 Silvia A. González1,2*
Silvia A. González1,2* Olga L. Sarmiento3Alberto Florez-Pregonero4Peter T. Katzmarzyk5Jean-Philippe Chaput2,6Mark S. Tremblay2,6
Olga L. Sarmiento3Alberto Florez-Pregonero4Peter T. Katzmarzyk5Jean-Philippe Chaput2,6Mark S. Tremblay2,6- 1School of Epidemiology and Public Health, Faculty of Medicine, Ottawa, ON, Canada
- 2Healthy Active Living and Obesity Research Group, Children's Hospital of Eastern Ontario Research Institute, Ottawa, ON, Canada
- 3School of Medicine, Universidad de los Andes, Bogotá, Colombia
- 4School of Education, Pontificia Universidad Javeriana, Bogotá, Colombia
- 5Pennington Biomedical Research Center, Baton Rouge, LA, United States
- 6School of Epidemiology and Public Health, Faculty of Medicine, University of Ottawa, Ottawa, ON, Canada
Objectives: Excessive recreational screen time (RST) is associated with detrimental effects for physical, psychological and cognitive development. This article aims to describe the prevalence of excessive RST among Colombian preschoolers, children and adolescents and explore its factors associated.
Methods: We analyzed data from the National Survey of Nutrition 2015. The sample included 4,503 preschoolers, 5,333 school-aged children and 6,623 adolescents. Poisson regression models with robust variance were conducted to estimate prevalence ratios and determine associated factors of excessive RST.
Results: Fifty percent of preschoolers, 61% of school-aged children and 73% of adolescents in Colombia had excessive RST. Positive associations were observed with the availability of TV in the child’s bedroom, the availability of video games at home, and eating while using screens. A negative association with rural area was observed for all age groups.
Conclusion: The majority of Colombian children and adolescents have excessive RST. Younger preschoolers, older school-aged children, wealthiest children and those from urban areas should be targeted by interventions to decrease RST. These interventions should promote limiting the availability of electronic devices in children’s bedrooms and not eating in front of screens.
Introduction
Sedentary behavior, defined by the Sedentary Behavior Research Network as “any waking behavior characterized by an energy expenditure ≤1.5 metabolic equivalents (METs), while in a sitting, reclining or lying posture” [1] has been identified as an important risk factor for poor health. Excessive time spent in sedentary behaviors, mainly recreational screen time (RST), has been associated with detrimental effects on health and development in children including unfavorable body composition, lower fitness, higher cardiometabolic risk scores, greater energy intake and poorer diet quality, lower measures of self-esteem and prosocial behaviors, lower quality of life and lower academic achievement [2–5]. Concerningly, there is a large proportion of children and adolescents around the world who spend excessive time in sedentary pursuits, and may have a higher risk of those conditions [6, 7].
The high prevalence of excessive sedentary time globally is likely a result of greater access to labor-saving technologies, motorized vehicles and screen-based entertainment which have led to a shift from active lifestyles to greater involvement in activities that require lower energy expenditure [4, 8]. In response to this situation, countries like Canada and Australia, and recently the World Health Organization, have developed public health guidelines to promote a reduction in sedentary behaviors [5, 9, 10]. These guidelines focus their message on the reduction of RST such as watching TV, playing videogames or using computers or tablets for non-school related purposes, as these are some of the main sedentary behaviors with important implications for health [4]. Using the cut-off point of Australian and Canadian sedentary behavior guidelines for children and adolescents, global data indicate that the prevalence of meeting sedentary behavior guidelines ranges from 7% in Estonia and China to 85% in Bangladesh [6, 11–13].
An important element to advance in the design of interventions to reduce sedentary behaviors is to identify the main factors positively or negatively associated to these behaviors. Sedentary behaviors can be driven by factors from multiple environments or at different levels of influence, therefore, these factors can be better understood and addressed from a context-specific approach, such as a socio-ecological framework of health behaviors [14]. The socio-ecological model applied to sedentary behaviors states that there are characteristics or variables at the individual, social, organizational/community, environmental, and policy level that can influence these behaviors [14]. Using a socio-ecological approach, a systematic review identified certain consistent positively associated factors at the individual, interpersonal and environmental levels, such as age, weight, Afro-American ethnicity, food consumption in front of the TV and built environment variables such as playground density and greater access to play and sports infrastructure [15]. However, the associations with sex and socioeconomic status found in this review were inconsistent, and evidence from low- and middle-income countries was absent.
In Colombia, screen time has been included as a relevant indicator for nutrition surveillance since 2005 [16], and its assessment has evolved over time. In the first version of the National Survey of Nutrition (ENSIN for its name in Spanish), screen time was assessed among 5–12 year-old children as TV viewing and videogame use [17]. In the 2010 survey, the same indicator was included and extended to adolescents aged 13–17 years [18]. For the most recent 2015 survey the indicator was modified to include time spent using other devices such as tablets, portable videogame devices and mobile phones for recreational purposes, and extended the population of interest to include preschool children in addition to the previously included age groups. Therefore, this is the first study in Colombia and among the first in Latin America that examines engagement in excessive RST in a nationally representative sample of pre-schoolers, children and adolescents between 3 and 17 years old. To the best of our knowledge, this is the first time that 2015 ENSIN data on RST among children and adolescents is presented. This initial approach to a broader range of recreational screen-based activities in a national sample with a larger age range provides a unique opportunity to help inform public health policies that contribute to decrease sedentary behavior in Colombia. In this context, this paper aims to describe the prevalence of excessive RST among Colombian preschoolers, children and adolescents and explore the factors associated with excessive RST within a socio-ecological framework.
Methods
Study Design and Participants
We analyzed data from the sedentary behavior component of ENSIN 2015. ENSIN is a cross-sectional population health survey with national representativeness of urban and rural areas of Colombia [19]. The sample of this survey was selected with a stratified, multistage probability cluster sampling design. The sub-sample for the sedentary behavior component included 4,503 preschoolers (3–5 years), 5,333 school-aged children (6–12 years) and 6,623 adolescents (13–17 years). The survey was administered by the Colombian Institute of Family Welfare.
Data Collection
Data were collected by trained nutritionists in the household setting between December 2015 and November 2016, using computer-assisted personal interview technology with a data collection system specifically designed for ENSIN. Data collection teams were regularly accompanied by researchers for quality control purposes. For preschoolers and school-aged children, one of the parents or the main caregiver responded to the survey, while adolescents self-reported their responses. Parents provided signed informed consent and children between 12 and 17 years provided informed assent before conducting the survey. The ENSIN protocol was approved by the Profamilia Institutional Review Board on Research involving Human Subjects and the Colombian National Institutes of Health (file number 2-2015, 26 February 2015). The secondary data analyses were approved by the University of Ottawa (file number H-06-19-3564). Data collection details according to the type of variables (dependent vs. potential associated factors) are described below.
Dependent Variables
Among preschoolers, RST was assessed with the Questionnaire for the Measurement of Physical Activity and Sedentary Behaviors in preschool to fourth grade children (C-MAFYCS), which has low internal consistency for the sedentary behavior scale (Cronbach’s alpha = .31) and moderate to good reproducibility mainly for items such as computer and videogame use (Kappa = .71 and .62, respectively) [20]. Engagement in screen-based activities was assessed with three questions: “During the last 7 days, did (name of the child) watch television, movies or videos in the TV? During the last 7 days, did (name of the child) play or listen to music in the computer? And during the last 7 days, did (name of the child) play with consoles such as X-Box, Play-Station, manual videogames such as Nintendo DS, etc., play with a cellphone, smartphone, iPad or other tablets?” Each of these questions was informed with the amount of time spent in each activity with the following questions: How much time did he/she spend on weekdays? And how much time did he/she spend on weekends? (for each day) The total time in all screen-based activities per weekdays and weekend days was estimated in minutes and the average screen time per day, per weekday and per weekend day was calculated. A dichotomous variable to indicate if the preschooler achieved excessive RST was calculated (excessive vs. not excessive RST). Excessive RST was defined as engaging in more than 1 h of RST per day among preschoolers under 5 years of age or more than 2 h of RST per day among 5-year-olds, in accordance with the WHO and the Canadian sedentary behavior guidelines [9, 21].
Among school-aged children and adolescents, RST was assessed with the following questions adapted from the US Youth Risk Behavior Surveillance System (YRBSS) [22]: “On an average school day or weekday, how many hours did (name of the child)/you watch TV?; On an average school day or weekday, how many hours did (name of the child)/you play video games or use a computer for something that is not schoolwork?; On a weekend day, how many hours did (name of the child)/you watch TV? And, on a weekend day, how many hours did (…) play video games or use a computer for something that is not schoolwork?” The question inquiring about videogames and computer use included the following examples of devices and activities to consider: Xbox, PlayStation, iPod, iPad or other tablet, smartphone, cellphone, YouTube, Facebook or other social media and internet. The response options were: 1) Did not watch TV/played videogames or used the computer, 2) less than 1 h, 3) between 1 and 1:59 h, 4) between 2 and 2:59 h, 5) between 3 and 3:59 h, 6) between 4 and 4:59 h, and 7) 5 h or more. A screen time score was calculated converting these categories as follows: 1 and 2 = 0 h, 3 = 1 h, 4 = 2 h, 5 = 3 h, 6 = 4 h and 7 = 5 h. With these values we calculated a weighted mean score of daily screen time, as previously estimated in other studies [23]. A dichotomous variable to indicate excessive RST was created using a cut-off of more than 2 h of screen time, according to the sedentary behavior guidelines in the Canadian 24-h movement guidelines [9].
Potential Associated Factors
We selected variables that were potentially relevant for the analysis of RST at different levels according to the socio-ecological framework of sedentary behaviors [14].
Intrapersonal Level
Sex (female vs. male), age, ethnicity (Afro-Colombian vs. Indigenous vs. Other ethnic identity), overweight (yes vs. no), physical activity program participation (yes vs. no), physical activity (meeting vs. not meeting the WHO physical activity guidelines), and food frequency consumption variables (yes vs. no) were included at the individual level. Sociodemographic variables (i.e., sex, age, ethnicity) were measured with the Household Questionnaire designed for ENSIN [19]. Overweight (including obesity) was ascertained based on body mass index, calculated from objective measurements of height and weight, and categorized according to WHO growth standards and reference tables [24, 25]. Physical activity program participation (organized activities, sports clubs, and Ciclovías for school-aged children and adolescents, and programs at the school and community levels among adolescents) was assessed with questions designed for the Physical Activity and Sedentary Behavior Questionnaire for ENSIN [19]. Physical activity was proxy-reported (by parents or caregivers) for pre-schoolers and school-aged children and self-reported by adolescents. For pre-schoolers, physical activity was assessed with the C-MAFYCS questionnaire, and for school-aged children and adolescents it was assessed with a question adapted from the YRBSS. A dichotomous variable to indicate if the child/adolescent met the physical activity guidelines was created, using a cut-off of 180 min of physical activity per day with at least 60 min of energetic play for preschool children, and 7 days of being active at least 60 min per day for school-age children [26]. More details on the physical activity assessment are described elsewhere [27]. Food consumption variables were measured with the Food Frequency Questionnaire designed for ENSIN [19] and specific food groups were incorporated in the analysis including: charcuterie products, sodas, snacks and fried foods at least three times per week; fast food consumption at least once per week; and daily consumption of candy. We also assessed usual food consumption while using screens during the last month.
Household Level
At the household level, we included wealth index, area of residence (urban vs. rural), and TV and video game device availability in the child’s bedroom. To estimate wealth index, data on asset ownership, availability of public utilities and materials used for housing construction were collected in the socio-demographic section of the survey. Then, the index was calculated using a principal component approach and categorized into quartiles. TV and videogame availability were assessed with questions adapted from the Neighborhood Impact on Kids (NIK) survey [28].
Environmental and Community Level
At the community level we included parks availability in the neighbourhood and perceived safety in the parks, which were assessed with questions adapted from the NIK survey [28]. For the natural environment level, we included the geographic region where the children lived at the time of the survey (Orinoquia-Amazonia vs. Atlantic vs. Central vs. Eastern vs. Pacific vs. Capital District).
Statistical Analysis
Descriptive statistics (means, standard deviations, and frequencies) were estimated for demographic and contextual characteristics of the sample and chi-squared tests were conducted to determine differences between groups. Poisson regression models with robust variance were conducted to estimate prevalence ratios (PR) and determine associated factors of excessive RST. Three types of models were run for each age group: 1) bivariate models with potential associated factors, 2) multivariable model 1 included the variables available for the whole sample that showed at least marginally significant associations (p < .10) and were adjusted for age and sex and 3) multivariable model 2 included the food consumption and program participation variables that had p-values <.10 in the bivariate analyses and were conducted as a sub-analysis with a smaller sample size. The reason for running two different multivariable models was that not all the participants had the same covariates available, as some components of ENSIN had different selection probabilities. Therefore, multivariable model 1 included the whole sample, and multivariable model 2 explored additional variables with the sub-sample of participants that also had food consumption and programs attendance data available. Variables with p-values <.05 in the multivariable models were considered associated factors of excessive RST. We used STATA 14.0 (StataCorp, College Station, TX, United States) for the analyses, with the survey (SVY) module for complex samples to take into account the clustering of data and the characteristics of the study design, sample weights and missing data. Respondents with missing data on the main variables of interest were excluded from the study (4 observations). Missing data on covariates are described in the footnotes for Tables 1 and 2.
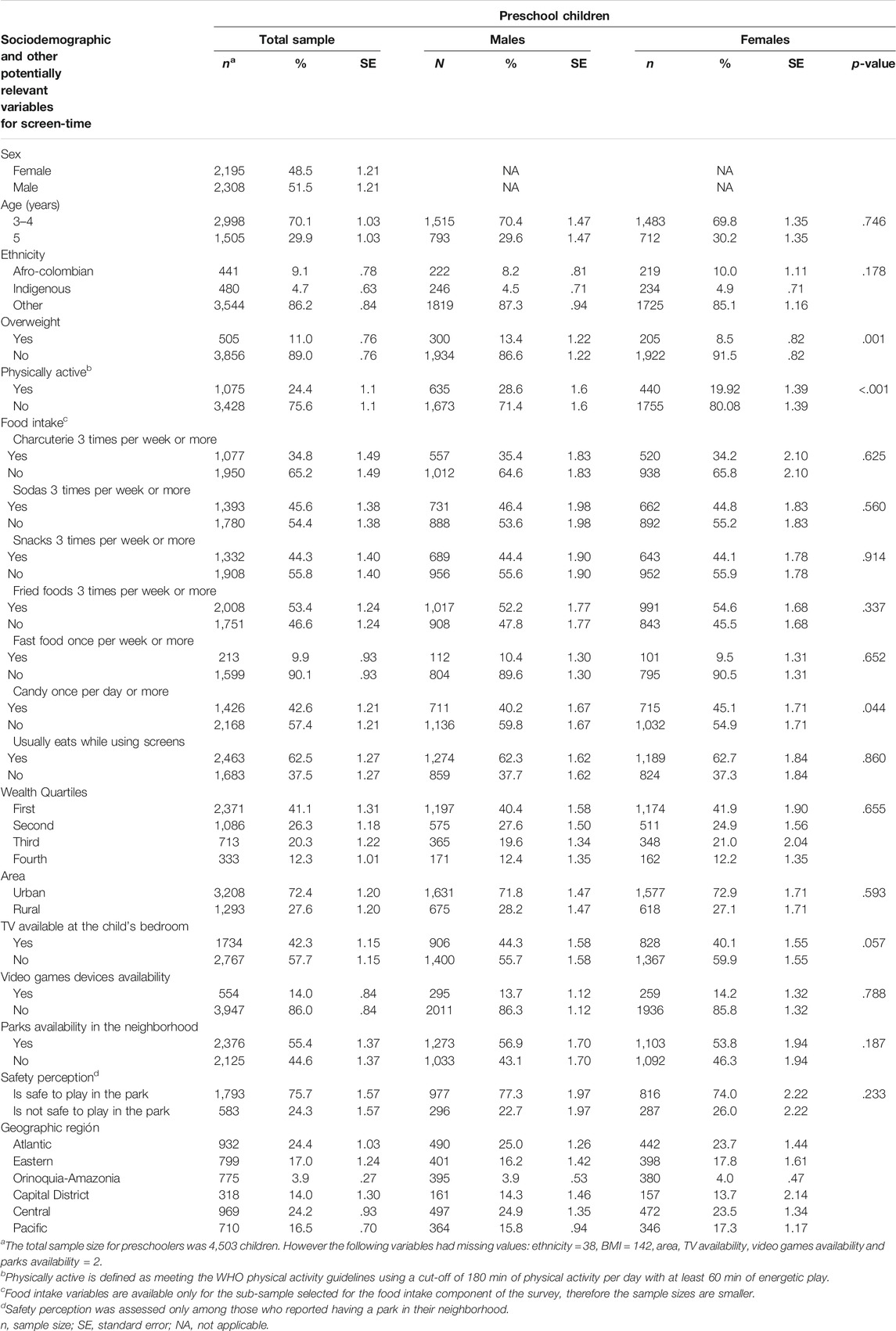
TABLE 1. Sociodemographic and lifestyle characteristics of 4,503 preschoolers from Colombia. National Survey of Nutrition, Colombia, 2015.
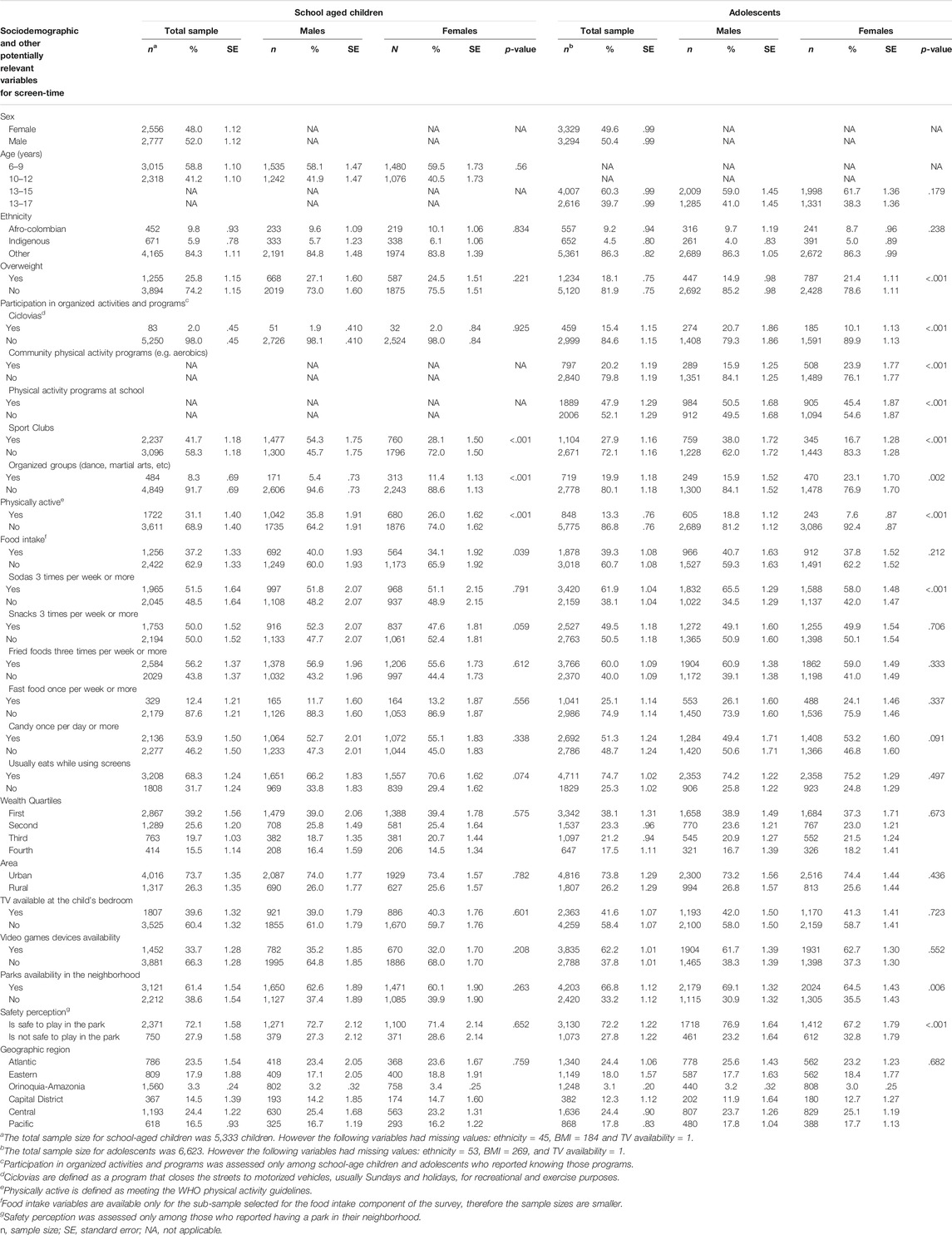
Table 2. Sociodemographic and lifestyle characteristics of 11,956 children and adolescents from Colombia. National Survey of Nutrition, Colombia, 2015.
Results
Sociodemographic characteristics of the sample and other descriptive statistics for this analysis are presented in Tables 1, 2. Approximately 48% of the sample for each age group were females. About 9% and 5% of the children and adolescents were Afro-Colombian or indigenous, respectively. Overweight prevalence was 11.0% for preschoolers, 25.8% among school-aged children, and 18.1% among adolescents. Male preschoolers had a higher prevalence of overweight compared to females, while female adolescents had a higher prevalence of overweight compared to male adolescents. Low proportions of active children were observed across all age groups and were lower among females. More than 60% of preschoolers and school-aged children, and over 70% of adolescents reported eating in front of screens. Over 70% of children and adolescents lived in urban areas, about 40% had a TV available in their bedroom, and availability of video game devices ranged from 14% among preschoolers to more than 60% among adolescents (Tables 1, 2).
Prevalence of Excessive Recreational Screen-Time
Table 3 presents the overall prevalence of excessive RST and the prevalence according to potentially relevant variables. We found that 50% of preschoolers, 61% of school-aged children and 73% of adolescents in Colombia had excessive RST (Table 3). This prevalence did not differ by sex. Among preschoolers, younger children (3–4 years) had a greater prevalence of excessive RST, while in school-aged children this prevalence was higher for older children (10–12 years). Indigenous preschoolers, children and adolescents had a lower prevalence of excessive RST. Among school-aged children, those with overweight or who were physically inactive, had greater prevalences of excessive RST.
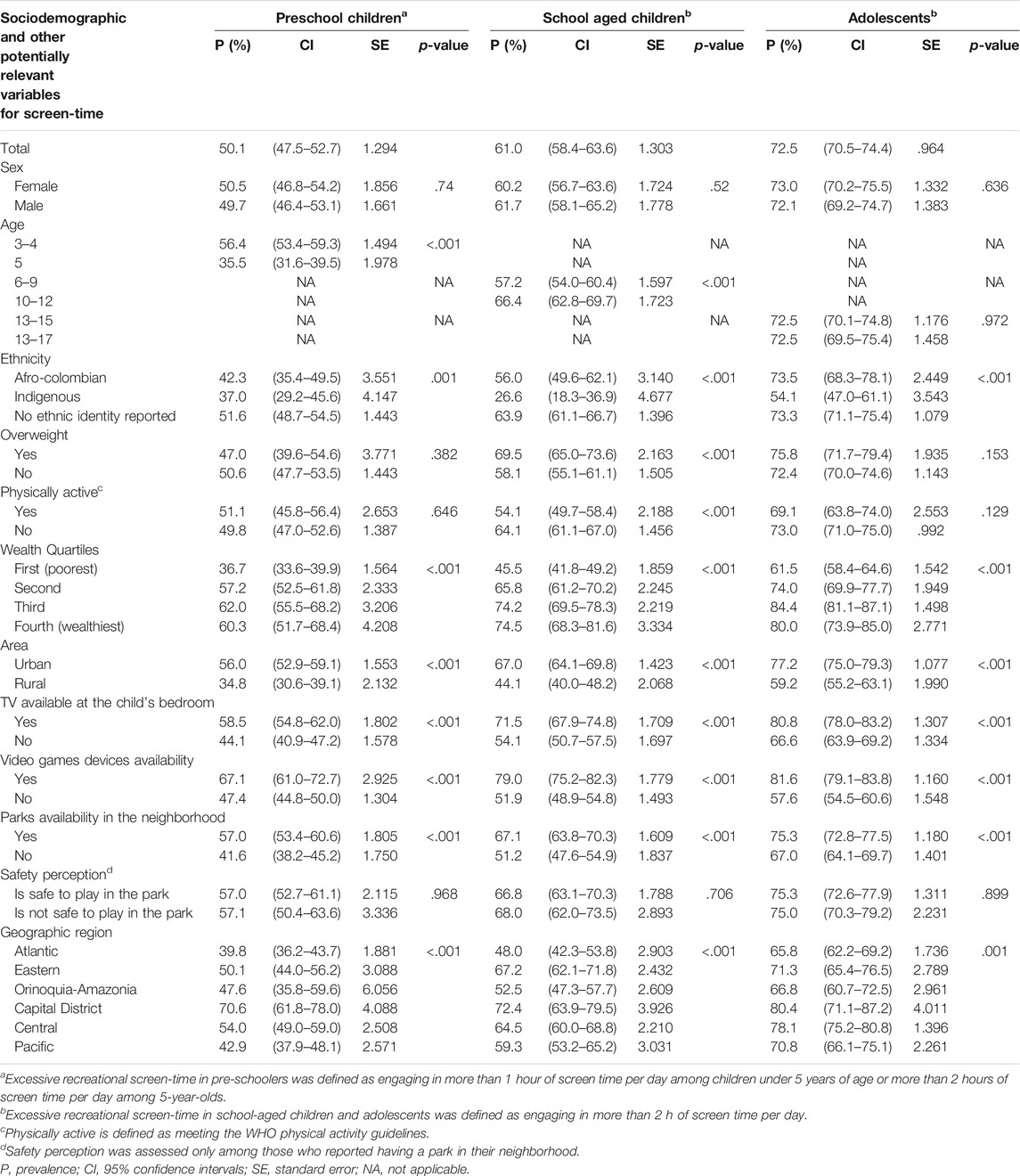
TABLE 3. Prevalence of excessive recreational screen-time among Colombian preschoolers, school-aged children and adolescents. National Survey of Nutrition, Colombia, 2015.
The prevalence of excessive RST differed by socioeconomic status, with those in the third and fourth wealth quartiles having a higher prevalence across all age groups. Also, children and adolescents from urban areas, with TV in the bedroom, video-game devices available and those with park availability in the neighborhood had higher prevalence of excessive RST. According to geographic region, children and adolescents living in the capital district had a higher prevalence of excessive RST (Table 3).
Associated Factors of Excessive Screen Time Among Preschoolers
Figure 1 and Supplementary Table 1 presents the associated factors of excessive RST among preschoolers. According to multivariable model 1, younger preschoolers (3–4 year-olds), those with TV availability in their bedroom, video-game devices available, and those with parks available in their neighbourhood were more likely to have excessive RST compared to their counterparts. Also, preschoolers in the lowest wealth quartile, those living in rural areas, and those living in the Atlantic or Pacific region were less likely to have excessive RST (Figure 1A). According to multivariable model 2, soda consumption three or more times per week and eating while using screens were positively associated with having excessive RST (Figure 1B).
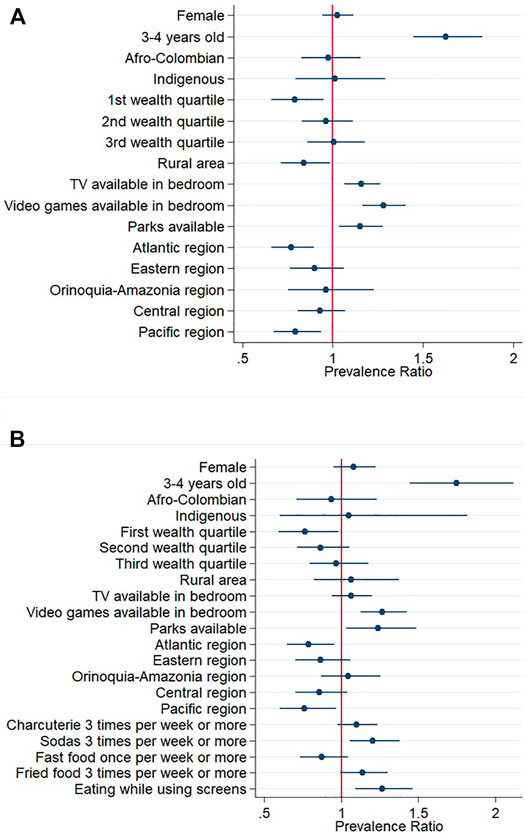
FIGURE 1. Prevalence ratios and 95% confidence intervals of associated factors of spending excessive recreational screen-time among Colombian preschoolers. Excessive screen-time was defined as spending more than 1 h of screen-time per day among children under 5 years, and engaging in more than 2 h of screen-time per day among 5-year-olds. (A) Mutivariable model 1 (B) Mutivariable model 2 including food consumption variables. Reference categories were male sex, 5 years of age, no ethnic identity reported, fourth wealth quartile, urban area, no TV availability, no video games availability, no parks availability, Capital District region, no consumption of the food items included, and no eating while using screens. National Survey of Nutrition, Colombia, 2015.
Associated Factors of Excessive Screen Time Among School-Aged Children
According to multivariable model 1, among school-aged children, those who had a TV in their bedroom or video-game device availability were more likely to have excessive RST. Younger age, Indigenous ethnicity, those in the lowest socioeconomic level, and those living in rural areas were less likely to have excessive RST (Figure 2A; Supplementary Table 2). According to multivariable model 2, there was a positive association with the usual consumption of foods in front of screens (Figure 2B; Supplementary Table 2).
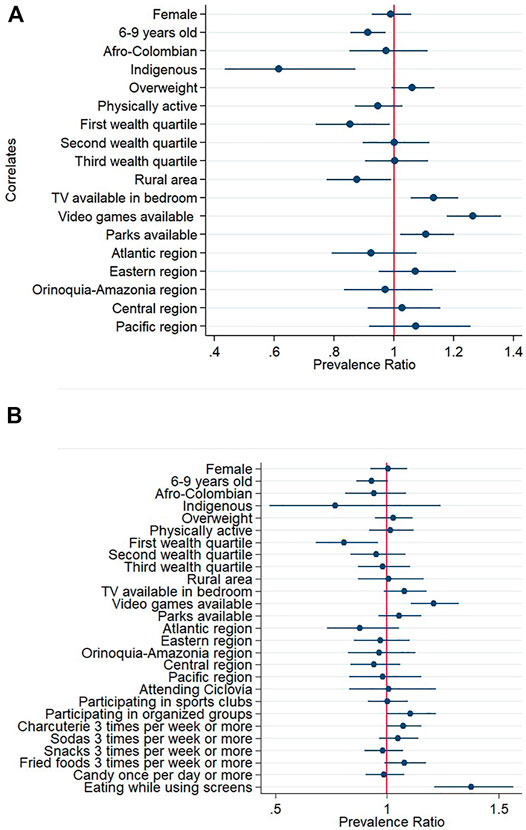
FIGURE 2. Prevalence ratios and 95% confidence intervals of associated factors of spending excessive recreational screen-time among Colombian school-aged children. Excessive screen-time was defined as spending more than 2 h of screen-time per day. (A) Mutivariable model 1 (B) Mutivariable model 2 including food consumption and program participation variables. Reference categories were male sex, 10–12 years of age, no ethnic identity reported, no overweight, not meeting physical activity guidelines, fourth wealth quartile, urban area, no TV availability, no video games availability, no parks availability, Capital District region, not attending Ciclovía, not participating in sport clubs, not participating in organized groups, no consumption of the food items included and not eating while using screens. National Survey of Nutrition, Colombia, 2015.
Associated Factors of Excessive Screen Time Among Adolescents
According to multivariable model 1, Afro-Colombian adolescents, those in the third wealth index quartile and those who had TV available in their rooms or video-games available were more likely to have excessive RST than their counterparts. On the contrary, those living in rural areas were less likely to have excessive RST than their counterparts (Figure 3A; Supplementary Table 3). Program participation variables were not associated in the bivariate models and therefore were not included in model 2. According to multivariable model 2, adolescents who usually eat in front of screens were more likely to have excessive RST (Figure 3B; Supplementary Table 3).
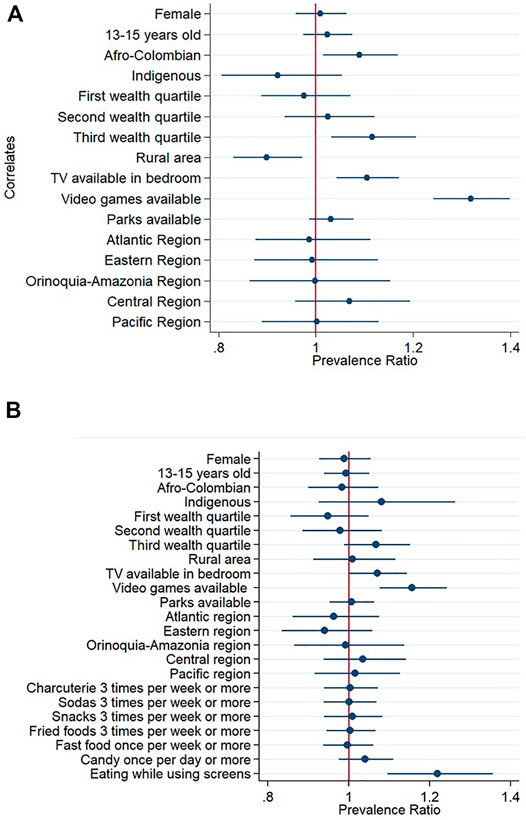
FIGURE 3. Prevalence ratios and 95% confidence intervals of associated factors of spending excessive recreational screen-time among Colombian adolescents. Excessive screen-time was defined as spending more than 2 h of screen-time per day. (A) Mutivariable model 1 (B) Mutivariable model 2 including food consumption variables. Reference categories were male sex, 16–17 years of age, no ethnic identity reported, fourth wealth quartile, urban area, no TV availability, no video games availability, no parks availability, Capital District region, no consumption of the food items included and not eating while using screens. National Survey of Nutrition, Colombia, 2015.
Discussion
Our results indicate that a large proportion of Colombian children and adolescents have excessive RST and the prevalence increases with age. Approximately five out of every 10 preschoolers, six out of every 10 school-aged children, and seven out of every 10 adolescents had excessive RST. Associated factors differed across age groups, but consistent positive associations were observed with the availability of TV in the child’s bedroom, the availability of video games, and eating while using screens. Also, a negative association with rural area was observed for all age groups. Factors at the intrapersonal, household and environmental levels are discussed below.
At the intrapersonal level RST associated factors included age, ethnicity, consumption of energy dense foods and food intake while using screens. Younger preschoolers (3–4 years old) and older school-aged children (10–12 years old) were more likely to have excessive RST. Our findings for school-aged children are consistent with other studies that have reported a positive association between age and screen time [29, 30]. However, among preschoolers, our results, which contribute to the limited studies on this population, showed an opposite association, which can be related to the fact that the sedentary behavior guidelines used as cut-offs in this analysis are stricter for younger children [31]. It is important that public health messages consider this difference in the sedentary behavior guidelines according to age. The observed associations with ethnicity suggest that children belonging to Indigenous communities use screens less and this situation should be preserved. On the contrary, Afro-Colombian adolescents showed an increased likelihood of having excessive RST, which indicates that initiatives or programs to decrease sedentary behaviors should have a special focus on this population and further research is needed to better understand the drivers of this association. Our findings for food consumption are aligned with other studies, showing that children and adolescents with excessive RST have a greater consumption of energy dense foods and drinks [32] and tend to eat their meals while using screens [32, 33]. These associations are concerning considering that these obesogenic behaviors are present at a high proportion from early ages. Specific public health messaging for parents and children should be designed not only to reduce RST but also to avoid practices like eating while watching TV or other screens. The dietary guidelines of Brazil, for example, encourage sitting with the family to eat meals in an appropriate environment paying full attention to the act of eating and without engaging in another activity [34].
At the household level, living in a rural area and electronic devices availability emerged as consistent associated factors across all age groups. The negative association with rural area was a common correlate [17, 35] that highlights the importance of focusing interventions on populations living in the continuously growing urban areas. The association of RST and sitting time with devices availability has been previously reported, mainly for school-aged children and adolescents [35–37]. In our study we observed that this is a relevant correlate from early age, which is a reason for concern considering that TV availability in the bedroom contributes to an obesogenic environment [38]. Future actions should take into account that having a TV in the bedroom and video-game availability are modifiable factors, and removing them from children’s bedrooms can contribute to limiting screen time, as demonstrated by Atkin et al. [39] in a longitudinal study. Our results also indicate that the wealthiest children and adolescents are more likely to have excessive RST than their poorer counterparts. This association was also reported in a systematic review and meta-analysis that found a positive relationship between socioeconomic level and excessive RST in adolescents form low-middle income countries, and opposite to the association observed in high income countries [40]. These different patterns in the association between RST and socioeconomic level resemble the patterns proposed by the obesity transition stages, where earlier stages are characterized by higher prevalence, in this case of obesity, among the wealthiest people and later stages show higher prevalence among those in the lowest socioeconomic status [41]. These results can suggest a lifestyle transition that require urgent action to reduce the high prevalence of RST among the wealthiest children and to prevent the increase of these behaviors among the most vulnerable ones.
At the environmental level, we did not find a statistically significant association of RST with the availability of physical activity programs. Previous evidence on Ciclovía participation, showed that children who attended this program had lower total sedentary time on sundays, however RST was not specifically assessed in this study [42]. The lack of associations observed in our results can be understood by the fact that the programs included in the survey are focused on physical activity promotion, and may indicate the need to have specific interventions or strategies aimed at reducing RST together with the already existing physical activity programs to have an impact on the children and adolescent’s movement behaviors in Colombia. In this regard, it is important to highlight that there is a lack of policies and interventions to reduce screen time among Colombian children and adolescents, as previously reported by a group of experts in the Colombian Report Card of Physical Activity [43]. We also observed a counter-intuitive positive association of excessive RST with parks availability. This finding could be related to safety conditions of the existing parks, as suggested by the non-statistically significant positive association between excessive RST and lack of safety perception observed in the bivariate analysis for preschoolers and school-aged children. In terms of geographic region, we also observed that preschoolers from the Atlantic and Pacific regions, and adolescents from the Atlantic region were less likely to have excessive RST compared to their counterparts from Bogotá (the capital district). This could be probably influenced by differences in internet accessibility and cultural norms on the use of leisure time that should be further studied.
Our estimates seem higher than the prevalence of excessive RST reported in previous versions of the ENSIN survey [17]. However, it is important to mention that our results may not be comparable, since different questionnaires have been used and the most recent version of ENSIN includes a wider range of screen-devices. In the global context, our results are similar to the engagement in RST reported by very high-income countries like Canada, Denmark, England and Qatar [6]. Having a prevalence comparable to those observed in rich countries may be indicative of the lifestyle transition that low- and middle-income countries are experiencing and reinforces the urgent need to proactively implement actions to decrease risk behaviors such as excessive RST [44]. In the current context of the COVID-19 pandemic that has drastically changed the routine and movement behaviors of children and adolescents it would be expected that the observed estimates have largely increased, as observed in other countries [45]. This adds to the urgency for the design and implementation of strategies to reduce RST. These actions should align with the call made by the WHO-UNICEF- Lancet Commission to place children as the center of the Sustainable Development Goals. Specifically, greater regulation of advertising and commercial governance to protect children from the exposure to marketing of unhealthy products and harmful contents of videogames should be priorities for decision-makers [46].
Our results should be interpreted considering strengths and limitations of the study. The main strength is that our estimates inform the situation of RST for a nationally representative sample of 3- to 17-year-old individuals from Colombia, the broadest age range evaluated at the national level, to the best of our knowledge. Also, the survey data used for this analysis provides a wide range of contextual covariates of relevance to understand the RST situation in Colombia. Limitations include the cross-sectional design of the survey, which does not allow to make causal inferences from our findings, and the use of self- and proxy-report of screen time engagement. Despite self-report being the most feasible method of assessment of RST for population surveys, it is important to recognize that this measure of screen time can be influenced by social desirability bias and recall bias and may lead to a certain degree of misclassification. Also, the questionnaire used to ascertain engagement in RST did not allow for a continuous variable of the total time engaged in RST. In addition, the questionnaire used for preschoolers showed a low internal consistency for the sedentary behaviors section [20], which suggests low agreement between the items to assess the sedentary behaviors construct. However, for the analyses conducted in this paper, not all of the items were taken into account given that the variable of interest was RST and not sedentary behaviors as a broad construct. Finally, RST at the school setting may be underestimated, since the questionnaire used for preschoolers only inquired about activities conducted out of the school setting. For school-aged children and adolescents, the context of the screen time-related activities was not assessed, but the questions used inquired exclusively about non schoolwork-related activities.
In conclusion, the majority of Colombian children and adolescents have excessive RST and several factors were identified that can be considered in the design of strategies to decrease these behaviors. The non-modifiable factors identified in this study can guide interventions aimed at decreasing RST among children and youth, for target populations such as younger preschoolers, older school-aged children, children and adolescents from urban areas and the wealthiest children and adolescents. Significant modifiable factors, such as availability of electronic devices, provide guidance for promising strategies that can be considered as part of a comprehensive initiative to reduce RST, such a public health campaigns to reduce the availability of TVs and electronic devices in children’s bedrooms and not eating in front of the TV.
Ethics Statement
The studies involving human participants were reviewed and the ENSIN protocol was approved by the Profamilia Institutional Review Board on Research involving Human Subjects and the Colombian National Institutes of Health (file number 2-2015, 26 February 2015). The secondary data analyses were approved by the University of Ottawa (file number H-06-19-3564). Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Author Contributions
Conceptualization, SG, OS, and MT; Data curation, SG; Formal analysis, SG; Data interpretation, SG, OS, AF-P, PK, J-PC, and MST; Writing—original draft, SG; Writing—critical review and editing, OS, AF-P, PK, J-PC, and MT. All authors have read and agreed to the submitted version of the manuscript.
Funding
SG was funded by the Government of Ontario and the University of Ottawa through the Ontario Trillium Scholarship for doctoral studies.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.ssph-journal.org/articles/10.3389/ijph.2022.1604217/full#supplementary-material
References
1. Tremblay, MS, Aubert, S, Barnes, JD, Saunders, TJ, Carson, V, Latimer-Cheung, AE, et al. Sedentary Behavior Research Network (SBRN) – Terminology Consensus Project Process and Outcome. [Internet]. Int J Behav Nutr Phys Act (2017) 14(1):75. doi:10.1186/s12966-017-0525-8 [cited 2018 Oct 22] Available from: http://www.ncbi.nlm.nih.gov/pubmed/28599680, 2021-02-07.
2. Carson, V, Hunter, S, Kuzik, N, Gray, CE, Poitras, VJ, Chaput, J-P, et al. Systematic Review of Sedentary Behaviour and Health Indicators in School-Aged Children and Youth: an Update. [Internet]. Appl Physiol Nutr Metab (2016) 41(6 Suppl. 3):S240–65. doi:10.1139/apnm-2015-0630 [cited 2018 Dec 9]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/27306432, 2020-03-31.
3. Stiglic, N, and Viner, RM. Effects of Screentime on the Health and Well-Being of Children and Adolescents: A Systematic Review of Reviews. [Internet]. BMJ Open (2019) Vol. 9:e023191. doi:10.1136/bmjopen-2018-023191 [cited 2021 Feb 7]. Available from: /pmc/articles/PMC6326346/?report=abstract, 2021-02-07.
4. LeBlanc, A, Gunnell, K, Prince, S, Saunders, T, Barnes, J, and Chaput, J-P. The Ubiquity of the Screen: An Overview of the Risks and Benefits of Screen Time in Our Modern World. [Internet]. Transl J Am Coll Sport Med (2017) 2(17):104–13. doi:10.1249/TJX.0000000000000039 [cited 2021 Feb 7] Available from: https://journals.lww.com/acsm-tj/Fulltext/2017/09010/The_Ubiquity_of_the_Screen__An_Overview_of_the.1.aspx, 2021-02-07.
5. Chaput, JP, Willumsen, J, Bull, F, Chou, R, Ekelund, U, Firth, J, et al. 2020 WHO Guidelines on Physical Activity and Sedentary Behaviour for Children and Adolescents Aged 5-17 years: Summary of the Evidence. Int J Behav Nutr Phys Act (2020) 17(1):141–9. doi:10.1186/s12966-020-01037-z
6. Aubert, S, Barnes, JD, Abdeta, C, Abi Nader, P, Adeniyi, AF, Aguilar-Farias, N, et al. Global Matrix 3.0 Physical Activity Report Card Grades for Children and Youth: Results and Analysis from 49 Countries. [Internet]. J Phys Act Health (2018) 15(S2):S251–73. doi:10.1123/jpah.2018-0472 [cited 2018 Dec 9]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/30475137, 2020-03-31.
7. Arundell, L, Fletcher, E, Salmon, J, Veitch, J, and Hinkley, T. A Systematic Review of the Prevalence of Sedentary Behavior during the After-School Period Among Children Aged 5-18 Years. [Internet]. Int J Behav Nutr Phys Act (2016) 13(1):93. doi:10.1186/s12966-016-0419-1 [cited 2018 Jun 4] Available from: http://ijbnpa.biomedcentral.com/articles/10.1186/s12966-016-0419-1, 2021-02-07.
8. Ng, SW, and Popkin, BM. Time Use and Physical Activity: a Shift Away from Movement across the globe. [Internet]. Obes Rev (2012) 13(8):659–80. doi:10.1111/j.1467-789x.2011.00982.x [cited 2018 May 25] Available from: http://www.ncbi.nlm.nih.gov/pubmed/22694051, 2021-02-07.
9. Tremblay, MS, Carson, V, Chaput, J-P, Connor Gorber, S, Dinh, T, Duggan, M, et al. Canadian 24-Hour Movement Guidelines for Children and Youth: An Integration of Physical Activity, Sedentary Behaviour, and Sleep. [Internet]. Appl Physiol Nutr Metab (2016) 41(6 Suppl. 3):S311–27. doi:10.1139/apnm-2016-0151 [cited 2018 Jul 17] Available from: http://www.ncbi.nlm.nih.gov/pubmed/27306437, 2020-03-31.
10.Australian Government Department of Health. Australia’s Physical Activity and Sedentary Behaviour Guidelines 5-12 Years. [Internet] (2017). Available from: http://www.health.gov.au/internet/main/publishing.nsf/Content/F01F92328EDADA5BCA257BF0001E720D/$File/brochure PA Guidelines_A5_5-12yrs.pdf, 2021-02-07.
11. Kruusamäe, H, Kull, M, Mooses, K, Riso, EM, and Jürimäe, J. Results from Estonia's 2016 Report Card on Physical Activity for Children and Youth. J Phys Act Health (2016) 13(11):S150–6. doi:10.1123/jpah.2016-0239
12. Liu, Y, Tang, Y, Cao, ZB, Zhuang, J, Zhu, Z, Wu, XP, et al. Results from China's 2018 Report Card on Physical Activity for Children and Youth. J Phys Act Health (2018) 15(Suppl. 1):S333. in press. doi:10.1123/jpah.2018-0455
13. Khan, A, Kadir, MA, Choudhury, SR, Ashraf, F, Rahman, M, Ahmed, KR, et al. Results from Bangladesh's 2018 Report Card on Physical Activity for Children and Youth. J Phys Activity Health (2018) 15:S318–S319. [cited 2021 Feb 8]. doi:10.1123/jpah.2018-0419
14. Owen, N, Sugiyama, T, Eakin, EE, Gardiner, PA, Tremblay, MS, and Sallis, JF. Adults' Sedentary Behavior. Am J Prev Med (2011) 41(2):189–96. doi:10.1016/j.amepre.2011.05.013
15. Stierlin, AS, De Lepeleere, S, De Lepeleere, S, Cardon, G, Dargent-Molina, P, Hoffmann, B, et al. A Systematic Review of Determinants of Sedentary Behaviour in Youth: A DEDIPAC-Study. Int J Behav Nutr Phys Act (2015) 12(1). doi:10.1186/s12966-015-0291-4
16.Instituto Colombiano de Bienestar Familiar. In: ICBF Bogotá, editor. Encuesta nacional de la situación nutricional en Colombia ENSIN 2005. Bogota: Instituto Colombiano de Bienestar Familiar (2005).
17. Gomez, LF, Parra, DC, Lobelo, F, Samper, B, Moreno, J, Jacoby, E, et al. Television Viewing and its Association with Overweight in Colombian Children : Results from the 2005 National Nutrition Survey : A Cross Sectional Study. Int J Behav Nutr Phys Activity (2005) 8:1–8. doi:10.1186/1479-5868-4-41
18.Instituto Colombiano de Bienestar Familiar. In: ICBF Bogotá, editor. Encuesta Nacional de la Situación Nutricional en Colombia ENSIN 2010. Bogota: Instituto Colombiano de Bienestar Familiar ICBF (2010).
19.Instituto Colombiano del Bienestar Familiar, Instituto Nacional de Salud. Ministerio de la protección social. [Internet]. In: DC Bogotá, editor. Encuesta Nacional de la Situación Nutricional en Colombia 2015 ENSIN (2018). Available from: https://www.icbf.gov.co/bienestar/nutricion/encuesta-nacional-situacion-nutricional, 2020-03-31.
20. Camargo, DM, Santisteban, S, Paredes, E, Flórez, MA, and Bueno, D. Confiabilidad de un cuestionario para medir la actividad física y los comportamientos sedentarios en niños desde preescolar hasta cuarto grado de primaria. Biomédica. (2015) 35(3):347–56. doi:10.7705/biomedica.v35i3.2502
21.World Health Organization. Guidelines on Physical Activity, Sedentary Behaviour and Sleep for Children under 5 Years of Age. [Internet]. Geneva (2019). Available from: https://apps.who.int/iris/handle/10665/311664, 2020-03-31.
22.U.S. Centers for Disease Control and Prevention. Youth Risk Behavior Surveillance System (YRBSS). [Internet] (2012). [cited 2018 Jan 11]. Available from: https://www.cdc.gov/healthyyouth/data/yrbs/index.htm, 2019-01-29.
23. LeBlanc, AG, Katzmarzyk, PT, Barreira, TV, Broyles, ST, Chaput, JP, Church, TS, et al. Correlates of Total Sedentary Time and Screen Time in 9-11 Year-Old Children Around the World: The International Study of Childhood Obesity, Lifestyle and the Environment. PLoS One (2015) 10(6):e0129622–20. doi:10.1371/journal.pone.0129622
24.WHO Multicentre Growth Reference Study Group. WHO Child Growth Standards Based on Length/height, Weight and Age. (Oslo, … [Internet]. Acta Paediatr (2006) 95:76–85. doi:10.1111/j.1651-2227.2006.tb02378.x [cited 2014 Jun 16] Available from: http://www.ncbi.nlm.nih.gov/pubmed/16817681, 2021-04-01.
25. de Onis, M, Onyango, AW, Borghi, E, Siyam, A, Nishida, C, and Siekmann, J. Development of a WHO Growth Reference for School-Aged Children and Adolescents. [Internet]. Bull World Health Organ (2007) 85(9):660–7. doi:10.2471/blt.07.043497 [cited 2014 May 28] Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2636412&tool=pmcentrez&rendertype=abstract, 2021-04-01.
26.World Health Organization. [Internet]. In: Global Recommendation on Physical Activity for Health. Geneva: World Health Organization (2010). p. 10–58. [cited 2018 Jan 11] Available from: http://www.who.int/dietphysicalactivity/factsheet_recommendations/en/, 2021-04-01.
27. González, SA, Sarmiento, OL, Katzmarzyk, PT, Chaput, J-P, Camargo-Lemos, DM, and Tremblay, MS. Prevalence and Correlates of Meeting Physical Activity Guidelines Among Colombian Children and Adolescents. [Internet]. J Phys Act Health (2021) 18:400–17. doi:10.1123/jpah.2020-0568 [cited 2021 Apr 1] Available from: https://pubmed.ncbi.nlm.nih.gov/33657528/, 2021-04-01.
28. Saelens, BE, Sallis, JF, Frank, LD, Couch, SC, Zhou, C, Colburn, T, et al. Obesogenic Neighborhood Environments, Child and Parent Obesity: The Neighborhood Impact on Kids Study. Am J Prev Med (2012) 42(5):e57–64. doi:10.1016/j.amepre.2012.02.008
29. Vancampfort, D, Van Damme, T, Firth, J, Hallgren, M, Smith, L, Stubbs, B, et al. Correlates of Leisure-Time Sedentary Behavior Among 181,793 Adolescents Aged 12-15 Years from 66 Low- and Middle-Income Countries. PLoS One (2019) 14(11):e0224339. doi:10.1371/journal.pone.0224339
30. Shalani, B, Azadfallah, P, and Farahani, H. Correlates of Screen Time in Children and Adolescents: A Systematic Review Study. J Mod Rehabil (2021) 15(October):187–208. doi:10.18502/jmr.v15i4.7740
31.World Health Organization. Global 24-Hour Movement Recommendations for the Early Years (0-4 Years). Geneva (2019).
32. Pearson, N, and Biddle, SJH. Sedentary Behavior and Dietary Intake in Children, Adolescents, and Adults. Am J Prev Med (2011) 41(2):178–88. doi:10.1016/j.amepre.2011.05.002
33. Jusienė, R, Urbonas, V, Laurinaitytė, I, Rakickienė, L, Breidokienė, R, Kuzminskaitė, M, et al. Screen Use during Meals Among Young Children: Exploration of Associated Variables. [Internet]. Medicina (2019) 55(10):688. doi:10.3390/medicina55100688 [cited 2021 Apr 1] Available from: /pmc/articles/PMC6843261/, 2021-04-01.
34. Monteiro, CA, Cannon, G, Moubarac, JC, Martins, APB, Martins, CA, Garzillo, J, et al. Dietary Guidelines to Nourish Humanity and the Planet in the Twenty-First century. [Internet], A blueprint Brazil Public Health Nutr (2015) 18. 2311–22. doi:10.1017/s1368980015002165 [cited 2021 Apr 16] Available from: https://www.cambridge.org/core, 2021-04-16.
35. Temmel, CP, and Rhodes, RE. View of Correlates of Sedentary Behaviour in Children and Adolescents Aged 7-18_ A Systematic Review.Pdf. Heal Fit J Can (2013) 6(1):119–99. doi:10.14288/hfjc.v6i1.146
36. Chaput, JP, Leduc, G, Boyer, C, Bélanger, P, LeBlanc, AG, Borghese, MM, et al. Electronic Screens in Children's Bedrooms and Adiposity, Physical Activity and Sleep: Do the Number and Type of Electronic Devices Matter. Can J Public Health (2014) 105(4):e273–9. doi:10.17269/cjph.105.4511
37. Sheldrick, MP, Maitland, C, Mackintosh, KA, Rosenberg, M, Griffiths, LJ, Fry, R, et al. Associations between the Home Physical Environment and Children's Home-Based Physical Activity and Sitting. Int J Environ Res Public Health (2019) 16(21):1–21. doi:10.3390/ijerph16214178
38. Parkes, A, Green, M, and Pearce, A. Do bedroom Screens and the Mealtime Environment Shape Different Trajectories of Child Overweight and Obesity? Research Using the Growing up in Scotland Study. [Internet]. Int J Obes (2020) 44(4):790–802. doi:10.1038/s41366-019-0502-1 [cited 2021 Apr 1] Available from: https://pubmed.ncbi.nlm.nih.gov/31827254/, 2021-04-16.
39. Atkin, AJ, Corder, K, and van Sluijs, EMF. Bedroom media, Sedentary Time and Screen-Time in Children: A Longitudinal Analysis. [Internet]. Int J Behav Nutr Phys Act (2013) 10(1):137. doi:10.1186/1479-5868-10-137 [cited 2021 Apr 1] Available from: http://ijbnpa.biomedcentral.com/articles/10.1186/1479-5868-10-137, 2021-04-01.
40. Mielke, GI, Brown, WJ, Nunes, BP, Silva, ICM, and Hallal, PC. Socioeconomic Correlates of Sedentary Behavior in Adolescents: Systematic Review and Meta-Analysis. [Internet]. Sport Med (2017) 47(1):61–75. doi:10.1007/s40279-016-0555-4 [cited 2021 Mar 30] Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5215067/, 2021-03-30.
41. Jaacks, LM, Vandevijvere, S, Pan, A, McGowan, CJ, Wallace, C, Imamura, F, et al. The Obesity Transition: Stages of the Global Epidemic. Lancet Diabetes Endocrinol (2019) 7(3):231–40. doi:10.1016/s2213-8587(19)30026-9
42. Triana, CA, Sarmiento, OL, Bravo-Balado, A, González, SA, Bolívar, MA, Lemoine, P, et al. [Internet]. In: A Vuillemin, editor. Active Streets for Children: The Case of the Bogotá Ciclovía, 14. San Francisco: PLoS One (2019). p. e0207791. doi:10.1371/journal.pone.0207791 [cited 2019 May 15] Available from: http://dx.plos.org/10.1371/journal.pone.0207791, 2021-04-16.
43. González, SA, Triana, CA, Abaunza, C, Aldana, L, Arias-Gómez, LF, Bermúdez, J, et al. Results from Colombia’s 2018 Report Card on Physical Activity for Children and Youth. [Internet]. J Phys Act Health (2018) 15(S2):S335–7. doi:10.1123/jpah.2018-0422 [cited 2018 Dec 9] Available from: http://www.ncbi.nlm.nih.gov/pubmed/30475133, 2021-04-16.
44. Popkin, BM, Adair, LS, and Ng, SW. Global Nutrition Transition and the Pandemic of Obesity in Developing Countries. [Internet]. Nutr Rev (2012) 70(1):3–21. doi:10.1111/j.1753-4887.2011.00456.x [cited 2018 Jun 12] Available from: http://www.ncbi.nlm.nih.gov/pubmed/22221213, 2021-04-16.
45. Moore, SA, Faulkner, G, Rhodes, RE, Brussoni, M, Chulak-Bozzer, T, Ferguson, LJ, et al. Impact of the COVID-19 Virus Outbreak on Movement and Play Behaviours of Canadian Children and Youth: A National Survey. [Internet]. Int J Behav Nutr Phys Act (2020) 17(1):6. doi:10.1186/s12966-020-00987-8 [cited 2021 Apr 3]. Available from: https://pubmed.ncbi.nlm.nih.gov/32631350/, 2021-04-03.
Keywords: children, surveillance, adolescents, screen exposure, sedentary behaviors
Citation: González SA, Sarmiento OL, Florez-Pregonero A, Katzmarzyk PT, Chaput J-P and Tremblay MS (2022) Prevalence and Associated Factors of Excessive Recreational Screen Time Among Colombian Children and Adolescents. Int J Public Health 67:1604217. doi: 10.3389/ijph.2022.1604217
Received: 24 April 2021; Accepted: 21 January 2022;
Published: 23 February 2022.
Edited by:
Lena Isabel Barrera Vergara, University of Valle, ColombiaReviewed by:
Marta Lima-Serrano, Sevilla University, SpainGerardo Zavala, University of York, United Kingdom
Copyright © 2022 González, Sarmiento, Florez-Pregonero, Katzmarzyk, Chaput and Tremblay. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Silvia A. González, c2dvbnowMjVAdW90dGF3YS5jYQ==