMed Healthcare Providers Study, Sweden, 2021.
We define the term liberal social values as being permissive within matters of sexual and reproductive rights, against gender-based violence, for gender equality, and for immigration. Some social value items are therefore reversed in the following analyses (see Table 1) so that all higher values imply more liberal. The questions had different scales. If not stated otherwise, all value items are scaled to 0–1 to facilitate comparison.
Data Collection
Data was collected between January and May 2021 with a non-probability sample by distributing the questionnaire through the target population’s workplaces and through professional associations and interest groups for Swedish midwives and gynaecologists. At the data collection stage, all participants were welcome to answer the questionnaire without any exclusion based on workplace or profession. This resulted in a total sample of 1,257 respondents. The analytical sample is constructed by excluding respondents who do not fit the target population: either working in other fields of medicine than sexual and reproductive healthcare, in another profession, or being of retirement age (above 67). This produces an analytical sample of 1,041 respondents, covering 594 midwives, 411 physicians and 36 hospital social workers (Supplementary Table S1). Based on official statistics [27], and using the number of midwives working in healthcare and gynaecologists/obstetricians under the age of 65 as baselines, the analytical sample covers roughly nine and 30%, respectively, of the target populations. The difference was likely due to more effective marketing by the professional association for gynaecologists, distributing the survey to all members by e-mail, and a higher proportion of Swedish gynaecologists being members in comparison to the association for midwives. To our knowledge, there are no statistics of hospital social workers in sexual and reproductive healthcare. Tests of the values for the each of three professions in the sample revealed no substantial differences between them, and we therefore refrain from dividing up the presentation of results by profession.
Statistical Analysis
The research questions are analysed using descriptive statistics, comparing means of values and distributions between HCPs and the Swedish population. Almost all respondents in the HCP sample are women and, by definition, highly educated with at least a bachelor’s degree (including midwives), and no older than 67 years old (Supplementary Table S1). Demographic variables such as gender, education, and age are known to correlate with social and religious values [28–30]. To study whether the values of HCPs are different from what can be expected given their demographic composition, i.e., to answer the second research question, a representative sub-sample of the Swedish population that only includes highly educated (bachelor and above) women under the age of 67 is created (Supplementary Table S2, for demographic variables of the Swedish population). If HCPs and the sub-sample exhibit the same value patterns, then the values of HCPs are explained by their demographic composition. However, if differences in values are found between the two groups, then the explanation for HCPs’ values must be found in relation to their profession. Additional analyses are performed for issues on which HCPs stand out in comparison to the sub-sample to study whether their values vary with clinical years. We do not assume any specific correlation pattern and consequently use locally weighted scatterplot smoothing (LOWESS) for variables we treat as continuous (all but religious affiliation) and a multinomial logistic regression with clinical years and clinical years squared for the nominal variable religious affiliation. LOWESS is a non-parametric analysis presenting the data as it is, and multinomial logistic regression does not assume any specific relation between the included categories.
Ethical Approval
Ethical approval was gained by the Regional Ethical Committee (Dnr 2018/425) and by the Swedish Ethical Review Authority (Dnr 2020-07187). Questions were designed to minimize the risk of discomfort and invasion of privacy, and informed written consent was obtained.
Results
HCPs’ Self-Expressed Values
Starting with the first research question on HCPs values, the respondents displayed homogeneous values, often at the extremes of included scales (Supplementary Table S1). Regarding questions whether sexual and reproductive rights matters are never or always justifiable, HCPs found on average that IVF (average of 0.8 on a 0–1 scale), adoption (0.8), abortion (0.9), homosexuality (1.0), sex before marriage (0.9), underage teenage sex (0.8) and divorce (0.9) were all almost always justifiable. Likewise, parents spanking their children and gender-based violence were universally considered never justifiable with averages of 1.0 on both items on a reversed scale. More mixed results were recorded for commercial surrogacy (0.4) and prostitution (0.2).
There was even less variation in answers relating to gender equality values. HCPs strongly disagreed to statements that one should prioritize boys’ university education (1.0) and men’s right to work (1.0), and that men are better political leaders than women (1.0). HCPs also expressed low anti-immigrant sentiments, wanting to allow more migrants of different race/ethnicity to live in Sweden (0.9), and thinking that migrants enrich Swedish culture (0.8) and make the country a better place to live in (0.7).
Religion was measured in two ways. First, a self-estimation of religiosity, originally on a scale with seven steps, ranging from extremely non-religious to extremely religious, and second, regarding membership in a church or religious denomination. On average, HCPs defined themselves as neither religious nor non-religious (0.4). About 71% were not members of any denomination. In addition to non-affiliation, membership in the Church of Sweden was most common, while other Christian and other denominations were quite rare.
Comparison Between HCPs and the Swedish Population
The second research question concerns HCPs values in relation to the Swedish population. As previously noted, HCPs have a particular demographic composition that might be correlated with their values, therefore, we created the representative Swedish sub-sample of highly educated women no older than 67 as a comparison. Consistent with previous research on correlation between demographic characteristics with social values [28–30], there are clear differences between average Swedish values and the values of the sub-sample regarding sexual and reproductive rights, gender equality and migration (Figure 1). T-tests reveal that the difference in average values is statistically significant (p < 0.001, Supplementary Table S3) for everything but gender-based violence and spanking children, with the sub-sample being more permissive of issues in sexual and reproductive rights, more for gender equality, and less anti-immigrant.
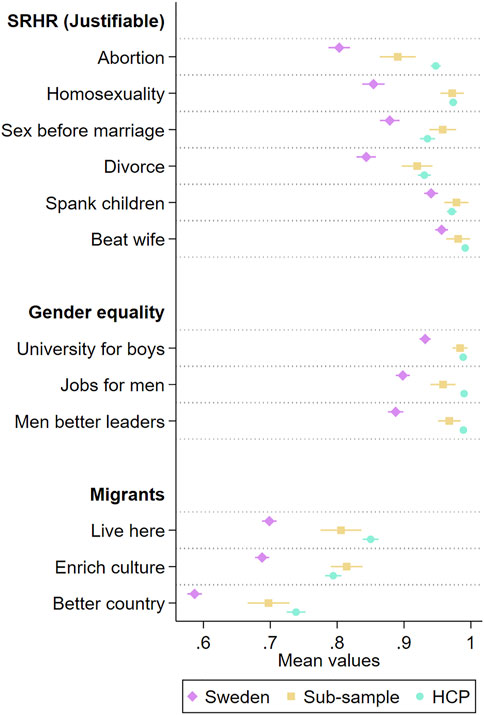
FIGURE 1. Values in relation to sexual and reproductive rights, gender equality and migration for the Swedish population, a sub-sample of highly educated women no older than 67, and healthcare providers in sexual and reproductive healthcare. Average values with 95 percent confidence intervals. MigraMed Healthcare Providers Study, Sweden, 2021.
Comparing the sub-sample and HCPs across these issues, only abortion stands out where HCPs have different values than expected given their demographic composition. On the question whether abortion is justifiable, HCPs have a higher value. For all other issues, there are no real differences.
In contrast to the measures of social values, there is no difference in either membership or religiosity between the general Swedish population and the sub-sample (Figure 2; Supplementary Table S3). Seventy percent of the Swedish population and 68% of the sub-sample are members in a religious denomination and both samples have an average religiosity of 3.2.
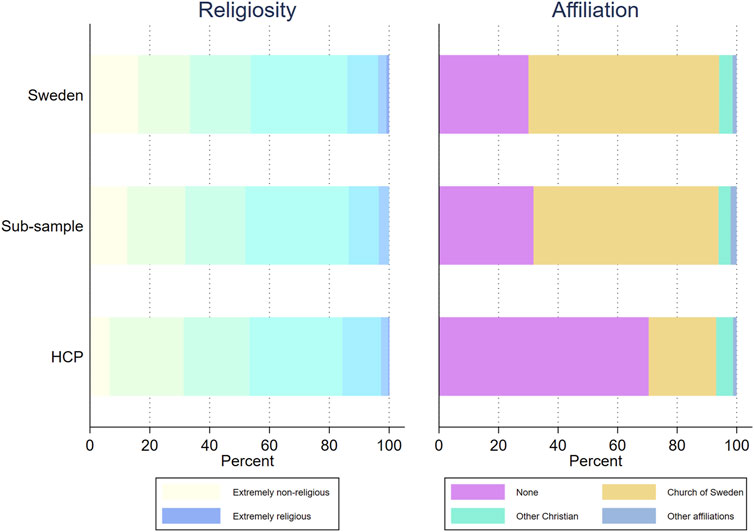
FIGURE 2. Religiosity and religious affiliation for the Swedish population, a sub-sample of highly educated women no older than 67, and healthcare providers in sexual and reproductive healthcare. MigraMed Healthcare Providers Study, Sweden, 2021.
Comparing all three samples, HCPs have a very similar distribution as the other two for religiosity. However, as an unexpected result, they are in stark contrast regarding religious membership, particularly HCPs’ lower degree of membership in Church of Sweden.
The Relationship Between Profession and Values
The results indicate that HCPs have largely the expected values given their demographic composition, with two exceptions. First, they find abortion even more justifiable than the already high value among the sub-sample, and second, they are largely less members in a religious denomination. These differences can be caused by both a causal mechanism, i.e., having a profession and being at a workplace affects values, and selection, i.e., specific individuals choosing or being selected for these professions and workplaces based on personal values they already had.
We test these causes by analysing whether there is variation in abortion values and religious affiliation across clinical years. While it is not possible to make a direct test of causality with our cross-sectional sample, clinical years can function as an indirect test of change over time. That is, if there is a causal effect of profession and workplace, there should be a correlation between, on the one hand, clinical years and, on the other, values and affiliation, with more senior HCPs finding abortion to be more justifiable and the least have a religious affiliation.
For abortion values, Figure 3 contains the results from a LOWESS. The result is that no such correlation with time exists, and respondents found on average abortion to be equally justifiable regardless of years in the profession. For religious affiliation, Figure 4 displays predicted probabilities of each affiliation over clinical years after a multinomial logistic regression with clinical years and clinical years squared as independent variables (results in Supplementary Table S4). Results indicate some variation over clinical years, but nothing that supports a negative relationship between affiliation and clinical years. In both cases, the indication is that individuals with specific values of abortion and religious choices are different from their demographic counterparts already at the start of their professional careers, i.e., are selected into these professions.
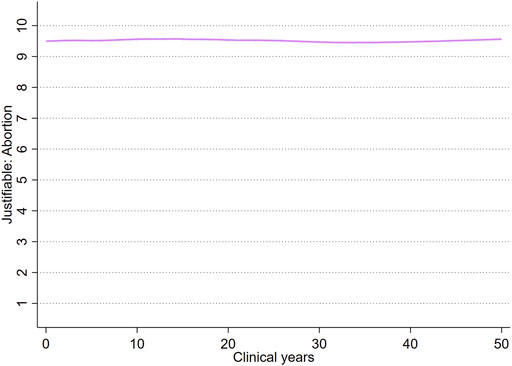
FIGURE 3. Locally weighted scatterplot smoothing (LOWESS) of Justifiable: abortion values over clinical years. MigraMed Healthcare Providers Study, Sweden, 2021.
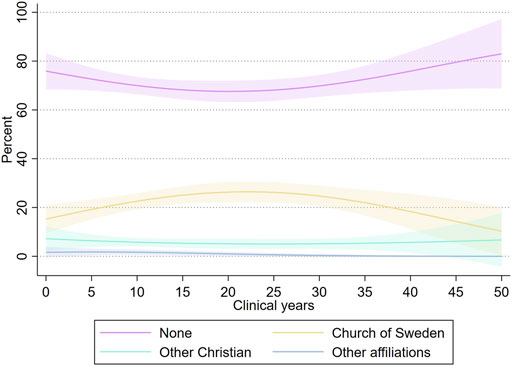
FIGURE 4. Predicted probability with 95 percent confidence intervals from robust standard errors of religious affiliation over clinical years. MigraMed Healthcare Providers Study, Sweden, 2021.
Discussion
This is the first large-scale values survey conducted in Swedish sexual and reproductive healthcare. The study highlights complex relationships between individual and professional values. In theory, HCPs as individuals may choose to follow the hospital’s policy despite subjective values contrary to healthcare’s norm system. Our major findings demonstrate high homogeneity in liberal values among HCPs. Thus, there is a strong correlation between HCPs’ personal values and Swedish healthcare’s policies on gender equality and equal care. We conclude that HCPs in sexual and reproductive healthcare share a professional ethos of written and unwritten rules prioritizing gender equality and liberal values in relation to sexual and reproductive rights, religion and migration, i.e., they did not hold anti-immigrant views.
Longitudinal results of WVS and EVS suggest that “individual choice norms,” such as acceptance of gender equality, divorce, abortion and homosexuality, change faster than other values [5]. The change from traditional “pro-fertility norms,” emphasizing traditional gender roles and linking sexual behaviour to reproduction, towards individual choice norms is fastest in high-income societies [5]. Sweden is a forerunner in this trend by having the most liberal and individualistic sexual and reproductive rights and gender equality values in international comparison [5].
As an extended analysis of abortion values and religious affiliation, the comparison group was changed based on occupation instead of demography, comprising HCPs in outpatient and inpatient care in all fields of medicine and coded based on occupational codes (ISCO) in the two relevant data sources. In accordance with the main analysis, HCPs working within sexual and reproductive healthcare stand out in their permissiveness towards abortion and religious non-affiliation, implying a specific connection to the chosen workplace and not only the medical professions (Supplementary Tables S5, S6).
The difference in abortion values between the sub-sample and HCPs is intuitive. In general, HCPs in sexual and reproductive healthcare are expected to have the same position to, e.g., homosexuality, divorce or migrants as the demographically similar sub-sample. However, they have a different relationship to abortions based on their profession and workplace. Previous research has found that HCPs and medical students objecting to abortion or contraceptive counselling are not employed in Swedish sexual and reproductive healthcare due to the policy ban on conscientious objection, but they can usually find work in another field of medicine [3]. In addition to self-selection whether to work in sexual and reproductive healthcare, this may explain why HCP’s abortion values are more liberal compared to the Swedish population and the sub-sample. Another explanation is that clinical work may increase abortion permissiveness in Swedish sexual and reproductive healthcare with its strong gender equality policy [6, 7]. However, our findings demonstrated no variation in abortion values in relation to clinical years. For future research, longitudinal results are required to determine which explanation is correct.
Of the survey questions that we constructed, the distribution of answers about adoption and underage teenage sex follow the liberal pattern for other values, while results for questions about surrogacy and prostitution (selling sex) differ. Attitudes to surrogacy and prostitution are paradoxical in the Swedish context. Despite cross-border surrogacy being increasingly common among Swedes, arguments about women’s reproductive and bodily autonomy are used in public debates to criticise surrogacy as exploitation, which also is one of the arguments against selling sex [31, 32]. HCPs in sexual and reproductive healthcare had very permissive attitudes towards IVF, but in line with previous research, they had mixed attitudes towards surrogacy, which has never been practiced in Swedish healthcare [33, 34]. A previous survey found that 63% of physicians in Swedish sexual and reproductive healthcare were positive or neutral towards permitting altruistic surrogacy in healthcare, but 60% agreed that surrogacy involves exploitation of women’s bodies [33]. Prostitution is difficult to define with our definition of liberal social values, because both higher and lower values can be liberal depending on arguments used for each position. Sweden was a pioneer in 1999 through the enactment of a law criminalizing sex purchase [35]. Previous research suggests that criminalization of sex purchase has broad societal support, while attitudes to selling sex are mixed in Sweden [35, 36].
Religiosity has during recent decades declined in most high-income countries [5]. Sweden’s population is religiously diverse due to immigration. However, membership in the Church of Sweden remains high despite Sweden’s low levels of religiosity in terms of beliefs [37, 38]. Our comparative results show low levels of religiosity among HCPs within sexual and reproductive healthcare as well as in the Swedish population, but a significantly smaller proportion of the HCPs are members of Church of Sweden. This low propensity to be religiously affiliated did not vary much across clinical years, which again indicates a selection mechanism at work.
Previous research suggests that person-centeredness correlates well with multiculturalist ideologies emphasizing religious and cultural diversity, but conflicts may emerge between promotion of cultural sensitivity and gender equality [6]. Hence, in sexual and reproductive healthcare, HCPs’ homogeneity in liberal values and their incorporation of gender equality perspectives may contribute to tensions in healthcare encounters with migrants from countries with different values. Reflexivity can help HCPs to observe and question taken-for-granted assumptions in clinical encounters [6, 39]. Reflecting on one’s own values is the first step in counteracting conflicts in healthcare encounters. To ensure equal care, HCPs need self-reflexivity about their own values when encountering migrants, and their presumed more restrictive values in relation to sexual and reproductive rights and equality. They also need to reflect on where the limit goes between accommodating differences and providing equal treatment. This is especially important given that HCPs have very liberal values in comparison to their patients and society. Our results pointing towards a selection mechanism based on values and religious affiliation indicate that recruiting healthcare students with religious conservative ideas may entail a future challenge. Further studies are necessary to investigate value conflicts in healthcare encounters and the impact of migration on HCPs’ values.
Strengths and Limitations
The benefits of the study were a large sample size (n = 1,041) and consistent results in comparisons of HCPs in sexual and reproductive healthcare, the general Swedish population and the sub-sample. Due to the non-probability sample and lack of longitudinal data, our study focuses on descriptive results and makes few causality claims. However, the analyses of abortion values and religious affiliation all point to a selection into the specific combination of professions and workplace as the main mechanism for the difference HCPs and their demographic peers. Our sample has different coverage rates between the included professions and an underrepresentation of HCPs who had immigrated; 12% in the sample compared to approximately 23% in Sweden [40]. In values surveys, there is also a risk of social desirability bias. The underrepresentation of immigrants and possible bias risks the answerers of being too liberal. We have not explicitly tested for the magnitude of this possibility. However, the fact that there was strong alignment in values between the respondents and the Swedish sub-sample implies that there is no great bias present in the data.
Conclusion
Our findings demonstrate that HCPs in Swedish sexual and reproductive healthcare share a professional ethos emphasizing gender equality, and are homogeneous in their secular liberal values in relation to sexual and reproductive rights, gender equality, migration and religion. They did not hold anti-immigrant views and had zero tolerance to gender-based violence and child spanking. Compared to the Swedish population, HCPs displayed even more liberal social values. Their values correspond to Swedish women of similar demographic background, with the exception of having more liberal abortion values and being less religiously affiliated. The results point towards a selection mechanism of individuals with very liberal values choosing or being selected to work in Swedish sexual and reproductive healthcare. Hence, HCPs need self-reflexivity to provide culturally sensitive care and to avoid conflicts in clinical encounters in a diversified society.
Ethics Statement
The studies involving human participants were reviewed and approved by the Regional Ethical Committee, Uppsala, Sweden (Dnr 2018/425) The Swedish Ethical Review Authority, Sweden (Dnr 2020-07187). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
BE and PS had the original idea. IV was responsible for survey design. LE and BE conducted data collection. AT was responsible for statistical analysis. LE and AT wrote the first draft of the manuscript. All authors contributed to interpretation of data and manuscript writing.
Funding
The authors declare that this study received funding from the Swedish Research Council (2018-03365) and the Swedish Research Council for Health, Working Life and Welfare (2014-4576). The funders were not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank all HCPs who answered or distributed the questionnaire, despite the challenging work situation in healthcare during the COVID-19 pandemic. We are especially grateful to the Swedish Association of Midwives and the Swedish Society Obstetrics and Gynecology, which contributed with distribution of the questionnaire and several reminders to their members. We also thank Soorej Jose Puthoopparambil for his valuable contribution, particularly by aiding in the development of the questionnaire and supervising a pilot study.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.ssph-journal.org/articles/10.3389/ijph.2022.1605000/full#supplementary-material
References
1.ICPD Programme of Action. Programme of Action Adopted at the International Conference on Population and Development. New York City, US: UN Population Fund (1994).
2. Starrs, AM, Ezeh, AC, Barker, G, Basu, A, Bertrand, JT, Blum, R, et al. Accelerate Progress-Sexual and Reproductive Health and Rights for All: Report of the Guttmacher- Lancet Commission. The Lancet (2018). 391:2642–92. doi:10.1016/s0140-6736(18)30293-9
3. Fiala, C, Gemzell Danielsson, K, Heikinheimo, O, Guðmundsson, JA, and Arthur, J. Yes We Can! Successful Examples of Disallowing 'conscientious Objection' in Reproductive Health Care. Eur J Contraception Reprod Health Care (2016). 21:201–6. doi:10.3109/13625187.2016.1138458
4. Ramondetta, L, Brown, A, Richardson, G, Urbauer, D, Thaker, PH, Koenig, HG, et al. Religious and Spiritual Beliefs of Gynecologic Oncologists May Influence Medical Decision Making. Int J Gynecol Cancer (2011). 21:573–81. doi:10.1097/igc.0b013e31820ba507
5. Inglehart, RF, Ponarin, E, and Inglehart, RC. Cultural Change, Slow and Fast: The Distinctive Trajectory of Norms Governing Gender Equality and Sexual Orientation. Soc Forces (2017). 4:1313–40. doi:10.1093/sf/sox008
6. Arousell, J, Carlbom, A, Johnsdotter, S, Larsson, EC, and Essén, B. Unintended Consequences of Gender Equality Promotion in Swedish Multicultural Contraceptive Counseling: A Discourse Analysis. Qual Health Res (2017). 27:1518–28. doi:10.1177/1049732317697099
7. Arousell, J, Carlbom, A, Johnsdotter, S, and Essén, B. Does Religious Counselling on Abortion Comply with Sweden's 'Women-Friendly' Abortion Policies? A Qualitative Exploration Among Religious Counsellors. Sex Cult (2019). 23:1230–49. doi:10.1007/s12119-019-09614-6
8. Ahlberg, BM, Hamed, S, Bradby, H, Moberg, C, and Thapar-Björkert, S. "Just Throw it behind You and Just Keep Going": Emotional Labor when Ethnic Minority Healthcare Staff Encounter Racism in Healthcare. Front Sociol (2022). 6:741202. doi:10.3389/fsoc.2021.741202
9. Esscher, A, Binder-Finnema, P, Bødker, B, Högberg, U, Mulic-Lutvica, A, and Essén, B. Suboptimal Care and Maternal Mortality Among Foreign-Born Women in Sweden: Maternal Death Audit with Application of the 'migration Three Delays' Model. BMC Pregnancy Childbirth (2014). 14:141. doi:10.1186/1471-2393-14-141
10. Essén, B, Bödker, B, Sjöberg, N-O, Langhoff-Roos, J, Greisen, G, Gudmundsson, S, et al. Are Some Perinatal Deaths in Immigrant Groups Linked to Sub-optimal Perinatal Care Services? Br J Obstet Gynaecol (2002). 109:677–82. doi:10.1111/j.1471-0528.2002.01077.x
11. Byström, M, and Frohnert, P. Invandringens Historia – Från ”folkhemmet” till Dagens Sverige [The History of Immigration – from the “People’s home” to Today’s Sweden]. Delmi kunskapsöversikt (2017). 5:127.
12. Malmusi, D. Immigrants' Health and Health Inequality by Type of Integration Policies in European Countries. Eur J Public Health (2015). 25:293–9. doi:10.1093/eurpub/cku156
13. Borevi, K. Multiculturalism and Welfare State Integration: Swedish Model Path Dependency. Identities (2014). 21:708–23. doi:10.1080/1070289x.2013.868351
14. Svensson, P, Carlzén, K, and Agardh, A. Exposure to Culturally Sensitive Sexual Health Information and Impact on Health Literacy: a Qualitative Study Among Newly Arrived Refugee Women in Sweden. Cult Health Sex (2017). 19:752–66. doi:10.1080/13691058.2016.1259503
15.National Board of Health and Welfare. Att Mötas I Hälso- Och Sjukvård. In: Ett utbildningsmaterial för reflektion om bemötande och jämlika villkor [Encounters in healthcare. An education material for reflection about encounters and equal conditions]. Stockholm: Socialstyrelsen (2015). p. 124.
16. Fiala, C, and Arthur, JH. "Dishonourable Disobedience" - Why Refusal to Treat in Reproductive Healthcare Is Not Conscientious Objection. Woman - Psychosomatic Gynaecol Obstet (2014). 1:12–23. doi:10.1016/j.woman.2014.03.001
17. Lennerhed, L. Kvinnotrubbel. Abort I Sverige 1938–1974 [Women Trouble. Abortion in Sweden 1938–1974]. Möklinta: Gidlunds förlag (2017). p. 208.
18. Jülich, S. Picturing Abortion Opposition in Sweden: Lennart Nilsson’s Early Photographs of Embryos and Fetuses. Soc Hist Med (2018). 2:278–307. doi:10.1093/shm/hkv114
19.SOU 1972: 39 [Swedish Government Official Report]. Abortfrågan. Remissyttranden Över 1965 Års Abortkommittés Betänkande Rätten till Abort (SOU 1971: 58) [The Abortion Issue. Statements on the 1965 Abortion Committee’s Report the Right to Abortion] (1972). https://lagen.nu/sou/1972:39?attachment=index.pdf&repo=soukb&dir=downloaded (Accessed January 18, 2022).
20. Lennerhed, L. No Backlash for Swedish Women? the Right to Abortion on Demand, 1975–2000. J Mod Eur Hist (2019). 3:326–36. doi:10.1177/1611894419854681
21. De Zordo, S, Mishtal, J, and Anton, L. Introduction. In: De Zordo, S, Mishtal, J, and Anton, L, editors. A Fragmented Landscape: Abortion Governance and Protest Logics in Europe. New York/Oxford: Berghahn (2017). p. 1–19.
22.International Maternal and Reproductive Health and Migration (IMHm). Health Care Providers’ Values and Knowledge about Sexual and Reproductive Health and Migration: Documentation and Codebook. Uppsala, Sweden: Department of Women’s and Children’s Health, Uppsala University (2022).
23.European Social Survey 2002 (ESS2002). Data from: ESS Round 1: European Social Survey Round 1 Data. Data file edition 6.6. Bergen, Norway: NSD - Norwegian Centre for Research Data, Norway – Data Archive and distributor of ESS data for ESS ERIC (2002).
24.European Values Study 2017 (EVS2017). Data from: EVS (2020): European Values Study 2017: Integrated Dataset (EVS2017). GESIS Data Archive. Cologne. ZA7500 Data file Version 4.0.0 (2020).
25.International Social Survey Programme 2018 (ISSP2018). Data from: ISSP Research Group (2020): International Social Survey Programme: Religion IV - ISSP 2018. GESIS Data Archive, Cologne. ZA7570 Data file Version 2.1.0 (2020).
26.World Values Survey 2011 (WVS2011). In: Inglehart, R, Haerpfer, C, Moreno, A, Welzel, C, Kizilova, K, Diez-Medrano, J, et al. editors. Data from: World Values Survey: Round Six - Country-Pooled Datafile Version. Madrid: JD Systems Institute (2014).
27.National Board of Health and Welfare. Statistics on Legitimated 2019 and Labour Market Status 2018. Healthcare Professionals. Appendix: Table 3a. Total Number of Specialist Licenses Issued for Physicians and Dentists 31 December 2015–2019, Women and Men. Stockholm: Socialstyrelsen (2020).
28. Houtman, D, and Aupers, S. The Spiritual Turn and the Decline of Tradition: The Spread of Post-Christian Spirituality in 14 Western Countries, 1981?2000. J Scientific Study Religion (2007). 46:305–20. doi:10.1111/j.1468-5906.2007.00360.x
29. Weakliem, DL. The Effects of Education on Political Opinions: An International Study. Int J Public Opin Res (2002). 14:141–57. doi:10.1093/ijpor/14.2.141
30. Miller, AS, and Stark, R. Gender and Religiousness: Can Socialization Explanations Be Saved? Am J Sociol (2002). 107:1399–423. doi:10.1086/342557
31. Arvidsson, A, Johnsdotter, S, and Essén, B. Views of Swedish Commissioning Parents Relating to the Exploitation Discourse in Using Transnational Surrogacy. PLOS ONE (2015). 10(5):e0126518. doi:10.1371/journal.pone.0126518
32. Gunnarsson Payne, J. Autonomy in Altruistic Surrogacy, Conflicting Kinship Grammars and Intentional Multilineal Kinship. Reprod Biomed Soc Online (2018). 7:66–75. doi:10.1016/j.rbms.2018.10.014
33. Stenfelt, C, Armuand, G, Wånggren, K, Skoog Svanberg, A, and Sydsjö, G. Attitudes toward Surrogacy Among Doctors Working in Reproductive Medicine and Obstetric Care in Sweden. Acta Obstet Gynecol Scand (2018). 97:1114–21. doi:10.1111/aogs.13342
34. Wennberg, A-L, Rodriguez-Wallberg, KA, Milsom, I, and Brännström, M. Attitudes towards New Assisted Reproductive Technologies in Sweden: a Survey in Women 30-39 Years of Age. Acta Obstet Gynecol Scand (2016). 95:38–44. doi:10.1111/aogs.12781
35. Jakobsson, N, and Kotsadam, A. Gender Equity and Prostitution: An Investigation of Attitudes in Norway and Sweden. Feminist Econ (2011). 17:31–58. doi:10.1080/13545701.2010.541863
36. Kuosmanen, J. Attitudes and Perceptions about Legislation Prohibiting the purchase of Sexual Services in Sweden. Eur J Soc Work (2011). 14:247–63. doi:10.1080/13691451003744341
37. Furseth, I, Kühle, L, Lundby, K, and Lövheim, M. Religious Complexity in Nordic Public Spheres. Nordic J Religion Society (2019). 32:71–90. doi:10.18261/issn.1890-7008-2019-01-05
38. Kasselstrand, I. Nonbelievers in the Church: A Study of Cultural Religion in Sweden. Sociol Religion (2015). 76:275–94. doi:10.1093/socrel/srv026
39. Liberati, EG, Gorli, M, Moja, L, Galuppo, L, Ripamonti, S, and Scaratti, G. Exploring the Practice of Patient Centered Care: The Role of Ethnography and Reflexivity. Soc Sci Med (2015). 133:45–52. doi:10.1016/j.socscimed.2015.03.050
40.Statistics Sweden. Anställda (Yrkesregistret) 16-64 År Efter Yrke (SSYK 2012), Födelseregion Och År [Employees (Occupational Register) 16-64 Years by Occupation (SSYK 2012), Region of Birth and Year (2021). https://www.statistikdatabasen.scb.se/sq/114832 (Accessed October 14, 2021).
Keywords: migration, gender equality, migrant healthcare, sexual and reproductive healthcare, sexual and reproductive rights, values
Citation: Eriksson L, Tibajev A, Vartanova I, Strimling P and Essén B (2022) The Liberal Social Values of Swedish Healthcare Providers in Women’s Healthcare: Implications for Clinical Encounters in a Diversified Sexual and Reproductive Healthcare. Int J Public Health 67:1605000. doi: 10.3389/ijph.2022.1605000
Received: 08 April 2022; Accepted: 20 June 2022;
Published: 11 July 2022.
Edited by:
Sonja Merten, Swiss Tropical and Public Health Institute (Swiss TPH), SwitzerlandReviewed by:
Prabhat Lamichhane, Deakin University, AustraliaCopyright © 2022 Eriksson, Tibajev, Vartanova, Strimling and Essén. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lise Eriksson, bGlzZS5lcmlrc3NvbkBrYmgudXUuc2U=
This Original Article is part of the IJPH Special Issue “Migration Health Around the Globe—A Construction Site With Many Challenges.”